
Abstract
We are in the process of discovery of new vistas for technological advances in terms of various appliances with a vision of making orthodontic treatment compliance free as well as successful. Due to improved technology, the enigma of treating the Class II syndrome is palliated. “Out of the box” thinking has become a norm to treat certain situations that were not corrected in noncompliant patients. Fixed functional appliances are valuable tools introduced to assist the correction of skeletal Class II malocclusion with mandibular retrognathia at the deceleration stage of growth for achieving stable results. In this direction a case series is reported of patients having the above conditions and undergoing orthodontic treatment using a Forsus FFA. Joining hands with technology is a win-win situation for both the patient and the orthodontist.
Keywords
Introduction
Over the last century, there have been many debates and controversies regarding the finest treatment modalities to accomplish skeletal Class II malocclusion in the orthodontic world. In that era, McNamara challenged the conventional wisdom and corroborated the salient characteristic of Class II malocclusion to be mandibular retrognathism rather than maxillary prognathism. 1
In contemporary orthodontics, there exist many appliances that are employed to maximize the residual growth in noncompliant skeletal Class II patients. These appliances are predominantly rigid, flexible, and hybrid. The evolution of fixed functional appliance (FFA) from its origination as a rigid appliance in the form of Herbst (Emil Herbst, 1905) to a flexible hybrid appliance like the Forsus Fatigue Resistant Device (FFRD; William Vogt, 2006) allows flexibility in the position of the mandible and better compliance, as it permits a greater range of mandibular movements.
In 2006, William Vogt published an article in Journal of Clinical Orthodontics introducing the FFRD, which is marketed by 3M Unitek for clinical use, designed as an interarch push spring device that produces about 200 g of force when fully compressed. 2
The distal end of the FFRD’s push rod is inserted into the telescopic cylinders, and a hook on the mesial end is crimped directly to the arch wire near the canine or the premolar brackets. The telescopic cylinders consist of inner and outer sliding tubes surrounded by an open coil spring. An eyelet at the distal end of the cylinders is connected to the maxillary molar headgear tube with L pin Module or EZ2 Module (Figure 1). 2
Spring Modules22

The sole purpose of preferring an FFA over any other treatment modality was to improve the soft tissue profile. This was further emphasized as both the patients led a positive visual treatment objective (VTO), and extraction if carried out to reduce the overjet would have given the patient a flat profile. 3 The ideal means of correction is to target the source and try to alter the amount or direction of growth in that jaw.
We exhibit the following cases to expound the expediency of the FFRD in skeletal Class II patients reported during the residual growth stages of puberty.
Case Series
Two patients, one female and the other male, aged 15 and 17 years, respectively, presented with the chief compliant of irregularity of upper front teeth and no significant past medical and dental history.
Extraoral Examination
Extraoral examination of both the patients exhibited a convex profile, retruded chin, deep mentolabial sulcus, competent lips, and full incisor exposure while smiling. There was no facial asymmetry, and the male patient had a significant difference in clinical Frankfort–mandibular plane angle (FMA). No significant symptom of temporomandibular joint (TMJ) dysfunction was present (Figures 2 and 12).
Pre-treatment Photographs

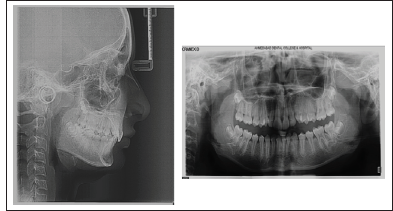
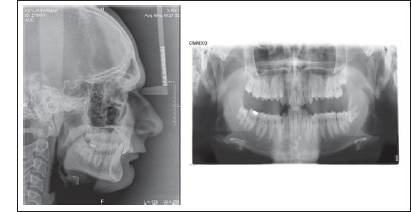
Pre-Treatment Radiographs
SMI Stages FISHMAN STAGE 6 – Capping of Epiphysis (third finger and middle phalanx). JULIAN SINGER STAGE 4 – PUBERTAL, calcified ulnar sesamoid. Mp3 capping (capping of shaft of middle phalanx of 3rd digit by its epiphysis)

Initial levelling and Alignment

FORSUS – Fixed Functional Appliance

Post FORSUS Fixed Functional Appliance

Post Treatment Photographs

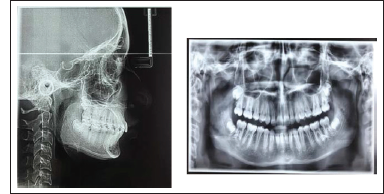
Post Treatment Radiographs
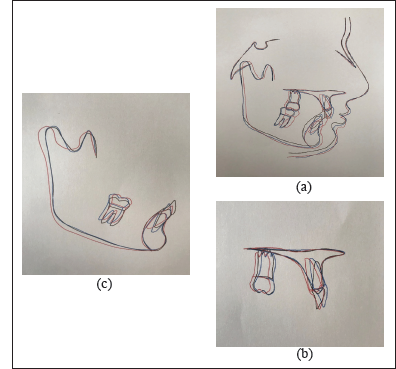
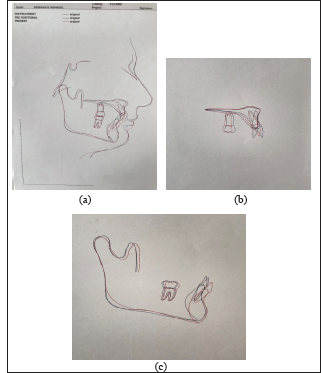
Superimposition Tracing Where Blue Line – Pretreatment, Black Line – Pre-Functional, Red Line – Post Treatment
Follow Up photographs taken after 4 years of debonding

Pre-treatment Photographs

Intraoral Examination
Upon intraoral examination, the cases revealed Class II molar and Class II canine on the right and left side, along with Class II Division 2 incisor relationship. The patients had a square-shaped maxillary and U-shaped mandibular arch. Crowding was present in the anterior region. Maxillary and mandibular midlines were coinciding. An overjet of 2 mm and overbite of 5 mm was present in the female patient, whereas the male patient presented with an overjet of 1 mm and overbite of 8 mm (Figures 2 and 12).
Radiographic Examination
The panoramic radiograph of both the patients showed the presence of all permanent teeth. The molar buds of all four third molars were seen in the female patient (Figure 3). No third molar of the male patient had erupted (Figure 13).
Pre-treatment Radiographs
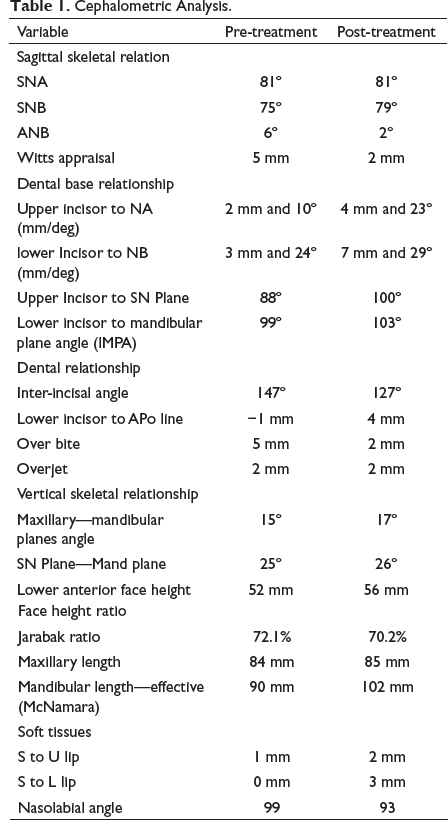
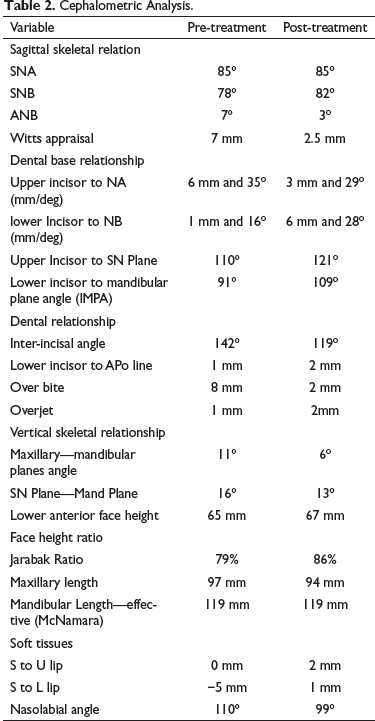
Cephalometric Analysis
Cephalometric Analysis.
Cephalometric Analysis.
Diagnosis
The patients were diagnosed with Angle’s Class II malocclusion superimposed on Class II skeletal jaw bases with orthognathic maxilla in the female patient and prognathic maxilla in the male patient. Both the patients exhibited a retrognathic mandible with accompanying Class II molar and Class II canine relationship on the right and left side, along with a Class II Division 2 incisor relationship with retroclined upper and lower incisors, competent lips, and deep mentolabial sulcus.
Treatment Objectives
To achieve Class I skeletal jaw bases.
To achieve Class I molar and Class I canine relation.
To achieve ideal overjet and overbite.
To correct crowding and individual tooth rotations.
To level the Curve of Spee.
Treatment Progress
The cases were started with 0.022 MBT fixed appliance therapy. A protraction utility arch (0.016″ × 0.016″) was introduced in the maxillary arch in the male patient (Figure 14). Alignment of the cases was started with a 0.014″ round nickel–titanium arch wire (NiTi), followed by a 0.016″ round NiTi and a 17 × 25 rectangular NiTi (Figures 5 and 15). The arches were then stabilized with upper and lower flat 19 × 25 stainless steel wires. Forsus FFA was introduced at this stage after the leveling and alignment were completed (Figures 6 and 16). Maxillary second molars were banded from the beginning. The FFA was removed after 11 months in the female patient and after 10 months in the male patient after achieving Class I molar and Class I canine relationship (Figure 7).
Treatment Results
The desired treatment objectives were achieved—increase in the mandibular length and increase in the lower anterior facial height—and as a result the facial profile was improved. Along with the skeletal changes, Class I molar relation was achieved by the distal movements of the maxillary molars and the mesial movements of the mandibular molars. Ideal overjet and overbite were attained at the end of the treatment which lasted 2 years and 1 month in the female patient and 2 years and 3 months in the male patient (Figures 8, 9, 17, and 18).
Superimposition
The two sets of superimposition tracings highlighted the increase in the lower anterior facial height and the increase in the mandibular length. The maxillary incisors were intruded and mandibular incisors were proclined (Figures 10 and 19).
Retention
A Hawley’s retainer in the upper arch with an inclined plane was delivered, and a fixed lingual retainer was bonded in the lower arch. The patients were recalled after every 6 months to check the retention and stability of the treatment achieved. Photographs for long-term follow-up after 4 years of debonding are integrated in the present series (Figures 11 and 20).
With Protraction Utility Arch

Levelling and Alignment

With Forsus Appliance

Post Treatment Photographs

Post Treatment Radiographs
= Superimposition Tracing Where Blue Line – Pretreatment, Black Line – Pre-Functional, Red Line – Post Treatment
Follow Up photographs taken 4 years after debonding

Discussion
There are various techniques and appliances available to treat Class II malocclusion, which include removable and fixed appliances, extraoral appliances, various extraction patterns, and the surgical option. The appliance selection is based on the severity of the problem, as well as the patient’s cooperation.
The FFRD was familiarized for correcting Class II skeletal and dental complications in pre- and post-adolescence patients. The Fatigue Resistant Device (FRD), when used to treat mandibular retrognathism, showed more dentoalveaolar effects (66%) compared to skeletal effects (34%). 4 One major side effect of FRD, as with any functional appliance, is undesirable tooth movement of the lower incisors which limits the skeletal correction.5, 6 Various methods are mentioned in the literature to prevent lower anterior proclination, which include the use of negative-torqued lower incisor brackets or adding negative torque in the anterior section of the arch wire, soldering of hooks distal to the lower canines, tight cinch back of the lower arch wire distal to mandibular first molars, and miniscrews. 7 Lower incisor proclination can be minimized but cannot be completely eliminated.
According to Bowman et al, 8 the breakage rate of FRD is low and mainly depends upon the patient’s cooperation level. FRD when used with or without miniscrews had no significant effect on the maxillary or mandibular sagittal and vertical positions.7, 9 Some authors have reported significant maxillary growth restraint effect at either the peak or the post-peak period.10, 11 Gunay et al 9 found no significant effect in either the sagittal position of the mandible or the mandibular length. Dentoalveolar changes are more prominent with FRD.9, 10, 12, 13 Molar intrusion and distalization were because of the vertical and distal force vectors of the appliance.12, 13 The distally directed force of the FRD causes maxillary incisor extrusion, as well as retrusion. The mandibular molars are extruded as a result of downward and forward forces to the mandibular dentition by the appliance. In FRD, the overbite reduction was due to a combination of greater relative intrusion of mandibular incisors and lower extrusion of maxillary incisors. Overjet correction was totally dentoalveolar, typically by retroclination of maxillary incisors and proclination of mandibular incisors.
The cases reported in this article are of young patients at the late stage of puberty. FRD typically demonstrates mesial movement of the mandibular molars, tipping of the mandibular incisors, and variable effects associated with mandibular growth. The posttreatment results displayed significant improvement in the facial profile, that is, increase in the SNB angle and decrease in the ANB angle, showing skeletal changes in the mandible. The incisor mandibular plane angle (IMPA) was increased due to arch length deficiency in the lower arch. The end treatment outcome was satisfactory for both the orthodontist and the patients, with pleasing soft tissue profile changes, improved facial aesthetics, average lower anterior facial height, and an amiable smile arc.
FFAs have helped integrate the functional and fixed phases of treatment into a single-phase treatment. 12 The FFRD offers the following advantages to the clinician: anticipated results, 12 long-term dependability, 14 ability to be used in noncompliant patients, 15 ease of installation, 16 fewer breakages, 17 short treatment duration, 14 ability to make use of residual growth even beyond the pubertal growth spurt, 17 and negligible susceptibility to mechanical fatigue due to the spring. 18
Conclusion
On our menu, there are a plethora of appliances for the treatment of Class II malocclusion. However, it can be professed that the FFRD technique is an ultimate treatment option for noncompliant patients, as it provides stable results. In tune with the emerging concepts of soft tissue paradigm in treatment planning, Forsus works well with soft tissue contours and soft tissue adaptation.
Footnotes
Statement of Informed Consent
Written informed consent was obtained from the subject for the use of photographs for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.