
Abstract
Objective
To assess the association between hypodontia and skeletal malocclusions in orthodontic patients.
Materials and Methods
This cross-sectional study comprised of orthodontic records of 40 hypodontic patients (12 males and 28 females) and 120 non hypodontic patients (58 males and 62 females) as control group matched for gender and age with the study sample who came to the orthodontic department for their treatment were selected. Orthopantamograms were evaluated for hypodontia, whereas lateral cephalogram were traced to determine the cephalometric parameters. The association between different classes of skeletal malocclusion and hypodontia was determined using Pearson’s Chi-square test and the cephalometric parameters between patients with hypodontia and without hypodontia (controls) were assessed using Student’s t-test.
Result
In hypodontic group, 19 (47.5%) patients had skeletal class II, 18 (45%) patients had skeletal class I, and only 3 (7.5%) patients had skeletal class III malocclusions. Whereas in non-hypodontic group (control group), 86 (53.75%) patients had skeletal class II, 63 (39.38%) patients had skeletal class I, and 11 (6.87%) patients had skeletal class III malocclusions. There was no statistical difference between hypodontia and different skeletal classes of malocclusions (p = .654). Cephalometric parameters between the control group and hypodontic group did not reveal any significant difference (p > .05).
Conclusion
This study did not find any association between different classes of skeletal malocclusions and hypodontia. The cephalometric skeletal parameters were not significantly different in hypodontic and control group. It is suggested that the patients having hypodontia will be evaluated on an individual basis for their treatment.
Introduction
Hypodontia is a developmental condition in which there is an absence of one or more teeth, when excluding third molars. 1 The prevalence of hypodontia varies from 2.3% to 15.7% in different ethnic groups, genders, and locations. 2 The prevalence in Nepalese orthodontic patients is 7.48% and the common missing teeth was upper lateral incisor. 3
Homeobox gene those are contained in the neural crest cells might undergo some genomic mutations leading to faulty signaling pathways, which ultimately affects the midface and teeth development.4, 5 Some studies have found significant association between hypodontia and sella turcica bridging.6, 7
Many studies revealed that the patients with hypodontia have different craniofacial features when compared with the normal.1, 8, 9 Cephalometric studies showed a higher chance toward a Skeletal III pattern having retruded maxilla and progranthic chin in hypodontia patient. It also showed the reduced jaw lengths and reduced mandibular length to cranial base length ratio.10, 11 Some studies revealed reduced mandibular plane angle, anterior cranial base-mandibular plane, and Frankfort-mandibular angles along with the short upper and lower facial heights.1, 8, 12–14
Although some studies have evaluated the relation between some specific craniofacial features and tooth hypodontia but the results are controversial.8, 10, 15–18 Some authors did not find an association between tooth hypodontia and malocclusions,15, 16 while others observed association or tendency with skeletal Class II malocclusion.17, 18 On the other hand, some studies revealed that tooth hypodontia had tendency with the skeletal Class III malocclusion.8, 10, 19, 20 Along with this, no such type of study has been carried out in population of Nepal. Therefore, this study aimed to assess the association between hypodontia and skeletal malocclusions in orthodontic patients of Kathmandu, Nepal.
Materials and Methods
This cross-sectional study comprised of orthodontic records of the patients who came for their treatment were collected from the orthodontic department of Tribhuvan University Teaching Hospital, Kathmandu, Nepal.
Study Population
Orthodontic records of 40 patients from the age of 10 to 35 years (28 females and 12 males; mean age of 13.9 ± 2.5 years) who came to orthodontic department for their treatment and must be affected by dental hypodontia having good quality of orthopantamograms and lateral cephalograms were included.
Patients with a history of orthodontic treatment, craniofacial anomalies/congenital syndrome, systemic disease and missing teeth due to tooth decay, avulsions, or extracted were excluded.
Control Group
The control group comprised of 120 subjects matched for age and gender without hypodontia (58 males and 62 females; mean age of 14.1 ± 1.8 years) were randomly selected from those referred for orthodontic treatment at the same place and time frame. The exclusion criteria were the same as for the study population.
Determination of Hypodontia
Orthopantamograms were examined by a single operator. In orthopantamogram, when the mineralization of crown was not identified, then it was diagnosed as congenitally missing. Orthopantomogram was assessed on a computer screen with a resolution of 1,280 × 800 pixels. Patient’s age, gender, number of teeth which is missing, and its location were recorded.
Determination of Skeletal Parameters
Tracing and analysis of pretreatment lateral cephalometric radiographs were done digitally using Vistadent OC 1.1 software program (GAC International Inc, Bohemia, New York, USA) to obtain the craniofacial morphology details of 15 cephalometric skeletal parameters related to maxilla, mandible, maxillomandibular relation and vertical relation (Figure 1). Parameters related to maxilla were sella-nasion to point A (SNA), N perpendicular to point A (N perp. A), and effective maxillary length (Co-A), whereas cephalometric parameters related to mandible were sella-nasion to point B (SNB), N perpendicular to pogonia (N perp. Pog), and effective mandibular length (Co-Gn). The cephalometric parameters related to maxillomandibular relation were ANB angle (ANB), Wits appraisal (Wits), and maxillomandibular difference, whereas parameters related to vertical relation were Frankfort mandibular plane angle (FMA), Mandibular plane angle (SN-GoGn), lower anterior facial height (ANS-Me), Articular angle (SArGo), Sella angle (NSAr), and Gonial angle (ArGoMe).
Digital Measurements of Craniofacial Morphology on Lateral Cephalogram.

The entire sample was classified as skeletal Class I, Class II, and Class III malocclusions based on ANB angle, Wits, and maxillomandibular difference. At least two out of three parameters showed the same inference to diagnose the case of different classes of skeletal malocclusion.
Statistical Analysis
The data collected were transferred into an MS Excel sheet. The dataset was analyzed using SPSS Statistics Version 21.0 (IBM Corp., Armonk, New York, USA). The confidence level was set at 95%. Descriptive statistics were used to represent skeletal malocclusions and different cephalometric parameters in hypodontic and non hypodontic patients. The association between different classes of skeletal malocclusions and hypodontia was determined using Pearson’s Chi-square test. The cephalometric parameters between patients with and without hypodontia were analyzed with Student’s t-test.
Results
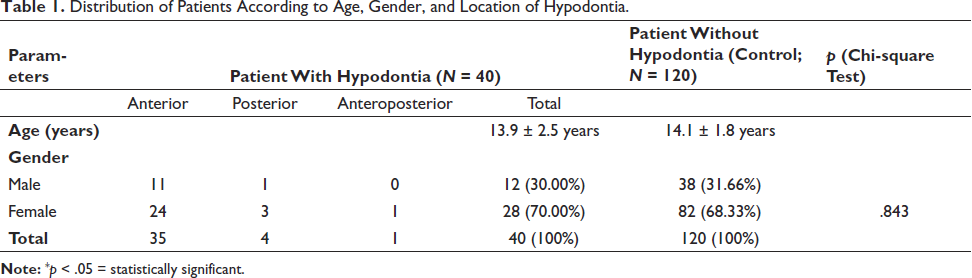
This study comprised of 40 patients with hypodontia, out of which 12 were male and 28 were female, whereas 120 patients without hypodontia regarded as control group consists of 38 males and 82 females. Out of 40 hypodontic patients, 35 patients had missing teeth in only anterior region referred as anterior hypodontia, 4 had missing teeth in only posterior region referred as posterior hypodontia, whereas 1 patient had missing teeth both in anterior and posterior region referred as antero-posterior hypodontia.
The distribution of patients with hypodontia and without hypodontia according to age, gender, and location of hypodontia in the arch is demonstrated in Table 1. There was no significant difference in male and female distribution in both the groups as stated by the Chi-square test (p = .843).
Distribution of Patients According to Age, Gender, and Location of Hypodontia.
In hypodontic group, 19 (47.5%) patients had skeletal class II, 18 (45%) patients had skeletal class I, and 3 (7.5%) patients had skeletal class III malocclusions. Whereas in control group (non hypodontic group), 86 (53.75%) patients had skeletal class II, 63 (39.38%) patients had skeletal class I and 11 (6.87%) patients had skeletal class III malocclusions (Figure 2).
Distribution of Skeletal Malocclusions in Both Groups.
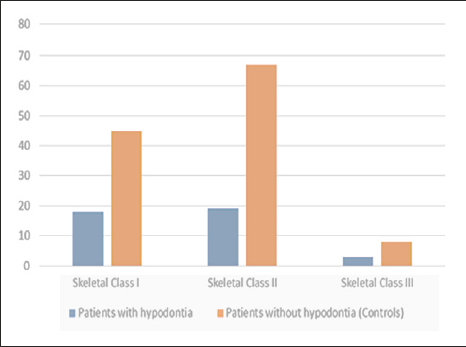
Chi-square test showed that there was no statistical difference between hypodontia and different classes of skeletal malocclusions (p = .654) (Table 2).
Distribution of Patients According to Different Classes of Skeletal Malocclusions.

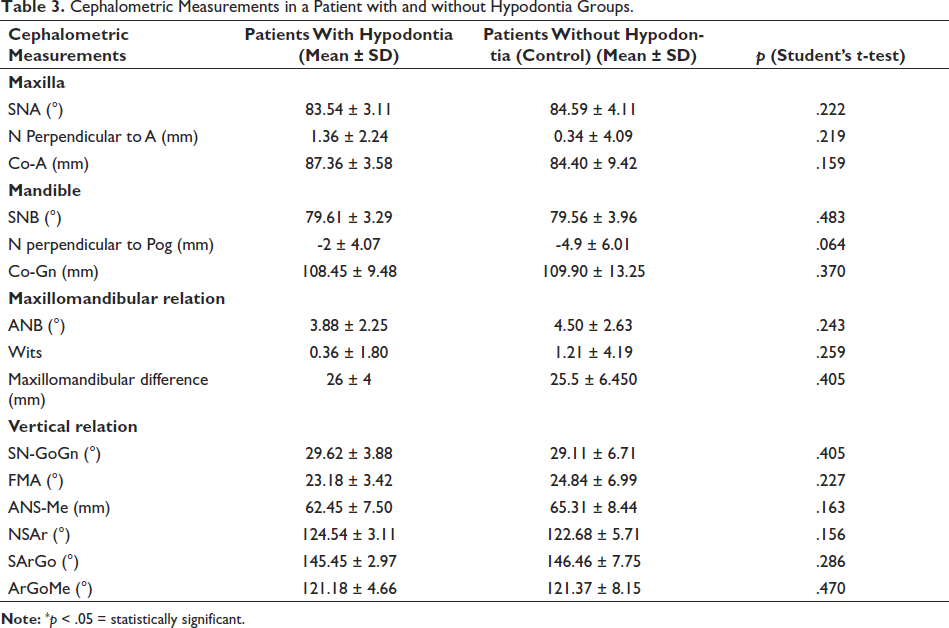
The cephalometric parameters between hypodontic and non hypodontic patients are demonstrated in Table 3 and these parameters were assessed using Student’s t-test. It showed no statistically significant difference in the cephalometric parameters between hypodontic group and control group (p > .05). However, SNA angle, ANB angle, and ANS-Me (lower facial height) are lesser in hypodontic group compared to control group.
Cephalometric Measurements in a Patient with and without Hypodontia Groups.
Discussion
This study evaluated the relationship between different classes of skeletal malocclusions and hypodontia by using two groups: one group consisted of patients with hypodontia, whereas another group consisted of patients without hypodontia as a control group. Reason for selecting 120 patients in control group is based on previous studies that states at least three times the size of control to have good statistical comparison. 7
Tooth agenesis is the developmental anomaly that can be diagnosed clinically when it is not seen in the oral cavity but confirmed by radiographic examination when dental crypt is not visible in the radiograph. 21 Agenesis leads to hypodontia. Hypodontia might be located either in the anterior region only or in the posterior region only or in the anteroposterior region.
It is believed that Homeobox genes have a crucial role in regulating craniofacial morphogenesis and tooth development. In mice, it was found that expression of MSX 1 and MSX 2 is necessary for direct epithelial-mesenchymal interactions which initiate the formation of tooth. 22 Along with this, MSX 1-deficient mice showed tooth agenesis, abnormalities of the malleus, frontal, nasal and parietal bones and cleft of secondary palate, which suggests that tooth agenesis was related genetically to the development of maxillary complex and cranium. 23 It is said that there is some genetic difference in various populations regarding tooth agenesis. 24
The findings of this study revealed that in both groups, most of the patients had skeletal Class II malocclusion followed by skeletal Class I malocclusion and least patients were having skeletal Class III malocclusion. But there was no statistically significant difference between different classes of skeletal malocclusions in hypodontic and non-hypodontic patients (p > .05).
In this study, while comparing the 20 different cephalometric parameters between hypodontic and non-hypodontic patients, it showed that there was no significant difference in those parameters between both the groups. Although cephalometric parameters showed less mean value of SNA angle, ANB, angle and ANS-Me (lower facial height) in hypodontic group compared to control group, there was not statically significant difference in these parameters among two groups (p > .05), which is similar to the study by Taju et al. 25 Contradictory to this finding, study by Costa et al. showed statistically significant lesser ANB angle in hypodontic patients in compared patients without hypodontia. 26
Other studies also suggested that skeletal Class III malocclusion has been associated with the patients with hypodontia.8, 10, 19, 20 Reason might be that it is hypothesized that same genes are involved in the etiology of both conditions. Hirukawa et al. 27 also suggested that agenesis of upper tooth might be involved in skeletal Class III malocclusion.
Reasons for lesser anterior lower facial height in hypodontic group could be hypothesized that increased masticatory load on lesser teeth lead to increased occlusal wear of the existing dentition and/or intrusion. Whereas another theory suggested that hypodontic patients has less development of the alveolar process in vertical plane, which ultimately affects the vertical development of lower third of face. 25
This study showed no statistically significant difference in the maxillary length (Co-A) between patients with hypodontia and in control group. Contradictory to this, the study by Endo et al. revealed shorter maxillary length in patients with hypodontia compared to normal patients. 28 Kreczi et al. stated that tooth agenesis might affect the sagittal development of a jaw. 29
Results of this study and previous studies suggested that patients with hypodontia can be assessed on an individual basis for the treatment need.
This study was carried out among the orthodontic patients of only one tertiary health care center rather than the general population. Along with this, ethnicity was not taken into account. Hence, it is recommended to conduct multicenter studies involving large samples of diverse population along with healthy controls, as it might give a better picture.
Conclusion
Hypodontia are more common in the anterior region of jaw while excluding third molars. This study did not find any association between hypodontia and different classes of skeletal malocclusions. The cephalometric skeletal parameters were not significantly different in hypodontic and control group. It is suggested that the patients having hypodontia will be evaluated on an individual basis for their treatment.
Footnotes
Data Availability Statement
Data can be made available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the institutional review committee of the Institute of Medicine [Ref. 551 (6-11) E 2 ,078/079] before conducting this research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.