
Abstract
Fixed functional appliances are used at either the fag end of the growth spurt or after the completion of the same. We orthodontists are yet to come across an appliance which satisfies all the ideal requirements for a fixed functional appliance. Most disadvantages of the fixed functional appliances such as increase in lower anterior facial height, proclination of lower anteriors, constant breakages, and huge expenses were taken into consideration in the basic designing of this ingenious appliance. In this article, a simple fixed functional appliance was designed to function along with fixed appliance therapy to stimulate mandibular growth. After the initial leveling and aligning, 0.019 × 0.025 stainless steel posted arch wires were placed. The bite jumping blocks were fabricated in the upper and lower arches with light cure blue composite. Using indirect bonding trays they were bonded in position. The case finished in an ideal overjet and overbite with a balanced face. Cephalometric values demonstrate an advancement of the mandible.
Keywords
Introduction
The most challenging situation for the orthodontist is to convince adolescent patients to use class II elastics or wear removable appliances. 1 This could probably be one of the reasons that most fixed functional appliances (FFAs) are secured permanently. Thus, Emil Herbst developed an appliance which was fixed to the teeth to advance the mandible. After the Herbst appliance reappeared or was rediscovered by Pancerz, different types of fixed appliances were developed to correct class II malocclusion in the past few years. 2
FFA are mostly used when the patient has already attained puberty or is at the fag end of growth. The ultimate motive, is to be more efficient than a routine functional appliance, by being in situ 24 × 7 and thus attaining the required results.
However, FFA have their own drawbacks and appear to be reason for most orthodontists not having them in their armamentarium. Some of the major drawbacks are that they are expensive and sometimes even more expensive than that of a preadjusted edgewise bracket kit. Additionally, the patient is burdened with the expenditure of a second phase fixed therapy. Most appliances use the buccal vestibule as the region of operation and this can be traumatic to the buccal mucosa. Most FFA do not make it possible to carry out fixed appliance therapy with extractions, especially because the premolars are used for anchoring the appliance. Additionally certain appliances such as the Herbst (type I) restrict lateral mandibular movements. Breakages, especially at soldered joints or at the bonded tooth taken for anchorage is common. In regard to the dental adverse effects, extrusion of posteriors causing an increase in lower anterior facial height and proclination of lower anteriors is a common feature.
Taking into consideration these drawbacks, it was planned to construct a FFA which would overcome these issues.
Case History and Treatment Plan
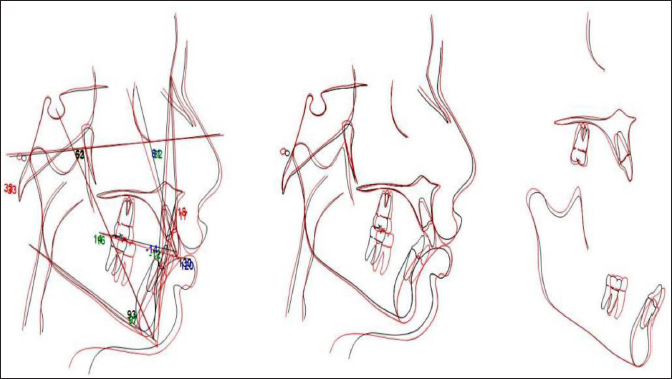
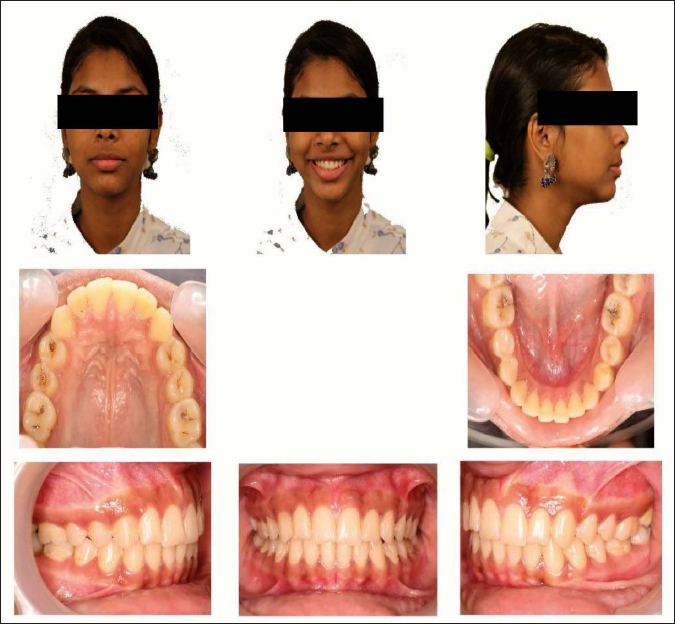
A 13-year-old female patient who had attained puberty exhibited a convex profile, posterior divergence, and incompetent lips with 3 mm of interlabial gap. The lower anterior facial height was increased by 1 mm. The intraoral examination revealed unerupted 25, 35, an end on molar relation, class 2 div 2 incisor relation with 7 mm overjet and 4 mm overbite. The cephalometric analysis revealed a class II skeletal relationship with an orthognathic maxilla and a retrognathic mandible, normal growth pattern and the visual treatment objective (VTO) was positive (Figures 1 and 2). The hand wrist radiograph showed skeletal maturity indicators (SMI) stage 8 indicating 22.3% mandibular growth remaining.
Pretreatment Records.

VTO.

As the incisors were retroclined and the overjet was insufficient for the mandible to be advanced, prefunctional orthodontic therapy was initiated. A second phase of functional therapy was planned to advance the mandible after sufficient overjet was attained.
Treatment Progress
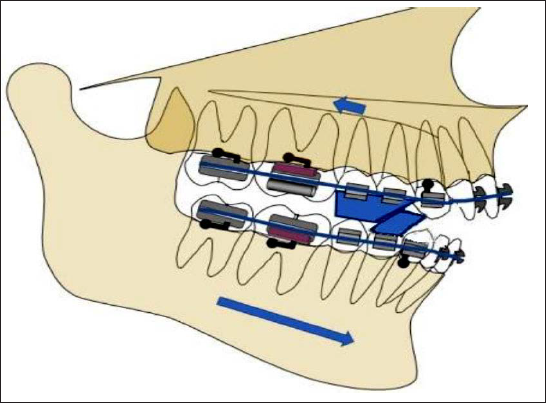
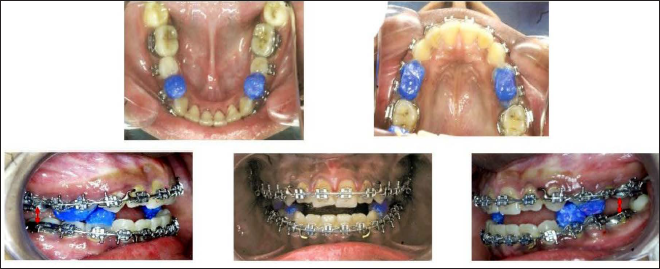
After the initial leveling and aligning, an upper and lower 0.019″ × 0.025″ stainless steel arch wire was placed. Ensuing, the upper and lower impressions were taken, a construction bite with 5 mm advancement and vertical clearance of 5 mm in the premolar region was recorded. The models were then mounted on an articulator along with the construction bite. Once articulated, the construction bite was removed. Subsequently, separating media were applied and the blue bite blocks were fabricated on the models in a similar manner to Clark’s Twin block appliance (TBA) (70° inclination) 3 and cured. Unlike the TBA blocks, the blue bite blocks involved only one or two teeth per arch. After the models were removed from the articulator, using thermoplastic material (bioplast 1mm), indirect bonding trays were fabricated with the blue bite blocks in position. Later, routine etching and application of the bonding agent were carried out and the bite blocks were bonded in position intraorally (Figures 3–5).
Construction Bite and Blue Bite Block Construction.

Positioning of Blue Bite Blocks.
Blue Bite Blocks Bonded.
After an active phase of 6 months, as in conventional twin block therapy, trimming of the upper blocks was initiated followed by the lower blocks (Figure 6). Just like trimming of acrylic blocks in conventional TBA therapy, the upper composite block was trimmed initially and later the lower blocks too, intraorally using airotors. Initially the posterior aspect of the blocks was trimmed and thinned down and it was to the end that the anterior portion of the block was reduced. Subsequently, after 12 months the blue bite blocks were completely removed, and a good class I molar relation was achieved with a mild open bite tendency in the premolar region which was settled with aligning wires. The fixed appliance was then debonded and thermoplastic retainers were delivered. The total treatment duration was 18 months.
Trimming of Bite Blocks.

Treatment Outcome
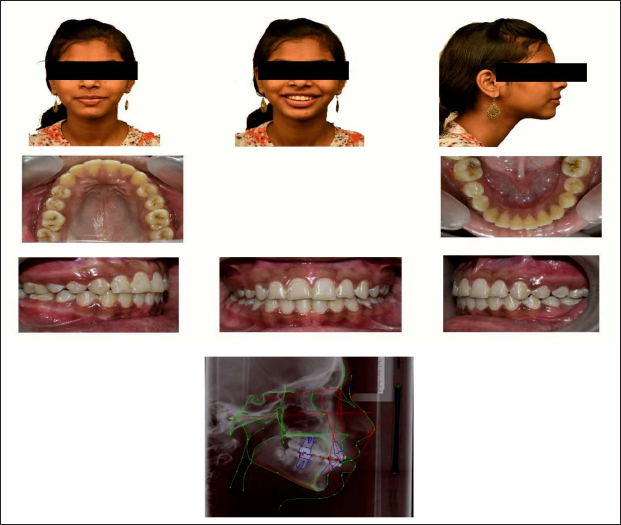
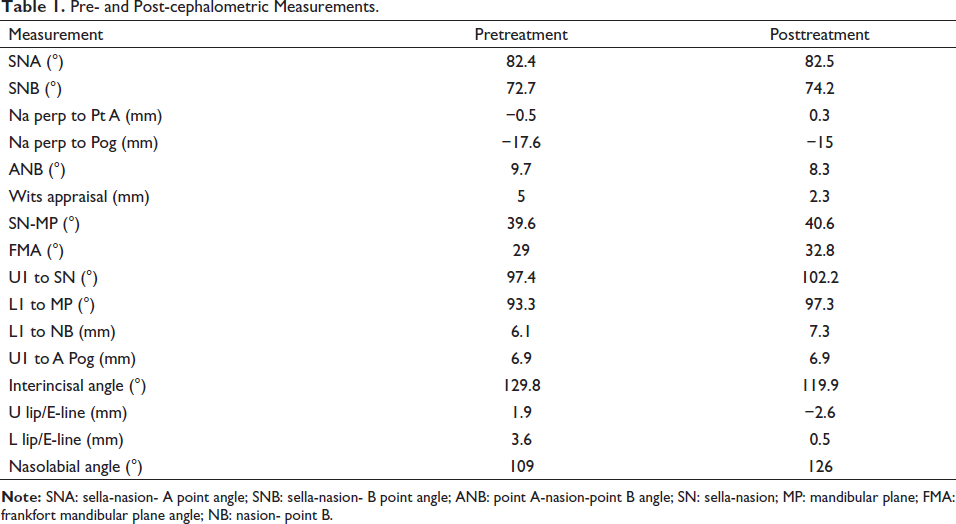
The profile of the patient had improved to an ideal profile after the treatment. The incisor, canine, and molar relationships were class I at the end of treatment. The overbite and overjet were reduced to the average values (Figure 7). The cephalometric values demonstrated reduction in ANB angle and witts appraisal, improved anteroposterior position of the mandible, upright maxillary incisors, and proclined mandibular incisors (Table 1). Overall superimposition of the lateral cephalometric radiographs is illustrated in Figure 8. Eight months after debonding is illustrated in Figure 9.
Posttreatment Records.
Pre- and Post-cephalometric Measurements.
Cephalometric Superimposition.
Eights Months After Debonding.
Discussion
One of the common issues encountered in FFA therapy is repeated breakages during the treatment period. However, no breakages were encountered during the entire duration of therapy. Sanden et al. described some of the major drawbacks during fixed functional therapy. The most commonly encountered issues were breakage of bands or splints, breakage of telescoping mechanisms, loosening of bands or splints, trauma to buccal mucosa, rotated and/or intruded teeth, canting in the occlusal plane, and development of posterior cross bite.4, 5
This versatile appliance almost takes care of all the disadvantages encountered with routine FFA. As the upper and lower posterior teeth are all engaged to a rigid rectangular archwire there is no eruption of posteriors which causes and increase in lower anterior facial height. Additionally, the labial movement of lower anterior teeth, which is almost always associated with FFA could be managed by placing labial root torque in the lower anterior section of the archwire.
The composite bite blocks are very patient friendly especially because it facilitates lateral movements of the mandible. It has no additional metal assemblies on the buccal aspect thus decreasing the tendency for trauma.
Whenever a “step by step” advancement of mandible is intended, additional increments of blue composite can easily be added or could even be newly constructed and bonded in place with no great difficulty. The versatility of being able to be used along with fixed appliances is another advantage of this appliance. 6 This is especially so because the appliance is not attached to the fixed appliance directly and thus reduces the likelihood of debonding of brackets (lower canines).
Needless to mention the composite bite block fixed class II corrector is a simple and inexpensive appliance.
Conclusion
The appliance takes care of almost all the drawbacks that are usually encountered with FFA. It is simple, versatile, and inexpensive and could be considered as a routine appliance in the orthodontist’s armamentarium.
Ethical Approval
Ethical approval from relevant committee or Institutional Review Boards (IRBs) was obtained.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal.