
Abstract
Objective
The study aims to comprehensively assess skeletal, dentoalveolar, condylar, and soft tissue adaptations following treatment with the Class II corrector appliance in growing individuals diagnosed with Class II Division 1 malocclusion using cephalometric and pitchfork analyses.
Materials and Methods
The study was carried out as a prospective clinical study on 14 growing patients (mean age: 12.6 ± 1.8 years) diagnosed with skeletal Class II Division 1 malocclusion, with treatment outcomes assessed using lateral cephalograms following functional appliance therapy. Cephalometric analysis was used to evaluate skeletal, dentoalveolar, condylar, and soft tissue adaptations. The assessment focused on variations in the skeletal base relationship, maxillomandibular lengths, and facial forms. Pitchfork analysis was used to determine molar correction and overjet reduction percentages attributable to skeletal versus dentoalveolar changes. A Wilcoxon signed-rank test was used to analyze pre-treatment (T1) and post-treatment (T2) cephalometric values, with p value <.05 was set as significant.
Results
Treatment with Class II corrector provides ANB angle with mean reduction of 1.9° and Wits appraisal with mean of −1.0 mm, indicating skeletal correction. Mandibular advancement was evident with an increase in Pg/OLp by 3.41 mm. Retroclined maxillary incisors and proclined mandibular incisors were also noted. The nasolabial angle increased (mean: 5.2°), and facial convexity was reduced significantly. Pitchfork analysis revealed that 48% of molar correction was skeletal and 52% dentoalveolar. Condylar head remodeling and anterior glenoid fossa remodeling contributed to mandibular advancement.
Conclusion
The Class II corrector (Leone Inc.) appliance produced significant skeletal, dentoalveolar, and soft tissue changes in growing individuals with Class II Division 1 malocclusion, with skeletal effects accounting for nearly half of the treatment changes. It presents a reliable alternative for noncompliant patients.
Keywords
Introduction
Successful orthodontic treatment hinges significantly on patient compliance. However, achieving consistent cooperation—especially among adolescent patients—remains an enduring challenge in clinical orthodontics. Noncompliance has been recognized as a limiting factor for over four decades, with numerous studies highlighting its potential to compromise treatment outcomes.1, 2 Although clinicians and patients alike often anticipate high levels of cooperation, these expectations are frequently overestimated. This has prompted increasing interest in treatment modalities that reduce the dependency on patient participation.
Functional appliances are routinely used in growth modification therapy to correct jaw discrepancies, particularly in growing individuals presenting with skeletal Class II malocclusion. These appliances may be either removable or fixed. Fixed functional appliances (FFAs) offer a distinct advantage by functioning independently of patient compliance, thereby improving the predictability and efficiency of treatment. 3 They are often referred to as “noncompliance Class II correctors” and have undergone significant evolution over the years, resulting in the development of numerous designs tailored to maximize skeletal and dentoalveolar correction with minimal reliance on patient cooperation. 4
Class II malocclusion, frequently due to a retrusive mandible, is one of the most commonly encountered orthodontic problems in growing individuals. 5 Functional orthopedic intervention has long been advocated for its potential to harness the patient’s growth phase to effect favorable skeletal changes. 6 Functional appliances (removable), like Twin Block, Bionator, and Activator, have been widely used, but they often depend heavily on patient compliance. 7 This drawback is largely circumvented by functional appliances (fixed), like Herbst, Jasper Jumper, Forsus, and the more recent Class II Corrector from Leone Inc.8–10
Recent systematic reviews comparing functional appliances (removable and fixed) demonstrated that FFAs are capable of producing modest but clinically significant skeletal changes.11, 12 Among various fixed appliances, the Class II Corrector by Leone Inc. has emerged as a promising option. However, despite increasing clinical adoption, comprehensive data evaluating its effects remain limited. Due to the growing adoption of the Class II Corrector in orthodontic practice and the absence of dedicated studies assessing its outcomes, it becomes imperative to systematically evaluate its influence on skeletal, dentoalveolar, and soft tissue parameters. This study aims to address this gap by evaluating the treatment effects of the Class II Corrector (Leone Inc.) in growing individuals with skeletal Class II Division 1 malocclusion primarily caused by mandibular retrognathism.
Materials and Methods
The study, designed as a prospective interventional trial, was conducted in the Department of Orthodontics and Dentofacial Orthopaedics with approval from the Ethics Review Board. Sample size estimation was performed using G*Power version 3.1.9.4 and determined a sample size of 5, with a statistical power of 80% and a permissible alpha error of 5%. Considering the possibility of potential dropouts during the study and inter-individual variability, 14 patients were initially recruited. A total of 14 growing patients (ages 12-16 years), diagnosed with skeletal Class II Division 1 malocclusion caused by retrognathic mandible, were selected through random sampling.
The inclusion criteria were: Skeletal Class II Division 1 malocclusion and a convex profile; Orthognathic maxilla (SNA = 82° ± 2°); Retrognathic mandible (SNB = 74°-77°); Overjet ≤8 mm; Positive visual treatment objective (VTO); Well-aligned arches or minimal anterior crowding; Patients in active growth phase (CVMI stage III or IV); Horizontal or average growth pattern.
The exclusion criteria were: Patients with prognathic maxilla; Severe anterior crowding; Requirement of extractions as part of treatment; Neuromuscular or systemic disorders; History of trauma or temporomandibular joint (TMJ) disorders.
Routine orthodontic records, including extraoral and intraoral photographs, lateral cephalograms, and study models, were taken. Informed consent was collected from all patients and/or their guardians. All patients were initially bonded with 0.022″ MBT-prescription brackets. Leveling and aligning were completed using a sequence of archwires up to 0.019″ × 0.025″ SS archwires. Pre-functional treatment records (T1), including cephalograms, photographs, and study models, were obtained. The appropriate size of the Leone Class II Corrector was selected according to the manufacturer’s guidelines. The appliance, comprising bilateral push rods and spring modules, was installed as per manufacturer’s instructions. Figure 1 shows an intraoral photograph of the patient with the appliance. Patients were reviewed biweekly for the first month and monthly thereafter. Molar relationship was monitored at each visit. Upon achieving Angle’s Class I molar relationship, the appliances were removed, and post-treatment records (T2) were obtained. Cephalometric tracings were manually performed by a single calibrated examiner to eliminate inter-examiner bias. Data from T1 and T2 were statistically analyzed to assess skeletal, dentoalveolar, condylar, and soft tissue changes.
Intraoral Photograph of Patient with the Appliance.

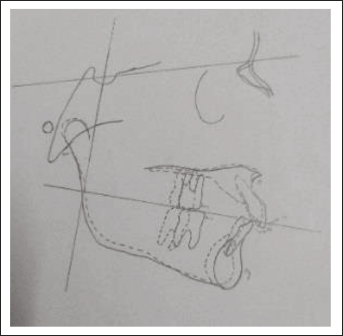
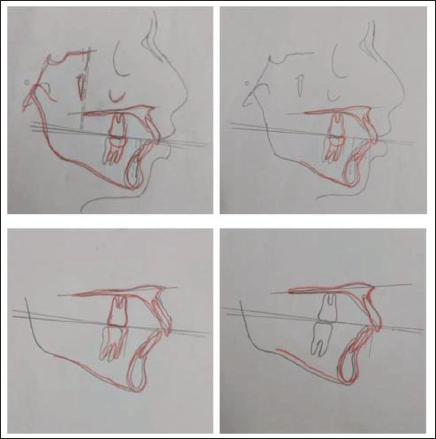
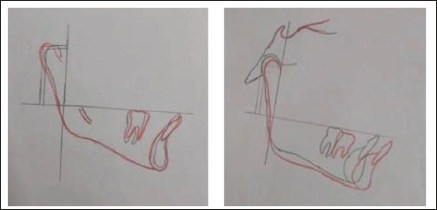
Three cephalometric analyses were employed: sagittal occlusal (SO) analysis (Pancherz) (Figure 2) to assess sagittal skeletal and dental movements; pitchfork analysis (Figure 3) to quantify the skeletal and dental changes involved in molar and overjet reduction; Buschang and Santos Pinto Analysis (Figure 4) to assess condylar and glenoid fossa positional changes. In addition, conventional angular measurements, including SNA, SNB, and ANB, were assessed. Vertical skeletal changes were analyzed using ANS–Me measurements.
Sagittal Occlusal (SO) Analysis (Pancherz).
Pitchfork Analysis.
Buschang and Santos Pinto Analysis.
Statistical Analysis
The collected data were processed and analyzed using SPSS software (version 23.0; IBM Corp., Armonk, NY, USA). Comparisons between pre-treatment (T1) and post-treatment (T2) cephalometric parameters were performed using the Wilcoxon signed-rank test. Statistical significance was set at a p value of less than .05.
Results
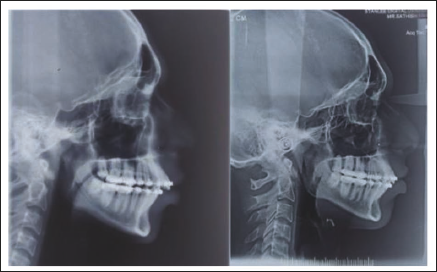
A total of 14 male patients were initially recruited for the study. However, 4 patients were lost to follow-up, resulting in a final sample of 10 participants. Pre-treatment (T1) and post-treatment (T2) cephalometric values were analyzed (Figure 5).
Pre-treatment and Post-treatment Cephalograph of the Patient.
Skeletal Effects
Significant skeletal changes were noted in the mandible following treatment (Table 1). Mandibular length (Pg/OLp) increased significantly from 66.2 mm to 69.7 mm (p = .024). Effective mandibular length (Pg/OLp + Ar/OLp) showed a statistically significant increase from 77.2 mm to 80.2 mm (mean increase of 3 mm; p = .041). SNB angle increased from 77.7° to 80.3° (p < .026), suggesting forward mandibular displacement. SNA angle and SS/OLp showed no statistically significant changes, indicating stability of the maxillary position.
Sagittal Occlusal (SO) Analysis Skeletal.
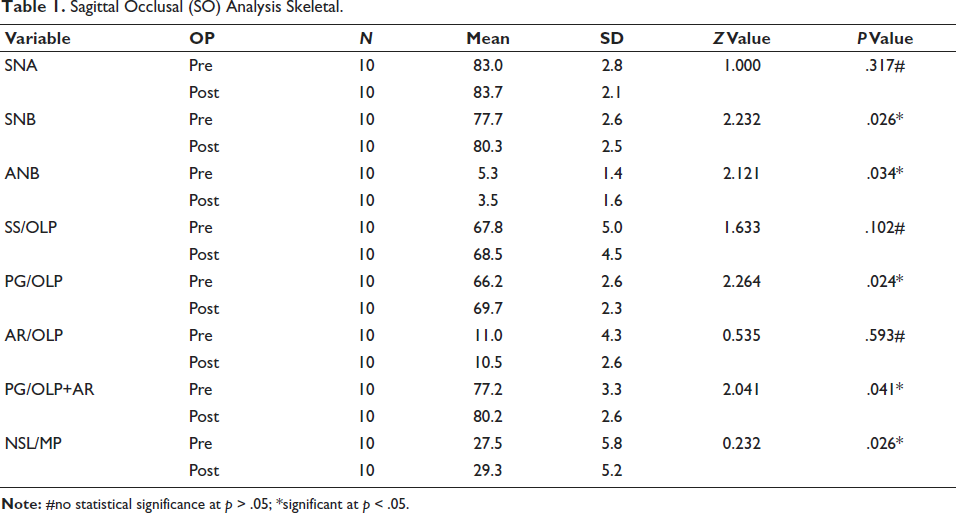
ANB angle decreased significantly by a mean of 2.3°, reflecting an improved maxillomandibular relationship. Vertical skeletal change (ANS–Menton) increased from 57.8 mm to 59.4 mm (p < .05), indicating vertical facial height increase. The mandibular plane angle rotated significantly in a clockwise direction from 27.5° to 29.3°.
Dental Effects
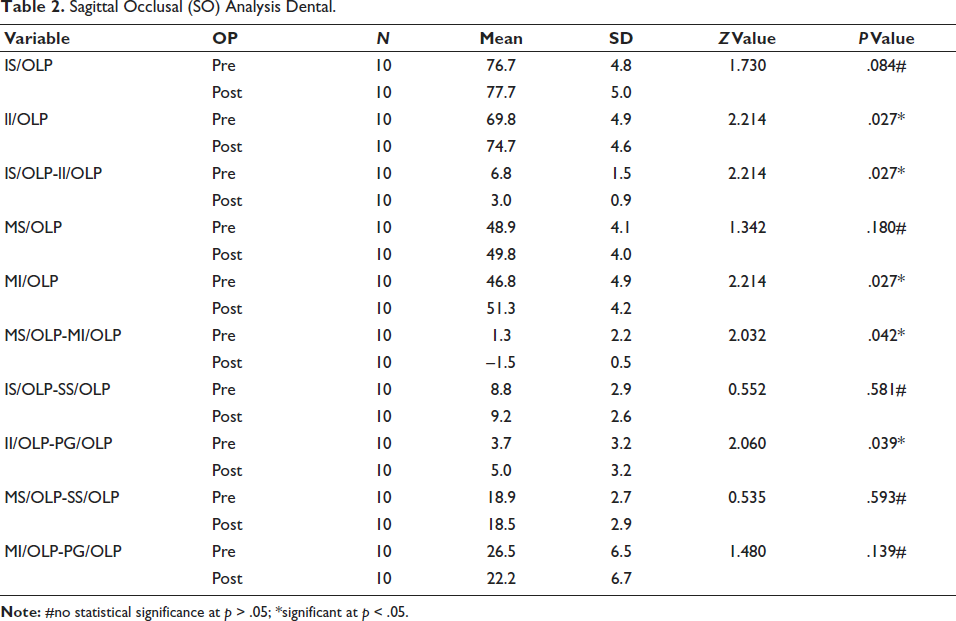
Significant dental changes contributed to Class II malocclusion correction (Table 2). Overjet reduced significantly from 6.8 mm to 3.0 mm (p < .027). Upper incisor position remained largely unchanged. Lower incisor proclination increased significantly, with Pg/OLp to ii/OLp changing from 3.6 mm to 5 mm. Lower molar (mi/OLp) moved mesially, with an average improvement of 4.5 mm in the molar relationship noted. The correction of Class II malocclusion involved both skeletal and dental contributions. The lower molar exhibited a significant mesial shift within the arch (p = .02), reflecting favorable dental movement.
Sagittal Occlusal (SO) Analysis Dental.
Soft Tissue Changes
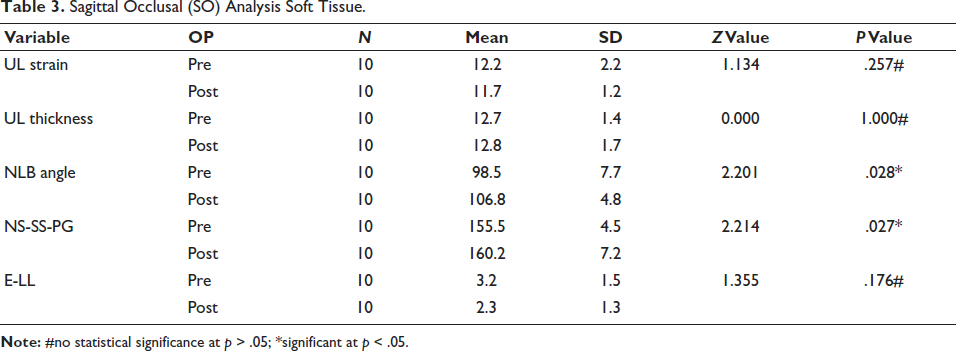
A reduction in upper-lip strain was observed, though it was not statistically significant. Nasolabial angle increased significantly from 98.5° to 106.8° (p = .028), indicating soft tissue improvement. Soft tissue convexity angle improved from 155.5° to 160.2° (p = .027) (Table 3), suggesting profile straightening. Lower-lip position relative to Ricketts’ E-plane did not show significant change.
Sagittal Occlusal (SO) Analysis Soft Tissue.
Condylar and Glenoid Fossa Changes
Glenoid fossa changes (Table 4) showed a mean shift of 0.5 mm, which was not statistically significant but favored Class II correction. Condyle position demonstrated significant changes in both sagittal and vertical directions (Table 5). Sagittal shift increased from 11.7 mm to 12.9 mm (mean = 1.2 mm); vertical shift increased from 33.7 mm to 34.8 mm (mean = 1 mm). These changes suggest forward and vertical growth of the condyle.
Glenoid Fossa Changes.

Condylar Changes.

Pitchfork Analysis
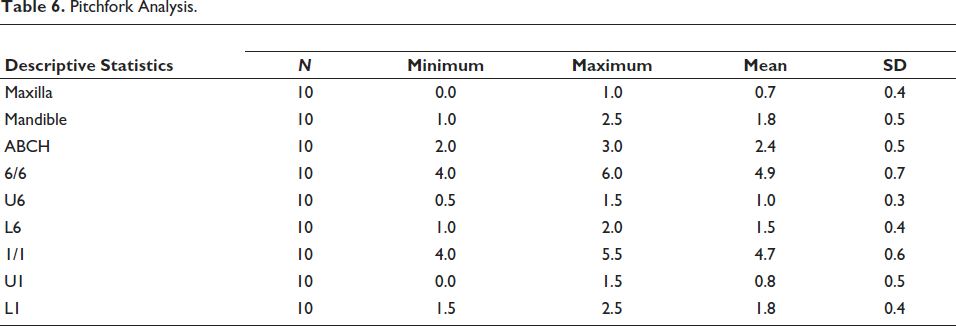
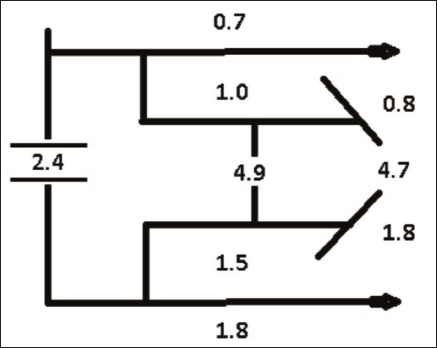
The classic pitchfork diagram illustrated the following mean treatment effects: maxillary growth (upper fork): 0.7 mm; mandibular sagittal skeletal change (lower fork): 1.8 mm; molar correction (total: 4.9 mm), comprised of 48% skeletal base change (ABCH) and backward movement of the upper molar, and 52% dental contribution. Overjet correction (4.7 mm) consisted of 51% skeletal contribution and 49% dental, including 1.8 mm of lower incisor proclination (Table 6, Figure 6).
Pitchfork Analysis.
Pitchfork Diagram.
Discussion
Functional jaw orthopedics remains a reliable approach for treating Class II malocclusions associated with retrognathic mandibles during active growth periods. Functional appliances (fixed and removable) have been employed for correcting skeletal discrepancies, with fixed appliances offering distinct advantages, including reduced dependency on patient compliance and a continuous bite-jumping mechanism.13, 14 In this study, the Class II Corrector (Leone Inc.), a modified Eureka Spring, was evaluated for its skeletal, dentoalveolar, condylar, and soft tissue effects in growing male patients.
The appliance’s design—comprising a spring module and a push rod—enabled uninterrupted force application and allowed lateral excursions during mandibular movement. 15 The manufacturer’s claims of increased comfort and patient mobility were clinically supported, as no appliance breakage, discomfort, or functional limitations were reported.
The study included 10 male subjects with skeletal Class II malocclusion characterized by normal maxilla and retrognathic mandible. The cephalometric evaluation was performed using Pancherz’s SO analysis. 16 Statistically significant mandibular skeletal changes were observed. Mandibular length (Pg/OLp) increased from 66.2 mm to 69.7 mm (p = .024), and effective mandibular length (Pg/OLp + Ar/OLp) increased by 3 mm (p = .041), indicating true mandibular growth. The SNB angle increased significantly (p < .026), supporting anterior mandibular repositioning. These findings are consistent with previous reports by Pancherz, 16 Franchi and Bacetti, 17 who demonstrated increase in mandibular length with other FFAs. Interestingly, no significant reduction of maxillary growth was noted, aligning with findings from Covell et al. 18 and Pancherz and Anehus-Pancherz, 19 who documented minimal or no maxillary restraint with fixed appliances.
Vertical facial changes were evaluated using ANS–Menton and mandibular plane angle measurements. A mean increase in lower anterior facial height of 1.6 mm and clockwise rotation of the mandibular plane (from 27.5° to 29.3°) were observed, consistent with vertical changes reported in similar studies.17, 18
Dental changes also contributed significantly to Class II correction. Overjet was reduced significantly from 6.8 mm to 3.0 mm (p < .027). The upper incisors remained relatively stable, while the lower incisors showed significant proclination (from 3.6 mm to 5 mm), partially accounting for the overjet reduction. Molar relationship improved by 4.5 mm, with mesial movement of lower molars. The magnitude of these dental movements is consistent with findings from Ruf and Pancherz, 20 as well as Ernest et al., 21 who reported dentoalveolar contributions to Class II correction.
The pitchfork analysis further delineated the nature of these corrections. Approximately 48% of molar correction and 51% of overjet correction were attributed to skeletal changes, with the remaining attributed to dental movements. These findings affirm that both skeletal and dental components synergistically contribute to successful Class II correction using fixed-functional appliances.
Soft tissue evaluation revealed favorable profile changes, including a significant increase in the nasolabial angle (from 98.5° to 106.8°, p = .028) and improved soft tissue convexity (from 155.5° to 160.2°, p = .027), resulting in a straighter facial profile. While upper lip strain was reduced, this change was not statistically significant. These soft tissue changes were comparable to those reported by Ruf and Pancherz. 22
Condylar remodeling and changes in glenoid fossa position were also observed. Although glenoid fossa changes were minimal and not statistically significant, condylar growth was evident in both sagittal and vertical directions, with a mean increase of 1.2 mm and 1 mm, respectively. This forward movement of the condyle supports the concept of true mandibular adaptation, though magnetic resonance imaging (MRI)-based studies have previously questioned the extent of condylar remodeling’s contribution to Class II correction. 23
Conclusion
The Class II Corrector appliance (Leone Inc.) demonstrated a favorable combination of skeletal, dentoalveolar, condylar, and soft tissue effects in the treatment of growing individuals with Class II Division 1 malocclusion and retrognathic mandible. Significant forward mandibular growth, overjet reduction, correction of molar relationship, and enhanced soft tissue profile were observed. The treatment results were achieved through both skeletal and dentoalveolar mechanisms, with nearly equal contributions from each.
The Class II Corrector appliance (Leone Inc.) effectively corrected skeletal Class II Division 1 malocclusions through combined skeletal and dental effects, leading to significant profile improvement and providing a dependable option in noncompliant patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval has been obtained from Institutional Ethics Committee.
Informed Consent
Not applicable.