
Abstract
Mini-implant-assisted rapid palatal expansion (MARPE) offers a less invasive option for management of skeletal maxillary transverse discrepancy in advanced stages of palatal sutural maturation that cannot be optimally addressed by conventional rapid maxillary expansion techniques. This article briefly discusses two cases of transverse skeletal maxillary discrepancy matched for age and sutural maturation but with varied outcomes. One of the cases was successfully managed with MARPE using the maxillary skeletal expander II (MSE II) appliance, while the other failed. This communication also aims to highlight the possible cause–effect relationship and the caution required in case selection for such techniques. Since the technique is still in its infancy, MSE II should be avoided in palatal region with bone density below 1,000 HU to prevent inadvertent failure.
Keywords
Introduction
Mini-implant-assisted rapid palatal expansion (MARPE) with appliances like maxillary skeletal expander (MSE) provides minimally invasive treatment option for addressing transverse maxillary deficiency without adverse impact on the dentition or vertical dimension. 1 Although the patency of most of the facial sutures is maintained even till sixth to eighth decade of life, the midpalatal suture undergoes differential fusion at the earliest and is the first decisive factor in appliance selection for nonsurgical management of maxillary transverse discrepancy.2, 3 MSE offers significant advantages but, it has numerous limitations as well like inability to use in narrow palate, extremely thin palate with low bone density, extremely thick dense palatal bone or zygomatic buttress bone, and in patients with previous mid-facial trauma.4, 5 Though extremely thick and thin palatal bones have been mentioned by proponents as limitation, there is no objective measure assigned for evaluation. This short communication aims to highlight two cases of Indian-origin patients, matched for maturity of the midpalatal suture and age range, with successful outcome in one and failure in the other, and reflect on the possible cause–effect relationship.
Case Presentation
Case 1: A 21-year-old girl reported for retreatment of open bite malocclusion and had associated maxillary transverse discrepancy. Cone-beam computed tomography (CBCT) evaluation of maxilla revealed midpalatal maturation stage “D.” The maxillary expansion was planned with MSE II appliance. MSE II appliance (8 mm, 1.8 mm × 11 mm) was placed under local anesthesia, and expansion was initiated as per the manufacturer’s protocol. 4 The activation schedule, considering the age of the patient, followed as per recommendations, was 2–3 turns/day, equivalent to 0.4–0.6 mm/day till the appearance of diastema, followed by 1 turn/day (0.2 mm) till the correction of discrepancy. This resulted in successful opening of the palatal suture, clinically verified with midline diastema, correction of transverse discrepancy, and confirmed by parallel midpalatal suture opening with repeat CBCT. The salient characteristics of the case are presented in Figures 1 and 2, and the details of palatal bone height and density of bone cross-section are shown in Table 1.
Pre- and Post-expansion Intraoral Occlusal Photographs (a and b) and CBCT (c and d), Respectively, of Case 1.
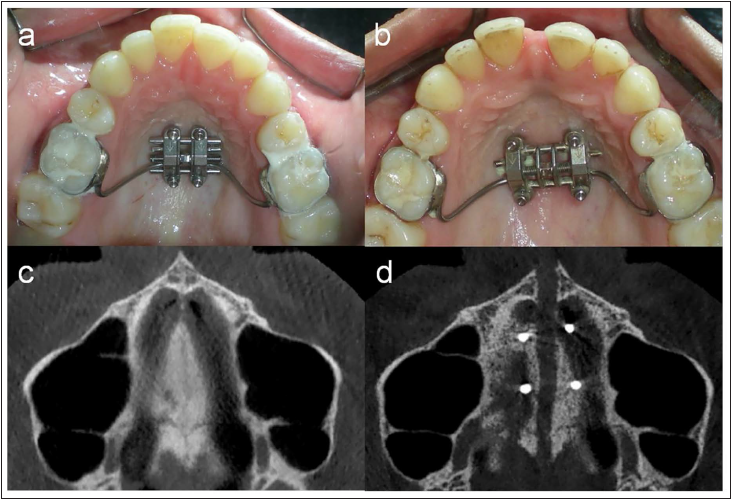
CBCT Showing Bone Density (a) and Palatal Bone Thickness and Bicortical Engagement (b) in Case 1.
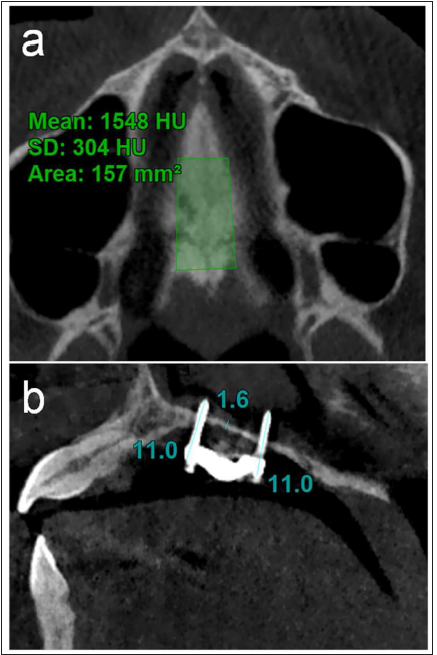
Palatal Bone Characteristics in Two Cases.
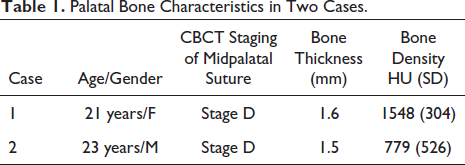
Case 2: A 22-year-old boy reported skeletal class III malocclusion and bimaxillary transverse discrepancy. The case was planned for maxillary arch expansion with MSE II appliance (8 mm, 1.8 mm × 11 mm). Pre-treatment CBCT revealed midpalatal suture maturation stage “D.” The appliance was placed, and activation was initiated as per the manufacturer’s protocol, as elucidated in Case 1. The expansion appliance opened, but there was no clinical sign of suture opening. The repeat CBCT after 10 days of activation revealed that the implants traversed transversely through the palatal bone, leaving a thin radiolucent streak in the palate. This proved that MSE II expanded, but the palatal bone could not offer sufficient resistance to open the palatal suture, resulting in failure. The salient characteristics of the case are presented in Figures 3 and 4, and the details of palatal bone height and density of bone cross-section are shown in Table 1.
Pre- and Post-expansion Intraoral Occlusal Photographs (a and b) and CBCT (c and d), Respectively, of Case 2.
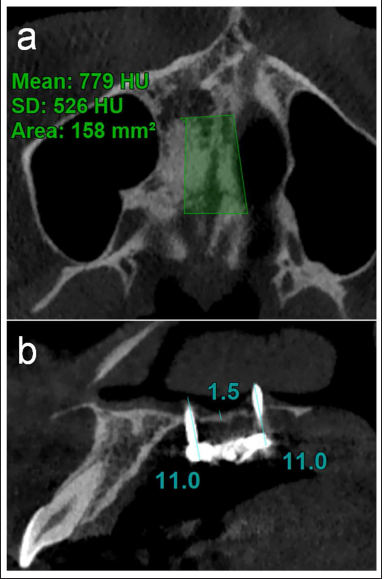
CBCT Showing Bone Density (a) and Palatal Bone Thickness and Bicortical Engagement (b) in Case 2.
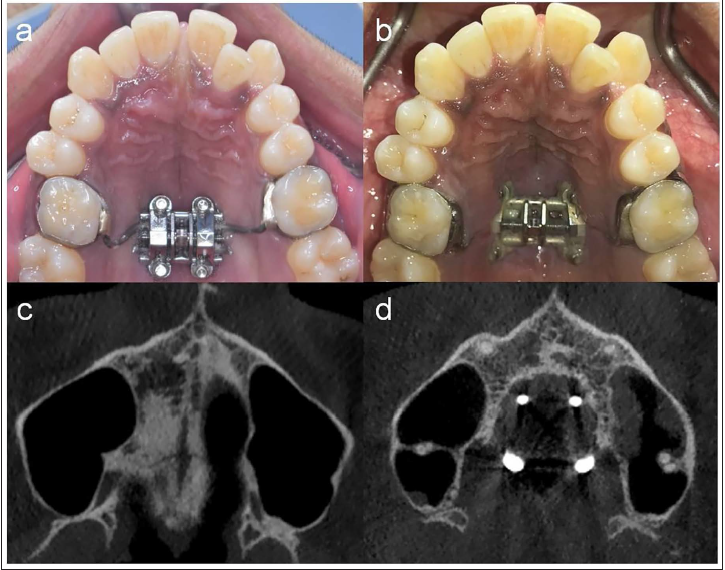
The pre- and post-treatment/post-expansion phase frontal intraoral results for Cases 1 and 2 are shown in Figure 5. The treatment for Case 1 was successfully completed post-MARPE phase, while for Case 2, following the failure of MARPE, alternative modality was adopted for treatment.
Pre- and Post-treatment/Post-expansion Intraoral Frontal View in Cases 1 and 2, Respectively.

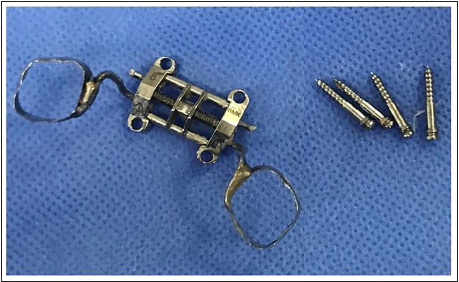
Intact, Unbent TAD’s on Removal Post-expansion in Case 2.
Discussion
The concept of MSE is based on directing the forces against the buttress bone to achieve the midpalatal suture opening by placing the appliance in posterior palate between first and second molars. This usually takes the appliance to the region with thinnest palatal bone. The palatal bone thickness and density may vary in different facial patterns and different ethnicities, which can be a limitation in the use of this technique. This placement is usually in contravention to the T-zone, which is the palate region with the best cortical bone quality.6, 7 The bone density in Case 2 was approximately half of the first case, though palatal bone height was similar (Table 1). In both cases, the appliance had bi-cortical engagement, never tilted, and on appliance removal, the temporary anchorage device (TAD) screws were intact and unbent while being expanded8, 9 (Figure 6); the usual reasons cited for failure. Yet, it resulted in failure in second case. In the second case, the opening of MSE II on activation, increase in space between the TADs, and embedding of the molar connecting arms of the appliance in the palatal soft tissue laterally are testimony to appliance activation, but lack of appearance of diastema, increase in arch width, and minimal patient discomfort during expansion are proof of the inadequate resistance offered by palatal bone. In the first case, the appliance could not be placed as per recommendation and was ahead of its usual position, where the bone density was better, though thickness was same, which may have resulted in successful suture opening. Though it needs further investigation, as a clinical guideline, MSE-II should be avoided in palate with bone density below 1,000 HU, where TADs of MSE II are to be placed, to prevent inadvertent failure in Indian patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the Institutional Ethical Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
It is hereby submitted that informed consent was obtained by the patient/s in writing on prescribed format, and they do not have any objection to the work being submitted for publication.