
Abstract
This case report was presented at the Indian Board of Orthodontics (IBO) examination under category III in September 2022. It describes the case of 13-year-old female with hyperdivergent facial pattern and class II skeletal base, treated using microimplant anchorage. Patient presented with vertical maxillary excess, increased lower facial height, gummy smile, and incompetent lips. All four first premolar extraction treatments were planned with simultaneous retraction and intrusion of maxillary and mandibular dentition. The case was treated using 022 slot MBT prescription appliance. Lip exercises were prescribed to increase the tone of lips, which would aid in attainment of lip seal. Case was completed with class I molars, normal overjet–overbite, and improved smile aesthetics. The patient exhibited competent lips and reduced anterior–posterior gingival show.
Keywords
Introduction
Excess vertical growth of maxilla, producing class II skeletal pattern, is a common occurrence. Due to vertical descent of maxilla, mandible rotates posteriorly. 1 Clockwise rotation of mandible increases the convexity of profile, giving appearance of deficient chin. If the patient is in growing phase, then it opens up an avenue for orthodontist. If they are able to control the eruption of posterior teeth and allow the vertical growth of ramus to express itself, then the resultant anticlockwise rotation of mandibular plane brings about following favorable changes in the face: (a) Control of lower facial height, (b) reduction of sagittal maxilla–mandibular discrepancy, and (c) reduction of convexity of facial profile while ‘carving out the chin’. Control of vertical dimensions in orthodontics is no more a challenge with the invention of various temporary anchorage devices (TADs). Among them, mini-screws have the advantage of easy insertion–removal, versatility of locations of insertion, minimal trauma, and a low cost. 2
Chief Complaint
The patient has forwardly placed upper and lower front teeth, with excessive gums displayed during smile.
Relevant Medical History
Age at start of treatment was 13 years and 6 months. Menarche took place 6 months back. Parent reported that the patient offered excellent cooperation while undergoing previous general dentistry work.
Clinical Examination: Extra-Oral Features (Figure 1)
Pre-treatment Photographs: Extra-oral.

Facial profile: Convex. Mandible was retrusive with steep mandibular plane angle.
Facial height: Increased lower facial height
Lips: Incompetent with 6–7 mm separation at rest
Incisor show at rest and during function was excessive. Gingival display during smiling is excessive.
Nasolabial angle: Acute
Mentolabial sulcus: Shallow
Chin was deficient with hyperactive mentalis. Chin–throat angle was obtuse with decreased throat length.
Clinical Examination: Intraoral Features (Figure 2)
Pre-treatment Photographs: Intraoral.

Oral hygiene: Good
Soft tissues: Marginal and papillary gingiva in upper and lower anterior segment appeared dry but devoid of any inflammation. Frenal attachments were normal. Good amount of attached gingiva was present in maxillary and mandibular posterior segment.
Erupted teeth present: 17,16,15,14,13,12,11,21,22,23,24,25,26,27
47,46,45,44,43,42,41,31,32,33,34,35,36,37
General dental condition: Glass ionomer cement (GIC) restorations in 16,26,36,46
Maxillary arch spacing: 2 mm, mesiolabial rotation of all maxillary incisors
Mandibular arch crowding: 1 mm, mesiolabial rotation of 42 and crown lingual rolling of 47
Tooth size: 12,11,21,22 are larger in size mesiodistally and incisocervically.
Occlusal Features
Incisor relationship: Class II division I
Overjet (mm): 5 mm
Overbite: 3 mm
Center lines: Coincident
Left buccal segment relationship: Class I molar, class I canine
Right buccal segment relationship: Class I molar class I canine
Exaggerated curve of Spee in lower arch
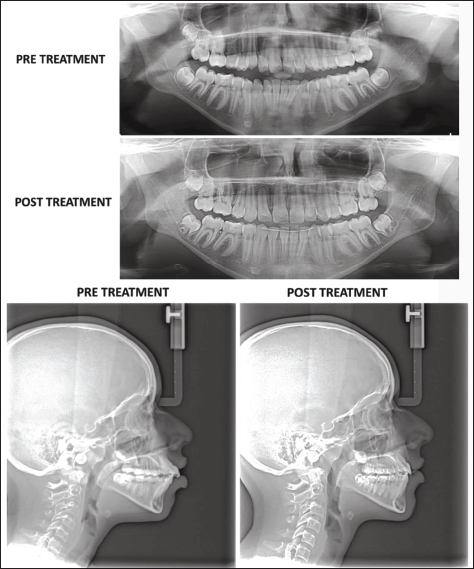
General Radiographic Examination (Figure 3)
Unerupted teeth: All four third molars
Relevant Radiographic Findings: (A) Lateral Cephalogram and (B) Orthopantomogram (OPG).
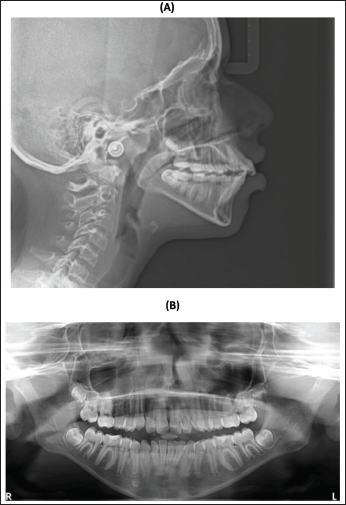
Partially erupted: All permanent second molars
Inter-radicular bone levels were normal. Canine and premolars in all quadrants show completion of root formation; however, apical closure was yet to take place. Second molars show incomplete root formation. Developing tooth buds of all four third molars were present. Temporomandibular joint (TMJ) appears normal.
Pharyngeal airway: Upper pharyngeal airway dimensions appear lesser than normal (5 mm), probably on account of hyperplastic nasopharyngeal adenoid tissue. Lower pharyngeal airway was normal.
Images of cervical vertebrae indicate patient was in stage III–IV (inferior border of body of vertebrae is flat, and shape of body is rectangular).
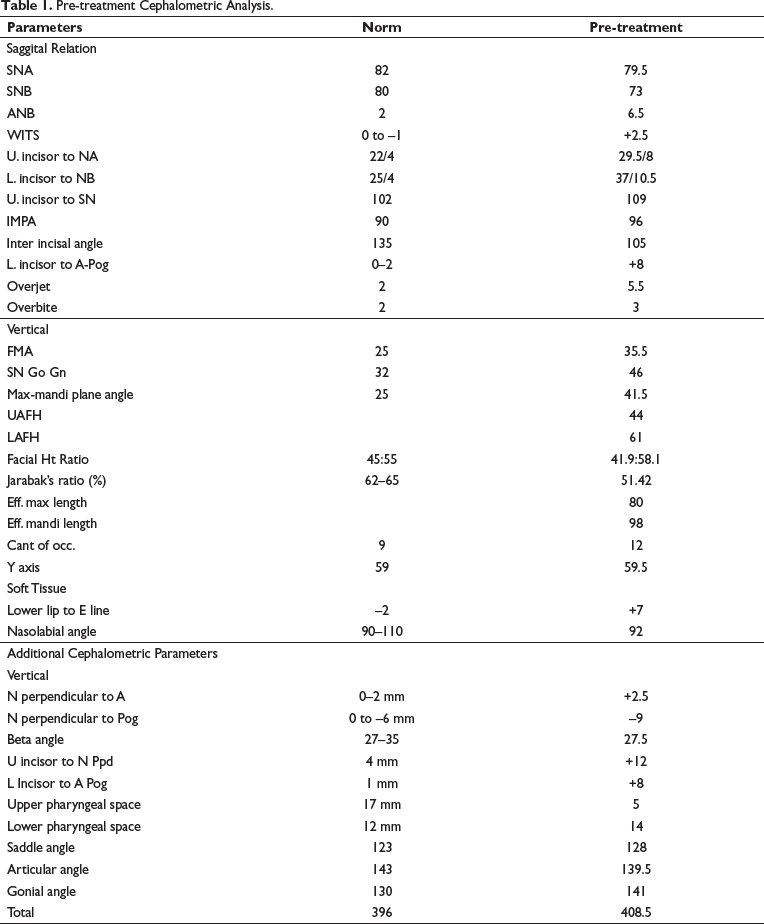
Interpretation (Table 1)
Maxilla was normally placed, and mandible was backwardly placed. There was a vertical growth pattern present, resulting in an increased lower facial height. Maxillary and mandibular incisors are proclined and forwardly placed. Bjork’s analysis suggests vertical growth pattern and downward and backward rotation of mandible. McNamara’s analysis suggests that sagittal discrepancy was caused by vertical descent of maxilla, resulting into clockwise rotation of mandible, and not due to deficiency of mandibular size. 1
Pre-treatment Cephalometric Analysis.
Diagnostic Summary
A 13-year-old female patient is diagnosed with Angle’s class I bimaxillary dentoalveolar protrusion on underlying class II skeletal base, vertical maxillary excess, vertical growth pattern, increased lower facial height, convex profile, proclined maxillary and mandibular incisors, increased overjet and overbite, protrusive incompetent lips, retrusive chin with hyperactive mentalis, and gummy smile.
Problem List
Backwardly placed mandible
Class II skeletal pattern
Vertical maxillary excess
Vertical growth pattern with increased lower facial height
Forwardly placed, proclined maxillary and mandibular incisors
Crowding in mandibular anterior segment
Incompetent lips with large interlabial gap
Aims and Objectives of Treatment
Correction of dentoalveolar proclination of maxillary and mandibular incisors
Intrusion of maxillary dentition to reduce anterior and posterior gumminess
Inducing upward and forward rotation of mandible, thereby improving chin prominence
Control of lower anterior facial height, thereby improving lip seal
Correction of crowding in mandibular arch
Increasing the tonicity of lip musculature
Treatment Plan
Since patient presents with Angle’s class I bimaxillary dentoalveolar protrusion on class II skeletal base, we planned to go ahead with dentoalveolar camouflage. Space required in mandibular arch for correction of proclination, crowding, and curve of Spee, as well as in maxillary arch for correction of proclination, overjet, and incisor derotation, can be achieved by extraction of all four first premolars.
Space analysis indicates that it is a group A (maximum anchorage) case. Cephalometric analysis indicates vertical anchorage is critical. TADs are used to augment anchorage in both sagittal and vertical planes. Four TADs are placed in maxilla (one each between second premolar and first molar bilaterally, one each mesial to lateral incisors bilaterally). The resultant force vector is expected to pass close to CR of maxillary dentition, thus causing simultaneous retraction and intrusion of maxillary anterior teeth. Intrusion of maxillary dentition is expected to bring about anticlockwise rotation of mandible. Two TADs are placed in mandible (one each between second premolar and first molar bilaterally). Apically directed force vector will keep the intrusive force over mandibular dentition during mandibular anterior retraction and maxillary arch intrusion. Maxilla is normally placed, and mandible is backwardly placed.2, 3
Bonding of all seven components could be delayed as they are partially erupted.
Extractions: 14,24,34,44 under local anesthesia
Appliance: PEA 022 slot MBT, friction mechanics for predictable force system
Special anchorage consideration: Microimplant anchorage
Proposed retention strategy: Hawley’s retainer for maxillary and mandibular arches. BLR for mandibular anterior segment to retain correction of lower incisor imbrications.
Additional notes on treatment plan:
Myofunctional exercises:1, 4
Lip-closed nasal breathing Puffer fish exercise to be done daily three times for 10 minutes Tug of war lip exercise daily three times for 5 minutes Tongue posture training (tip of the tongue behind incisive papilla) Chin massage to reduce hyperactivity of mentalis muscle
Prognosis for stability: Good. The main potential for relapse in this patient relates to the anterior and posterior teeth intrusion. Continued downward sutural growth of the maxilla in a vertical direction may increase incisor/gingival show and also cause clockwise rotation of mandible. 1
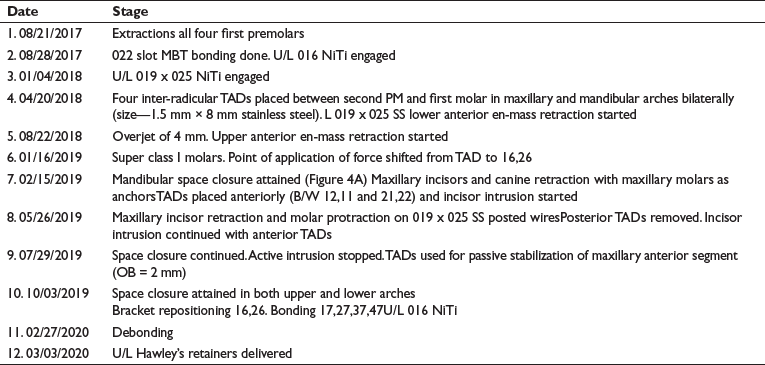
Treatment
Treatment Progress
Start of active treatment: 08/21/2017
Age at start of active treatment: 13 years and 8 months
End of active treatment: 02/26/2020
Active treatment time: 30 months
Key Stages in Treatment Progress (Figure 2)
(A) Incisor Retraction. (B) Second Molar Leveling and Maxillary First Molar Settling.
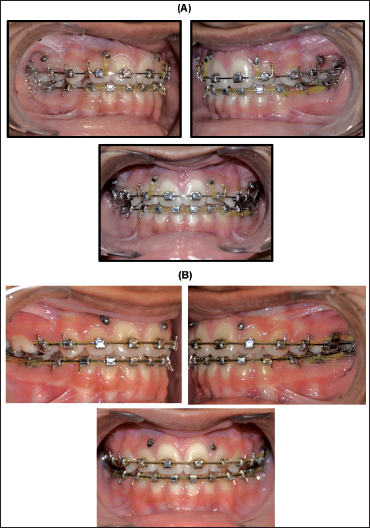
Mid-treatment Photographs (Figure 2)
Occlusal Features
Incisor relationship: Class I
Overjet (mm): 2.5 mm
Overbite: 2.5 mm
Center lines: Coinciding
Left buccal segment relationship: Class I molar, class I canine
Right buccal segment relationship: Class I molar, class I canine
Index of Treatment Need (IOTN)
Dental health component:
Start: 3a
Finish: 1
Aesthetic component:
Start: 2
Finish: 1
Peer assessment rating (PAR):
Start: 10
Finish: 1
Change: 9
Percentage change: 90%
Interpretation (Table 2)
Post-treatment Cephalometric Assessment.
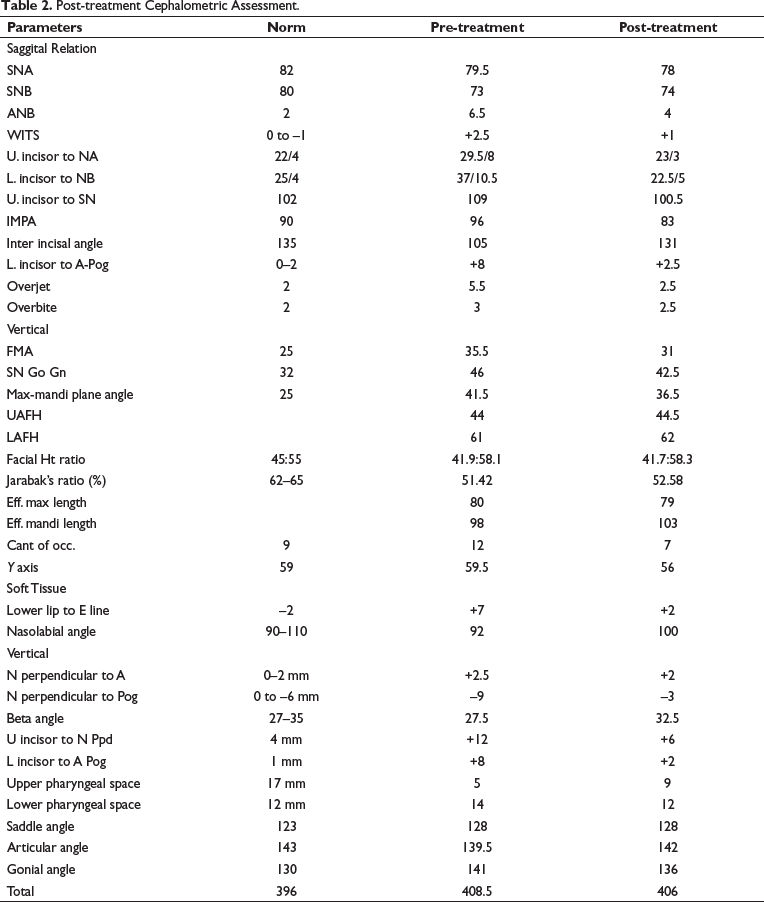
Maxillary incisors were normally placed with normal inclination.
Mandibular incisors were uprighted (high angle case) and are almost normally placed.
Forward rotation of mandible was evident.
Procumbancy of soft tissue lip profile was significantly reduced.
Nasolabial angle was increased.
Critical Appraisal
Smile Aesthetics
There is significant improvement in smile esthetics with correction of gummy smile due to true intrusion of maxillary anterior. Smile arc is consonant and follows curvature of lower lip. A 2 mm gingival display during function is ideal.
Facial Esthetics (Figure 5)
Anticlockwise rotation of mandible resulted into forward movement of chin. Convexity of the profile is reduced. Lip procumbency is reduced as a result of correction of proclination. Lip strain is eliminated, and interlabial gap is closed.
Post-treatment—Extraoral.

Dental (Figure 6)
Class I occlusion has been achieved on both the sides with stable intercuspation and ideal overjet–overbite. Intrusive force onto maxillary dentition had buccal point of application. In post treatment occlusion, buccal flaring of maxillary posterior segment with hanging of palatal cusps is evident, especially on right side. Settling of occlusion should take care of it. Caries activity appears to have increased, with pit and fissure caries in 17,27,37,46,47. Patient is advised continuation of fluoride mouthwash and to get the restorations done as soon as possible.
Post-treatment—Intraoral.

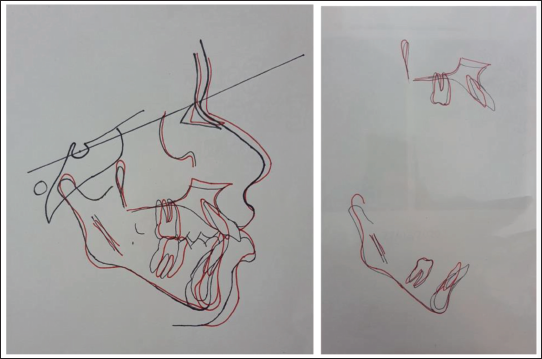
Skeletal (Figure 7)
Backward movement of Pt A is a result of bony remodeling due to bodily posterior movement of maxillary incisors. Changes in FMA, SnGoGn, and Y axis all point toward upward and forward rotation of mandible. The resultant forward movement of Pt B has contributed toward correction of skeletal discrepancy in sagittal plane. Vertical proportions remained unchanged, signifying continuation of vertical growth pattern. Lower facial height increased by 1 mm, though mandibular length increased by 5 mm. This suggests that the growth is expressed more in sagittal plane.
Post-treatment Radiographs.
Mechanics
Friction mechanics are used for retraction to be more compatible with TADs and to avoid any extrusive component. Microimplants controlled occlusal movement of molars, all the while allowing vertical growth of ramus. Outcome is clockwise rotation of mandibular plane.
Radiographic (Figures 7 and 8)
Mandibular left lateral incisor warrants further root uprighting. Maxillary right lateral incisor shows apical root resorption that is within normal range. Tongue posture has improved, and tongue now assumes higher position under palatal vault, improving the A–P pharyngeal airway dimensions. Nasopharyngeal adenoid tissue shows physiologic regression. Incisor mandibular plane angle (IMPA) of 83° is normal in correlation with Frankfort mandibular plane angle (FMA) of 31°.
Cephalometric Superimposition.
Post-treatment Assessment
Retention
Stability of maxillary incisors depends upon their relation with lower lip and attainment of normal overjet, overbite, and interincisal angle, which appears favorable. The potential for relapse in this patient relates to continuation of vertical growth of maxilla, which may cause gumminess; however, vertical growth of lip during adulthood will counter it.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient/participant has consented to the submission of the article to the journal.