
Abstract
Activator is a commonly used appliance that Andresen and Haupl created to correct retrognathic mandible in 1908. The appliance opens the bite, and the mandible is advanced for class II correction. However, it has disadvantages like strenuous laboratory work (back office work) and any error leading to ill-fitting. Whereas the advantages of a 3D printed activator over a conventional one can be less chair-side time, high-quality finish, relatively fast, good accuracy, etc. Thus, we introduce 3D printed activator a novel modification in the present fabrication method to make it more precise and ease the back office work.
Introduction
The activator is a removable functional appliance primarily utilized for the correction of class II, division 1 malocclusion. Based on the “bite jumping” principle introduced by Kingsley2 in 1877, the activator produces an intermittent functional jumping of the bite. This means that the mandible is advanced to a protrusive position whenever the patient bites into the appliance. 1
The stresses that the activator appliance applies to the teeth and jaws during therapy lead to dentoalveolar and skeletal adaptation mechanisms that induce the distal malocclusion to change into the therapeutically sought neutral occlusion. 2 The productivity of the appliance is dependent on its usage. Therefore, until the transformation process is completed, patients using this appliance take up new condylar positions in their habitual distal occlusion (condyle in the fossa) and the mandible therapeutically jumps to the position given by the appliance (protruded condylar position). 3
However, it has disadvantages it may be ill-fitting because of the warpage of wax during the transport of the bite and the delay in pouring the models. The advantage of using an intraoral scanner for digital impressions is patient comfort, less working time, and relatively less cost. A prototype of a working model is made using the same 3D printer using resin. 4 Thus we introduce a novel modification in the fabrication method to make it more precise.
Materials and Method
The process for design and 3D printing of digital reference models and fabrication of 3D printed activator is shown in the table below:
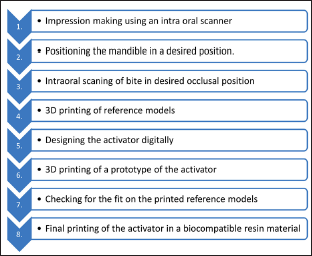
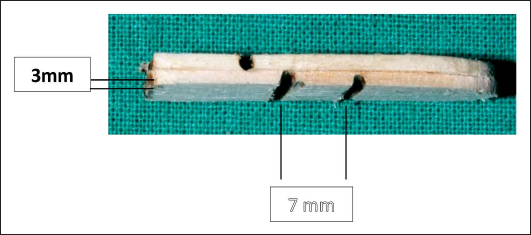
A patient with a compromised mandible and a class II skeletal discrepancy was chosen. To create the appropriate occlusion, two ice cream sticks were utilized as notches. An intra-oral scanner was used to comprehensively scan the upper and lower arches. After that, the patient was instructed to advance the mandible into the proper occlusion. To help stabilize the appropriate occlusion, the ice cream sticks’ notches were used as a guide to bite between the upper and lower incisors (Figure 1).
An Ice Cream Stick is Used to Position the Maxilla and the Mandible at the Desired Position.
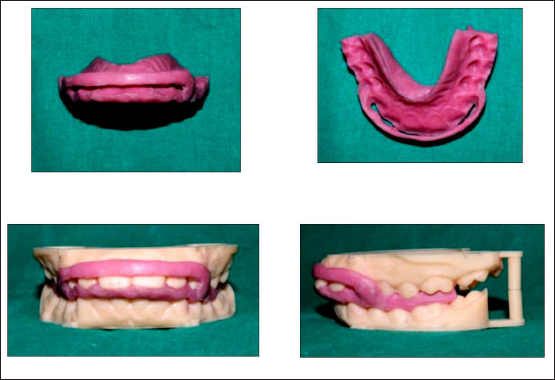
An intra-oral scanner was used to scan the entire bite in the appropriate occlusion. 3D reference models were then printed in the new occlusion using a resin material.
A simulated upper and lower model served as the basis for the appliance’s design (Figure 2). After that, a 3D printer was used to create a prototype. Following that, the prototype’s fit and quality were examined on the printed reference models (Figure 3).
The Activator is then Fabricated by Using 3D Designing Software.

Prototypes were Made and Checked on 3D Printed Models.
Discussion
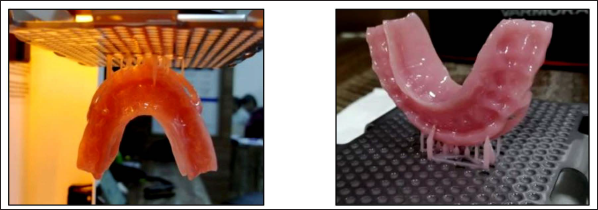
3D printed activator can be fabricated using the above method (Figure 4). The method described above has a number of advantages over the conventional method, including the avoidance of warpage of wax during transport of the bite, the elimination of the traditional method of making an impression, the avoidance of human error during fabrication, the ability to be easily refabricated if lost or damaged, a precise fit, a shorter finishing polishing time, and increased accuracy.
The Activator is then Printed Using a 3D Printer with a Biocompatible Resin Material.
Conclusion
A 3D-printed activator can be fabricated which has a lot of advantages over the traditional activator.
Footnotes
Acknowledgment
This work would not have been possible without the support of the Department of Orthodontics and Dentofacial Orthopaedics, Yashwantrao Chavan Dental College & Hospital, Ahmednagar.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Due to the fact that it simply relates to the fabrication of the appliance, ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.