
Abstract
Background
The most common congenital defects in the craniofacial region are the cleft lip and palate. It is thought that multiple factors contribute to the etiology, including environmental as well as genetic factors, leading to hyperdontia, hypodontia, microdontia, macrodontia, tooth rotation, and maligned teeth. These will result in functional issues, like difficulty with speech and aesthetic issues, which are quite prevalent among cleft patients.
Case Report
A 22-year-old female patient with a history of congenital unilateral cleft lip and palate had undergone surgical closure correction 10 years ago and recently underwent orthodontic treatment for malocclusion correction. On intraoral examination, she presented with a partially edentulous left maxillary lateral incisor and an oronasal opening in the anterior part of the hard palate. Treatment involved making an impression, pouring the cast, and performing block-out. A long labial bow was fabricated, and the prosthesis was constructed using chemically activated polymethyl methacrylate resin.
Conclusion
The multipurpose prosthesis enhanced the patient’s speech and aesthetics and acted as a retainer for the post-orthodontic phase.
Introduction
Cleft lip and palate (CL/P) and cleft palate (CP) are the most common congenital craniofacial anomalies, classified as unilateral or bilateral and as complete or partial defects. CL/P and CP occur in approximately 1 in 700 births worldwide and in about 2% of live births in Asian populations.1, 2 These defects arise between the 5th and 9th weeks of embryonic development due to a combination of genetic and environmental factors, such as maternal fever, zinc deficiency, alcoholism, smoking, stress, obesity, and inadequate folic acid intake. 3
CL/P and CP may present as either syndromic, associated with systemic conditions like Patau, Treacher Collins, Pierre Robin, or Goldenhar syndromes, or non-syndromic, occurring independently. Common dental anomalies—such as hyperdontia, hypodontia, microdontia, macrodontia, and malalignment—often lead to functional and aesthetic challenges. 4
Comprehensive management of CL/P involves a multidisciplinary approach from infancy through adulthood, engaging pediatricians, orthodontists, maxillofacial surgeons, and prosthodontists. Orthodontic intervention aims to achieve functional and aesthetic occlusion, facilitating secondary alveolar bone grafting in late childhood for bone continuity, tooth eruption, and future prosthetic stability. 5 Treatment typically progresses in stages: nasoalveolar molding and surgical correction in infancy, orthodontic therapy during mixed dentition, comprehensive orthodontics in the permanent dentition, and final prosthodontic rehabilitation. 2 This report describes the prosthodontic management of a patient with a residual oronasal opening and missing anterior teeth following orthodontic treatment.
Case Report
A 22-year-old female patient reported to the department of prosthodontics at SRM Dental College in Chennai, India, to replace a missing left maxillary lateral incisor. The patient had a history of unilateral CL/P. She had undergone a surgical closure of the CL/P 10 years ago, and then recently underwent orthodontic treatment for the correction of malocclusion and the debonding of her braces was done.
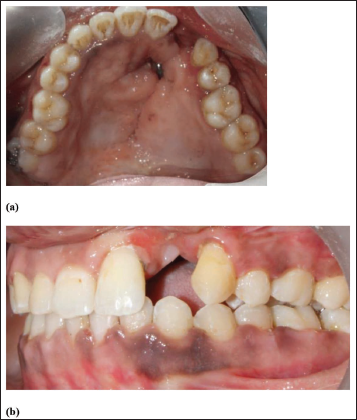
During the intraoral examination, an oronasal fistula measuring 0.3 mm × 0.3 mm × 0.5 mm was noted in the anterior hard palate, adjacent to the site of the missing left maxillary lateral incisor. The patient had difficulty with speech articulation and nasal air flow due to the presence of the oronasal fistula (Figure 1). The patient wanted the closure of the opening as well as the replacement of the missing tooth. This procedure, followed by the use of retainers, was advised for post-orthodontic management, and so a removable partial denture incorporated with a long labial bow was planned to be used. The prosthesis would act as both a retainer and a closure of the oronasal opening in the anterior part of the hard palate. Therefore, the treatment plan was explained and started after informed consent was obtained from the patient.
Step-by-step Procedure
The oronasal opening area was irrigated with sterile saline, and the opening was secured using povidone–iodine-impregnated sterile gauze.
A single-stage impression was made with addition silicone (Hydrorise Putty, Zhermack Dental, Italy), and the cast was poured using type III dental stone (Asian Chemicals, India) (Figure 2).
The cast was carefully retrieved, and the defect was blocked out with type II gypsum (Shruthi Products, India) to prevent acrylic flow (Figure 3).
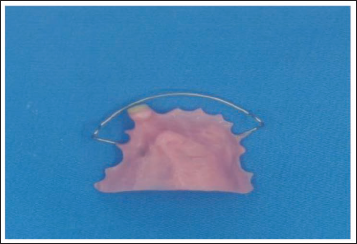
A 21-gauge (0.7 mm) stainless steel long labial bow (Konark, India) was fabricated, and suitable artificial teeth (Premadent, Ashwin Denture Materials, India) were selected and adapted to verify occlusion.
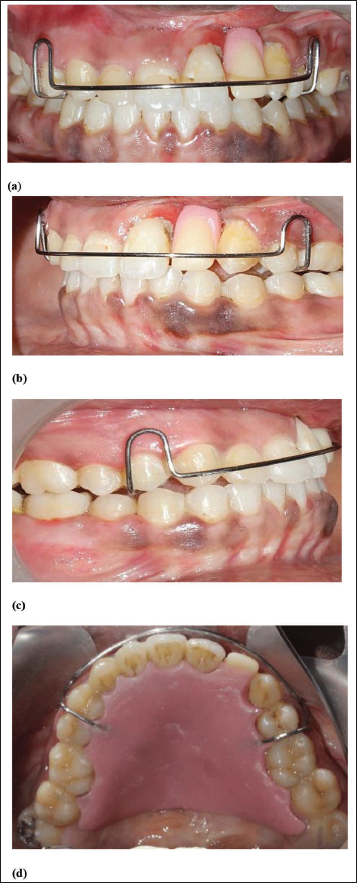
The prosthesis was fabricated with chemically activated PMMA (DPI Cold Cure, Mumbai, India) using the sprinkle-on method, followed by finishing and polishing with graded abrasives (3M Dental, India) and pumice (Giriraj Products, India) (Figure 4). Postoperative instructions were given, and follow-up was scheduled for every 6 weeks (Figure 5).
At the 6-week review, the patient showed a marked improvement in phonetics and aesthetics, verified through the subjective assessment of articulation and reduction in nasal speech. Objective phonetic tests were not performed and are acknowledged as a limitation.
(a) Intraoral Preoperative-palatal View. (b) Intraoral Preoperative-lateral View.
Final Impression.

Working Cast.

Multipurpose Appliance.
(a) Postoperative Frontal View. (b) Postoperative Lateral View. (c). Postoperative Lateral View. (d) Postoperative Palatal View.
Discussion
Charles Hawley first developed the Hawley retainer in 1919. The acrylic baseplate and wire components, which include clasps for retention and a long labial bow made of 0.7 mm stainless steel wire, comprise this design. 6 Patients with CP have their acrylic plates altered to accommodate prosthetic teeth in the spaces caused by missing teeth, which will eventually be replaced with prostheses or dental implants.
Dhole and Maheshwari 7 reported a case in which, in the upper arch, a wraparound retainer and a fixed lingual bonded retainer were given to the patient. The maxillary left lateral incisor was temporarily replaced with a tooth with a retainer. The maxillary left lateral incisor was replaced with a dental implant four to six months after the alveolar bone grafts were placed. Gardner et al. 8 reported a case in 1996 with a 16-year-old girl who had orthodontic correction of her permanent dentition done in addition to the surgical repair of her lip, alveolus, and palate for a bilateral CL/P. To seal a remaining tiny fistula in the palate and alveolus, conventional palatal coverage incorporating a removable partial denture framework with ball clasp retention was used. It replaced the four incisor teeth and served as a retainer.
After observing that many developing patients were unable to have their teeth erupt in the grafted cleft area of the maxilla, Singh et al. 9 modified the retention method by using a fixed bonded retainer on each of the affected teeth in addition to a removable retainer used post-orthodontic procedures. In 1987, Cohen et al. 10 presented a new technique for replacing the missing teeth related to an alveolar ridge defect in a 17-year-old individual with a unilateral CL/P. A customized Andrews-type bridge acted as the removable part of the design, while a resin-bonded retainer acted as the fixed partial denture segment.
A dual appliance was designed in 2010 by Basanagouda et al. 11 for a patient with CP undergoing orthodontic treatment. A fixed cast metal retentive plate was fixed to the lingual surface of the teeth, and a pontic was incorporated for the functional and aesthetic rehabilitation of the missing teeth. In 2010, Collins et al. 12 reported a removable retainer that incorporated components of the Essix and Hawley retainers in a hybrid design. The labial segment of the teeth was covered by a close-fitting Essix material that allowed the buccal segment to settle vertically. It additionally included an acrylic baseplate with various clasp designs, such as a ball-end clasp that worked similarly to a Hawley retainer to control the width and form of the arch.
Cold-cured acrylic resin was used due to its ease of manipulation, chairside adjustability, and faster fabrication, which was necessary for the immediate rehabilitation of the patient. Although heat-cured resin offers superior strength and longevity, the cold-cure resin allowed quicker closure of the oronasal opening, immediate phonetic improvement, and patient satisfaction. The prosthesis was planned as an interim measure, not a definitive long-term solution.
The management of a patient with a retained oronasal opening involves an interdisciplinary approach to treat the patient’s speech affected by a palatal opening with a prosthodontic approach to enhance the quality of life of the patient. If the patient completes the orthodontic treatment, a retainer should be incorporated with a removable prosthesis after the retention period, and either a fixed prosthesis or surgical correction needs to be taken into consideration later.
The long-term treatment plan would include the definitive closure of the oronasal fistula, either surgically or prosthetically, followed by an implant-supported prosthesis in the missing lateral incisor region once adequate alveolar bone grafting and healing are achieved. Until then, the current removable prosthesis serves as an interim functional and aesthetic solution.
Conclusion
For patients with retained openings after the surgical correction of congenital defects, a removable or other modified prosthesis should be fabricated based on the size and location of the defect to ensure the quality of life of the patient. This multipurpose prosthesis, incorporated with a retainer, enhances the patient’s speech and aesthetics as well as acts as a retainer for the post-orthodontic phase.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
Ganesh Ramkumar Rajapandi: Data curation, formal analysis, investigation, resources, writing original draft.
Ahila Singaravel Chidambaranathan: Conceptualization, methodology, project administration, validation, writing review and editing.
Muthukumar Balasubramanium: Writing review and editing, supervision.
Data Availability
Data will be available upon request.
Ethical Approval Institutional Statement
The study was approved by the Institutional Review Board of SRM Dental College, Ramapuram, Chennai.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent is obtained from the participants prior to start the treatment.