
Abstract
Introduction
The world of orthodontics has its fair share of debates. One such topic is that of one-phase versus two-phase treatment, or early versus late therapy, as some like to call it. To put it simply, a one-phase therapy is finished in a single stage, whereas the latter is carried out in two stages, throughout two different age periods.
Aims and Objectives
To assess and discuss the current notion of one-phase and two-phase therapy in the management of Class II malocclusion, along with their efficacy, long-term stability, cost effectiveness and patient compliance, as demonstrated by years of research.
Methods
All existing literature related to two-phase treatment and late single-phase treatment in Class II malocclusion cases were reviewed, analyzing the respective benefits and drawbacks.
Results
All the evidence advocates that two-phase treatment does not outperform one-phase treatment in skeletal correction, treatment stability, or reducing treatment complexity in Class II malocclusion. Early intervention can be beneficial in a few scenarios, but it typically prolongs treatment duration, increases costs, while reducing patient compliance.
Conclusion
This review indicates the need for re-evaluation of early two-phase treatment in Class II malocclusion. Rather than a generalized preference for early intervention, customised treatment planning is more desirable.
Introduction
Debates or controversies are a common occurrence in the scientific world, including the field of medicine and dentistry. The world of orthodontics has its own fair share. One such topic, frequently generating clashes of opinion in the orthodontic circle, is that of one-phase treatment versus two-phase treatment, or early treatment versus late treatment, as some like to refer to it. In simple words, one-phase treatment can be understood as treatment completed in a single stage, while in two-phase treatment, the execution is performed in two steps, in two separate age periods.
Now, it is generally understood that early diagnosis, along with timely intervention, is of utmost importance in treating malocclusion effectively. In fact, the American Association of Orthodontists (AAO) recommendation is that a child’s first consultation with an orthodontist should be done by the age of 7 years. 1 The goal of early intervention is to intercept or correct developing skeletal, dentoalveolar, and muscular imbalances. This is where the two-phase treatment protocol comes in, where in phase I, orthodontic treatment is initiated to intercept the developing malocclusion, 2 and later on, treatment is completed in phase II.
However, in the case of Class II malocclusion, the advantage of early or two-phase treatment has often been put into question. Although the textbook concept is to intercept Class II malocclusion with early intervention, a number of studies have reported that early two-phase treatment for Class II patients has, in fact, no particular advantage over late one-phase treatment.3–6
Hence, in this article, we shall be discussing in detail the current concept of one-phase and two-phase treatment in the management of Class II malocclusion and their effectiveness, as evidenced by years of research.
So, One-phase and Two-phase Treatment Protocols: What Is It, Exactly?
Traditionally, two-phase treatment refers to treatment done in primary or mixed dentition to intercept certain malocclusions, followed by a later treatment, with the aim to make the treatment easier as well as achieve stable results. 5 Two-phase treatment usually involves a waiting period between the first phase and the second phase, for the complete eruption of permanent teeth. Phase I generally involves 6–12 months of active treatment with the intent to change skeleto-dental relationships. Phase II is the final finishing stage after the eruption of appropriate permanent teeth. 7 Advocates of the two-phase treatment point to several advantages, including the reduction in the number of extractions required, the possibility of more consistent outcomes, and the opportunity to fully utilize the patient’s growth, perhaps preventing additional surgical procedures. 8
On the other hand, one-phase treatment is performed at the stage of early permanent dentition. 5 One of the benefits of one-phase treatment, which is often mentioned, is shorter treatment time. Proponents of one-phase argue that the total treatment time of two-phase is comparatively longer, that is, the total time spent in phase I and phase II exceeds the whole time needed to treat the case in a single-phase once the patient has attained full permanent dentition. 8
So, in essence, we can deduce that the major difference between one-phase and two-phase is the retention period or the gap between the treatment period. And, rather than the controversy of one-phase versus two-phase, the actual argument appears to be whether early intervention or late intervention is better. Or in other words, is early two-phase more beneficial, or is late one-phase better?
When Two-phase Treatment Protocol Usually Recommended?
Recommendations for two-phase treatment with early intervention in the orthodontic literature comprise of situations with crossbites complicated by a mandibular shift, certain patients with Class III malocclusions who could benefit from immediate resolution of the problem, Class II division 1 malocclusion cases, functional problems, and mild dental discrepancies or skeletal deficiencies with a predictable excellent growth potential.5, 9, 10
Other suggested criteria include developmental crossbites, functional shifts, severe crowding (more than 8 mm discrepancy), and overjet greater than 10 mm. 11
What Is Not Considered Two-phase Treatment?
Sometimes, we come across the words two-phase treatment and interceptive orthodontics used interchangeably. However, this is not exactly true. Not all interceptive interventions can be considered part of the two-phase treatment protocol. Habit-breaking appliances, space maintainers, and minor alignment of incisors, either due to trauma or for aesthetic reasons, are not considered part of conventional two-phase treatment. 5
One-phase/Two-phase Treatment in the Class II Malocclusion Scenario
Two-phase treatment in Class II malocclusion typically comprises the early use of functional or orthopedic appliances, or both, in the first phase or phase I of treatment during the mixed dentition period, followed by a period of retention. Finally, a second phase of fixed appliance treatment or aligner therapy follows in the early adolescent period. 12
While in one-phase, the whole treatment is integrated into a single-phase during the late mixed dentition or permanent dentition. 12 It involves functional jaw orthopedics followed by fixed appliances or clear aligner therapy to finalize the occlusion, without a period of mid-treatment retention. 13
Why Two-phase?
For preadolescent children with Class II malocclusion, the optimal timing for treatment remains controversial. Early intervention has often been advocated, as Class II malocclusion, which is characterized by significant overjet and overbite, can have detrimental repercussions on a patient’s functional, psychological, and self-image problems. Other commonly mentioned reasons include the risk of trauma to the proclined maxillary incisors present in Class II malocclusion, more stable treatment results, and less complex phase II treatment.8, 14–16 Thus, for all the above-mentioned reasons, the two-phase protocol is often recommended.
In regard to the improvement of psychosocial status, the Cochrane systematic review on Class II malocclusion suggested that, although self-concept and self-esteem improved initially for patients having treatment early, this effect was not maintained to the end of phase II treatment in adolescence. Nevertheless, the report also mentioned that the increase in self-esteem that occurs with early intervention may have clinical importance, particularly if a child is subjected to excessive teasing or bullying. 17
However, in terms of treatment stability, recent studies report that phase I results of two-phase therapy are not stable in the long-term. The skeletal effects of early treatment, on average, are not maintained, and little differences in the ANB angle could be observed in both early and late groups after completion of comprehensive fixed orthodontic treatment. In addition to this, it has been suggested that the skeletal changes in early treatment, particularly the increase in mandibular growth seen with functional appliances, may simply represent an acceleration in growth rather than a net gain.3, 18–20 Moyers also stated that there is no guarantee that early treatment outcomes will last, and receiving treatment in two phases will always result in a longer total treatment duration. 21
Apart from the questionable stability, early two-phase therapy is considered more expensive than late one-phase and also takes longer treatment time. When the treatment time is prolonged, patient compliance begins to decline. Early two-phase treatment can not only cause harm or lengthen therapy, but it can also drain a child’s willingness to cooperate and comply.4, 21 All this evidence clearly suggests that routine early two-phase treatment does not provide any advantage over one course of treatment provided in adolescence, in terms of treatment stability or reduced complexity of phase II treatment. Treatment in late childhood appears to be more practical and cost-effective because it reduces the total length of time a child is seen by an orthodontist. 22
Why Late Single/One-phase Treatment is a Better Option?
During treatment planning, it is required to take into account various factors such as the optimal timing for correcting the skeletal disparity, treatment effectiveness, the possibility of reducing the overall treatment duration, patient compliance, and overall expenses.
As mentioned earlier, one of the most common problems encountered in two-phase is the issue of poor compliance, often due to the long treatment duration. This, in turn, creates a sequela of events which ultimately affects the treatment result. Though the idea of two-phase treatment might be preferable to proactive parents, who prefer to address their children’s malocclusion before it fully develops, it is not always the best option for every patient. Even in some cases where early treatment is desirable, the young child may not be able to follow the treatment instructions effectively for a satisfactory result.
H. G. Barrer, in his article titled “Treatment Timing Onset or Onslaught?”, recommended a few conditions where late treatment is more beneficial:
Any deficiency in the skeletal structure where growth is not favorable will work against an early treatment technique that is successful. The patient finds the necessary treatment to be less tolerable than the malocclusion. The current condition of malocclusion does not result in psychological issues due to dental or facial disfigurement, is stable in its deformity, adequately satisfies function, permits reasonable maintenance of tissue health, and, finally, the delay will make treatment more predictable, feasible, successful, and stable.
9
Also, numerous studies conducted on the results of early and late treatment of Class II malocclusion have reported that the final treatment results, in both one-phase and two-phase treatment, turn out to be the same. In fact, recent studies have reported that early two-phase treatment is no more effective and considerably less efficient as compared to late one-phase treatment.
To quote a few studies:
Three major clinical trials of early two-phase versus late one-phase Class II malocclusion treatment, conducted at the universities of North Carolina, Florida, and Manchester, concluded that although headgear and functional appliances in the early phase I are effective in growth modification, resulting in a significant difference between treated and untreated groups of children; however, at end of the final fixed appliance stage, no difference was observed. 23
In another study conducted by McNamara et al., it was demonstrated that more mandibular growth was observed in patients who were older than 10.5 years, in comparison with the growth observed in younger patients when both groups were treated with the FR2 appliance. 24
Wieslander also compared the treatment results of extraoral appliance in two groups of patients, early and late mixed dentition patients, and found only a minor difference of 1 mm greater orthopedic effect in the early treatment group. This 1 mm difference does not seem to be a good bargain for the higher treatment cost and longer time duration needed in two-phase treatment. 25
The previous conclusions were also depicted in a study by Cha et al., in which the outcomes of early versus late treatment in severe Class II high-angle cases were compared. The results showed that early two-phase treatment showed no skeletal anteroposterior advantages over late one-phase treatment. Severe high-angle Class II patients showed similar dental anteroposterior outcomes with the use of both approaches. 26
In addition, there is also the risk of potential iatrogenic problems that may occur with early treatment, such as dilaceration of roots, decalcification, impaction of maxillary second molars from distalizing first molars, incisor root resorption, molar ankylosis, patient burnout, and, in some cases, frustration of the parents by the additional expense of the long treatment period. 27
In my early years of practice, I usually opted for the early correction of Class II malocclusion using functional and orthopedic appliances such as the FR II, activator, and headgear. The use of such appliances sometimes ended up becoming unbearable for the young, energetic, and playful child, ultimately exhausting the patient for the follow-up treatment phase.
During those days, I preferred the use of early activator-headgear, thinking of converting Class II malocclusion into non-extraction cases. However, on follow-up, in many of these cases, extraction often became a necessity in the final phase of treatment. A similar result was reported in a clinical trial conducted at the University of North Carolina. The clinical trial showed that there was no difference between the early treatment and late treatment groups in the requirement of premolar extraction during comprehensive treatment or the need for orthognathic surgery. 23 Another statement we often seem to dismiss is the theorem of retention. 28 Riedel’s fourth theorem of retention clearly states that “proper occlusion is a potent factor in holding teeth in their corrected positions.” Thus, it is important to keep in mind that proper occlusion is a prerequisite to prevent relapse, especially in cases of Class II bite jump.
The ideal timing for a Class II correction with the use of a functional appliance, such as twin-block and activator, has been reported to be peak pubertal growth.29–33 Giuntini et al. recommends that for the treatment of mandibular retrusion in growing Class II patients using functional jaw orthopedics, it is advisable to delay until at least CVM stage 3 is attained. 13 Also, Gianelly maintains that at least 90% of children with Class II malocclusions, with or without crowding, can be successfully treated in one period of care, lasting 2-3 years, if therapy is initiated in the late mixed dentition stage of development. 5 Hence, I would recommend late single-phase treatment instead of early intervention.
To mention some treatment protocols:
If the predicted occlusion is good, when the patient’s cast models are oriented in a Class I molar relationship, mandibular advancement with a functional appliance followed by fixed appliance treatment is a preferred treatment modality. In the case of non-compliant patients, a fixed functional appliance is a good option (Cases I, II, and III). In other scenarios, decompensation after extraction of either all four first premolars,
34
or lower first premolars, or an atypical extraction pattern, followed by bite jump is a good option (Case IV).
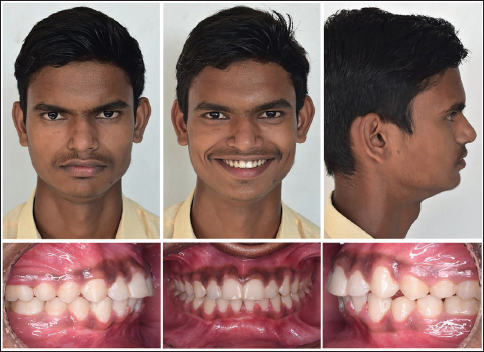
Case I: Late one-phase therapy in a 13-year-old Class II Division 1 male patient, with non-extraction protocol and a twin-block appliance (Figures 1–3).
A 13-year-old Patient with Class II Division 1 Malocclusion Before Treatment.

Twin-block Appliance After Alignment of the Upper Arch.

Post-treatment Extraoral and Intraoral Photos.
Case II: Late one-phase therapy in a 13-year-old Class II Division 2 male patient, with non-extraction protocol and a fixed twin-block appliance (Figures 4–6).
A 13-year-old Patient with Class II Division 2 Malocclusion Before Treatment.

Fixed Twin-block Appliance After Alignment of Upper Arch.

Post-treatment Extraoral and Intraoral Photos.

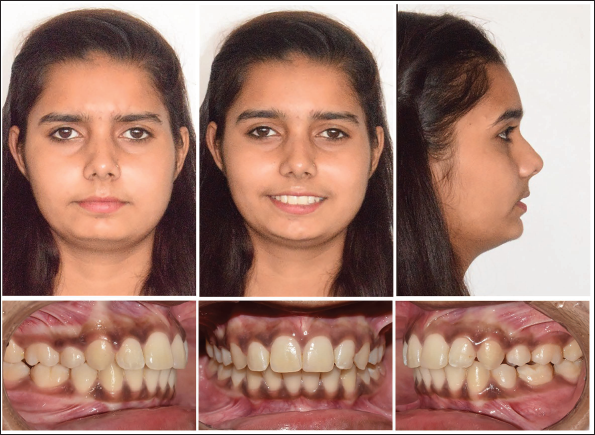
Case III: Late one-phase therapy in a 13-year-old Class II Division 1 female patient, with non-extraction protocol and a fixed functional appliance (Figures 7–9).
A 13-year-old Patient with Class II Division 1 Malocclusion Before Treatment.

Placement of Fixed Functional Appliance (PowerScope).

Post-treatment Extraoral and Intraoral Photos.

Case IV: Late one-phase therapy in a 13-year-old female patient, with decompensation after extraction of all four first premolars, followed by a fixed functional appliance (Figures 10–12).
A 13-year-old Patient with Class II Division 1 Malocclusion Before Treatment.

Class II Corrector Placed After Decompensation.

Post-treatment Extraoral and Intraoral Photos.
Many other research can be found in the orthodontic literature, providing evidence that, indeed, late one-phase treatment is a much better option than the long, cumbersome two-phase treatment. Of course, this does not mean that two-phase treatment is not effective or useless in the management of Class II malocclusion. In fact, early intervention is recommended in cases where it has the potential to improve psychosocial status in an excessive teasing or bullying environment, risk of occurrence of dental trauma, or interdisciplinary management of diagnosed obstructive sleep apnea (OSA) risk in growing patients with constricted maxilla (OSA diagnosis in children includes Apnea–Hypopnea Index (AHI), Respiratory Disturbance Index (RDI) index greater than 1, Pediatric Sleep Questionnaire from the University of Michigan, and others).35–40
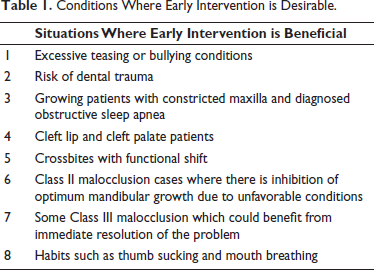
Phase II treatment is also beneficial in the case of cleft patients, where it is indeed important to initiate the treatment early and follow up in subsequent stages. However, apart from these cases, the literature is rich with evidence that two-phase has no advantage over one-phase, and instead, it might be detrimental to a child’s cooperation. Table 1 summarize specific situations where early intervention may be fruitful.
Conditions Where Early Intervention is Desirable.
So, in conclusion, the so-called one-phase/two-phase dilemma is quite obvious. Late one-phase treatment does seem to be the answer for the routine management of Class II malocclusion, unless, of course, the monetary gain from the long treatment period of two-phase is your priority.
Footnotes
Acknowledgment
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
No Institutional Ethical Committee approval was needed for this case study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the patients’ guardians.