
Abstract
Objective
To assess and compare the accuracy of 3D-printed digital models, orthognathic surgical splints, retainers or aligners, and implant surgical guides printed using various 3D printing technologies.
Methods
The search comprised prospective and retrospective studies related to the accuracy of 3D-printed models, splints, implant surgical guides, and retainers/aligners in patients undergoing orthodontic and orthognathic surgical procedures. The outcomes were assessed in terms of linear measurements, degree of fit, and positional deviations in comparison to conventional plaster models and surgical acrylic splints. The methodologic quality of the articles and the level of evidence were assessed using the QUADAS-2 tool. A meta-analysis was performed to compare the accuracy of models printed by different technologies to plaster models using the random-effects model.
Results
Twenty-one retrospective studies were included. Quality assessment of all included articles showed moderate risk of bias and no article was excluded. The systematic review showed that there were no significant differences between printed surgical splints, retainers/aligners compared, and the control group. Meta-analysis of six eligible studies showed that printed models had a general trend toward overestimation of linear measurements (mean difference = 0.22 mm; 95% confidence interval = – 0.09 to 0.36 mm, I2 = 85%). Measurements made on digital light processing-printed models were significantly different than those made on plaster models.
Conclusion
The mean difference of 0.22 mm in linear measurements made on 3D-printed models and plaster models was clinically acceptable. Among the various printing technologies, PolyJet and fused deposition modeling-printed models showed higher accuracy. The printed splints and retainers/aligners were as accurate and reliable as their respective gold standards. The findings should be interpreted with caution due to high level of heterogeneity.
Keywords
Introduction
The system of three-dimensional (3D) printers, functioning together with intraoral scanners and model scanners, is a landmark innovation in orthodontics. Synonymous to additive manufacturing, “3D printing is a technology whereby sequential layers of material are deposited on top of one another to eventually form an object”. 1 Chuck Hull in 1984 2 first developed the 3D printing concept and in 1986 established the “3D Systems Company” with the first machine for rapid prototyping, which was called “stereolithography (SLA)”. Fused deposition modeling (FDM) technology, developed by Scott Crump in 1988, was widely marketed by Stratasys in 1990. 3 Objet Geometries in 1988 introduced “PolyJet photopolymer printing (PPP)”. A multitude of 3D printers adopting variants of SLA, FDM, digital light processing (DLP), and PolyJet technologies are now accessible from various companies all over the world.
Rapid prototyping generates a physical reproduction of a digital model and thus overcomes the latter’s limitation of being intangible and is much more convenient to be used for complicated treatment planning procedures.
Virtual surgical planning for bimaxillary orthognathic surgery is faster and cheaper than standard planning. 4 3D-printed surgical splints seem to be a viable alternative to traditional acrylic splints. Lauren and McIntyre commercialized digital splints by fabricating the first computer-designed occlusal splints in the year 2008. 5
Geometric inaccuracies are common and are often caused during the impression collection and thermoforming processes for the fabrication of aligners and retainers; this could be minimized through the utilization of digital technologies, 3D modeling, and rapid prototyping techniques.
Miniscrew insertion using surgical guides is becoming increasingly popular as it improves the stability and accuracy of implant insertion. In 47.4% of maxillary and 48.3% of mandibular miniscrews inserted using a direct manual technique, contact with or damage to anatomic structures surrounding the roots of teeth was observed, according to Kuroda et al. 6 Current literature search revealed many studies that have compared the accuracy of 3D-printed models, surgical splints, retainers/aligners, and implant surgical guides to the current “gold standards” adopted in clinical practice such as plaster models, acrylic splints, and thermoformed retainers/aligners.
Thus, the objectives of this systematic review were to (a) determine and compare the reliability and accuracy of 3D digital models printed using various 3D printing technologies with those obtained through conventional oral impressions, intraoral scanning, and model scanning; (b) compare the accuracy of conventional acrylic surgical splints and 3D-printed surgical splints; (c) compare the accuracy of thermoformed retainers/aligners and 3D-printed clear aligners/retainers; and (d) check the accuracy of miniscrew implant placement using 3D-printed implant surgical guides.
Materials and Methods
Registration of Protocol
“The Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) 2020 guidelines 7 were followed in the execution of this systematic review. The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number (CRD42020175511).
Eligibility Criterion and Study Selection
Information and Sources
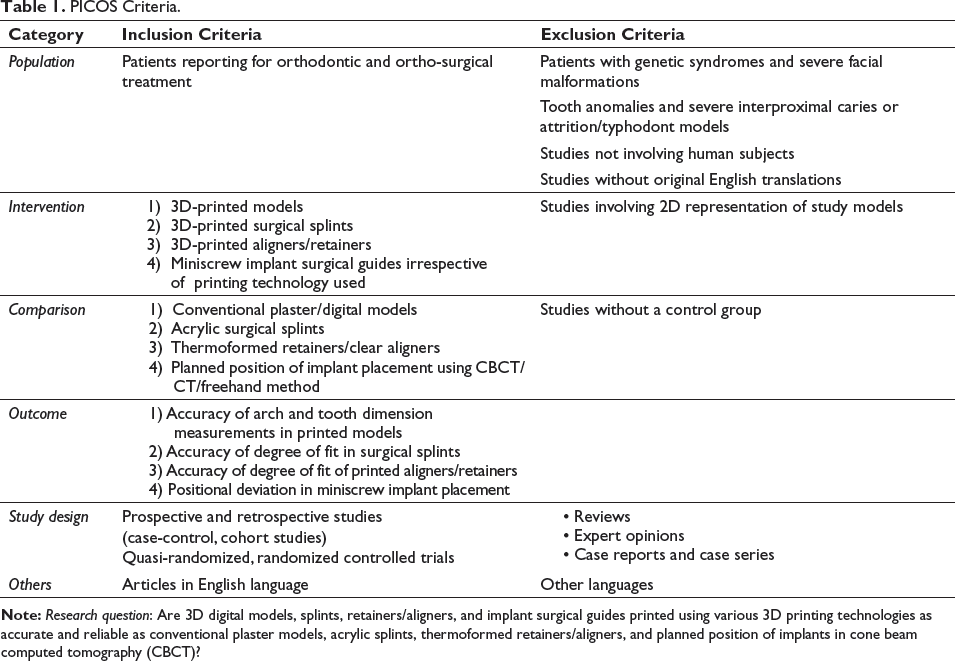
A literature search was conducted till April 2023 in the electronic databases, PubMed Central (NCBI), Cochrane Library, Embase, Scopus, and Web of Science as the primary sources. The electronic search was supplemented with manual search in the reference lists of relevant articles. Gray literature was identified by searching OpenGrey and Google Scholar (Table 1, Supplementary Table 1).
PICOS Criteria.
Search Strategy
All the searches were independently conducted by two different investigators. The stepwise strategy involved screening of the articles received after electronic search by reading the title and abstract. After the removal of duplicates, the references of these articles were manually searched to include all related studies that have been missed in the preliminary search. Finally, selected articles were included after full text reading according to the inclusion and exclusion criteria. Lack of agreement at any stage was resolved by mutual discussion and consensus
Data Extraction
Each study was assessed separately for result derivation. The primary data collected from the included studies were (a) author, journal name, and year of publication; (b) sample size; (c) number of subjects in the intervention group and type of intervention; (d) number of subjects in the control group; (e) mean age if mentioned; (f) printer type; (g) outcome measures; (h) results; and (i) conclusions.
Wherever standard error was not originally reported in individual studies, it was computed using MD – 1.96SD = loa; MD + 1.96SD = LOA, SE = SD/√(n); MD: mean difference, SD: standard deviation, loa: lower limit of agreement, LOA: upper limit of agreement, SE: standard error, n: sample size. 8
Data Analysis
“Review Manager (RevMan), Version 5.3, The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, 2014” was used to statistically pool the data and conduct the meta-analysis. Using the inverse variance weighted approach, the MD and SE of the individual studies were combined.
The trials that had similar treatments, participants, and results were combined, and the results were expressed as an effect measure using the highest reported MDs in linear measurements and the 95% confidence intervals (CIs) that went along with them. A random-effects model was used to calculate the weighted mean difference (WMD) of the treatment effect. Sensitivity analysis was done wherever there was a lot of heterogeneity. Publication bias was inspected using the generated funnel plot.
Quality (Risk of Bias) Assessment of the Selected Studies
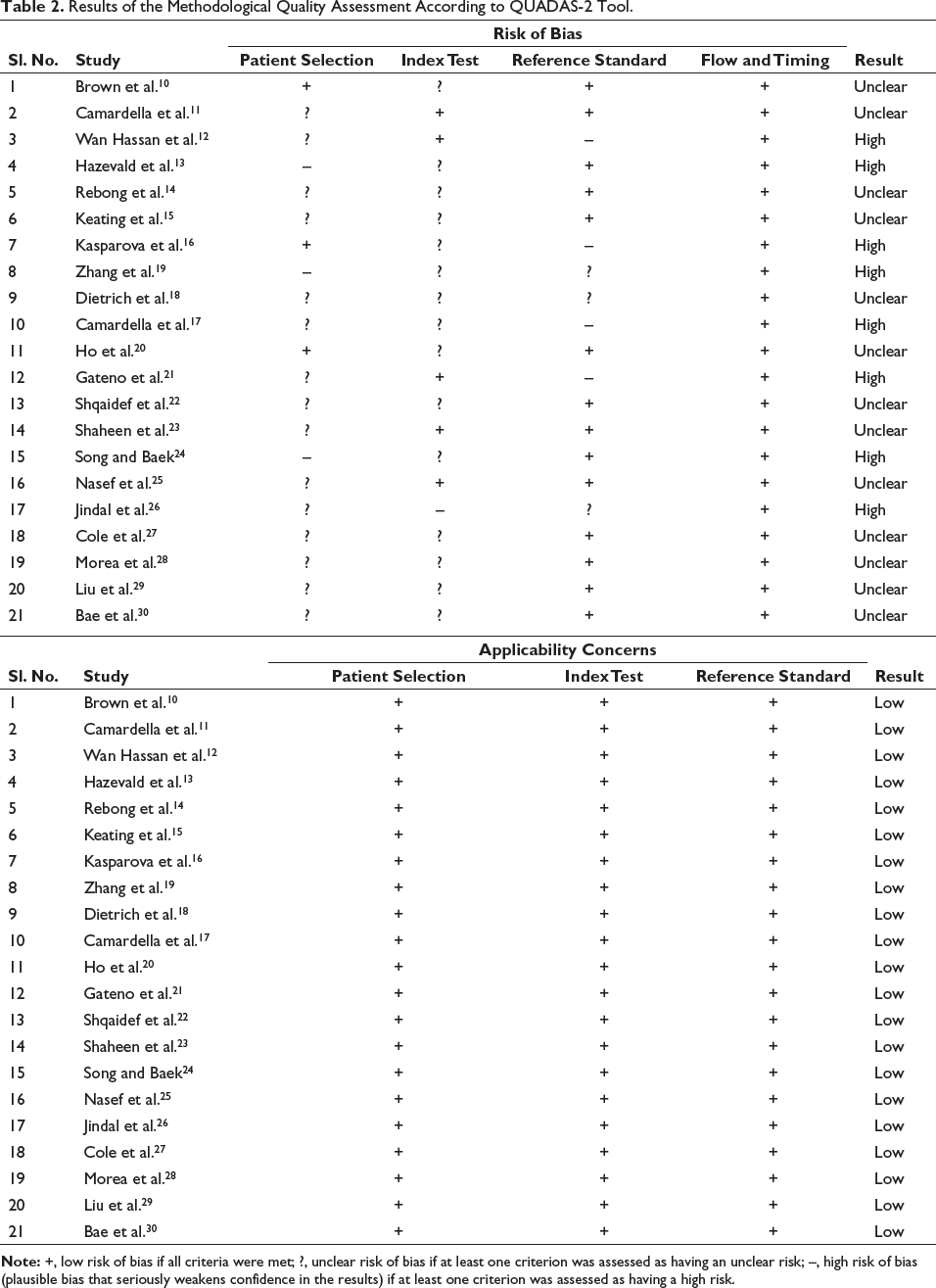
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool 9 (Table 2, Supplementary Table 2) was used to rate the methodologic quality of the articles and to assess the level of evidence. Quality assessment was done independently by two investigators. The quality assessment was based on patient selection, index test, reference standard, flow, and timing to measure the risk of bias and applicability concerns.
Results of the Methodological Quality Assessment According to QUADAS-2 Tool.
Results
Study Selection
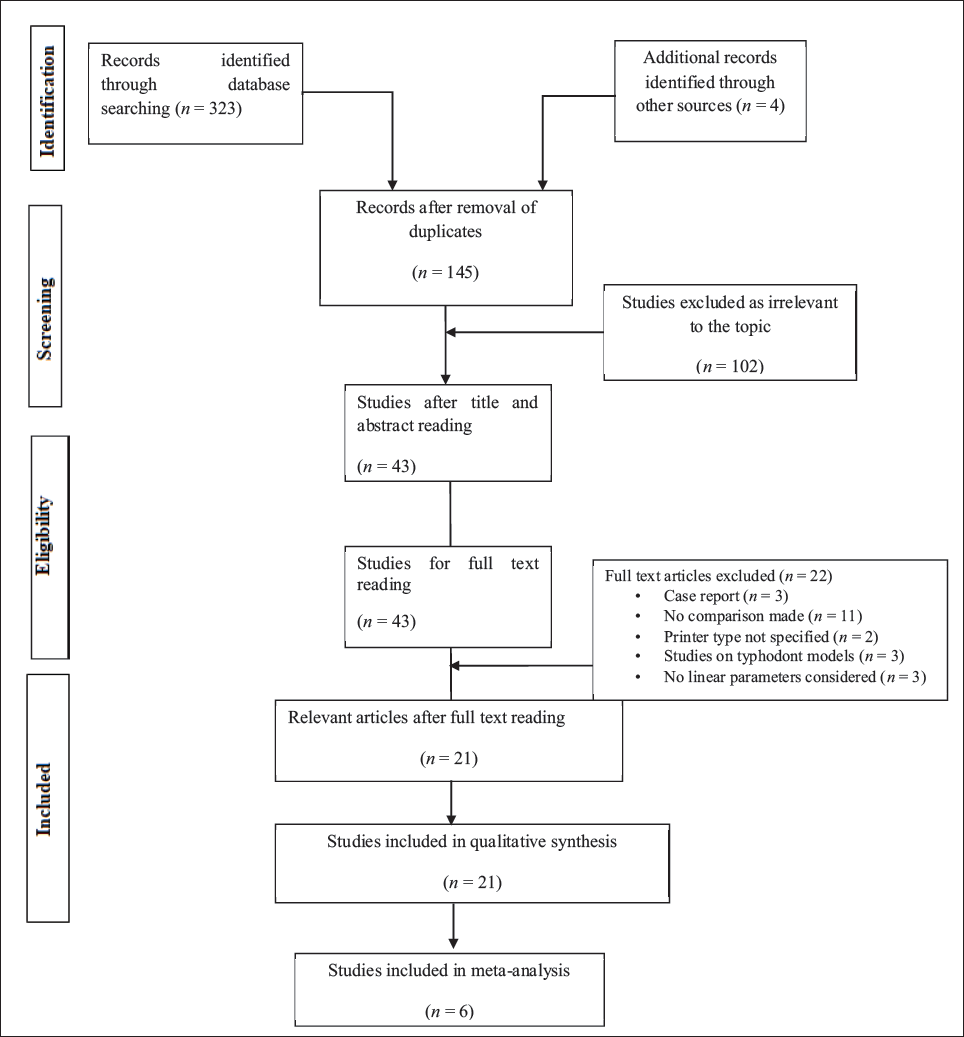
An overview of the selection process is depicted in the PRISMA flow diagram (Figure 1). The search strategy yielded a total of 43 studies. 21 studies were finally included in this systematic analysis after two-stage selection criteria which included title and abstract reading followed by full text reading. 22 studies were excluded including case reports and noncomparative studies due to lack of consideration of linear parameters (Figure 1 and Supplementary Table 3). No randomized clinical trials were found pertaining to this topic.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram of Study Selection.
Risk of Bias Assessment in Included Studies (Table 2)
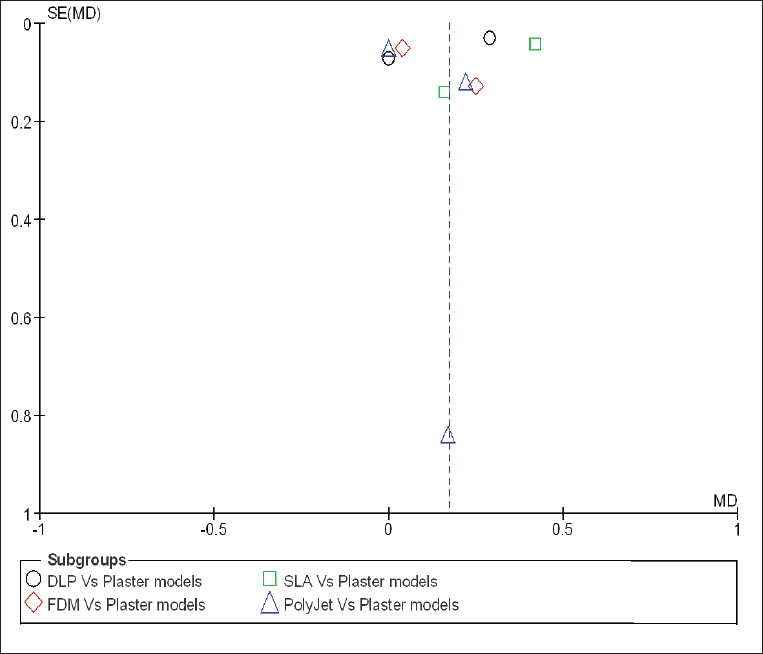
The most recurrent sources of bias were related to the patient selection processes and the lack of proper blinding procedures (Figure 2). No article was excluded after the QUADAS-2 tool application. A funnel plot, which is a scatterplot of each treatment effect (mean) by the standard deviation of the study’s precision, was used to analyze publication bias. Figure 3 shows all studies are of similar size and equally distributed on both sides. So, there is no need to repeat literature search. The symmetric funnel plot in this study shows the risk of bias by placing the most accurate studies at the top.
Funnel Plot of Comparison of Overall Outcome between 3D-printed Models and Plaster Models.
Risk of Bias for the Included Studies.
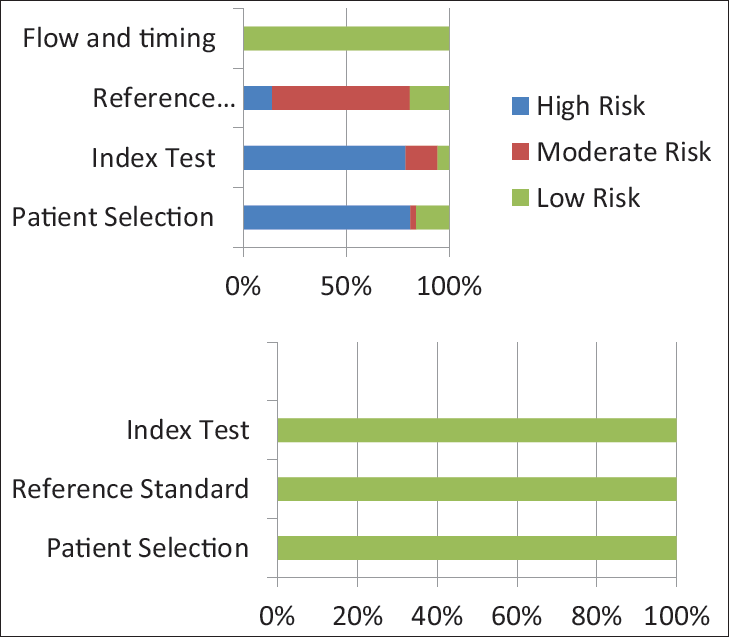
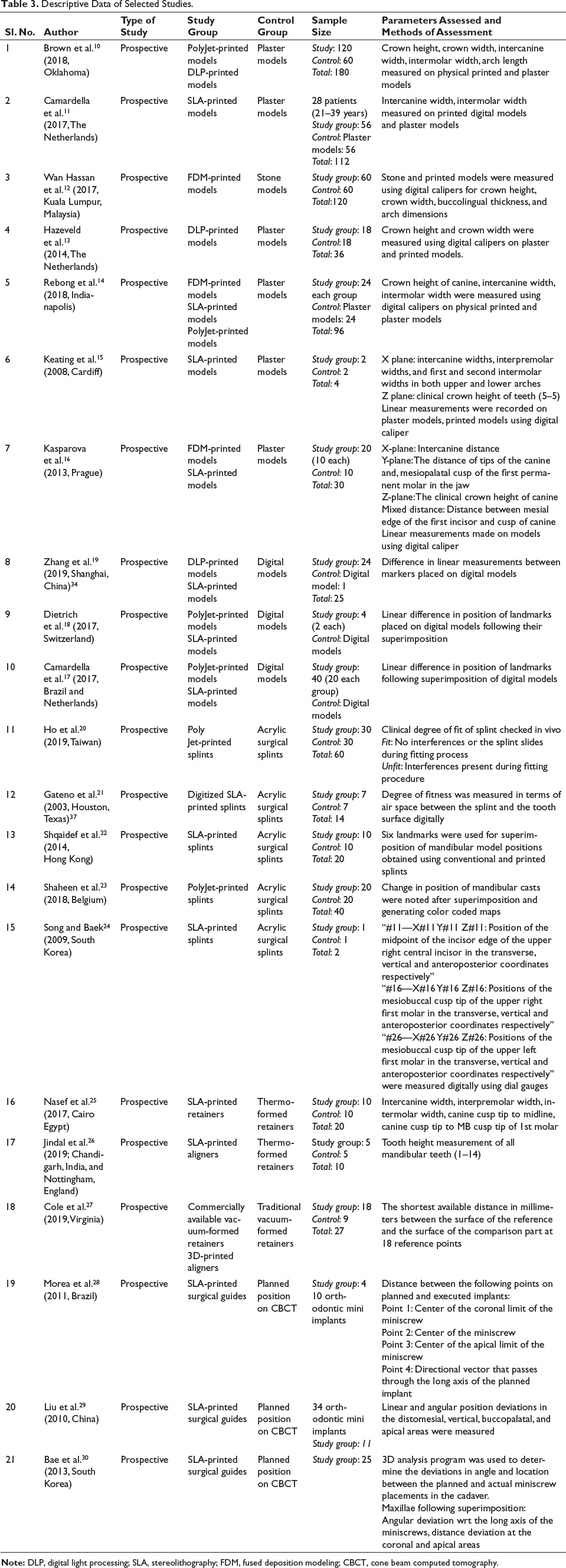
Table 3 shows descriptive data of the included studies. Out of 21 included studies, 7 assessed accuracy of 3D-printed models using digital caliper measurements on physical 3D-printed and plaster models.10–16 Three studies evaluated accuracy through 3D superimposition of the digitized models.17–19 Five studies assessed accuracy of printed surgical splints.20–24 The accuracy of 3D-printed clear aligners or retainers25–27 and accuracy of 3D-printed miniscrew implant insertion guides28–30 were evaluated by three studies each.
Descriptive Data of Selected Studies.
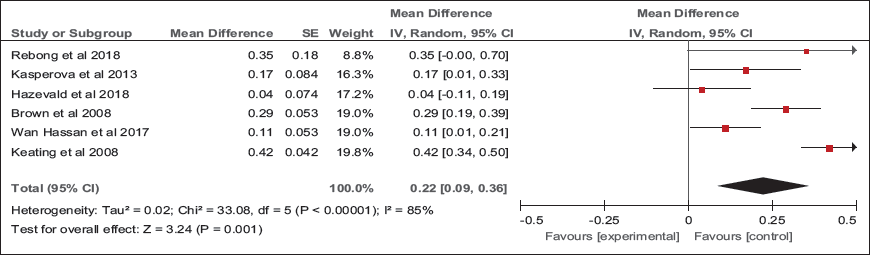
Six studies10, 12–16 out of twenty-one studies with adequate recording of data and similar methodology were included for meta-analysis. The MD in linear measurements (crown height, crown width, intercanine width, and intermolar width) between printed models and plaster models was presented using forest plot. Subgroup analysis was done to assess the accuracy of different printing technologies.
Accuracy of Printed Models
Linear Measurements
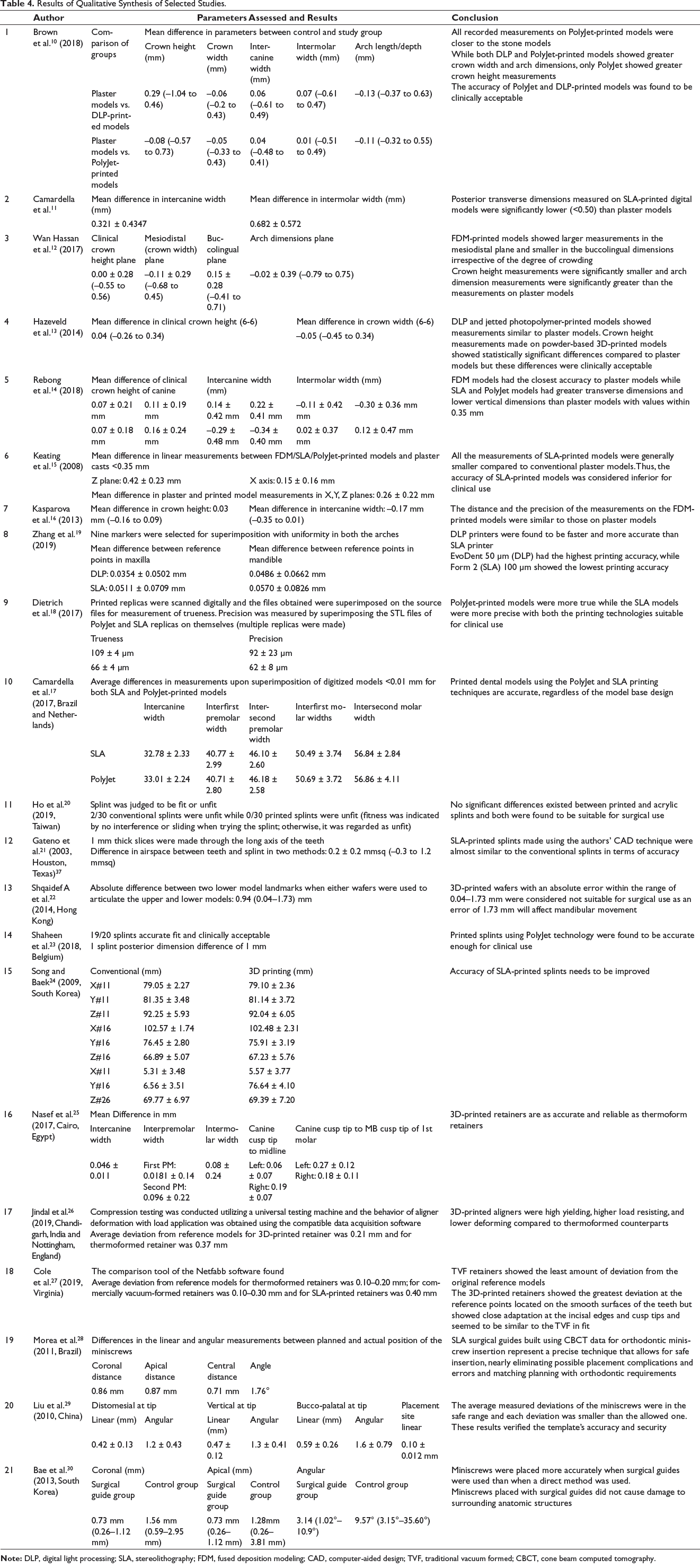
The arch dimensions measured in the included studies involved intercanine width, intermolar width, and arch depth. Three studies12, 13, 16 assessed these parameters individually while other studies15, 17, 20 evaluated all parameters combined as arch dimensions. Arch depth was measured as a separate entity only by Brown et al. 10 where the MD between plaster and printed models ranged from –0.37 to 0.63 mm for DLP and –0.32 to 0.55 mm for PolyJet printers.
Figure 4 shows forest plot of the combined results of the meta-analysis. The overall results showed significant difference between measurements made on printed models compared to plaster models (MD = 0.22 mm; 95% CI = 0.09–0.36 mm). However, this outcome showed high heterogeneity (I2 = 85%).
Forest Plot Depicting Comparison between Accuracy of Printed Models and Plaster Models.
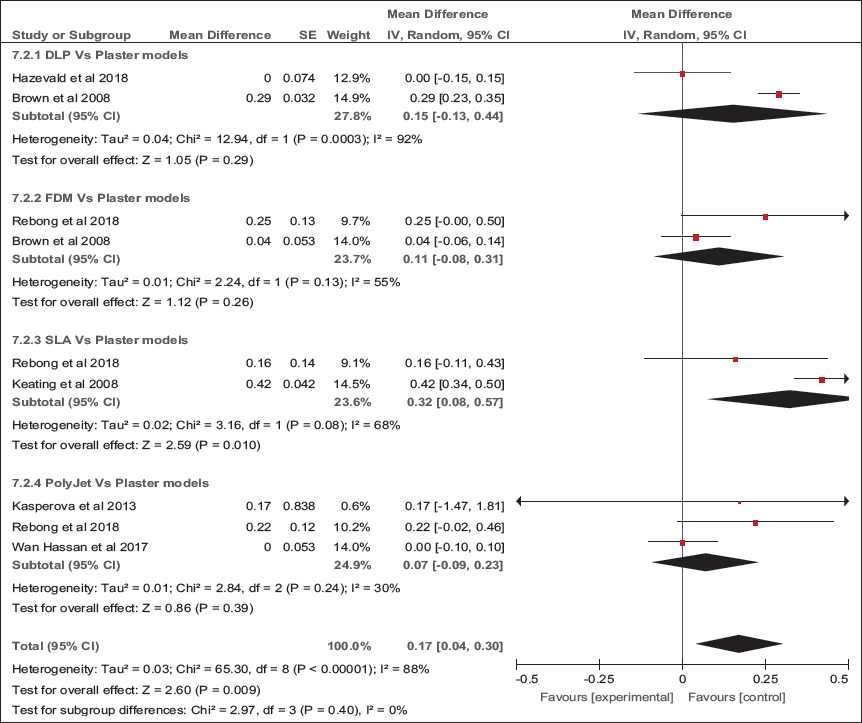
Subgroup analysis showed an overestimation of measurements by PolyJet models (MD = –0.07 mm; 95% CI = –0.09 to 0.23, I2 = 30%), SLA models (MD = 0.32 mm; 95% CI = 0.08–0.57, I2= 68%), DLP-printed models (MD = 0.15 mm; 95% CI = –0.13 to 0.44, I2 = 92%), and FDM models (MD = 0.11 mm; 95% CI = –0.08 to 0.31, I2 = 55%). Forest plot shows only significant results for SLA versus plaster models (p = 0.010), although with heterogeneity of 68%. All these findings show high heterogeneity and hence should be considered with caution (Figure 5).
Subgroup Analysis.
Accuracy of 3D-printed Splints
All studies showed acceptable accuracy of 3D-printed splints compared to conventional splints.20–24 The difference in only the vertical parameters showed clinical significance (Table 4). 23
Accuracy of Printed Aligners and Retainers
Cole et al. 27 reported that the traditional vacuum-formed (TVF) retainers had the smallest deviation from their reference models ranging from 0.10 to 0.20 mm as compared to 0.10 to 0.40 mm of deviation for the printed retainers. Jindal et al. 26 reported that the printed aligners showed a deviation of 2.55% (0.21 mm) and the thermoformed aligner, 4.41% (0.37 mm) from their parent STL file. Nasef et al. 25 found no clinically significant differences between thermoformed and printed retainers except for the distance of the left mandibular canine from the midline (Table 4).
Accuracy of Printed Miniscrew Insertion Guides
Planned and actual miniscrew positions were compared in three dimensions using cone beam computed tomography (CBCT). Morea et al., 28 Bae et al., 30 and Liu et al. 29 showed that the linear and angular deviations between planned and actual miniscrew positions were statistically significant (Table 4).
Discussion
In this systematic review, strict selection criteria were used to include the articles related to 3D-printed models, surgical splints, and retainers/aligners with the objective of evaluating the accuracy of 3D printing technologies. Funnel plot was used to analyze the publication bias. The upper portion of the plot shows the studies with lowest standard deviation and are the most accurate. The graph should have a shape of an inverted funnel which is symmetrical in the absence of bias and heterogeneity. In this study the funnel plot is symmetrical with the most accurate studies at the top of the plot.31 The six studies to assess the accuracy of printed models and conventional plaster models as control were included in the meta-analysis. The findings suggest that there was a significant difference in the linear measurements made on the printed 3D models compared to plaster models. Whereas subgroup analysis showed significant differences only for SLA compared to plaster models. The accuracy of all other printed models was statistically similar to plaster models. The accuracy of 3D-printed surgical splints, retainers, and implant surgical guides is also comparable to their respective gold standards. However, the reliability of the results is questionable due to the high degree of heterogeneity.
The quality assessment tool (QUADAS-2) showed that subject selection method was not random in most of the included studies. The methods used to perform the measurements were very clear and comprehensive enough to allow the reviewer to answer the review question in all studies. However, in only two studies, index tests were evaluated independent of the reference standard. Sample sizes in the studies included were small and the interpretations of results were also diverse. Thus, the lack of randomization and blinding may have introduced selection bias. Small samples and diverse results may have contributed to the high heterogeneity.
Accuracy of Printed Models
In terms of the printing process, the accuracy of the constructed models may be affected by the accuracy of the machine, the materials used, and the subsequent model shrinkage during building and postcuring. 32 The combined MD of linear measurements between printed models and plaster models according to the present meta-analysis is 0.22 mm (0.09–0.36 mm) which is in the clinically acceptable range of 0.20–0.50 mm.9, 12, 33, 34
The results of the present meta-analysis revealed that the MD between DLP, SLA, PolyJet and FDM-printed models, and plaster models were 0.15, 0.32, 0.07, and 0.11 mm, respectively. This shows that PolyJet printers were slightly more accurate than the rest of the printing technologies, though all of them were accurate enough for clinical use.9, 12, 33, 34
Dental models printed with the PolyJet technology are fully cured during the building process and do not need a postcuring process, which leads to a faster and more efficient printing process. The only disadvantage of this type of printer is its greater cost of printing and wastage of the printing resin. Our meta-analysis showed a significant overestimation of linear measurements in SLA-printed models than the other printing technologies as the SLA build technology requires postcuring the printed parts to improve the stability of the printed object; this residual polymerization affects the overall accuracy of the model as supported by almost every study which evaluated this type of printer.14–16, 22 DLP printers were reported to be faster than SLA printers by Zhang et al. 19 and this might be due to the use of light projectors in DLP printers that can cure a much larger area while in SLA printing technology, the laser source cures only a small area of the resin covering the build tray.
Accuracy of Printed Splints
Irrespective of the printing technology used, virtual planning of orthognathic surgery and printed splints generated using the STL files of the patients’ occlusion are accurate enough for surgical use and can replace acrylic splints. The difference between conventional model occlusion and virtual occlusion was found to be in the range of 0.45–0.6 mm,20, 35 which is within 1.5 mm that is considered to be tolerable positional variation between the virtual intermaxillary position and intraoperative intermediate intermaxillary relationship according to Hernández-Alfaro and Guijarro-Martínez. 36 Three out of five comparative studies included in this review reported that there exists no significant difference between printed and acrylic splints while the rest reported clinically significant differences. The difference in maxillary position registered using conventional and 3D digital splints was between 0.18 and 1.73 mm.22, 24, 37
Accuracy of Printed Aligners and Retainers
The direct 3D printing of clear orthodontic retainers has not been investigated much in the literature. Zilberman et al. 32 did not find any statistically significant differences between the selective laser sintering (SLS) printed and thermoformed retainers. This could be because the study’s measurements were small. In the study by Cole et al., the TVF retainers were used as a benchmark to assess and contrast the fit of the 3D-printed retainers. 27 The printed retainers deviated from the reference model the most, up to 0.40 mm, with the majority of the deviations occurring at the reference points that were on the teeth’s smooth surfaces. As opposed to this study, Jindal et al. 26 concluded that cured aligners that were 3D-printed exhibited superior dimensional accuracy and compressive mechanical strength in comparison with uncured 3D-printed aligners and thermoformed aligners.
Accuracy of Printed Miniscrew Insertion Guides
All three studies28–30 that evaluated the accuracy of miniscrew placement using printed surgical guides unanimously concluded that it was a superior and more accurate method of implant insertion. All the included studies suggest that root contact was rare and that the miniscrews could be stably placed with a surgical guide.
Limitations
The methodological quality of most of the included studies in this systematic review was moderate due to the lack of randomization of samples and lack of blinding procedures. Randomized clinical trials with proper blinding to compare the accuracy of printed models/splints/miniscrew surgical guides/retainers/aligners should be conducted.
Conclusion
Though the differences in linear measurements made to determine the accuracy of 3D-printed models and plaster models (mean: 0.22 mm) were significant but these differences were clinically acceptable for all the printers. However, the reliability of the results is questionable due to high heterogeneity. 3D-printed surgical splints were equal to acrylic splints in terms of accuracy and resultant positional variation of skeletal bases during orthognathic surgery. The accuracy of 3D-printed aligners/retainers when compared to thermoformed retainers had conflicting results. There is a need for further studies on a larger sample size. 3D-printed implant surgical guides were found to be accurate and reliable for precise miniscrew insertion.
Results of Qualitative Synthesis of Selected Studies.
Footnotes
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.