
Abstract
Objective
The aim of this study was to evaluate and compare the stress along the root surfaces of anterior maxillary dentition during retraction in labial and lingual mechanics with varying level of bone support.
Materials and methods
Eight 3D finite element models (FEM) having 340,215 nodes and 211,543 elements were created with normal periodontium and different levels of alveolar bone loss; four with labial brackets and four with lingual brackets. Sliding mechanics were simulated as en masse retraction of the anterior dentition. The equivalent stresses along the roots of six anterior maxillary teeth were measured in all the models.
Results
Equivalent stresses in pascals (Pa) generated at the root surfaces of central incisors are always higher in labial technique (right: 4.6013 × 10−2; left: 7.1158 × 10−2) and of canines (right: 10.003 × 10−2; left: 16.789 × 10−2) are always higher in lingual technique.
Conclusion
In labial technique, central incisor roots are experiencing maximum stress, which might be the explanation of commonly seen higher incidence of root resorption in them during en masse retraction. In lingual technique, canine roots are experiencing higher stresses as compared to other anterior teeth during en masse retraction. Equivalent stresses generated at the root surfaces of canines are more irrespective of the alveolar bone loss in lingual technique.
Introduction
Lingual orthodontics has become a well-recognized discipline in the light of growing demand for esthetics nowadays. Lingual appliances have their own separate biomechanics, distinct from that of conventional labial orthodontics. 1 In terms of indirect lingual bracket bonding, new archwire materials, and computerized planning systems, the lingual technique has become simpler and precise. 2 For aesthetic reasons, it is more common in contemporary orthodontics to do en masse retraction of the six anterior teeth as a unit in both the labial and lingual technique, so as not to create any visible space between canines and lateral incisors during speech or smile.
Ultimately, the stress generated in response to the retraction force along the root surfaces dictates the various tissue reactions of the teeth, periodontal ligament, and alveolar bone. It is very difficult to measure clinically the stress induced at various locations on the root surfaces in healthy as well as in various periodontally compromised bone depths in different types of orthodontic tooth movement. A variety of traditional analytical and experimental methods for analyzing dental stresses, such as photoelasticity, interferometric holography, and strain gauges have been used to discuss the mechanism of orthodontic tooth movement, but they were unable to clarify the different tissue responses to all types of stress levels. 3
Finite element modeling (FEM) is a mathematical method in which the shape of complex geometric objects and their physical properties are computer-constructed. The FEM analysis provides the orthodontist with quantitative data that can extend the understanding of physiologic reactions that occur within the dentoalveolar complex. 4 In order to take advantage of this powerful computational tool, this study uses three-dimensional (3D) finite element models of the upper anterior dentition in order to map and compare stress produced by en masse retraction performed with lingual and labial appliances in simulated varying bone depth in both the situations.
Previous literatures have described stress generation in response to orthodontic force on canine, 5 premolar, 6 central,7–9 and lateral incisors 9 individually. Comparison of stress generation during en masse retraction in lingual and labial technique has also been published. 10 Similar data in situations such as different levels of bone loss are limited. Lombrdo et al. in 2014 have done a 3D FEM of each lower tooth and constructed and located as appropriate to Roth’s prescription. They concluded that lingual and labial mechanics provoke very different stress patterns and consequently tooth movements. The stress exerted by the lingual bracket system was always greater than that generated by the labial appliance, except at the molars. 11 Zargham et al. have used finite element method to evaluate the long-term orthodontic tooth movement considering bone remodeling process and in the presence of alveolar bone loss using finite element method. This study suggested that applied force magnitude can be remarkably reduced in the patients with reduced bone height, particularly in the cases with extreme bone loss. 12 Bouton et al. in 2017 have presented tooth movement in a more clinically exact fashion with the use of new IT tools and imaging systems (cone-beam). The principle was to monitor tooth movement by obtaining optical impressions at each stage of treatment. FE analysis was correlated with the clinically observed displacement. 13
Material and Methods
The study has been approved by the Institutional Ethical Committee, Institute of Medical Sciences & Sum Hospital IEC Code No. IMS SH/IEC/2015/210/36. Finite element models of the maxillary anterior dentition from 13 to 23 with acceptable amount of leveling and alignment were developed. Computed tomography (CT) scan (head and neck) of one patient with apparently well leveled and aligned maxillary anterior teeth with healthy periodontium and no radiographic evidence of periodontal bone loss was taken from Radio Diagnostic Department of SUM Hospital, SOA Deemed to be University, Bhubaneswar. There was no rotation, crowding, spacing, extensive restorations, prosthesis, or any type of dental deformity present in that patient.
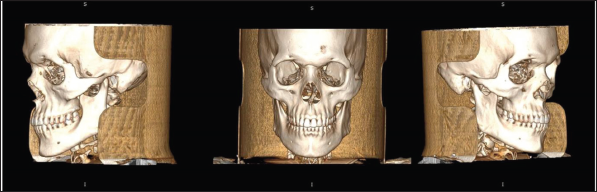
CT scan data in the DICOM (0.208×0208×2.0) format were collected from the bone and was scanned using CT scanning equipment (specs) as done by previous researchers14, 15 (Figure 1).
Three-dimensional (3D) Presentation of the CT Scan of the Patient Chosen for the Model Construction in DICOM Viewer.
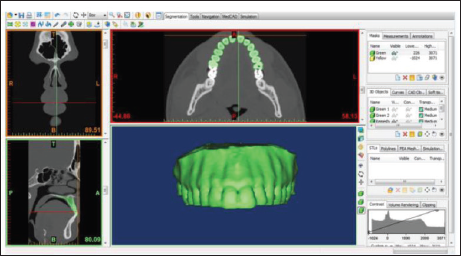
Geometric models of maxillary anteriors from canine to canine along with their supporting structures, that is, alveolar bone and periodontal ligament were first constructed using reverse engineering technique. (CT scan of the maxilla was taken as reference.) CT scan of the maxilla was taken into Mimics 10 software to create the 3D models (Figures 2–4). SOLIDWORKS 16 software was used to remesh the 3D models. The material properties of periodontal ligament (PDL) and all the dentoalveolar structures were assumed to be isotropic and homogeneous as in the earlier studies. 6
Segmentation of Maxillary Arch Being Processed in MIMICS 10 Software.
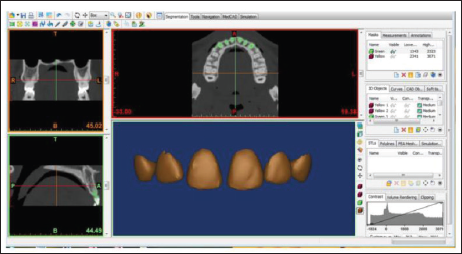
Segmentation of Individual Tooth Being Processed in MIMICS 10 Software.
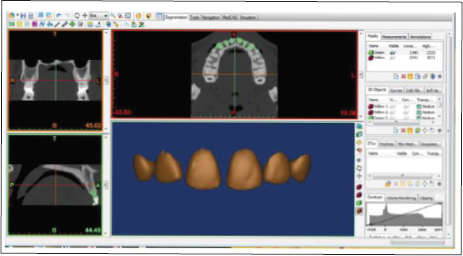
Segmentation of Enamel Being Processed in MIMICS 10 Software.
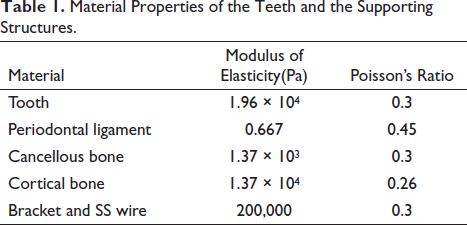
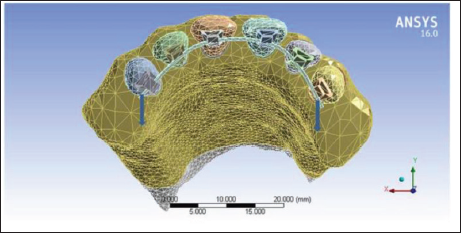
PDL of 0.25 mm width was constructed around the root surfaces of all maxillary anterior teeth, as the thin PDL layer could not be extracted from the CT scan data and the thickness of the alveolar cortical bone was taken as was in CT scan. Young’s moduli and Poisson’s ratios for the materials were assumed as the average values reported in the literature (Table 1). 9 Finite element model of the maxillary anteriors from canine to canine along with other supporting structures consisting of 340,215 nodes and 211,543 tetrahedral elements were imported into ANSYS 16 software for analysis (Figures 5 and 6). The minimum edge length of the model was 2.3013 × 10–4 mm. Linear elastic behavior was assumed for all the materials.
Material Properties of the Teeth and the Supporting Structures.
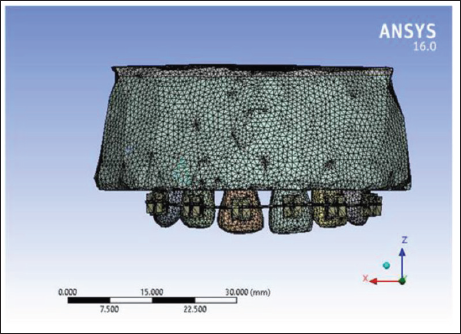
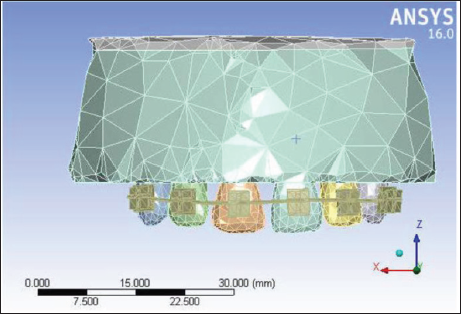
Mesh Processing Being Done in ANSYS 16.0 Software.
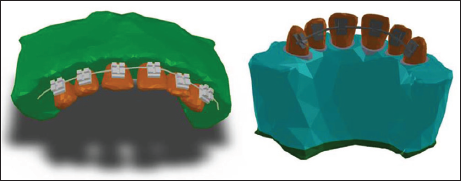
Assembling Done in SOLIDWORKS 16 Software.
The load and boundary conditions were applied in the solution stage, that is, solving each load case. Virtual models of MBT Prescription 0.018-inch DENTAURUM EQUILIBRIUM® 2 labial (DENTAURUM GmbH & Co. KG; Turnstraße 31, 75228 IChland) and Ormco 8th Generation lingual (ORMCO CORPORATIONE, Orange, California, USA) brackets; 0.016 × 0.022-inch SS labial and lingual archwires were constructed.
Finite element model of the whole maxilla with the anterior teeth from alveolar crest to nasal floor was generated. The finite element model has been extended up to 10 mm from the apex of anterior teeth into the bone making an artificial boundary of the maxilla.
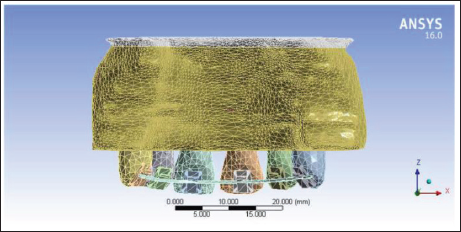
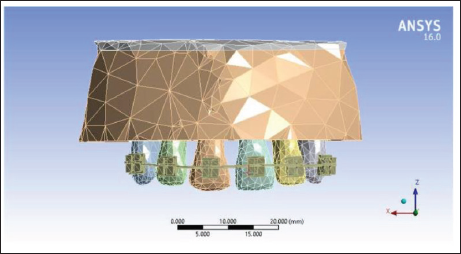
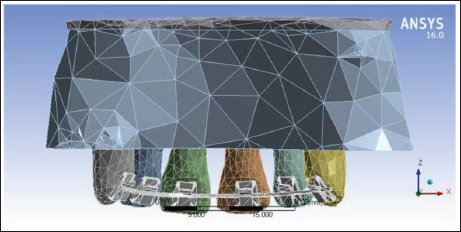
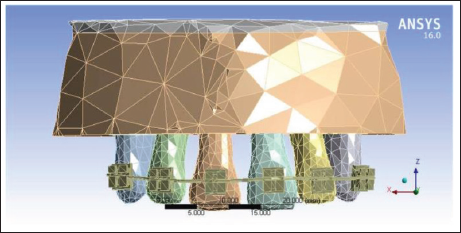
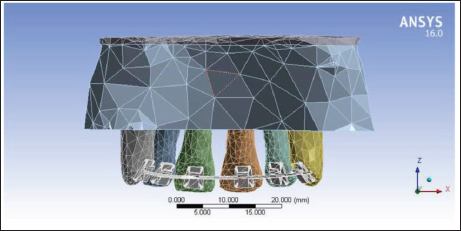
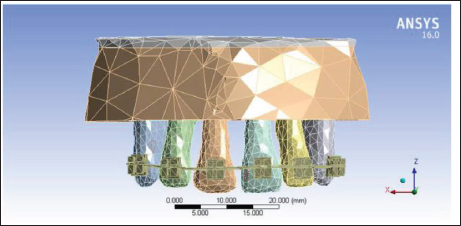
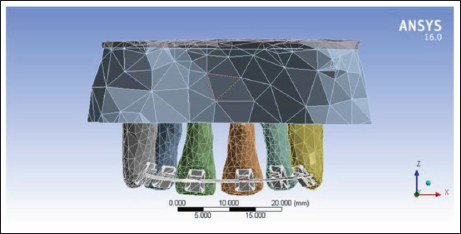
In the same process, total four sets of models have been constructed, that is, with normal periodontium (Figures 7 and 8), with 2 mm alveolar bone loss (Figures 9 and 10), with 4 mm alveolar bone loss (Figures 11 and 12), and with 6 mm alveolar bone loss (Figures 13 and 14). Each set has two models of same alveolar bone height: one with labial brackets and the other with lingual brackets. Total eight models were created. Four models had 0.018-inch slot MBT prescription labial brackets, placed as close to the ideal position as possible on the six anterior teeth and 0.016 × 0.022 SS stainless steel archwire placed in the slots. Similarly, other four models had 0.018-inch slot lingual brackets and 0.016 × 0.022 SS archwire. The wire size selected is the maximum used in most lingual appliance systems.
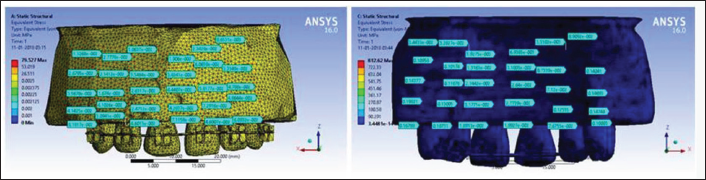
Finite Element Model of Maxillary Six Anterior Teeth with Normal Alveolar Bone Height and Labial Brackets.
Finite Element Model of Maxillary Six Anterior Teeth with Normal Alveolar Bone Height with Lingual Brackets Placed.
Finite Element Model of Maxillary Six Anterior Teeth with 2 mm Alveolar Bone Loss with Labial Brackets Placed.
Finite Element Model of Maxillary Six Anterior Teeth with 2 mm Alveolar Bone Loss with Lingual Brackets Placed.
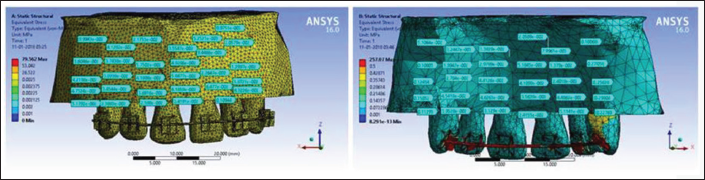
Finite Element Model of Maxillary Six Anterior Teeth with 4 mm Alveolar Bone Loss with Labial Brackets Placed.
Finite Element Model of Maxillary Six Anterior Teeth with 4 mm Alveolar Bone Loss with Lingual Brackets Placed.
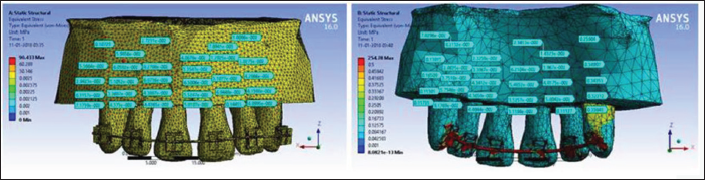
Finite Element Model of Maxillary Six Anterior Teeth with 6 mm Alveolar Bone Loss with Labial Brackets Placed.
Finite Element Model of Maxillary Six Anterior Teeth with 6 mm Alveolar Bone Loss with Lingual Brackets Placed.
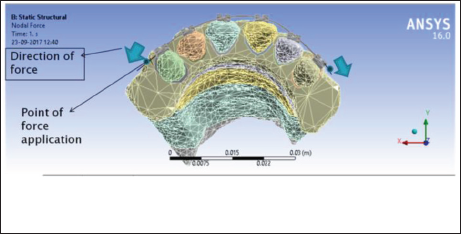
All models had boundary conditions defined at all peripheral nodes of the bone giving them 0° of movement in all directions. Link elements were defined between the nodes on the mesial and distal ends of the bracket to simulate bracket ligation and prevent the archwire coming out of the slots. To simulate the friction force, contact elements were defined between contact surfaces of the archwire and bracket slots assuming a friction coefficient of 0.2. Sliding mechanics were simulated as en masse retraction of the anterior dentition applying a 120 g 16 (1.1 N) distal force on both sides of the dentition (Figures 15 and 16). The point of application of force is 1 mm distal to the canine brackets bilaterally in all the models.
Point of Force Application in Labial Technique.
Point of Force Application in Lingual Technique.
The stress measurements were done along the root surfaces in both labial and lingual technique models at:
The level of alveolar bone crest, 2 mm below the alveolar bone crest, 4 mm below the alveolar bone crest, 6 mm below the alveolar bone crest, and The root apex.
Results
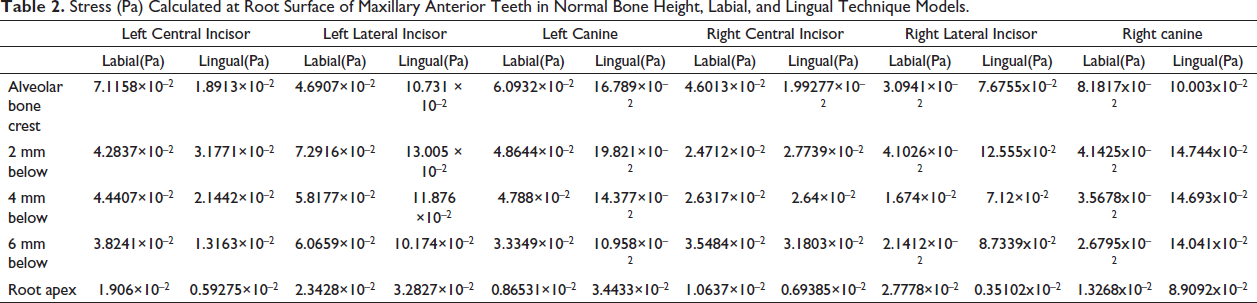
The equivalent stress measurements at different levels of root surfaces of individual teeth are collected from the analysis of all eight models using ANSYS16 software and are presented in Tables 2–5.
Stress (Pa) Calculated at Root Surface of Maxillary Anterior Teeth in Normal Bone Height, Labial, and Lingual Technique Models.
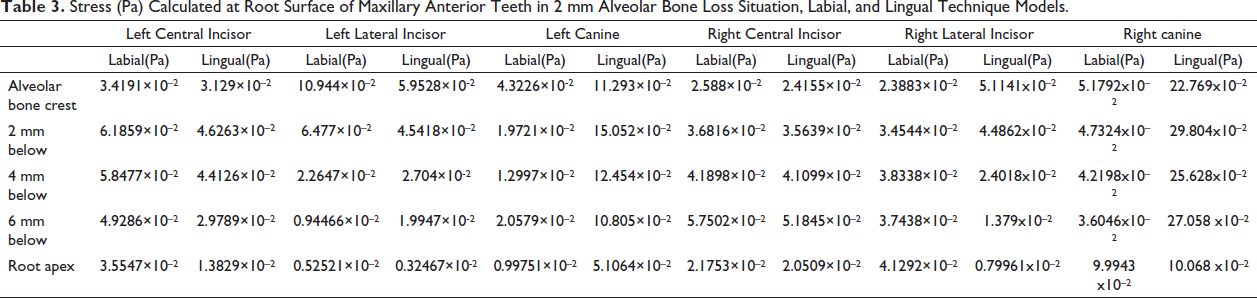
Stress (Pa) Calculated at Root Surface of Maxillary Anterior Teeth in 2 mm Alveolar Bone Loss Situation, Labial, and Lingual Technique Models.
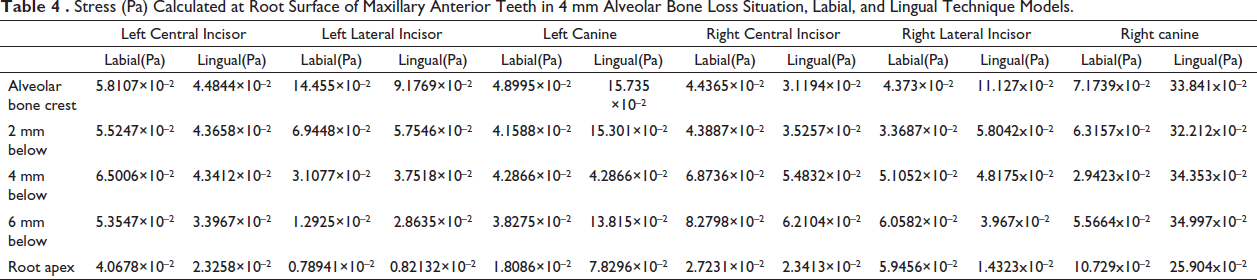
Stress (Pa) Calculated at Root Surface of Maxillary Anterior Teeth in 4 mm Alveolar Bone Loss Situation, Labial, and Lingual Technique Models.
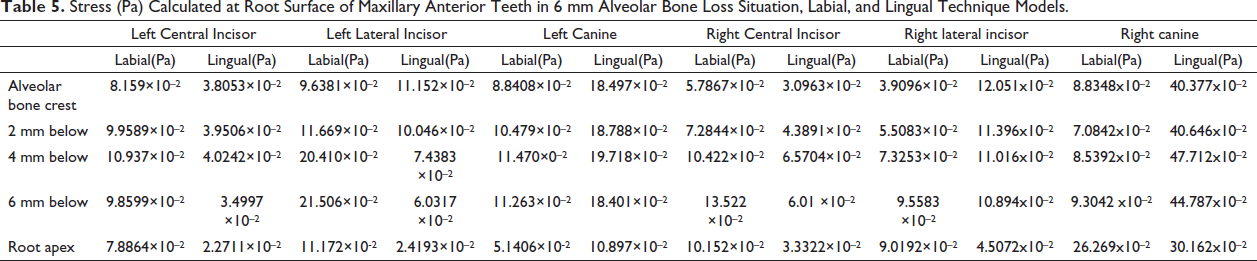
Stress (Pa) Calculated at Root Surface of Maxillary Anterior Teeth in 6 mm Alveolar Bone Loss Situation, Labial, and Lingual Technique Models.
Normal Bone Height Model
For both the central incisors, the stresses are higher in labial than in lingual technique (Figure 17). At all the level of root surfaces of both lateral incisors, equivalent stress generated is higher in lingual than in labial technique. At all the level of root surfaces and at the root apex of both the canines, equivalent stress generated is significantly higher in lingual than in labial technique models.
Equivalent Stress Calculated on the Root Surfaces of Maxillary Six Anterior Teeth with Labial and Lingual Brackets Placed.
2 mm Alveolar Bone Loss Model
At all the levels of root surfaces and at the root apex of both the central incisors, equivalent stress generated is higher in labial than in lingual technique (Figure 18). At all the level of root surfaces of left lateral incisor, equivalent stress generated is higher in labial than in lingual technique. In right lateral incisor, at the level of alveolar bone crest, 2 mm below the level of alveolar bone crest, and at the root apex, equivalent stress generated is higher in lingual than in labial technique. At 4 and 6 mm below the alveolar bone crest, stress generated is higher in labial than in lingual technique.
Equivalent Stress Calculated on the Root Surfaces of Maxillary Six Anterior Teeth (with 2 mm Alveolar Bone Loss) with Labial and Lingual Brackets Placed.
4 mm Alveolar Bone Loss Model
At all the levels of root surface and at the root apex of both right and left central incisors, equivalent stress generated is higher in labial than in lingual technique (Figure 19). In left lateral incisor, at the level of alveolar bone crest, at 4 and 6 mm below the level of alveolar bone crest and at the root apex equivalent stress generated is more in lingual than in labial technique. At 2 mm below the level of alveolar bone crest, equivalent stress generated is more in labial than in lingual.
Equivalent Stress Calculated on the Root Surfaces of Maxillary Six Anterior Teeth (with 4 mm Alveolar Bone Loss) with Labial and Lingual Brackets Placed.
In right lateral incisor, at the level of alveolar bone crest and at 2 mm below the level of alveolar bone crest, equivalent stress generated is significantly higher in lingual than in labial technique. At 4 mm, 6 mm below the alveolar bone crest and at the level of root apex, equivalent stress generated is higher in labial than in lingual technique.
6 mm Alveolar Bone Loss Model
At all the levels of root surface and at the root apex of both right and left central incisors, equivalent stress generated is higher in labial than in lingual technique (Figure 20). In left lateral incisor, at all the levels of root surfaces, equivalent stresses generated are higher in labial than in lingual technique, but at the alveolar crest level, results are opposite. In right lateral incisor, at all the levels of alveolar bone crest, equivalent stress generated is significantly higher in lingual than in labial technique, but at the root, apex results are opposite.
Equivalent Stress Calculated on the Root Surfaces of Maxillary Six Anterior Teeth (with 6 mm Alveolar Bone Loss) with Labial and Lingual Brackets Placed.
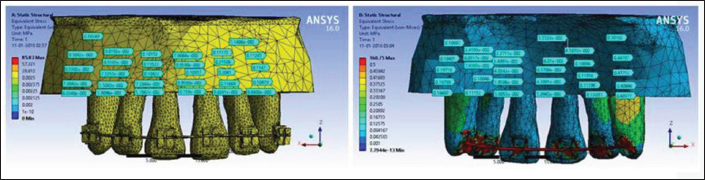
In the labial technique models, as the vertical bone loss is increasing, equivalent stresses generated are also increasing in the central incisor root surfaces. In the lingual technique models, magnitude of stresses observed along the root surfaces of canines are more than the lateral and central incisors irrespective of the bone level status.
Discussion
In contemporary orthodontics, en masse retraction of six anterior teeth is a preferred method in both labial and lingual techniques. In labial method, individual canine retraction followed by retraction of four incisors does not necessarily provide any advantage, except in certain cases, for example, crowding or transposition.16–19 In lingual method, en masse retraction is always preferred because the inset bend of the archwire distal to the canine would hinder the canine movement and from aesthetic point of view, space produced distal to lateral incisor after canine retraction would arise patient dissatisfaction.7, 10
The stress levels in different periodontally compromised conditions differ significantly, which demands altered biomechanical approach. That is why we have created models with various levels of bone loss and studied the stress levels in both labial and lingual situations.
Finite element analysis makes it possible to calculate the stresses on the root surfaces, which are close to accurate value, occurring during orthodontic tooth movement. 20
Normal Bone Height labial and lingual Models
At all the levels of root surfaces from alveolar bone crest to root apex, the left and right central incisors are showing higher equivalent stresses in labial technique than in lingual. In the labial technique model, the stress at the level of alveolar bone crest is highest, decreasing toward the root apex. Because we have simulated bodily tooth movement, stress concentrated is more at the alveolar crest as described by Rudolph et al. 7
At all the level of root surfaces from alveolar bone crest to root apex, the left and right lateral incisors are showing higher equivalent stresses in lingual technique than labial, which is supported in the previous study by Lombardo et al. 10 Lombardo et al. explained that due to smaller inter bracket distance in anterior six teeth region of lingual appliance, the load becomes greater even if the same size archwire is used, as in labial technique. 21
At all the level of root surfaces, the left and right canines are showing higher equivalent stresses in lingual technique than in labial, which is supported by the previous study. 10 In both the canines, the highest equivalent stresses generated are observed at 2 mm below the level of alveolar bone crest in lingual technique. In labial technique, maximum stress was concentrated at the level of alveolar bone crest and decreased toward the root apex in both the canines. According to McGuiness et al., 5 this type of stress distribution is seen in case of tipping force acting on a tooth.
Hence, we may have to add torque in the canine region to create additional couple force, which will result in translational tooth movement. In lingual technique, the stresses observed along the root surfaces of canines are more than the lateral and central incisors.
2 mm Alveolar Bone Loss labial and lingual Models
Stresses generated on the root surfaces of both left and right central incisors are showing higher values in the labial technique than in lingual technique models. The stress along both the central incisor roots in this model is higher than normal bone model exception being the level of alveolar bone crest.
For canines, the observations are similar to the labial and lingual normal bone models. Stresses generated are higher in the canines of this model than the normal bone height model. This is probably because of loss of 2 mm of bone as described by Kamble et al. 8
4 mm Alveolar Bone Loss Labial and Lingual Models
At all the levels of root surfaces from alveolar bone crest to root apex, the left and right central incisors are showing slightly higher equivalent stresses in labial technique than in lingual, which is also seen in the normal alveolar bone and 2 mm alveolar bone loss models. The stresses along the root surfaces of the central incisor are increasing, as the bone loss is increasing for both the labial and lingual technique. According to Kamble et al., 8 as the length of the root becomes shorter, the crown–root ratio also gets decreased resulting in enhanced load and root surface stress. The altered crown–root ratio due to alveolar bone loss, as seen in this model, enhances the loading on the root, which results in significant stress increase.
The stresses generated in this lingual technique model are more than the stress magnitude of the same technique in normal alveolar bone as well as 2 mm alveolar bone models, for the lateral incisors. Stresses generated in the labial technique in this model are more than the stress magnitude of the same technique in the 2 mm alveolar bone model. These patterns are observed because of increased bone loss as described by Kamble et al. 8
In this model, stresses generated at all the levels of the roots of canines are significantly higher in lingual technique than in the labial. The stresses observed along both the canine root surfaces are more than the lateral and central incisors of this 4 mm alveolar bone loss model. Canines of this model are also showing higher stress values for labial and lingual technique models of 2 mm alveolar bone loss.
6 mm Alveolar Bone Loss Labial and Lingual Models
In the central incisors, similar pattern of stress distribution are observed like previous models. In this model, stresses generated along the root surfaces in the labial technique are significantly higher than the rest of the models with different alveolar bone heights. In the lingual technique, stresses generated at the root apex of central incisors are increasing progressively from normal bone height to 6 mm bone loss model. According to Geramy et al.,22, 23 with the increase in alveolar bone loss, the periodontal membrane area and volume gets reduced; as a result, higher amount of displacements along with significant stress in surrounding structures occur.
So, in both the labial and lingual techniques, force magnitude must be decreased in proportion to the situation in order to maintain physiologically tolerable movements.22, 23
The stress generated at lateral incisors of this model is higher than the other bone height level models along the entire root surfaces as also seen and described previously.
In the canines, a similar pattern of stress distribution is observed like previous models. Stress generated in the labial and lingual technique, at the root apices, of both the canines of 6 mm bone loss model are higher than the stress generated in the canines of other bone level models.
In the labial technique models, as the vertical bone loss is increasing, equivalent stresses generated are also increasing on the central incisor root surfaces, which is also seen in the study by Kamble et al. 8
According to Mehrotra et al., 24 during retraction of anterior teeth with equal magnitude of horizontal retractive force, vertical intrusive force produced in lingual technique is double the amount of horizontal retractive force, whereas labial technique shows almost equal amount of horizontal retractive and vertical intrusive force. As a result, vertical intrusive force produced in lingual mechanics is almost 1.73 times the vertical force magnitude in labial mechanics, which indicates significantly more amount of stress generation in the lingual mechanics. Similar observations are made in various models of our study. So, in lingual technique, the magnitude of force should be kept less than the force applied in the labial technique to achieve desired result without affecting the roots of the anteriors. 24 A recent study by Biswas et al. 26 carried out to compare the stresses along the root surfaces of maxillary anterior dentition during labial and lingual mechanics with varying level of bone support showed similar results as our study.
All the stress levels observed at various sites on root surfaces of all the models are higher than the values advocated by Scwarz 25 and Miura 26 (26 g/cm2 or 0.2549729 × 10–2 Mpa), which can create periodontal ischemia leading to probable root resorption. Hence, the retraction force of 120 gm (1.1 N) per side should be decreased according to our study. As root resorption due to orthodontic force is multifactorial, it may not be very appropriate to suggest a particular force magnitude depending on our study.
In all the models, the lateral incisor teeth shows the most unpredictable pattern of stress distribution, irrespective of bone loss, labial, or lingual technique.
With the rise in adult patients seeking orthodontic treatment, periodontal health becomes a matter of great concern. Controlled predictable optimal forces are required to achieve good treatment results and optimum esthetics.27, 28
Conclusion
Equivalent stresses generated at the root surfaces of central incisors are always higher in labial technique than in lingual irrespective of the alveolar bone height loss. Equivalent stresses generated at the root surfaces of canines are always higher in lingual technique than in labial irrespective of the alveolar bone height loss.
In the labial technique models, as the vertical bone loss is increasing, equivalent stresses generated are also increasing in the central incisors, which suggest that the point of application of force or bracket position has to be changed accordingly and retraction force should be decreased with an increase in bone loss.
In labial technique, the stresses at the root apices of all the teeth are increasing progressively when the bone loss is progressively more than 2 mm, which demands above-mentioned alterations to be made.
Equivalent stresses generated at the root surfaces of canines in lingual technique are more than the stress generated at the root surfaces of central and lateral incisors irrespective of the alveolar bone loss situations.
Footnotes
Acknowledgment
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Technical Advisory Committee and Ethics Committee of Institute of Medical Sciences and Sum Hospital under Siksha ‘O’ Anusandhan (Deemed to be) University.