
Abstract
Objective
The aim was to evaluate the efficiency of customized orthodontic appliances, developed using patient-specific anatomical data, compared to conventional fixed appliances.
Materials and Methods
Electronic databases such as PubMed, ScienceDirect, LILACS, Cochrane Trials, German National Library of Medicine, and OpenGrey were searched for relevant articles without any restrictions on publication date or language. After removing duplicates, articles were screened based on the pre-established eligibility criteria using the PICOS (participants, intervention, comparison, outcomes, study design) framework. Risk of bias and quality of evidence were evaluated, and a random-effects meta-analysis with a 95% confidence interval was conducted.
Results
Nine studies (three randomized controlled trials and six observational studies) met the inclusion criteria. Four of them studied labial customized appliances, while five studies were on lingual customized appliances. The meta-analysis found that customized appliances significantly reduced treatment duration (−3.91 months, P = .02) compared to conventional systems, although heterogeneity was high (I2 = 88%). There were no significant differences in the American Board of Orthodontics-Discrepancy Index (ABO-DI) or cast-radiograph evaluation (ABO-CRE) scores. The overall risk of bias was moderate, and the certainty of evidence ranged from low to moderate. Narrative synthesis was carried out for peer assessment rating scores, emergency visits, patient discomfort, and speech difficulties. Sensitivity analyses were performed to assess the robustness of pooled estimates. Subgroup analyses showed a more pronounced treatment duration benefit in labial customized appliances, while lingual customized appliances showed more patient-reported issues.
Conclusion
Customized orthodontic systems significantly shorten treatment time compared to conventional systems; however, this should be interpreted with caution due to high heterogeneity. No significant difference was noted in clinical outcomes (ABO-DI and ABO-CR scores). While faster treatment is the primary benefit, factors such as cost, discomfort, and planning time need to be assessed in future trials. Further research on cost-effectiveness and long-term stability is needed to guide clinical decisions.
Introduction
Fixed orthodontic therapy to correct malocclusion was introduced almost a hundred years ago by Angle in 1925 with the Edgewise appliance, which was subsequently modified by Andrews, incorporating first-, second-, and third-order movements within the bracket. This modification served as the basis of the pre-adjusted edgewise appliance (PEA) as we know it. 1
Different prescriptions and bracket designs were developed over the years to improve treatment efficiency. 2 Despite these advancements, finishing requires wire bending to complete treatment due to variations in tooth morphology and inaccuracies in bracket placement. This not only increases total treatment duration, but also decreases treatment efficiency.
To reduce human error during bracket placement, indirect bonding was introduced by Silverman et al. in 1972. 3 However, a recent systematic review by Patano et al. revealed that even though it minimizes bracket placement errors, it still takes a longer time to complete than traditional methods. 4 Customization in brackets, wires, aligners, and various orthodontic appliances is now more feasible due to technological advancements like digital intraoral scanning, computer-aided design (CAD), 3D printing, and artificial intelligence.5, 6 Patients treated with a customized CAD/computer-aided manufacturing (CAM) orthodontic system showed fewer archwire appointments, shorter overall treatment time, and lower American Board of Orthodontics (ABO) scores. 7 However, systematic reviews on the comparison between customized and non-customized orthodontic appliances have been limited. Ke et al. systematically reviewed the treatment effectiveness between aligners and fixed appliances. 8 They found that aligners showed segmented movement of teeth and shortened treatment duration, but they were not as effective in producing adequate occlusal contacts, controlling tooth torque, and retention. Customized retainers fabricated via CAD/CAM showed a lower plaque index than conventional retainers. 9
Currently, customized fixed orthodontic appliances are fabricated in the office using CAD/CAM; commercially available, such as the Insignia™ (Ormco, Calif), and Incognito (3M Unitek, Bad Essen, Germany).10–12 Orthodontists can adopt customized systems to begin treatment with the final goal in mind and streamline mechanics to reach the best possible outcome. In the coming years, technological advancements such as artificial intelligence will be able to aid in making customization simpler and more accessible for orthodontists. Yassir et al. conducted a systematic review limited to prospective studies, which may have excluded relevant data from high-quality retrospective research. 13 To address this gap, the present review includes a broader range of study designs, including randomized, prospective, and retrospective cohort studies, to provide a more comprehensive evaluation of the available evidence on the treatment efficiency and clinical outcomes of customized fixed appliances. The review question guiding this systematic review was “Do customized fixed orthodontic appliances (labial or lingual) improve treatment efficiency or clinical outcomes compared to conventional fixed orthodontic appliances in adolescent and adult patients?”
Materials and Methods
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020 were followed for conducting this systematic review and meta-analysis. 14 The study protocol was registered with PROSPERO (International Prospective Registry of Systematic Reviews) with registration number CRD42022309855.
Eligibility Criteria
The PICOS (participants, intervention, comparison, outcomes, study design) framework was used to establish eligibility criteria (Appendix A). Both randomized and non-randomized studies comparing malocclusion treatment in orthodontic patients using customized versus conventional fixed appliances were included. Studies involving adjunct treatments like skeletal anchorage, extraoral traction, low-level laser therapy, pharmacological interventions, or supplemental vibration were excluded.
The primary aim of this study was to evaluate the efficacy of customized fixed appliances based on treatment duration, while secondary outcomes included clinical performance indicators (American Board of Orthodontics-Discrepancy Index (ABO-DI), American Board of Orthodontics-cast-radiograph evaluation (ABO-CRE), peer assessment rating (PAR)), treatment mechanics (e.g., bracket loss, number of visits), and patient-centered factors (e.g., comfort, speech, mastication), in comparison to conventional fixed appliances.
Search Strategy
Electronic databases, including PubMed, ScienceDirect, LILACS, Cochrane Trials, German National Library of Medicine, and OpenGrey, were searched for relevant articles without restrictions on publication date or language. The search strategy combined Medical Subject Headings (MeSH) and common terms such as “malocclusion OR dental alignment,” “orthodontic appliance design,” “orthodontics, corrective/instrumentation or methods,” “Custom* or computer-aided design or image processing,” and “treatment outcome or clinical efficacy.” Appendix B details the search sequence for each database. Manual cross-referencing was also conducted to identify any missed studies.
Screening and Selection of Papers
Articles from all sources were uploaded to the Rayyan QCRI application. 15 Two independent reviewers (SV and GM) removed duplicates and screened articles based on eligibility criteria. Full-text assessments were conducted for final inclusion. In the case of disagreement, the final reviewer (PC) was consulted, and resolutions were guided by the Cochrane Handbook for Systematic Reviews of Interventions. 16
Data Collection, Items, and Processing
Two reviewers (SV and NKD) independently extracted data using predesigned forms covering study design, patient characteristics, interventions, controls, total number of patients, mean age, treatment duration, measured parameters, statistical tests, and results. They recorded data, cross-checked entries, and resolved discrepancies with the final reviewer (PC). For studies with missing information, attempts were made to retrieve data through email correspondence with authors. If unsuccessful, estimation methods from the Cochrane Handbook for Systematic Reviews of Interventions were used. 16
Assessment of Quality and Risk of Bias (RoB) of Included Studies
Cochrane guidelines were used to evaluate the RoB in the included studies, using the ROBINS-I tool for non-randomized studies and the RoB 2 tool for randomized trials.17, 18 Two reviewers (SV and NKJ) conducted the assessment independently, resolving disagreements with the final reviewer (PC).
The ROBINS-I tool assessed bias across seven domains, rating each as “Low,” “Moderate,” “Serious,” “Critical,” or “No Information.” An overall RoB judgment was made after domain assessments. 17 For RoB 2, bias was rated in five domains as “Low,” “Some Concerns,” or “High,” with overall risk determined accordingly. 18
Summary Measures and Data Synthesis
The following details were recorded and evaluated based on the outcomes of the included studies: treatment duration, ABO index, PAR index, and differences in oral comfort, speech, mastication, and hygiene. Means and standard deviations were noted; if values were not reported, they were calculated per Cochrane guidelines or obtained from the authors. A random-effects model was used for the meta-analysis to account for heterogeneity in patient characteristics, interventions, and study designs. 19 Heterogeneity was assessed using forest plots, the Cochrane Q test, and I2 statistics. 20 I2 values of 0%-40% indicated minimal heterogeneity, 40%-60% moderate, 60%-90% substantial, and 90%-100% considerable. Publication bias was examined with funnel plots.21, 22
Certainty Assessment
GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) tool was used to evaluate the quality of evidence for each primary outcome variable via GRADEpro (
Results
Study Selection (Figure 1)
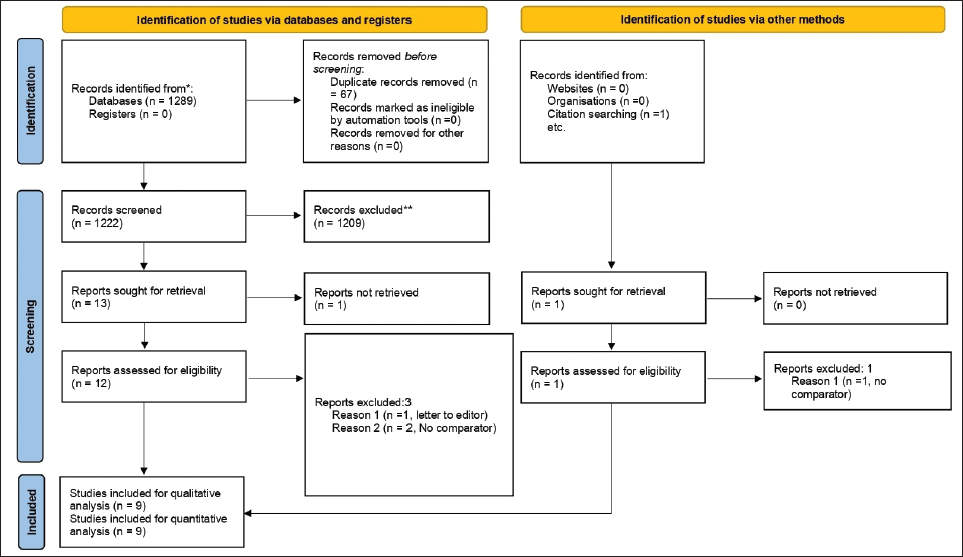
Figure 1 shows the PRISMA flow diagram for the study screening process. A total of 1,289 records were identified from databases like PubMed, ScienceDirect, LILACS, Cochrane Trials, German National Library of Medicine, and OpenGrey, and uploaded to Rayyan QCRI. After removing 67 duplicates, 1,222 studies were screened based on predefined eligibility criteria. Full-text assessment of 12 studies led to the exclusion of 3, with 9 included in the final analysis. Reasons for exclusion are detailed in Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Flow Diagram.
Study Characteristics
Study design, characteristics of patients, intervention, control, total number of patients, mean age (in years) of the sample, total treatment duration, parameters measured, statistical tests, and results of the included studies are presented in Table 1. Among the nine studies, six were observational cohort studies (three prospective, three retrospective), and three were randomized controlled trials (RCTs).7, 24–31
Characteristics of the Studies Included in the Systematic Review.
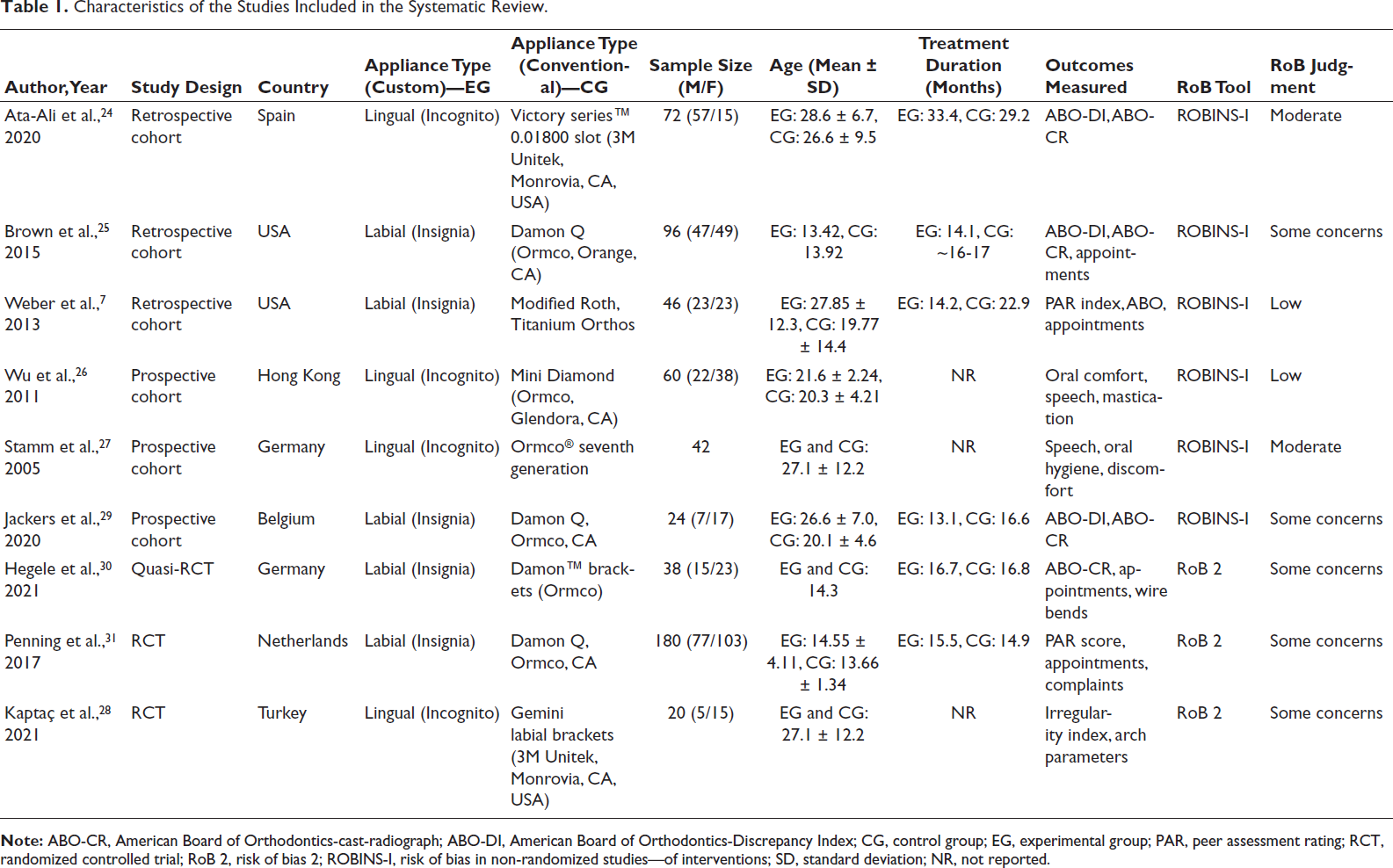
Conventional fixed orthodontic appliances were McLaughlin, Bennet, and Trevisi (MBT), Damon self-ligating appliances were most frequently used, whereas Incognito (lingual) and Insignia (labial) systems were the most commonly used customized fixed PEAs. The total number of patients varied amongst the studies from 20 to 180, with a mean age of 13-27 years, irrespective of sex.
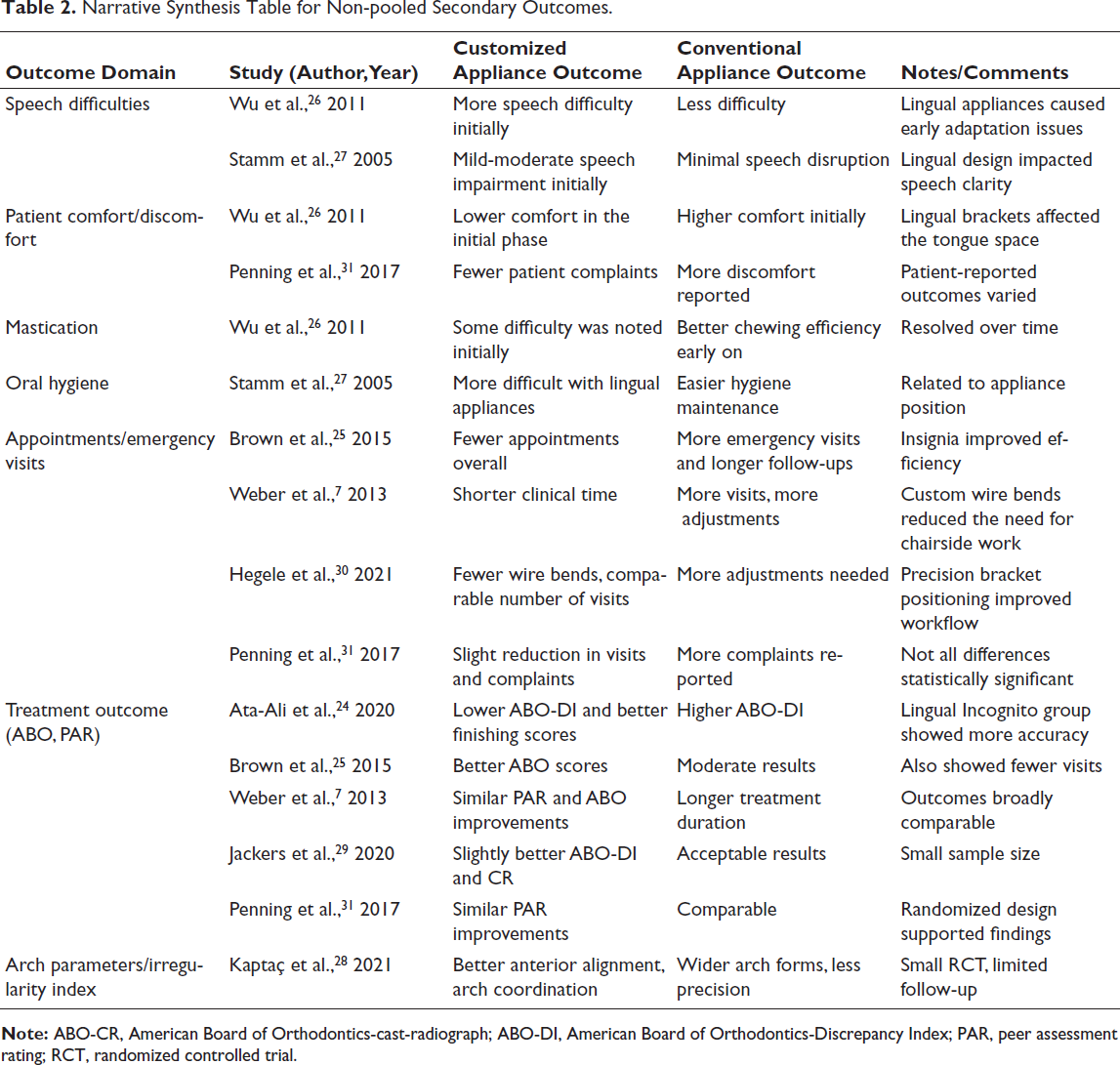
Most studies evaluated ABO and treatment duration, whereas two studies evaluated oral discomfort, mastication, speech disturbances, and social pressure. Primary studies by Hegele et al. 30 and Penning et al. 31 evaluated the number of lost or repositioned brackets, archwire bends, visits, and complaints, along with a little irregularity index. Kaptaç et al. measured the irregularity index, and it was the only study that measured intermolar width, intercanine width, and arch length between customized and conventional fixed orthodontic appliances. 28 PAR score was measured by Penning et al. 31 and Weber et al. 7 to evaluate orthodontic treatment quality. Detailed narrative synthesis of secondary outcomes, such as PAR scores, speech, oral discomfort, mastication, and emergency visits, is presented in Table 2.
Narrative Synthesis Table for Non-pooled Secondary Outcomes.
RoB in Studies (Figures 2 and 3)
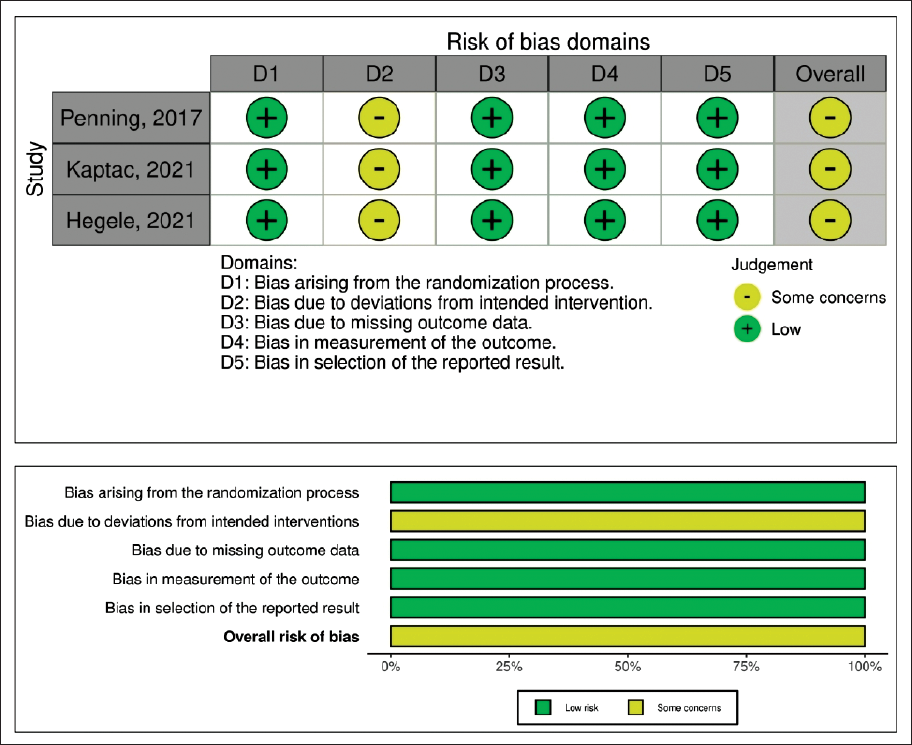
The ROBINS-I tool was used to assess the RoB in six non-randomized studies,7, 24–27, 29 and the RoB 2 tool was applied to three randomized trials.28, 30, 31 For ROBINS-I, two studies had moderate concerns in domain 1,25, 27 while the other domains showed low bias. Out of the six studies,7, 24–27, 29 only two had moderate concerns, as shown in Figure 2.25, 27 For RoB 2, all domains except domain 2 had a low RoB, with domain 2 showing some concerns in all three studies.28, 30, 31 Overall, the RoB was judged with some concerns, as shown in Figure 3.
ROBINS-I (Risk of Bias in Non-randomized Studies—of Interventions) of Included Studies.
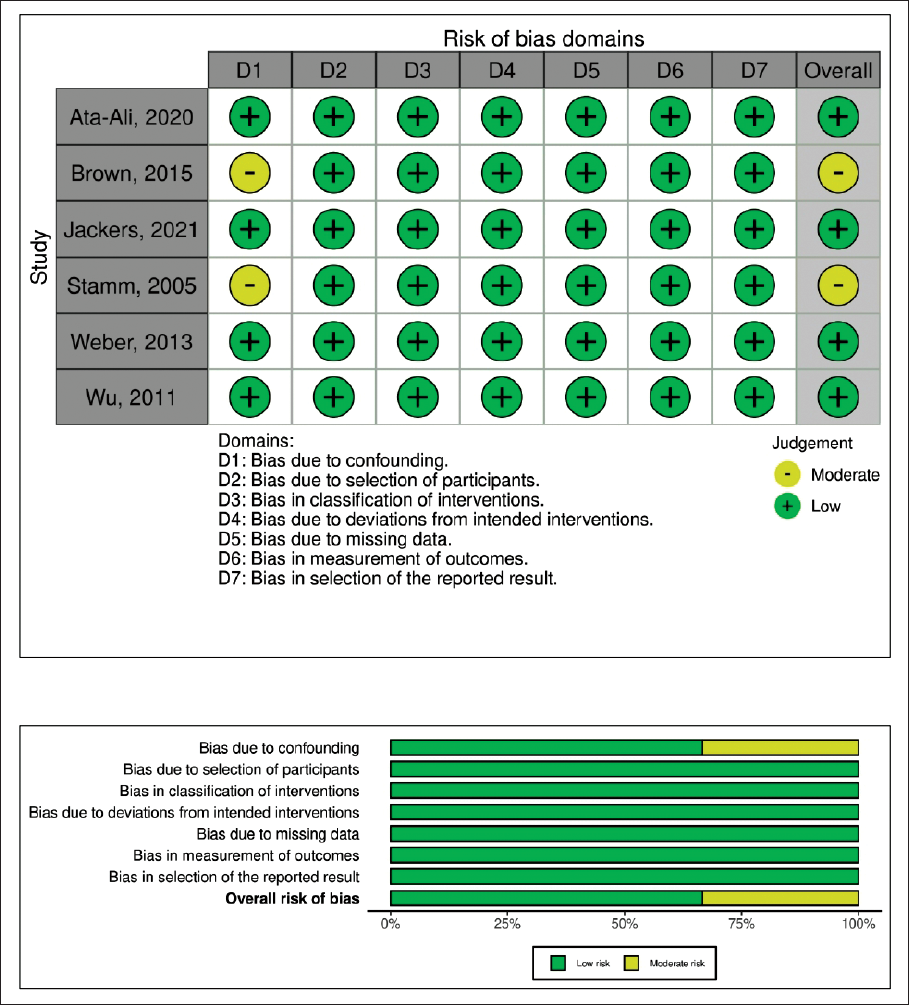
RoB 2 (Risk of Bias 2) of Included Studies.
Results of Meta Analysis (Figure 4)
Treatment Duration (Figure 4a)
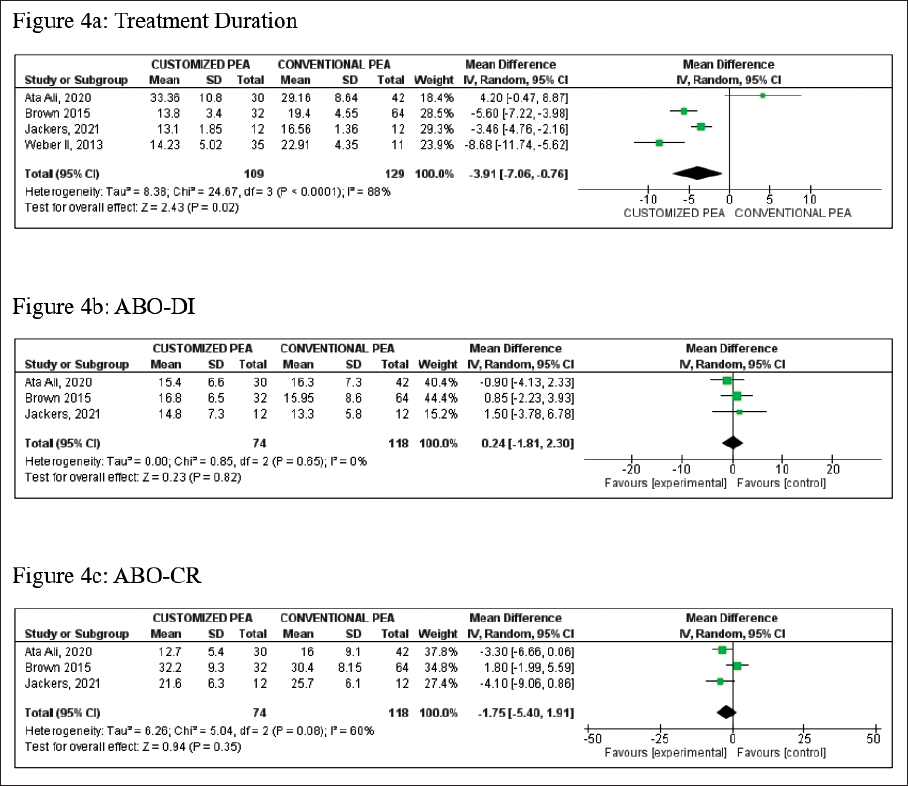
Comparison of treatment duration between customized PEA and conventional PEA is depicted in Figure 4a. The pooled mean difference in treatment duration was −3.91 months (95% CI: −7.06 to −0.76), indicating that customized PEA was associated with shorter treatment periods compared to non-customized PEA. However, considerable heterogeneity was seen among the included studies, with an I2 value of 88%, implying high variability in the results. Despite this heterogeneity, the overall effect was deemed to be statistically significant (P = .02), indicating that the shorter treatment duration associated with customized PEA is unlikely to be due to chance.
Results of Meta-analysis. (a) Treatment Duration. (b) American Board of Orthodontics-Discrepancy Index (ABO-DI) and (c) American Board of Orthodontics-cast-radiograph (ABO-CR).
ABO-DI (Figure 4b)
ABO-DI between customized PEAs and non-customized PEA revealed no significant differences between the two treatment approaches, as seen in Figure 4b (P = .82). The pooled mean difference was 0.24 (95% CI: −1.81 to 2.30), indicating a slight but statistically insignificant trend favoring customized PEA. The heterogeneity among studies was negligible, with an I2 value of 0%, suggesting that the results across studies were consistent.
ABO-CR (Figure 4c)
The ABO-CR scores between customized and non-customized PEAs showed no significant differences, as seen in Figure 4c. A slight trend toward better scores with customized PEA was observed with a pooled mean difference of −1.75 (95% CI: −5.40 to 1.91). Despite moderate heterogeneity in the studies (I2 = 60%), the difference in ABO-CR scores was not statistically significant (P value = .35).
Analysis of the Certainty of the Evidence
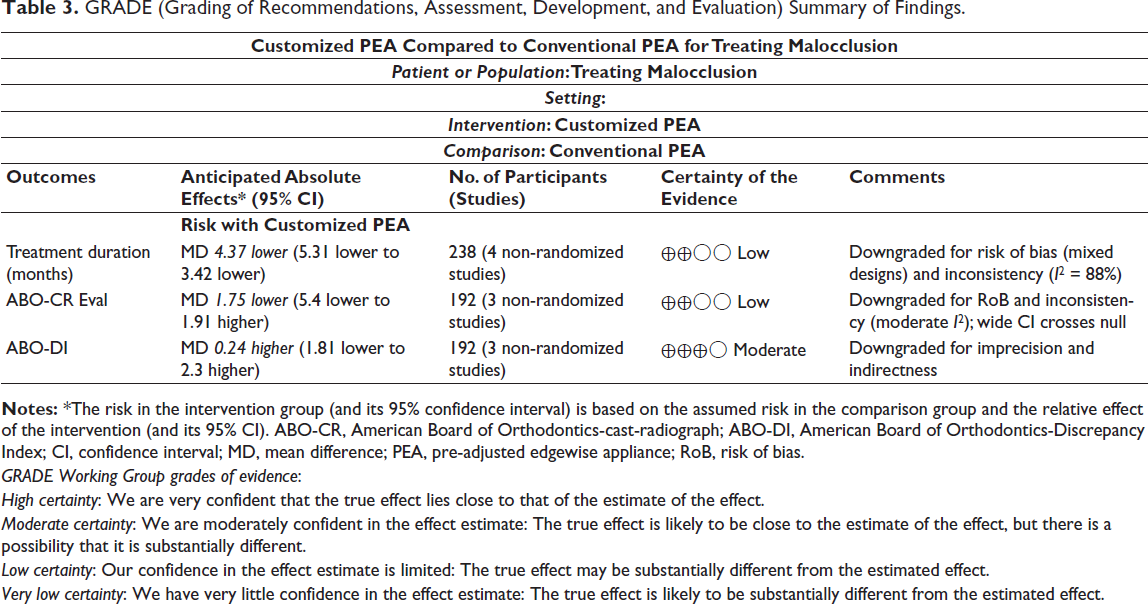
The certainty of evidence was assessed using the GRADE framework for treatment duration, ABO-CR scores, and ABO-DI. The GRADE certainty for reduced treatment duration and ABO-CR with customized PEA was rated low, likely due to study variation and biases as seen in Table 3. Certainty was downgraded based on GRADE domains: RoB (mixed study designs), inconsistency (heterogeneity in outcomes), and imprecision (wide confidence intervals). In contrast, the ABO-DI certainty was rated moderate, indicating higher confidence.
GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) Summary of Findings.
GRADE Working Group grades of evidence:
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimated effect.
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimated effect.
Sensitivity and Subgroup Analysis
Sensitivity analyses were performed to assess the robustness of pooled estimates. For treatment duration, the random-effects model continued to show a statistically significant reduction in the customized group (MD = −3.91 months; 95% CI: −7.06, −0.76), despite high heterogeneity (I2 = 88%). For ABO-DI and ABO-CR scores, results were consistent across fixed- and random-effects models, with no significant differences between customized and conventional systems. These analyses support the reliability of the observed treatment duration difference while highlighting the stability of ABO-DI and ABO-CR findings (Appendix C).
Subgroup analyses were conducted by appliance type (labial vs. lingual) and study design (RCTs vs. observational). The treatment duration benefit was more pronounced in studies using labially customized appliances. Lingual systems, though aesthetic, showed more patient-reported issues such as speech disturbances and discomfort. No consistent differences emerged in ABO-DI or ABO-CR outcomes across subgroups. These findings suggest that while customization may improve efficiency, appliance design and clinical context remain critical modifiers (Appendix D).
Discussion
Customized orthodontic appliances allow for precise and individualized treatment. The literature largely focuses on customized appliances like indirect bonding trays, aligners, and retainers.6, 7 To date, no comprehensive analysis has assessed the treatment efficacy of customized fixed orthodontic appliances. Thus, the aim of this systematic review was to compare treatment efficiency between customized- and conventional-fixed orthodontic appliances.
This review included nine studies, six observational7, 24–27, 29 and three RCTs,28, 30, 31 spanning diverse geographical regions. Participants were in their late teens to adulthood (mean age 20-30 years), with a slight skew toward females, with treatments involving lingual, labial, or self-ligating brackets.
This review provides strong evidence that customized systems like Incognito™ and Insignia™ offer several clinical advantages over conventional systems (e.g., Damon Q and Victory Series™), particularly in terms of shorter treatment durations. Patients treated with customized appliances completed treatment approximately 4 months earlier, a statistically significant and clinically relevant finding (P = .02), aligning with previous studies (Weber et al. 7 ; Jackers et al.; Bardideh et al.) that also reported fewer unscheduled appointments and more efficient outcomes. 9 A notable limitation of the meta-analysis is the substantial heterogeneity observed among the included studies (I2 = 88%), indicating high variability in study designs, patient demographics, and types of customized systems used. Notwithstanding this variability, the overall effect remains robust, with the probability of a chance finding being minimal. Brown et al. 25 and Jackers et al. 29 found that the number of treatment appointments and overall duration were significantly lower for patients using customized systems compared to conventional systems.25, 29 Jackers et al. reported a difference of over 100 days in treatment duration between groups treated with customized systems and conventional Damon brackets. 29 Additionally, fewer unscheduled emergency appointments and bracket repositioning were required in customized systems. This could be ascribed to better precision in bracket placement and higher control over tooth movements, thereby contributing to fewer treatment delays and more predictable treatment outcomes. These findings are in contrast with Yassir et al., 13 who found no significant differences in treatment duration. This could be explained by their stricter inclusion criteria, which resulted in the inclusion of fewer, primarily prospective studies, limiting the evidence base. 13
Clinical outcomes between customized and conventional orthodontic systems show varied results depending on the specific metric evaluated. For instance, studies indicate improvements in areas like treatment efficiency, but less so in others, such as the ABO-DI and ABO-CR scores. The meta-analysis revealed no statistically significant difference in ABO-DI scores between customized and conventional systems, exhibiting minimal heterogeneity (I2 = 0%), indicating consistency across studies analyzed. This undermines the notion that customized systems produce more improvements in discrepancy indices vis-à-vis conventional PEA systems. Similarly, for ABO-CR scores, the analysis showed a slight, nonsignificant trend toward better scores with customized systems. However, there was moderate heterogeneity (I2 = 60%), which may suggest some variability in the study’s results, but it was still insufficient to show a clear advantage of customized systems. Weber et al. highlighted that the total treatment time was shorter in the experimental group (using Insignia) than in the control group, with fewer unscheduled appointments and debonded brackets. 26 A more rapid realization of target outcomes, coupled with fewer in-treatment complications, contributes to better treatment efficiency. On a similar note, Penning et al. 31 and Hegele et al. 30 reported greater precision in tooth movement with customized systems. These findings are pivotal for orthodontists seeking optimized treatment timelines and bolstering long-term stability.
Patient experience plays a vital role in the success of orthodontic treatment, especially for adult patients who place great emphasis on aesthetics and comfort. The studies in this review offer mixed results in terms of patient satisfaction with customized systems. Wu et al. 26 and Stamm et al. 27 found that patients treated with lingual systems like Incognito™ reported more oral discomfort, speech disturbances, and difficulties with mastication. These negative experiences seemed to subside over time, and patient satisfaction eventually became comparable to those treated with conventional systems.
Lingual systems are commonly associated with speech disturbances, particularly during the initial phase of treatment, as noted by studies such as Stamm et al. 27 Nonetheless, patients adjusted to the lingual system within a few months with minimal long-term effects on speech. 27 It may be surmised that the long-term benefits of customized lingual systems, especially in terms of aesthetics, may outweigh the initial short-term speech impediment.
A recent systematic review by Yassir et al. found no significant differences in treatment duration, treatment outcomes, number of appointments, analgesic consumption, or patient satisfaction between customized and non-customized orthodontic appliances. 13 In contrast, the present meta-analysis reported a significant decrease in treatment duration with customized appliances. Yassir et al. followed a more exclusionary protocol, resulting in the inclusion of only four studies. A smaller pool of primary studies, along with variability in study design and quality, possibly impacted their findings. In contrast, this meta-analysis incorporated more studies, including rigorously designed RCTs, providing a more exhaustive dataset, allowing for stronger statistical power to detect differences.
Also, while Yassir et al. 13 focused primarily on clinical parameters of treatment outcomes, this review incorporated a broader spectrum of treatment-related factors, such as treatment efficiency, patient compliance, orthodontic precision, unscheduled appointments, and emergency visits, providing a more nuanced comprehension of clinical efficiency.
In comparing our findings with other forms of customization in orthodontics, it is worth noting that the systematic review by Ke et al., 9 which evaluated the treatment effectiveness of clear aligners versus conventional fixed appliances. Their meta-analysis concluded that while clear aligners offered superior aesthetics, patient comfort, and a significantly shorter treatment duration by 6.31 months (95% CI [−8.37, −4.24]), they were less effective than conventional braces in achieving adequate occlusal contacts, torque control, and transverse expansion.
This aligns with our findings, where customized fixed appliances such as Insignia™ and Incognito™ also demonstrated shorter treatment durations. However, unlike clear aligners, they preserved the full biomechanical advantages of fixed appliances. While both systems aim for personalization, aligners rely on segmented tooth movements and exhibit torque and rotational control limitations. In contrast, customized fixed appliances offer a combination of digital precision and full-arch mechanics, potentially providing a more optimal balance between treatment efficiency and control.
These insights emphasize the need for future research directly comparing all three systems, namely, conventional, clear aligners, and fully customized fixed appliances, to determine context-specific advantages and limitations.
Limitations and Future Research
Although they have a number of drawbacks, customized orthodontic systems show promise. The absence of subgroup-stratified outcome data from studies, which precluded quantitative subgroup analyses, was a limitation of the meta-analysis. This made it more difficult to investigate effect-modifiers such as patient age or appliance type. The heterogeneity of the study draws attention to differences in populations, interventions, and study designs. Subgroup-specific results or patient data should be reported in future research. The cost, which is frequently overlooked in research, is much greater than that of traditional systems, which restricts accessibility in areas with limited resources. Additionally, treatment may be delayed due to the longer planning time, particularly with CAD/CAM-based approaches. Twenty-seven studies’ sample sizes and follow-up times varied, and bias was introduced by smaller cohorts and retrospective designs. For results to be generalizable, larger, carefully planned trials are required.
Clinical Recommendations
Given their potential to reduce treatment duration and offer digitally guided precision, customized PEAs may be particularly suited for adult patients prioritizing aesthetics and efficiency. Although no significant differences were observed in ABO-DI and ABO-CR scores, customized systems can be advantageous in managing complex malocclusions requiring individualized mechanics. Long-term treatment success, however, depends on robust retention protocols and ongoing relapse surveillance. Strategic integration into clinical practice should be guided by case selection and tailored treatment planning.
Conclusions
Customized fixed orthodontic appliances may offer improved treatment efficiency, particularly in reducing overall treatment duration. However, these potential benefits were not consistently accompanied by improvements in treatment quality as measured by ABO indices. Significant heterogeneity across studies limits the strength of pooled conclusions, and the certainty of evidence remains low to moderate. Customization should therefore be considered a potentially valuable adjunct in appropriate cases, but not yet a replacement for sound biomechanical planning and clinical execution. Further well-designed, adequately powered randomized trials are needed to confirm these findings and guide routine clinical use.
Footnotes
Availability of Supporting Data
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A: PICOS (Participants,Intervention,Comparison,Outcomes,Study Design) Framework for Eligibility Criteria
Appendix B: Search Strategy for Electronic Databases
Appendix C: Sensitivity Analysis
Appendix D: Subgroup Analysis
Qualitative Subgroup Analysis
By appliance type (lingual vs. labial; customized vs. conventional) Treatment duration: Lingual customized (e.g., Ata-Ali 2020 Incognito™) showed longer mean treatment duration (~2.78 years) than labial conventional (Ata-Ali Labial group) (~2.43 years). This aligns with Figure 4a showing Ata-Ali 2020 with a positive mean difference favoring conventional PEA in treatment duration. Other studies using labial customized appliances (Penning et al.; Brown et al.; Jackers et al.; Weber et al.; Hegele et al.) mostly show shorter treatment durations compared to their conventional counterparts. For example, from Penning et al.,
31
there is a modest difference where treatment durations are similar but slightly longer in the customized group (1.29 vs. 1.24 years, respectively). Weber et al.
7
and Jackers et al.
29
report significantly shorter treatment durations with customized labial appliances (14.23 vs. 22.91 months, 393 vs. 497 days). Summary: Labial customized appliances tend to reduce treatment time relative to conventional labial appliances, while lingual systems tend to have longer or similar durations. ABO-DI and ABO-CRE scores: Ata-Ali’s data show slightly lower ABO-CRE and ABO-DI scores with lingual customized appliances (Incognito) relative to labial conventional (Victory), but differences are small and statistically uncertain. Penning et al. showed comparable orthodontic outcome quality (PAR reduction) between customized and conventional groups. Hegele et al. report median ABO score reductions of 32 points in both customized and conventional groups, indicating similar finishing quality. Jackers et al. also show similar ABO-CRE scores between CAD/CAM customized and conventional brackets. Summary: The finishing quality, as measured by ABO-DI and ABO-CRE, does not display consistent or significant differences between customized and conventional brackets, regardless of appliance type. Subgroup impact on other outcomes: Higher bracket failure rates in customized groups are noted in Penning et al. and Hegele et al. Patient complaints are consistently higher with customized appliances (Penning et al.). Oral comfort and speech disturbance were worse with customized lingual appliances (Wu et al.). Treatment planning time is longer with customized systems (Penning et al.; Yassir et al. review).
Subgroup analysis conclusion:
Customized appliance effects differ by appliance type and outcome. Labial customized appliances tend to shorten treatment duration, but lingual customized appliances do not consistently show this benefit. Clinical finishing outcomes are comparable across groups. Side effects like bracket failures, treatment planning time, and patient complaints tend to be greater with customized systems, especially lingual. These subgroup patterns should be interpreted cautiously, pending formal meta-analysis and individual patient data.