
Abstract
Introduction
The positional development of the mandibular third molars is influenced by orthodontic treatment mechanics and space availability. The impact of first premolar extractions on third molar angulation remains a subject of clinical interest, particularly in assessing whether the mesial movement of the buccal segment creates a favorable eruption pathway.
Objective
This retrospective study aimed to evaluate the effect of first premolar extractions on the angular and linear positional changes of the developing mandibular third molars following orthodontic treatment with a preadjusted edgewise appliance (PEA) [McLaughlin, Bennett, and Trevisi (MBT) prescription].
Methodology
Pre-treatment (T1) and post-treatment (T2) orthopantomographs of 60 patients were analyzed, with 30 patients undergoing first premolar extractions, and 30 were treated with a non-extraction approach. Changes in mandibular third molar angulation and space availability were assessed. A paired t-test was used for intra-group comparisons, while an unpaired t-test was employed for inter-group analysis.
Results
The extraction group exhibited a statistically significant improvement in third molar angulation, with a mean change of 6.3° in the right quadrant and 8.9° in the left quadrant (P < .05). In contrast, the non-extraction group demonstrated minimal angular changes, with a mean deterioration of −2.6° on the right and a non-significant mean increase of 1.7° on the left. Greater space availability was noted in the extraction group compared to the non-extraction group.
Conclusion
Premolar extractions in preadolescent orthodontic patients facilitate the mesial migration of the mandibular buccal segment, contributing to improved third molar angulation. This favorable positional change may enhance the likelihood of third molar eruption in an acceptable alignment, underscoring the potential benefits of extraction therapy in orthodontic treatment planning.
Keywords
Introduction
Third molar fate is often unpredictable because the usual 12-year-old orthodontic patient’s second molars may not have erupted yet, and the third molars would only have a little degree of calcification at this point. As orthodontic treatment initiation around this age is considered ideal, it is important to evaluate how the third molars are developing before formulating an orthodontic treatment plan. 1 Developing third molars continually change their angular positions and undergo important pre-eruptive rotational movements. They begin with a mesioangular orientation, progress to an upright position, and may finally even result in a distoangular inclination.2–4 These rotating movements occur when the bud of the third molar approaches the bud of the second molar. Richardson discovered that between the ages of 10 and 15, the mandibular third molar changes by an average of 11.2° (range: 20–42.5°) in relation to the mandibular plane. 5 This suggested a propensity for the teeth to straighten out. Impactions are unavoidable if these rotational movements do not take place, which makes them crucial. Thus, it would be helpful to understand how the development of lower third molars is affected by the extraction or non-extraction of the mandibular first premolars, followed by fixed appliance therapy. 6
There is a good chance that appliance therapy actively tips the mandibular molars distally or restricts them, which promotes aberrant rotational movements of the third molar crown and raises the risk of impaction. However, the development of third molars may undergo advantageous mesial movement and uprighting rotational modifications as a result of premolar extraction, thereby increasing the possibility of eruption. In order to allow for the mesial drift of the buccal segment, extraction of premolars has been the subject of many investigations.7–10
The current study aims to ascertain whether a more mesial movement of the mandibular buccal segment occurs after the extraction of the first premolars, and whether this will result in a positive positional change of the mandibular third molar. The mandibular third molars’ linear and angular alterations in relation to a reference plane and the second molar long axis are assessed in this study. The outcomes will also be compared between patients who had non-extraction treatment and those who had their first premolars extracted.
Material and Methods
A power analysis was performed to determine the minimum required sample size for detecting significant differences between groups. Based on 80% confidence level, a standard deviation of 0.2 mm, and a margin of error of 0.17 mm, it was calculated that a minimum of 60 sets (around 31–32 per group) of pre-treatment (T1) and post-treatment (T2) panoramic radiographs of individuals would be required to achieve sufficient statistical power. The study included patients aged 13–16 years (females) and 15–18 years (males) at the start of treatment.
Group I comprised 30 patients (15 males and 15 females) with a mean age of 15.96 ± 3.54 years who underwent extraction of all first premolars and were treated over a period of 24 ± 2 months. Group II consisted of 30 patients (15 males and 15 females) with a mean age of 16.66 ± 3.25 years, who were treated without extractions for a duration of 18 ± 2 months.
The study included growing subjects with an average growth pattern and a Class I skeletal relationship at the start of treatment. All participants had a Class I dental malocclusion on Class I skeletal bases at T1 and received treatment with preadjusted edgewise appliance (PEA) therapy using a 0.022” McLaughlin, Bennett, and Trevisi (MBT) prescription. Patients with an arch length discrepancy of more than 5 mm were treated with extractions, while those with less than 5 mm were treated without extractions, according to Carey’s analysis and individual treatment needs. Extraction cases exhibited complete closure of extraction spaces at the end of treatment and followed Type B anchorage planning. Only cases presenting with bilaterally unerupted mandibular third molars in a mesioangular position with no more than two-thirds root development at T1 were included. Panoramic radiographs at both T1 and T2 were required to be of acceptable and standardized quality.
Exclusion criteria included severely malpositioned third molars, cases where the molar profile could not be reliably traced on lateral cephalograms, and subjects with dentofacial deformities, mandibular pathologies, developmental anomalies, image distortions, or unusual magnifications.
Method of Measurement
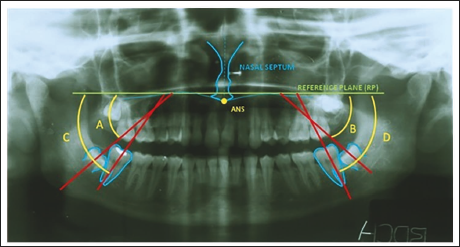
Angular Evaluation (Figure 1)
Horizontal reference plane (HRP) was established by bisecting the traced nasal septum and anterior nasal spine (ANS), followed by constructing a perpendicular bisector extending through the palatal shadow. The long axes of the mandibular second and third molars were defined as lines passing through the mid-occlusal point to the midpoint of the root bifurcation. The angles formed by the third molar axes with the HRP on the right (angle A) and left (angle B) sides were measured. Similarly, the angles formed by the second molar axes with the HRP on the right (angle C) and left (angle D) sides were recorded.
Dental Angular Parameters.
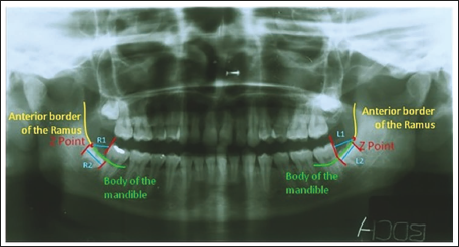
Linear Evaluation (Figure 2)
The Z point was defined as the junction of the anterior border of the ramus and the mandibular body, constructed as the bisector of the angle formed by the tangent to the anterior border of the ramus and the tangent to the superior surface of the mandibular body. The linear distance from the Z point to the distal aspect of the second molar crown at its maximum curvature was measured (R1 on the right and L1 on the left). The mesiodistal widths of the mandibular third molar crowns at their maximum curvature were also measured (R2 on the right and L2 on the left).
Dental Linear Parameters.
Evaluation of Methodological Error
To assess inter-observer variation in landmark identification and analysis, 10 randomly selected tracings were re-evaluated after 1 month. Agreement between the initial and repeated measurements was assessed using kappa statistics, yielding an agreement rate exceeding 90%.
Statistical Analysis
The Shapiro–Wilk test was used to assess if the data distribution was normal. As the data followed a normal distribution, parametric tests were used for comparisons. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) for Windows, Version 17.0 (Chicago, SPSS Inc.). Intragroup comparisons of pre-treatment and post-treatment values were conducted using the paired t-test, while intergroup comparisons were performed using the unpaired t-test.
Result
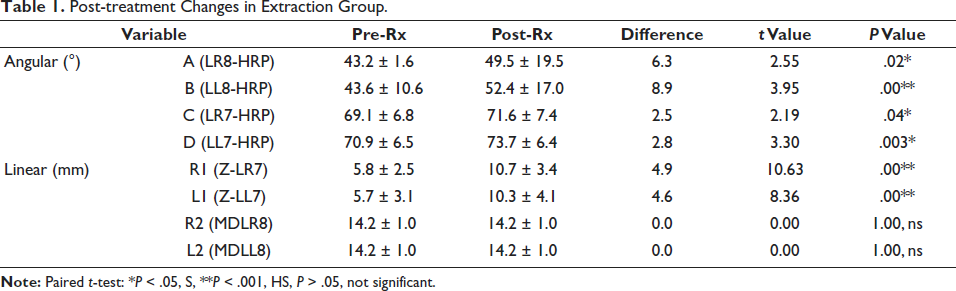
In the extraction group, significant angular and linear changes were observed. The third molars (LR8-HRP and LL8-HRP) exhibited notable increases in angulation (6.3° and 8.9°, respectively), with statistically significant differences (P < .05). The second molars (LR7-HRP and LL7-HRP) also showed mild but significant angular increases (2.5° and 2.8°, respectively). These changes suggest that the removal of teeth allowed for mesial drifting and uprighting of the posterior teeth.
Linear measurements revealed substantial forward movement of the second molars, as R1 (Z-LR7) and L1 (Z-LL7) increased by 4.9 and 4.6 mm, respectively (P = .00**), indicating a mesial shift. However, the mesiodistal widths of the third molars (MDLR8 and MDLL8) remained unchanged (P = 1.00, ns), suggesting that extraction did not impact tooth size (Table 1).
Post-treatment Changes in Extraction Group.
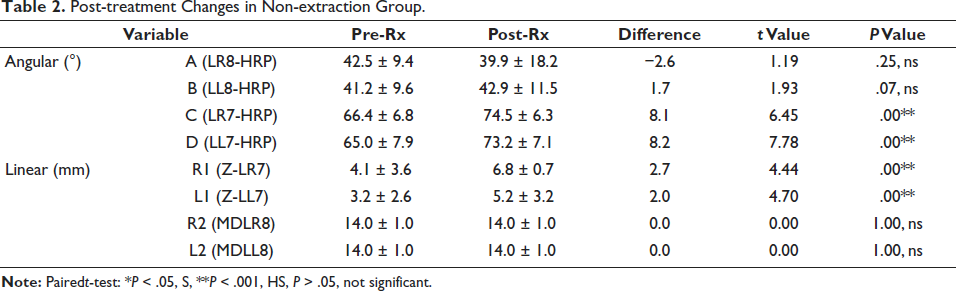
In contrast, the non-extraction group displayed different patterns of change. The third molars (LR8-HRP and LL8-HRP) exhibited minor or non-significant angular shifts, with LR8-HRP even showing a slight negative angulation (−2.6°), though not statistically significant (P = .25, ns). Meanwhile, the second molars (LR7-HRP and LL7-HRP) underwent greater angular increases (8.1° and 8.2°, respectively, P = .00**), indicating significant repositioning of these teeth.
Linear movements in the non-extraction group were also observed, but they were less pronounced than in the extraction group. R1 (Z-LR7) and L1 (Z-LL7) increased by 2.7 and 2.0 mm, respectively, showing significant movement (P = .00**), though to a lesser extent than in the extraction group. Similar to the extraction group, the third molars remained unchanged in their mesiodistal widths (P = 1.00, ns) (Table 2).
Post-treatment Changes in Non-extraction Group.
When comparing post-treatment changes between the extraction and non-extraction groups, statistically significant differences emerged. The third molars in the extraction group experienced greater angulation changes than those in the non-extraction group (6.3° vs. −2.6° for LR8-HRP and 8.8° vs. 1.7° for LL8-HRP), suggesting that extractions facilitated distal tipping of these teeth. Similarly, second molars in the extraction group underwent less angular change than those in the non-extraction group (2.5° vs. 8.1° for LR7-HRP and 2.8° vs. 8.2° for LL7-HRP), implying that the absence of extractions necessitated greater second molar repositioning to achieve alignment (Table 3).
Comparison of Post-treatment Changes Between Extraction and Non-extraction Groups.
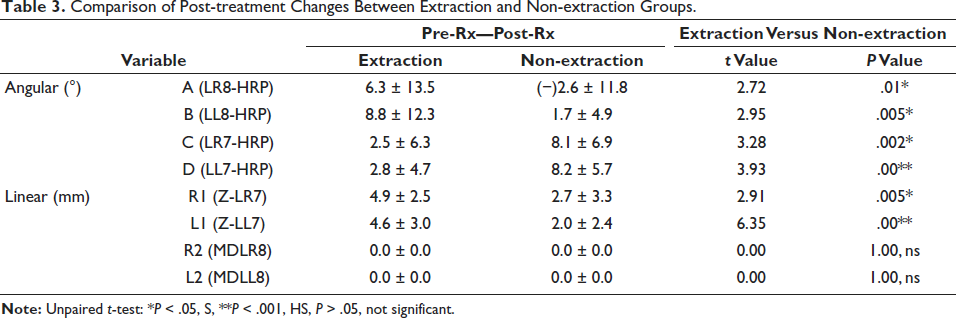
In terms of linear movement, the extraction group showed significantly greater mesial shifts of the second molars compared to the non-extraction group (4.9 vs. 2.7 mm for Z-LR7 and 4.6 vs. 2.0 mm for Z-LL7). These findings indicate that extractions create space for the second molars to migrate forward more freely, whereas in non-extraction cases, movement is more restricted.
Discussion
Impacted third molars present a significant clinical concern due to their high prevalence of impaction, primarily attributed to an inadequate dental arch space for eruption. The early prediction of their eruptive path is crucial for anticipating potential impaction.8, 9 This study evaluated subjects aged 13–18 years, with a mean age of 15.6 years in the extraction group and 16.2 years in the non-extraction group. This period marks a critical phase in which third molars undergo significant pre-eruptive movements. The chosen age range was ideal for assessing the impact of extraction versus non-extraction treatment modalities on the positional and angular pre-eruptive changes influencing third molar eruption. 5
Lateral cephalograms have been widely used in previous studies for third molar evaluation.6–8 However, superimposition-related biases have been reported. Richardson suggested that using 60° head films could mitigate these issues.11, 12 Panoramic radiographs, known for their accuracy in assessing mandibular third molar space and linear dimensions, were therefore utilized in this study.13, 14
Various reference planes, including the occlusal plane and the mandibular plane, have been employed in third molar angulation assessments. However, treatment-induced changes in the occlusal plane and mandibular border remodeling may lead to misinterpretation. The palatal plane, deemed more stable during growth and orthodontic treatment, was thus selected as a reference. Given the relatively short treatment period (approximately 2 years) and the absence of complex mechanics capable of altering the palatal plane, the study design ensured reliable measurements. 15
The availability of space for third molar eruption is influenced by multiple factors, including bone resorption at the anterior border of the ramus, the slope of the anterior ramus relative to the alveolar border, dentition movement, mandibular growth, and third molar morphology. Early prediction methods assessed third molar eruption potential based on the space between the Xi point and the distal second molar. The critical eruption threshold was identified as 25 mm. However, Richardson observed that the available space distal to the second molar does not guarantee its eruption. Studies further indicate that the retromolar space-to-third molar width ratio remains relatively unchanged in impacted cases, while it increases in erupted cases between ages 13 and 20.11–13 Consequently, the present study assessed the available space using panoramic radiographs to evaluate the influence of orthodontic treatment.
Impact of Extraction Treatment
A significant improvement in third molar angulation was observed following premolar extractions, with a mean uprighting of 6.3° on the right and 8.8° on the left. These findings align with previous studies that reported improved third molar angulation post-extraction. The study by Elsey and Rock, utilizing the mid-sagittal reference plane on panoramic radiographs, demonstrated a mean improvement of 7°. However, their study lacked a comparative evaluation of the right versus left sides and a non-extraction control group. 7 Contradicting these findings, McCoy suggested that premolar extractions may not enhance third molar eruption. 16
Linear assessments indicated a highly significant increase in space for third molar eruption—4.9 mm on the right and 4.6 mm on the left—following extractions. These changes may be attributed to the mesial migration of the buccal segment after space closure, allowing greater pre-eruptive third molar movement. Additionally, retromolar area growth may have contributed, as previously confirmed by Capelli. 6
Impact of Non-extraction Treatment
In contrast, third molar angulation exhibited minimal changes in the non-extraction group. A slight worsening of −2.6° was noted on the right, while the left side showed a minor improvement of 1.7°, neither of which was statistically significant. These findings may be attributed to the maintenance of molar positioning, although individual variations in angulation changes were observed. The results corroborate previous studies by Saysel et al., which reported worsening third molar angulations in non-extraction cases. 17 Additionally, Richardson noted that improvements in third molar space were significantly lower in non-extraction cases. 11 Silling proposed that non-extraction therapy, by distalizing or tipping the mandibular molars, may increase the risk of third molar impaction. 3 The minimal improvements observed may be attributed to natural growth and remodeling of the retromolar area.
Comparison of Extraction Versus Non-extraction Treatment
Consistent with previous research, the present study confirms that extraction treatment provides greater improvements in third molar angulation and space availability than non-extraction treatment.18–20 This contrasts with findings by Mang de la Rosa et al., who reported that premolar extractions did not significantly enhance third molar angulation compared to non-extraction therapy. 21 However, their study suggested that third molar angulation improved regardless of the treatment approach. 22 The present study demonstrated significant uprighting of second molars, likely attributed to leveling and alignment mechanics, facilitating improved occlusal interdigitation and space maintenance.
Although the projection of mandibular third molars in panoramic radiographs varies depending on the tooth position, mesiodistal width measurements in both groups remained constant, supporting the reliability of panoramic radiographs for diagnostic purposes. Notably, space availability in the extraction group increased by 4.9 mm on the right and 4.6 mm on the left, compared to minimal changes of 2.7 and 2 mm, respectively, in the non-extraction group. These results reinforce the utility of panoramic radiographs for evaluating the third molar eruption potential.
Clinical Implications
Premolar extractions in adolescent orthodontic patients facilitate mesial migration and improve third molar positioning, increasing the likelihood of favorable eruption. Although it remains uncertain how many third molars will fully erupt, improved angulations may ease future surgical interventions, when necessary. These findings underscore the need for third molar evaluation in borderline extraction cases. When third molar angulations are unfavorable but eruption potential remains high, premolar extractions may be beneficial in optimizing third molar alignment. Given the late development of third molars, orthodontists should carefully assess their positioning when planning treatment to optimize long-term outcomes.
Conclusion
The findings of this retrospective radiographic study underscore the influence of first premolar extraction on the angular and spatial development of mandibular third molars following orthodontic treatment with PEA therapy. Patients who underwent premolar extractions demonstrated a statistically significant improvement in the angulation of third molars, particularly in both the right and left mandibular quadrants, suggesting that the mesial migration of the posterior segment created a more favorable path for third molar eruption. Conversely, the non-extraction group exhibited minimal or even unfavorable angular changes, highlighting the restrictive nature of space in non-extraction mechanics.
Furthermore, the extraction group showed a clear increase in space availability in the posterior region, which likely contributed to the improved third molar positioning. These results suggest that premolar extractions not only address crowding and malocclusion correction but may also indirectly facilitate the spontaneous alignment and eruption potential of mandibular third molars. Clinicians should therefore consider the long-term implications on third molar development when formulating treatment plans, especially in younger patients in whom third molar positioning is still dynamic. Overall, extraction therapy—when appropriately indicated—can be a strategic decision in promoting a favorable third molar orientation and reducing the risk of future impaction.
Authors Contribution
Chris L. Saldanha: Conceptualization, data curation, methodology, and investigation.
Kiran Kumar H.C.: Supervision and original first draft.
Vishnupriya T.R.: Validation, visualization, formal analysis, and software.
Poorva Pravin Attarde: Resources.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to undertake the study was gained from institutional review board, Bapuji Dental College and Hospital dated on 22/02/2011.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has provided informed consent for the submission of the article to the journal.