
Abstract
Introduction
Streptococcus mutans and Lactobacillus count is found to be higher in orthodontic patients and is one of the leading causes of white spot lesion formation. Probiotics are emerging as alternative methods of plaque control.
Aims and Objectives
To determine the effects of different types of probiotics on S. mutans and Lactobacillus levels in saliva of orthodontic patients.
Materials and Methods
A total of 140 subjects were divided into Control group (Group I) with 20 subjects and study group taking probiotics (Group II) with 120 subjects. Saliva samples were taken at baseline (T0), after three weeks (T1), and after six weeks (T2). The samples were diluted and incubated on specific agar media plates. The colonies observed were expressed in colony forming units per milliliter (CFU/ml) of saliva. Group II was further subdivided into six subgroups based on probiotic intake with 20 subjects in each subgroup.
Results
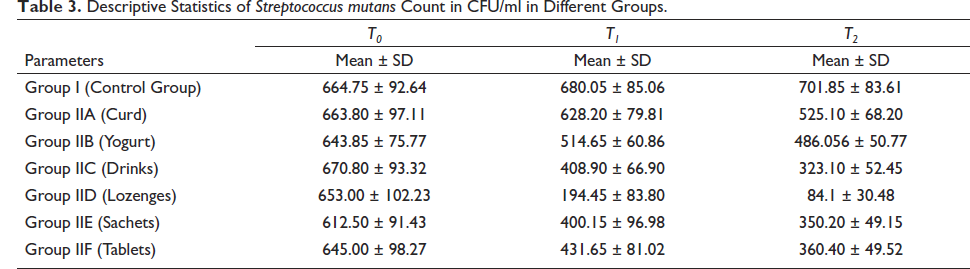
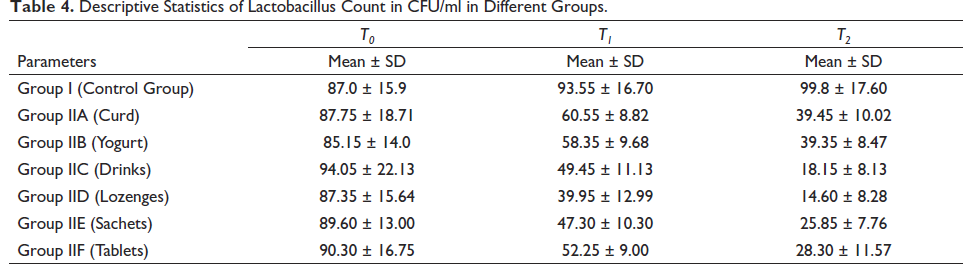
Statistically significant difference was found in salivary microbial counts in all the probiotic groups (p < 0.05). The highest reduction in count of S. mutans (653.00 ± 102.23 CFU/ml to 84.1 ± 30.48 CFU/ml) and Lactobacilli (87.35 ± 15.64 CFU/ml to 14.60 ± 8.28 CFU/ml) was seen in the lozenges group.
Conclusion
Probiotics decrease the number of salivary S. mutans and Lactobacilli and lozenges could be considered for orthodontic fixed appliance patients.
Keywords
Introduction
Fixed orthodontic appliances involve oral hygiene challenges as they are convenient areas for plaque retention due to restricted access and increase the risk of developing caries and inflammatory reactions in gingival tissues.1, 2 The deposition of plaque causes unfavorable changes in the oral environment, such as decreased pH due to organic acid production by acidogenic bacteria which may further result in gingival inflammation, white spot lesions, and dental caries. Level of acidogenic bacteria like Streptococcus mutans and Lactobacillus in the plaque is found to be higher in orthodontic patients and is one of the leading causes of white spot lesion formation. Many methods have been previously employed to reduce the incidence of white spot lesions and gingival inflammation including tooth brushing, topical fluoride application, bleaching, enamel microabrasion, sealants, varnishes, veneers, resin infiltration, use of chlorhexidine, use of xylitol, and so on, but each of them has their own set of advantages and disadvantages. 3
Probiotics are live microorganisms which when administered in adequate amounts confer a health benefit to the host. In order to maintain the oral health, probiotics exert anticariogenic effect on harmful bacteria by prevention of their multiplication and neutralization of the organic acid formed by the sugar metabolism.4, 5 This led to the idea of using probiotics as an alternative during the orthodontic treatment. However, the studies demonstrating the effects of different probiotic products on microbial flora of Streptococcus mutans and Lactobacillus during fixed orthodontic therapy are limited in the literature. Therefore, the aims and objectives of the present study were to evaluate the effects of different types of probiotic intake on salivary levels of S. mutans and Lactobacillus in orthodontic patients.
Materials and Methods
A total of 140 subjects were selected from the patients visiting the Department of Orthodontics and Dentofacial Orthopaedics for fixed orthodontic treatment, which were divided into two groups: Control group (Group I) containing 20 subjects and study group taking probiotics (Group II) containing 120 subjects. The Group II was further subdivided into six subgroups based on probiotic intake with 20 subjects in each subgroup. The sample size was calculated using Daniel’s formula. 6 Based on the 1:1 ratio between groups, a total sample size of 20 participants in Group I (Control group) and each of the 6 six subgroups in Group II would give more than 80% power (actual power, 0.8173). 7 A signed consent was obtained from all the subjects/parents/guardians participating in the study.
The inclusion criteria of the study were patients with mild-to-moderate crowding, nonextraction treatment cases, patients with good oral hygiene and general health, patients with permanent dentition and patients with fewer than five decayed, missing, or filled teeth.
Patients with significant medical history of chronic systemic illness or immune disorders, patients on any medication during or in the previous month of the study, patients who have undergone topical fluoride treatment within the past four weeks, patients using antiinflammatory medications or antibiotics, and patients with the habit of chewing gum or using mouthwashes were excluded from the study.
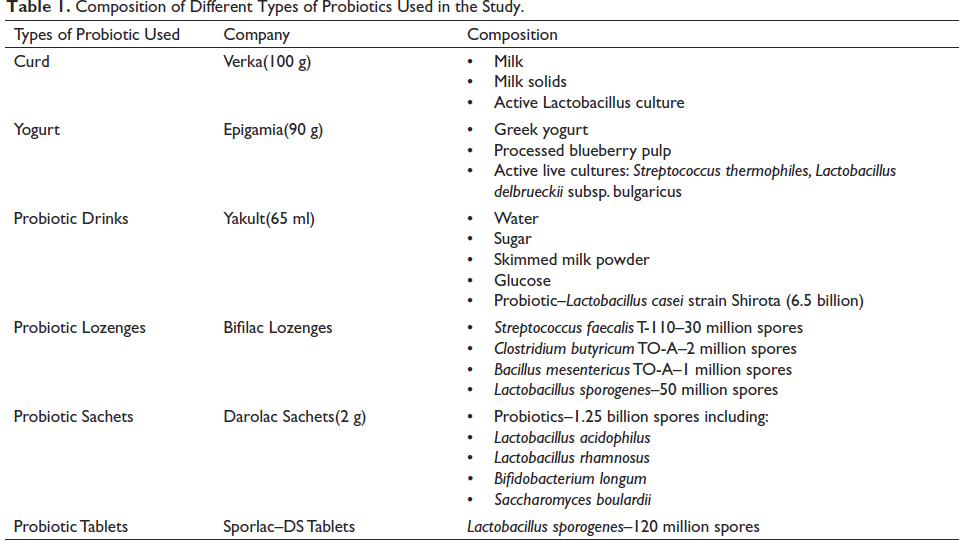
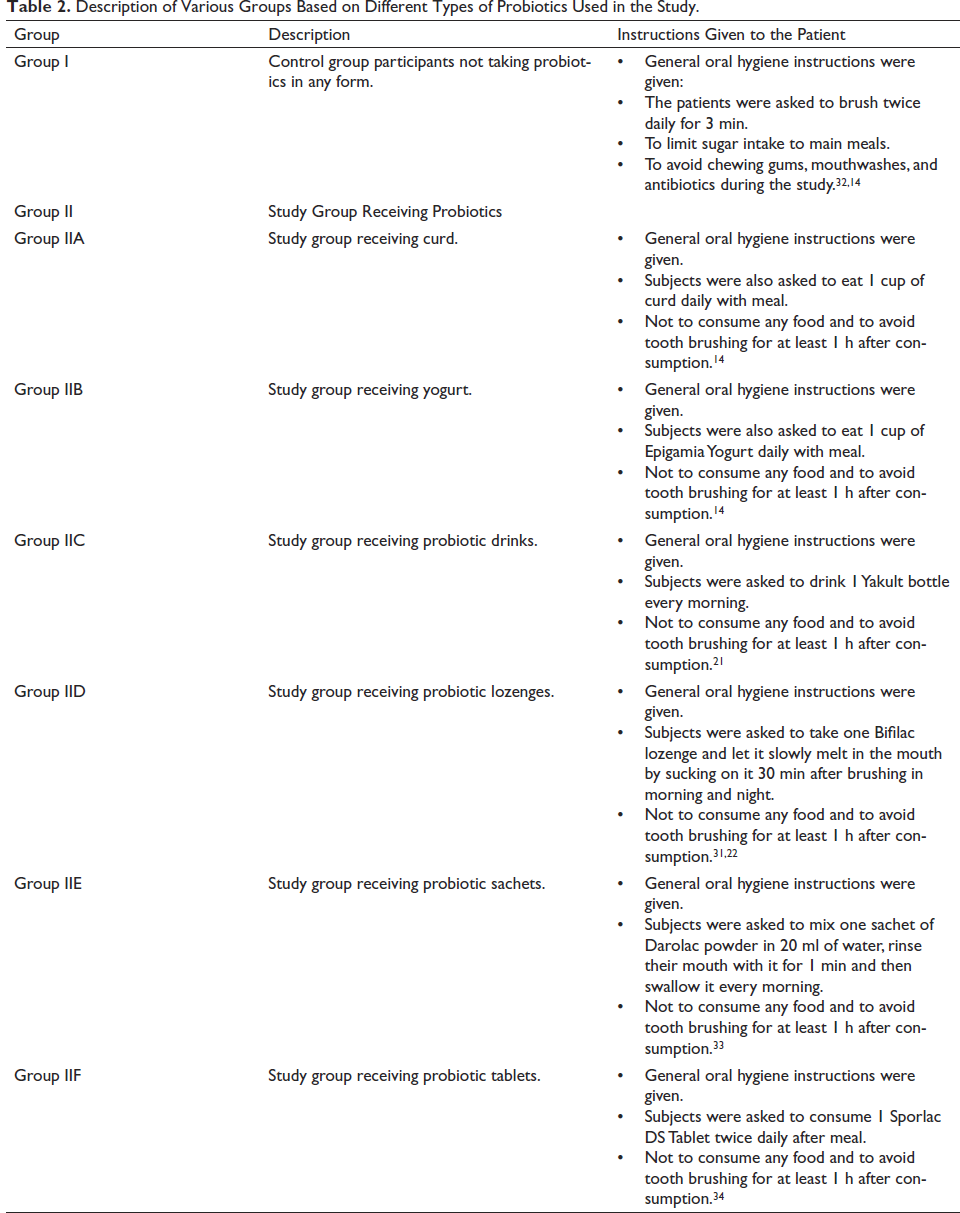
The patients were divided into two main groups: Group I containing 20 subjects and Group 2 containing 120 subjects. Group II was further subdivided into six subgroups with 20 subjects each based on the various probiotic products prescribed (Table 1). The subjects in experimental group (Group II) received instructions on how to use the specific probiotic product prescribed to them (Table 2).
Composition of Different Types of Probiotics Used in the Study.
Description of Various Groups Based on Different Types of Probiotics Used in the Study.
All the subjects were bonded with 0.022 × 0.028 inch slot brackets with the same adhesive material (3M Unitek Transbond XT adhesive) using an LED light source. Stainless steel wire ligatures of 0.009-inch diameter were used throughout the treatment. Materials like elastic ligatures, chains, coil springs, or figure-eight ligatures were not used before or during the study as they could adversely affect oral hygiene. Same oral hygiene instructions were given to all the patients and were prescribed same toothbrushes. The subjects were also advised to avoid sugary substances and to include healthy food in their diet.
Samples were taken at the beginning of the study (baseline sample T0), after three weeks of probiotic intake (T1), and after six weeks of probiotic intake (T2). To ensure regular use of probiotic products, the patients in the study group were given daily checklists to mark after each use and were regularly recalled to check their use of products.
Method of Saliva Collection
Saliva collection was done one month after the initiation of fixed orthodontic mechanotherapy. After swallowing preexisting saliva, subject was given paraffin wax to chew. A total of 2 ml of saliva was then collected by expectorating in a sterile test tube.
Laboratory Procedures
Three test tubes were taken with 9 ml of distilled water in each of them. The initial dilution was prepared by adding 1 ml of sample using a pipette to the first test tube and was mixed thoroughly, thus diluting the original sample 10 times (1:10 or 10−1).
From the first dilution, 1 ml of suspension was transferred to the next test tube diluting the original sample to 100 times (1:100 or 10−2). Repeating this procedure with the third test tube, the original sample was diluted 1,000 times (1:1000 or 10−3). From the third tube, 1 ml of diluted sample was spread on the Mitis Salivarius Bacitracin agar media selective for S. mutans and Rogosa SL agar media selective for Lactobacillus. 8
Both plates were incubated in aerobic conditions at 37°C for 48 h in the incubator. After 48 h, agar plates were checked for colonies of S. mutans and Lactobacillus. The colonies were counted by using a magnifying glass and expressed in colony forming units per milliliter (CFU/ml) of saliva. The number of organisms developed on the plates after incubation were calculated by using the formula
8
:

Statistical Analysis
The data was analyzed and compared using SPSS software version 21. Student t test was done for intergroup multiple comparisons of S. mutans and Lactobacilli counts at different time intervals and analysis of variance (ANOVA) was used for intragroup comparison of S. mutans and Lactobacilli counts at different time intervals. The level of statistical significance used in this study was set at p < 0.05.
Results
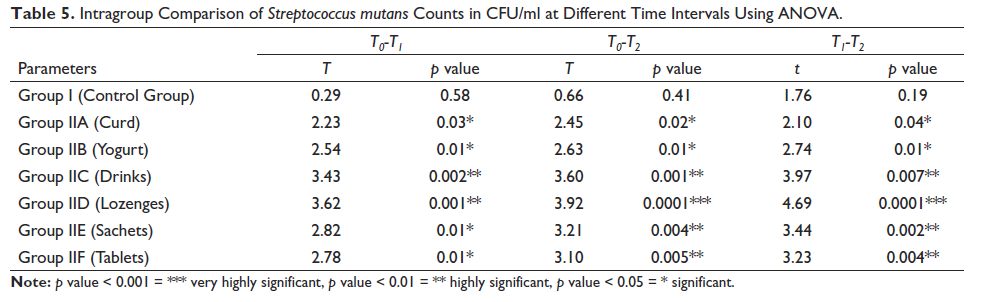
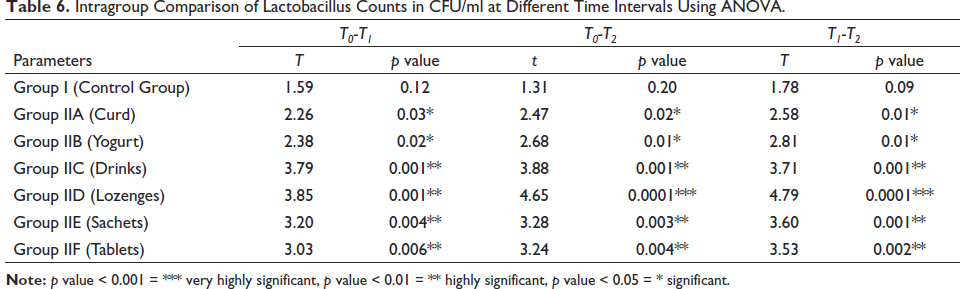
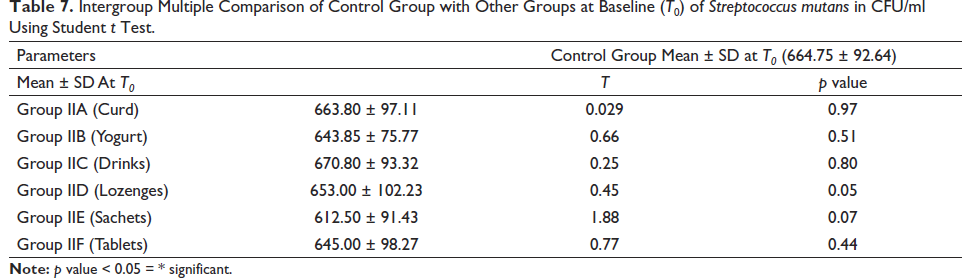
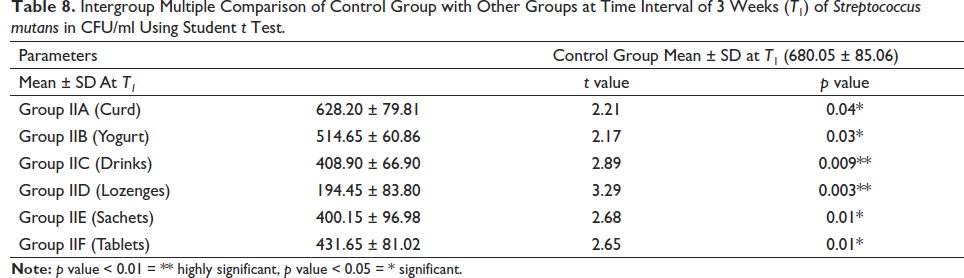
The descriptive statistics of effects of different types of probiotics on S. mutans and Lactobacilli are shown in Tables 3 and 4. Intragroup comparison of S. mutans and Lactobacilli counts at different time intervals done using ANOVA revealed that the reduction in the count of S. mutans and Lactobacilli was more in group IID (lozenges) followed by group IIC (drinks), IIE (Sachets), IIF (Tablets), IIB (yogurt), and IIA (Curd) as shown in Tables 5 and 6. Student t test was done for intergroup multiple comparisons of S. mutans and Lactobacilli counts at baseline (T0), three weeks (T1), and six weeks (T2) as shown in Tables 7–12.
Descriptive Statistics of Streptococcus mutans Count in CFU/ml in Different Groups.
Descriptive Statistics of Lactobacillus Count in CFU/ml in Different Groups.
Intragroup Comparison of Streptococcus mutans Counts in CFU/ml at Different Time Intervals Using ANOVA.
Intragroup Comparison of Lactobacillus Counts in CFU/ml at Different Time Intervals Using ANOVA.
Intergroup Multiple Comparison of Control Group with Other Groups at Baseline (T0) of Streptococcus mutans in CFU/ml Using Student t Test.
Intergroup Multiple Comparison of Control Group with Other Groups at Time Interval of 3 Weeks (T1) of Streptococcus mutans in CFU/ml Using Student t Test.
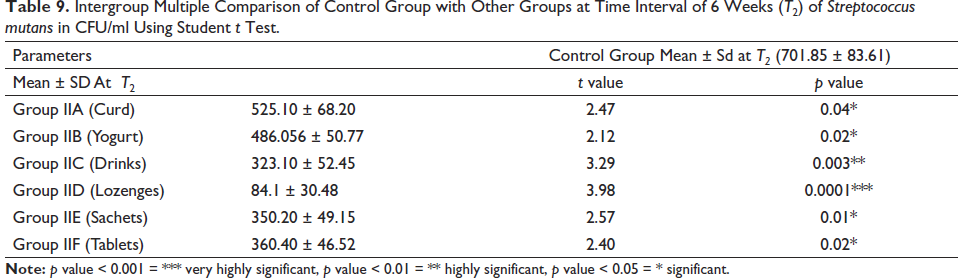
Intergroup Multiple Comparison of Control Group with Other Groups at Time Interval of 6 Weeks (T2) of Streptococcus mutans in CFU/ml Using Student t Test.
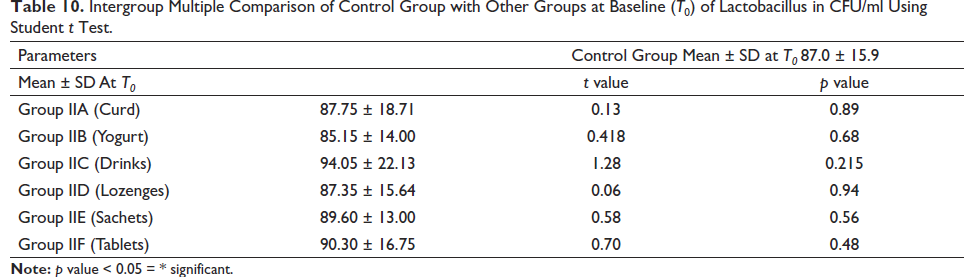
Intergroup Multiple Comparison of Control Group with Other Groups at Baseline (T0) of Lactobacillus in CFU/ml Using Student t Test.
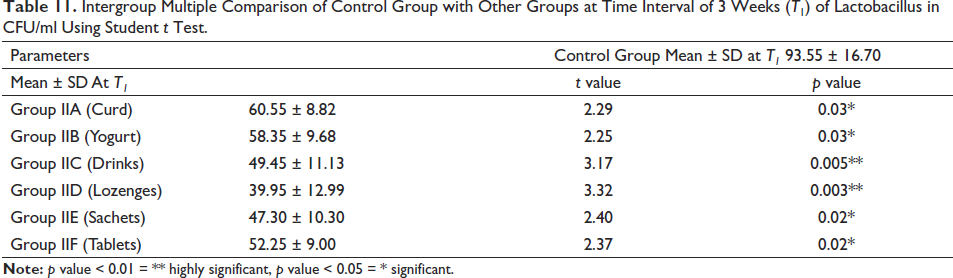
Intergroup Multiple Comparison of Control Group with Other Groups at Time Interval of 3 Weeks (T1) of Lactobacillus in CFU/ml Using Student t Test.
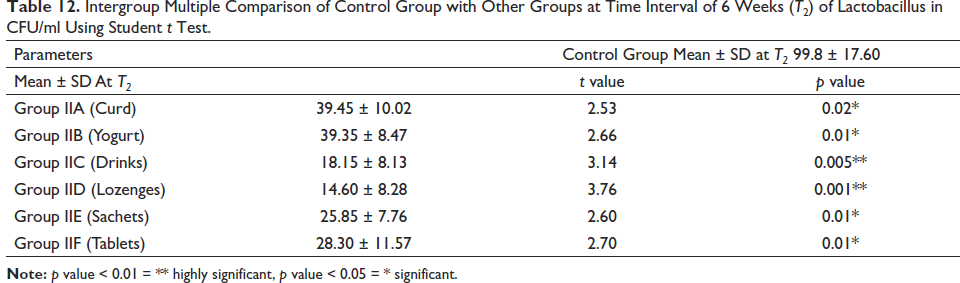
Intergroup Multiple Comparison of Control Group with Other Groups at Time Interval of 6 Weeks (T2) of Lactobacillus in CFU/ml Using Student t Test.
Discussion
One of the most important iatrogenic effects of fixed orthodontic appliance therapy is white spot lesion formation on the enamel surfaces around orthodontic attachments due to substantial increase in the surface area harboring dental plaque owing to their complex design and restricted access for self-cleansing. 4 As the presence of these lesions hamper the final aesthetic result, various preventive and corrective measures and techniques have been suggested previously, but each has its own set of drawbacks. Recently, probiotics, a new and innovative method, started gaining importance as an alternative and emerged as a solution. The beneficial bacteria compete with the pathogenic bacteria, thereby reducing their number and harmful effects on our body. 5
In the present study, there was increase in the S. mutans and Lactobacillus count in the control group as shown in Tables 3 and 4. This is because of the increase in accumulation of plaque due to the presence of fixed appliances in the patient’s mouth and this group has not been instructed to use any probiotic products. This was in accordance with the study done by Scheie et al. and Rosenbloom and Tinanoff.9, 10
The results of the present study showed that there was a significant decrease in S. mutans and Lactobacilli count in this group after curd consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This might be due to the fact that the curd being semisolid in consistency may be retained in the oral cavity for a long period of time with extended beneficial effect. Also, lactose-based dairy products have high concentrations of calcium, phosphorous, and casein which help in preventing dissolution of enamel. Curd contains Lactobacillus as one of its components which has the ability to produce hydrogen peroxide and antibacterial substances such as lactocidin and acidophilin. They do not ferment lactose and sucrose and temporarily colonize the oral cavity for two weeks, thereby inhibiting the colonization and growth of the other bacteria in the oral cavity including Streptococci. This was in accordance with the study done by Srivastava et al., 11 Sudhir et al., 12 and Selvarajan et al. 13 They also found a significant reduction in S. mutans counts after intake of curd. Further, on intragroup comparison from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the curd group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
The results of the present study showed that there was a significant decrease in S. mutans and Lactobacilli count in this group after yogurt consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This might be due to the fact that yoghurt contains around 10 8 –10 9 Streptococcus thermophilus and Lactobacillus delbrueckii subsp. Bulgaricus microorganisms per gram multiply in associated growth. The lactobacilli hydrolyze proteins to amino acids and dipeptides which stimulate the growth of S. thermophilus. S. thermophilus produces low pH conditions favoring Lactobacilli growth. These microorganisms produce nisins and lactic acid which are antimicrobial in nature. The Lactobacillus bulgaricus species is more active against streptococcal species and Aggregatibacter actinomycetemcomitans whereas S. thermophilus shows selective antimicrobial activity against periodontal pathogens. This was in accordance with the study done by Petti et al. 14 They found that regular consumption of yogurt can decrease the number of salivary Streptococcus mutans and lactobacilli. Another reason might be the presence of k-casein in yogurt, which reduces the adherence of dental plaque microorganisms to tooth surfaces, resulting in decrease in the number of oral microflora. This was in accordance with the study done by Neeser et al., Vacca-Smith and Bowen, and Guggenheim et al.15–17 Furthermore, on intragroup comparison of the mean values from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the yogurt group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
The results of the present study showed that there was a significant decrease in S. mutans and Lactobacilli count in this group after probiotic drink consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This might be due to the fact that the probiotic drink is of milk origin and has casein phosphopeptides which reduce enamel demineralization and promote remineralization. This was in accordance with the study done by Glavina et al. 18 and Yadav et al. 19 The drink contains Lactobacillus casei Shirota strain which selectively colonize on tongue and in saliva. They affect the oral ecology by specifically preventing the adherence of other bacteria by modifying the protein composition of salivary pellicle and masking the receptors for binding by coaggregation, thereby preventing adhesion and colonization of S. mutans. This was in accordance with the study done by Yadav et al. 19 , Haukioja et al., 20 and Koul et al. 21 Further, on intragroup comparison of the mean values from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the drinks group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
The present study showed that there was a significant decrease in S. mutans and Lactobacilli count in this group after probiotic lozenge consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This group showed the highest reduction in salivary microbial count as compared to other groups. This might be due to the fact that lozenges are medicated tablets intended to be dissolved slowly in the mouth, hence the duration of contact of probiotic strains in the oral cavity will be more, leading to increased local action of probiotics. This was in accordance with the study done by Kavitha et al. 22 Another reason could be that the combination of probiotics in the lozenges act synergistically in symbiosis and enhance the possibility for permanent installation on oral surfaces. This was in accordance with the study done by Dhawan and Dhawan 23 ; they also found a significant reduction in S. mutans levels in the probiotic lozenge group. The Lactobacilli present in the lozenges also produces various antimicrobial components including organic acids, low molecular weight bacteriocins, hydrogen peroxide, and adhesion inhibitors which further reduce the levels of S. mutans in saliva. This was in accordance with the study done by Elavarasu et al. and Silva et al.24, 25 Furthermore, on intragroup comparison of the mean values from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the lozenge group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
The present study showed that there was a significant decrease in S. mutans and Lactobacilli count in this group after probiotic sachet consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This might be due to the fact that in the complex environment of human mouth, probiotic cocktails or combinations of multiple strains as present in the sachet are more effective than any single probiotic agent. This was in accordance with the study done by Purunaik et al. 26 ; they found that probiotic sachets showed a significant reduction in plaque. Sachets contain the combination of Lactobacillus rhamnosus and Bifidobacterium which has been shown to improve periodontal health. The reason could be that Bifidobacteria present in sachet can survive in saliva for 24 h and bind to the Fusobacterium nucleatum covered hydroxyapatite present on the tooth surface; Lactobacillus rhamnosus competes with S. mutans for adherence sites on hydroxyapatite and doesn’t ferment sucrose thereby reducing acid production. This was in accordance with the study done by Glavina et al., 18 Haukioja et al., 20 Meurman et al., 27 and Cildir et al. 1 Furthermore, on intragroup comparison of the mean values from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the sachet group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
The results of the present study showed a significant decrease in S. mutans and Lactobacilli count in this group after probiotic tablet consumption for three weeks and further reduction in six weeks as shown in Tables 3 and 4. This might be due to the fact that the tablets contain Lactobacillus sporogenes which produces low molecular weight bacteriocins that have an inhibitory effect on the bacterial species present in the oral cavity. They also reduce pathogenic bacteria by means of aggregation, competition for adhesion sites, nutrients and growth factors, production of acids, and affect the immune response of the host. This was in accordance with the study done by Silva et al., 25 Nishihara et al., 28 Teughels et al., 29 and Stamatova et al. 30 Furthermore, on intragroup comparison of the mean values from baseline (T0) to three weeks (T1), from baseline (T0) to six weeks (T2), and from three weeks (T1) to six weeks (T2) in the tablet group, statistically significant difference was found (p < 0.05) as shown in Tables 5 and 6.
Thus, the reduction in S. mutans and Lactobacilli count was found to be more in group IID (lozenges) followed by group IIC (drinks), IIE (Sachets), IIF (Tablets), IIB (yogurt), and IIA (Curd). This shows that the introduction of the concept of probiotic intake would be beneficial for the orthodontic patients by reducing S. mutans accumulation which is considered as a prime etiological factor in the development of white spot lesions. Due to the brevity of consumption period of different probiotics and the limitation of the probiotic microorganism types used in the study, more longitudinal studies are required to show the effect of longer duration of consumption of probiotic products on the salivary levels of different microorganisms.
Conclusion
The reduction in the count of salivary level of S. mutans in orthodontic patients was found to be maximum in lozenges and least in curd.
The reduction in the count of salivary level of Lactobacillus in orthodontic patients was found to be maximum in lozenges and least in curd.
This suggested that regular consumption of probiotics is a better alternative to decrease the number of salivary S. mutans and Lactobacilli.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval for probiotic administration was taken from the research ethics committee of Sunder Nagar (Himachal Pradesh).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.