
Abstract
Background and Objectives
A probable association between dermatoglyphics and malocclusions related to skeletal discrepancy may exist as dermal ridges, and craniofacial structures develop from the same embryonic tissues during the same embryonic period. The study aims to assess and correlate the pattern of fingerprints, lip prints, and palatal rugae in individuals with malocclusions related to skeletal discrepancy.
Materials and Methods
The 180 samples collected in the study were divided into 3 groups based on cephalometric analysis into class I, II, and III malocclusion. The fingerprints, lip prints, and palatal rugae patterns were obtained for each participant and pattern analysis was done.
Results
Class I malocclusion with no skeletal discrepancy showed a statistically significant difference in the loop fingerprint patterns on all fingers except the first finger on the right and left hand, branched lip pattern, and straight palatal rugae pattern in primary rugae 1 and 4. Class II malocclusion related to skeletal discrepancy showed a statistically significant difference in the loop pattern on all fingers except in the fourth finger of the right hand which showed a whorl pattern, branched lip pattern, and straight palatal rugae pattern in primary rugae 1, 4, and 5. Class III malocclusion related to skeletal discrepancy showed a statistically significant difference in the loop pattern on all fingers except in the fourth finger of the right hand which showed an absence of arch pattern, vertical lip print pattern, and straight palatal rugae pattern in primary rugae 1.
Conclusion
Dermatoglyphics analysis can be used to indicate developing malocclusions related to skeletal discrepancies. at an early age, thereby aiding the development of treatment aiming to establish favorable occlusion. Prospective and various ethnic and racial-based studies would be valuable for the establishment of dermatoglyphic markers of malocclusion.
Keywords
Introduction
Valleys and ridges that present on the surface of the skin are patterns of every individual. They are unique and present on the skin of the palms, fingers soles, and toes. These patterns are called “dermatoglyphics.” 1 This term coined by Harold Cummins and Mildo in the year 1926 was derived from the Greek word derma, which means “skin,” and glyphae meaning “to carve.”2, 3 Fingerprint analysis, also termed as dactyloscopy, is based on the uniqueness of the fingerprints. 4 It is an established scientific fact that no 2 individuals have the same pattern of fingerprints. Fingerprints are typically considered into 3 basic groups namely arches (60-65%), loops (30-35%), and whorls (5%). A person may have the same pattern on all 10 fingers but various patterns often occur on different digits. 4
Other unique dermal ridge derivatives include lip prints and palatal rugae morphology. The characteristic normal lines and fissures are in the form of wrinkles and grooves existing in the zone of transition of the human lip, between the inner labial mucosa and outer skin are the lip prints, the examination of which is referred to as “cheiloscopy.” 5 McDonell in 1972 studied identical twins and determined that lip prints are analogous to thumbprints 6 in uniqueness as these are epidermal derivatives established early in the intrauterine life.
Another epidermal derivative is the palatal rugae and the study of palatal rugae is called palatoscopy or palate rugoscopy. Palatal rugae appear in the third month of intrauterine life and occupy most of the length of palatal shelves. The stability and hereditary inclination exhibited by palatal rugae led to the suggestion that various occlusal characteristics that display a strong genetic basis may display an association with palatal rugae. 7 Development of the dermal ridges occurs by the sixth week of gestation and their maximum size is reached between the 12th and 13th weeks. The development of teeth commences during the sixth week of intrauterine life. Craniofacial characteristics and dermal ridge patterns could be mainly genetically governed structures, but not exclusively. It could be assumed that the genetic and environmental factors that cause changes in alveolar bone may also cause peculiarities in the appearance of dermatoglyphic patterns. 8
Dermatoglyphics extends its application to unique fields like anthropology and has been the heart of forensic medicine for a long time. Forensic medicine is the best and most widely used method for personal identification 9 postmortem and antemortem. In application to the field of medicine, it has been shown that there is an association between fingerprint patterns and various conditions like diabetes mellitus, hypertension, 10 psychosis, 11 breast cancer, 12 , alcohol embryopathy, 13 , epilepsy, 14 congenital heart diseases, 15 and many other conditions. 16
Also, a wide variety of chromosomal disorders like Autosomal aneuploidy such as mongolism, trisomy18, and trisomy15. Aberrations of sex chromosomes such as Turner’s syndrome, and Klinefelter syndrome. Single Gene Disorders; such as Wilson’s Disease, and Huntington’s Chorea. Exogenous influences such as thalidomide-damaged infants, cerebral palsy, and rubella show a deviation in their dermatoglyphic patterns.17 In the field of dentistry, irregular fingerprints have been observed among patients with periodontitis, 18 dental caries19, 20 certain types of congenital anomalies like cleft lip and palate,21, 22 and recently, dermatoglyphics has been related to malocclusion23, 24 and other developmental disturbances of the orofacial structures.25–27
Several researchers 28 have claimed a high degree of accuracy in the prognosis of disorders using dermatoglyphic patterns. The dermatoglyphic pattern can become a primary means of assessing complex genetic traits in the future. The heterogeneous nature of dermatoglyphics can be a possible factor for distinguishing different malocclusions among the population.
Malocclusion is one of the most prevalent oral conditions affecting facial aesthetics which may involve irregular alignment of teeth, faulty positioning of the jaws, or a combination of both, and dermal ridge development could be relevant to each other as they share the same developmental time frame. Any abnormality in the genome may reflect in these dermal ridge derivatives and in turn may aid as a diagnostic adjunct for malocclusions very early in life and help in preventive or interceptive measures to alleviate imminent dentoskeletal aberrations which have been one of the main goals of orthodontic treatment for many years.7, 29 The study aims to assess and correlate the pattern of fingerprints, lip prints, and palatal rugae in individuals with malocclusions related to skeletal discrepancy.
Materials and Methods
A total of 180 patients in the age group 18 to 40 years who reported for treatment were selected from the Department of Orthodontics and Dentofacial Orthopedics, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Center. The study was conducted after obtaining ethical clearance from the institution and informed consent from the patients. (IEC No: PMVIDS&RC/IEC/ORTHO/DN/0237-2018).
The sample included 180 patients of the south Indian demography whose ethnicity is Asian. Out of the 180 samples taken randomly to represent the population, 72 of them were females and 108 were males.
Inclusion Criteria 1
Patients in the age group 18 to 40 years.
Systemically healthy patients.
Patients who did not undergo any orthodontic treatment previously.
Patients who have consented to the study.
Exclusion Criteria1, 5
Patients who had undergone orthodontic treatment.
Patients with cleft lip and palate and who underwent surgical procedures in the orofacial region.
Patients with wounds or scars on the hand.
Patients with any lesion on the lips.
Patients with developmental anomalies, any systemic disease affecting bone and general health, children and pregnant women, and mentally retarded patients.
Patients who did not give informed consent.
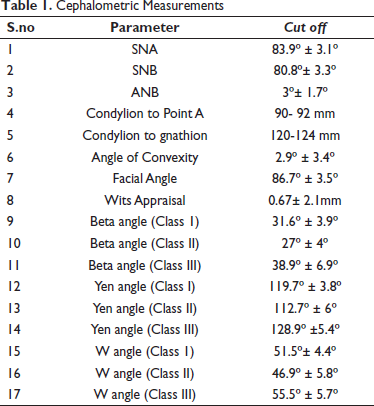
Fingerprints and lip prints were recorded from every subject to evaluate their pattern. Alginate impressions of the subjects were made to study the morphology of the rugae pattern after making study models from the impressions. The data was sent confidentially to an expert in forensic analysis. Cephalometric X-rays of the subject were used to divide them based on malocclusion with skeletal discrepancy into class I, II, and III groups using the following composite parameter like SNA, SNB, ANB, Wits appraisal, Condylion to Point A, Condylion to gnathion, Angle of convexity Facial angle, Beta angle, Yen angle, and W angle. South Indian cephalometric norms were taken into consideration to decide the cut-off for each malocclusion1, 30, 31 (Table 1).
Cephalometric Measurements
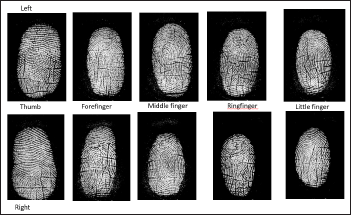
The subjects were asked to clean their hands with soap and water to remove the sweat, oil, and dirt from the skin surface. Fingerprints were collected digitally using DMIT Test software Research, provided by DMIT Lab India Bangalore compatible with Futronic FS80H model which is a digital fingerprint scanner (Figures 1 and 2).
Digital Scanning of Fingerprints Using Futronic FS80H Model.

Digital Scanning of Fingerprints.
The most frequently used lipstick-cellophane technique was implemented in the study, which provides good clarity and accuracy. A piece of colored lipstick was cut and applied to the lips with the lip brush (Figures 3 and 4). The subjects were then asked to gently rub both lips together to spread the lipstick evenly. Over the lipstick, a cellophane tape strip was placed and the lip impression was obtained by patting it first in the center and then pressing it toward the corners of the lips (Figure 5). The cellophane strip was then stuck to the white bond paper (Figure 6) for record-keeping and the lip impressions were then visualized with the use of a magnifying lens. Tsuchihashi’s classification 32 of lip prints was followed. For classification, the middle part of the lower lip (10 mm wide) was taken as a study area, similar to the study by Sivapathasundharam et al. 33 The lip print pattern was determined by counting the highest number of lines in this area which was similar to the Tsuchihashi’s classification.
Materials Used for Collection of Lip Prints and Application of Lip Color.

Application of Lip Color.

Collection of Lip Prints Using Cellophane Adhesive and Lip Pattern on Bond Paper.

Lip Pattern on Bond Paper.

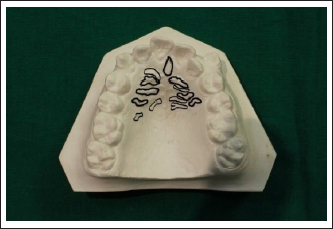
The subjects whose palatal rugae were visible on the cast models were included in the study. The number and pattern of palatal rugae were determined from maxillary cast models obtained before orthodontic treatment in all groups made from alginate impressions (Figure 7). The modified Thomas and Kotze classification system was used to determine the types of palatal rugae. 34
Tracing of the Palatal Rugae.
Statistical Analysis
The fingerprint, lip print, and palatal rugae morphology data analyzed were entered into a Master Excel sheet and descriptive statistics were performed. The data was analyzed using SPSS version 23. The frequencies of the patterns were calculated as a percentage and the chi-square test was done for comparison between the various parameters.
Results
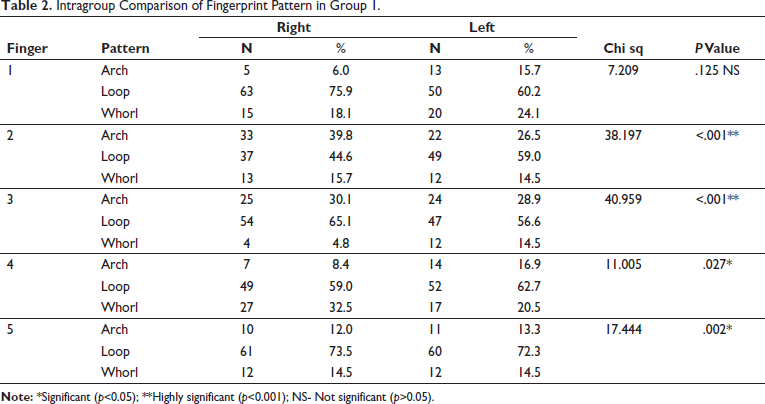
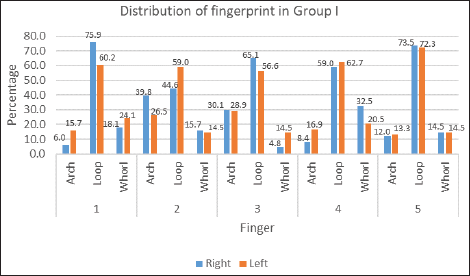
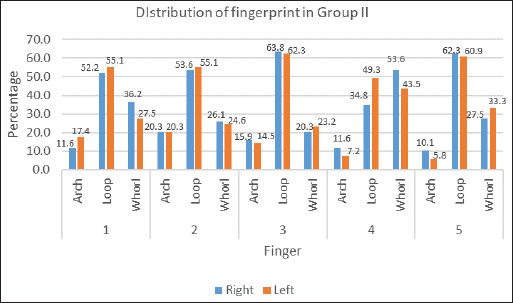
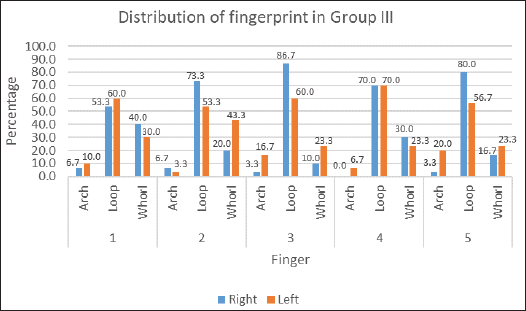
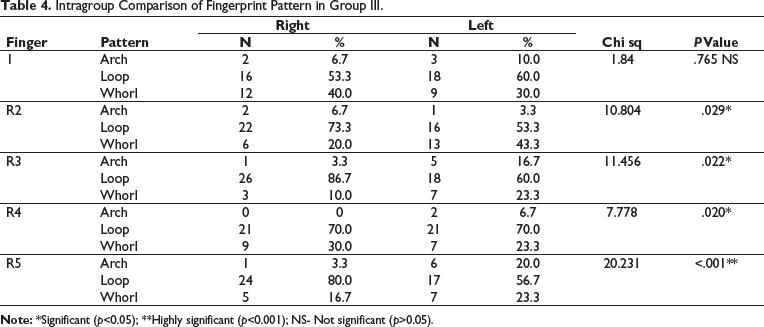
Group I, including class I malocclusion with no skeletal discrepancy, showed a loop pattern having the highest frequency of repetition in all the fingers of the right and left hand except in the first finger of the right and left hand (Table 2 and Figure 8). Group II, including class II malocclusion related to skeletal discrepancy, showed a loop pattern having the highest frequency of repetition in all the fingers of the right and left hand except in the fourth finger of the right hand which showed a predominant whorl pattern (Table 3 and Figure 9). Group III including class III malocclusion related to skeletal discrepancy showed a loop pattern having the highest frequency of repetition in all the fingers of the right and left hand. But in the fourth finger of the right and left hand, an arch pattern was absent (Table 4 and Figure 10).
Intragroup Comparison of Fingerprint Pattern in Group 1.
Intragroup Comparison of Fingerprint Pattern in Group 1.
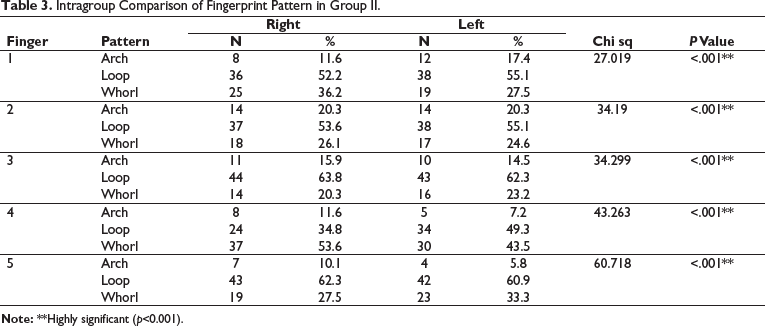
Intragroup Comparison of Fingerprint Pattern in Group II.
Intragroup Comparison of Fingerprint Pattern in Group III.
Intragroup Comparison of Fingerprint Pattern in Group II.
Intragroup Comparison of Fingerprint Pattern in Group III.
Intergroup Comparison of Lip Print Patterns.
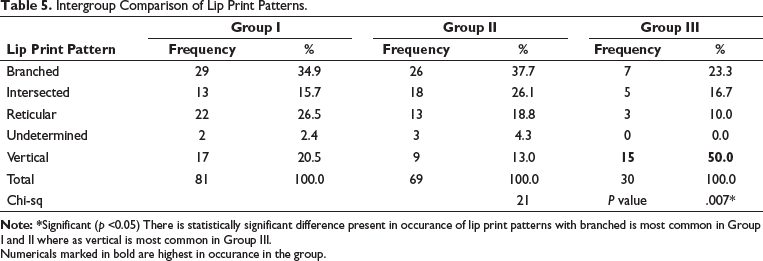
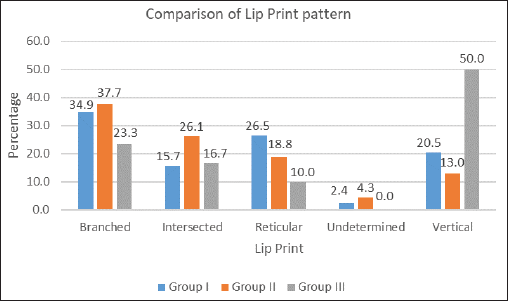
Branched patterned lip prints were most common in group I and group II, that is, in class I malocclusion with no skeletal discrepancy and class II malocclusion related to skeletal discrepancy respectively whereas vertical pattern was the most common in group III, that is in class III malocclusion related to skeletal discrepancy (Table 5 and Figure 11).
Intergroup Comparison of Lip Print Patterns.
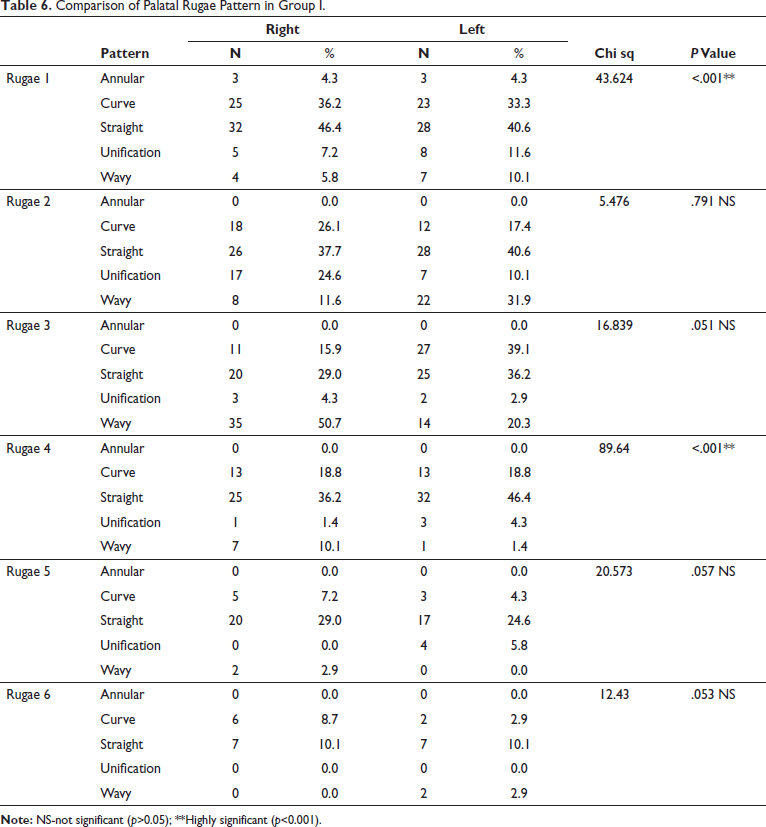
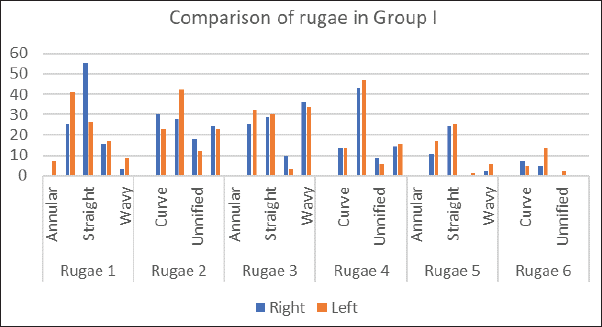
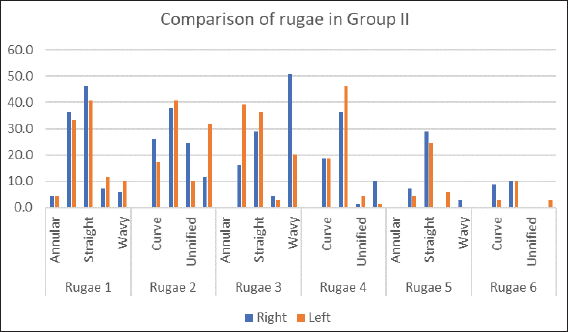
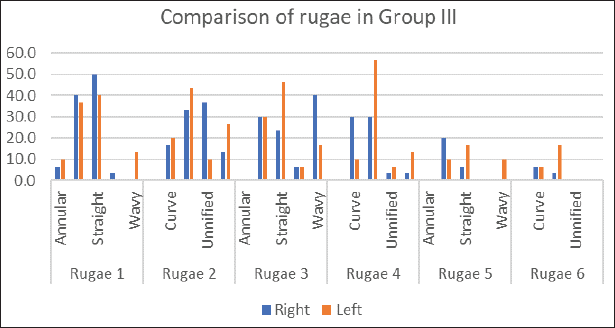
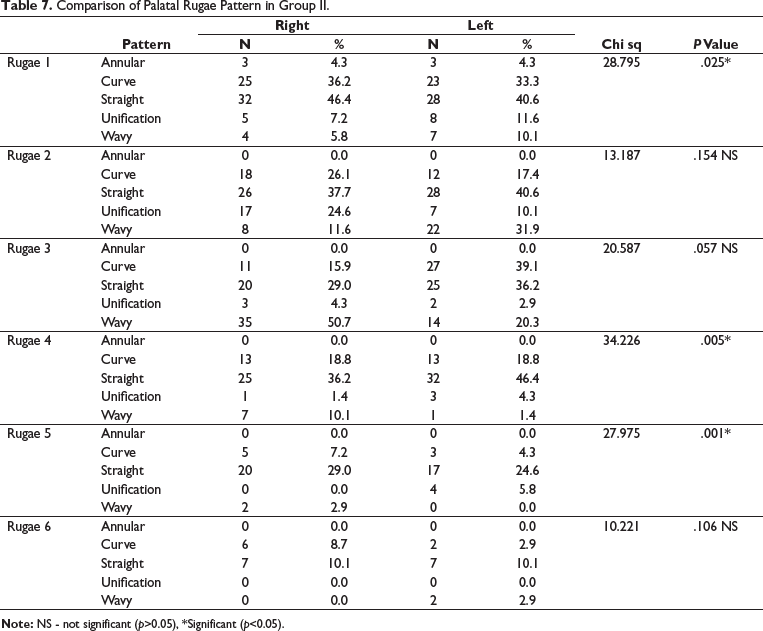
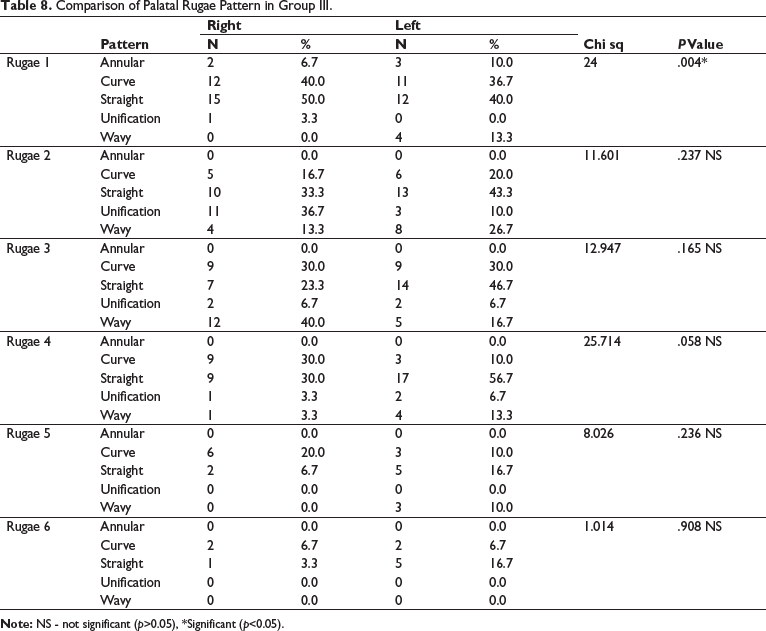
In Group 1, consisting of class I malocclusion with no skeletal discrepancy, a statistically significant difference was seen only in the patterns of primary rugae 1 and primary rugae 4 with straight patterned rugae showing the highest frequency (Table 6 and Figure 12). In group II, consisting of class II malocclusion related to skeletal discrepancy, a statistically significant difference was seen in the rugae pattern of primary rugae 1, primary rugae 4, and primary rugae 5 with straight patterned rugae showing the highest predominance (Table 7 and Figure 13). In group III, consisting of class III malocclusion related to skeletal discrepancy, a statistically significant difference was seen in the rugae pattern of primary rugae 1. Straight patterned rugae were the most frequent pattern (Table 8 and Figure 14).
Comparison of Palatal Rugae Pattern in Group I.
Comparison of Palatal Rugae Pattern in Group I.
Comparison of Palatal Rugae Pattern in Group II.
Comparison of Palatal Rugae Pattern in Group III.
Comparison of Palatal Rugae Pattern in Group II.
Comparison of Palatal Rugae Pattern in Group III.
Discussion
Dermatoglyphics are naturally occurring unique representative features present on the palms of hands and plantar surfaces of feet. 1 They are significant because they could provide important clues to early fetal development. The rationale behind dermatoglyphics being an indicator of intrauterine anomalies is because of its developmental time. Dermal ridges are developed by the sixth week of gestation and attain their determined size between the 12th and 13th weeks. 8 Other organs, teeth, and jaws also share the same developmental time frame as they develop concurrently. Craniofacial characteristics and dermal ridge patterns could be mainly genetically governed structures, but not exclusively. So, any abnormality in the formation stages of the organs or jaws could potentially be reflected in the dermatoglyphic patterns. 8
Sagittal skeletal discrepancies have a multifactorial etiology involving both the genetic and environmental factors. As skeletal malocclusion is not the norm, the genetic abnormality leading to this may be reproduced in the dermatoglyphic patterns. Because of its heterogenic nature and developmental time frame, the application of dermatoglyphics in various fields like modern medicine, anthropology, forensics, and dentistry has been widespread. 17
Recently, dermatoglyphics in combination with computed software helps in career using Dermatoglyphics Multiple Intelligence Test (DMIT) software. 35 The development of fingerprints of a person is directly associated with the development of the brain, and intelligence is too closely associated with the development of the brain. Hence, by reviewing the fingerprints of a person, various forms and manifestations of intelligence can be determined by DMIT.
Other unique dermatoglyphic patterns apart from fingerprints are lip prints and palatal rugae. It is specified that fingers, palms, lip, alveolus, and palate develop during the same embryonic period. 36 Lip prints are established at a very early period in comparison to sagittal jaw relation and dental relation. Palatal rugae are unique epidermal derivatives synonymous with lip prints and fingerprints. The left- and right-sided rugae patterns present on the palate vary in several factors. These include the number, shape, width, height, and location of palatal rugae to another. The palatal rugae are heterogeneous, and they can be classified into various patterns like fingerprints and lip prints.
Malocclusions related to skeletal discrepancies usually require complex single or bi-jaw orthognathic surgeries having the drawbacks of long treatment duration and also a psychological burden to the patient. 37 Early identification of developing malocclusion can be helpful in an interception and can ultimately be useful in reducing the need for complex surgeries. Thus, dermatoglyphics like fingerprints, lip prints, and palatal rugae can be used as a noninvasive, predictive tool for identifying developing malocclusion. In the present study, a total of 180 patients were taken and analyzed for the pattern of fingerprints, lip prints, and palatal rugae to malocclusions related to skeletal discrepancies. The 180 samples were divided into 3 groups based on cephalometric measurements as class I, class II and class III malocclusions with skeletal discrepancy.
The sample included 180 random patients representing the population of Hyderabad, Telangana. The ethnicity of the sample group was Asian, nationality Indian, more specifically from the southern part of India. According to the study by Shyam Kumar, 31 the ethnic features of this population included more convex profiles, and protrusive dentofacial patterns when compared to Caucasians.
Another study by Kalha 38 highlighted the different characteristics in both men and women from the south Indian region and found that men had thicker soft tissues, acute nasolabial angle, and longer faces, whereas the women had more amount of incisor exposure and increased interlabial gap. They concluded that the south Indian population has more deep-set midfacial structures and protrusive dentitions and more convex profiles.
Arora 39 concluded that the South Indian population had significantly protruded dentition, thinner soft-tissue drape, shorter vertical face heights, prominent forehead and midface with retrusive lower facial thirds, and convex profiles as compared to Caucasians.
The fingerprint pattern analysis results from the present study revealed that there was a statistically significant difference present in the occurrence of various fingerprint patterns on right and left hand in group I, that is, in class I malocclusion with no skeletal discrepancy which indicated the heterogeneous nature of the fingerprint patterns. The loop pattern had the highest frequency of repetition (61.4%). In class 1 malocclusion with no skeletal discrepancy, the key difference in fingerprint pattern was seen on the first finger of both hands which showed a statistically nonsignificant difference in the different patterns of fingerprints (Table 2 and Figure 8).
In group II, the class II malocclusion with skeletal discrepancy group, the results revealed that there was a statistically significant difference present in the occurrence of various fingerprint patterns on the right and left hand. The loop pattern had the highest frequency of repetition (55.1%). In class II malocclusion with skeletal discrepancy, the key difference in the fingerprint pattern was seen in the fourth finger of the right hand which showed an increase in a whorl pattern (53.6%). When compared to class I malocclusion with no skeletal discrepancy, there was an increase in the whorl pattern in the class II malocclusion with skeletal discrepancy (Table 3 and Figure 9).
In group III, class III malocclusion related to skeletal discrepancy, there was a statistically significant difference present in the occurrence of various fingerprint patterns on all fingers on the right and left hand. The loop pattern had the highest frequency of repetition (65%) in all the fingers of the right and left hands. In class III malocclusion with skeletal discrepancy, the key difference in the fingerprint pattern was seen in the first finger of the right and left hand which showed a nonsignificant difference, and the differing feature with other malocclusions is that there was an absence in the arch pattern on the fourth finger of the right and left hand (0%) (Table 4 and Figure 10).
In the present study, the loop pattern had the highest predominance in all the 3 groups which is the same as the study by George et al, 1 the loop pattern was the most frequently repeating pattern. There was an increased distribution of the whorl pattern in class II malocclusion and an increased distribution of the loop pattern in class III malocclusion. This is similar to the present study which also showed loop pattern as the most common pattern. In the class II malocclusion group, the fourth finger of the right hand showed a predominant whorl pattern and there was an increase in the whorl pattern in class II malocclusion when compared with class I malocclusion.
In another study by Jindal et al 40 on the association of dermatoglyphic features with different classes of malocclusion, although no fingerprint pattern was found to be specific for a particular class of malocclusion, in subjects with class II malocclusion increased frequency of whorl pattern especially on the thumb was observed, while subjects with class III malocclusion showed an increased frequency of plain arches.
Reddy et al 41 evaluated the dermatoglyphics parameters of individuals and corelated them with normal occlusions and various classes of malocclusions. It was concluded that there was an increase in twinned loops in class II malocclusions and the absence of radial loops in class III malocclusions was found to be statistically significant. In the present study, the loop pattern was also significant in class II malocclusion with only the fourth finger showing a whorl pattern. The other differences could be because Reddy et al compared dermatoglyphics to dental malocclusion whereas the present study compared dermatoglyphics to malocclusion related to skeletal discrepancy.
Tikare et al 42 assessed the relationship between fingerprints and malocclusion. It was concluded that although there was no statistically significant difference found between the fingerprint pattern and malocclusions, it was noted that the whorl pattern showed the highest predominance in class I and class II malocclusions which are different from the current study in that loop pattern was the most prominently repeating feature, although, in class II malocclusion, the fourth finger on the right hand showed predominant whorl pattern. The difference could be because of the large sample size in the study by Tikare and the concerned age group which was 12 to 16 years.
Shetty et al 43 conducted a study to explore an association, if any, between the dermatoglyphic patterns and type of malocclusion. Statistically, a significant association was seen with loop ridge pattern and class I normal occlusion, and class III malocclusion. It was in accordance with the present study in which class I, II, and III malocclusions with related skeletal discrepancies showed statistically significant difference with loop pattern.
Baswaraj et al 44 determined the correlation between dermatoglyphics and malocclusion. It was concluded that loops were found to increase and the whorls decreased, with increasing severity of malocclusion which is similar to the present study in which the loop pattern showed the most frequency in malocclusions with related skeletal discrepancies.
Within the lip prints the branched pattern was the most common in group I and group II, that is, class I malocclusion with no skeletal discrepancy and class II malocclusion related to skeletal discrepancy, respectively, whereas the vertical pattern was the most common in group III, that is in class III malocclusion related to skeletal discrepancy.
In group I, including class I malocclusion with no skeletal discrepancy, the branched lip pattern was the most prevalent followed by the reticular pattern, vertical pattern, intersected pattern, and undetermined pattern. In group II, including class II malocclusion with skeletal discrepancy, the branched lip pattern was the most prevalent followed by the intersected pattern, reticular pattern, vertical pattern, and undetermined pattern. In group III, including class III malocclusion with skeletal discrepancy, the vertical pattern was the most prevalent followed by the branched pattern, intersected pattern, and reticular pattern (Table 5 and Figure 11).
Kulkarni et al 45 assessed 90 subjects to find a correlation between sagittal skeletal jaw relation and lip prints. The patients were categorized into skeletal class I, class II, and class III. Lip prints obtained were analyzed. It was concluded that a significant difference was observed in the lip print pattern and the quadrants of upper and lower lips. Raghav et al 5 evaluated the correlation between lip prints and different skeletal malocclusions. The prevalence of vertical lip patterns was significantly higher in subjects having skeletal class III malocclusion.
For the palatal rugae analysis, the maxillary casts were used to analyze the rugae pattern using Thomas and Kotze’s classification of rugae morphology. For palatal rugae pattern, class I malocclusion with no skeletal discrepancy showed statistically significant difference only in straight pattered rugae for primary rugae 1 and primary rugae 4. Class II malocclusion related to skeletal discrepancy showed a statistically significant difference in primary rugae 1, 4, and 5 and class III malocclusion related to skeletal discrepancy showed statistically significant difference only in primary rugae 1 (Tables 6–8 and Figures 12–14).
Kapoor et al 29 concluded that the palatal rugae in all malocclusions showed a predominantly curvy pattern but in class I and class III patients on the left side for which the forking-diverging type was mainly seen. The results from the study done by Oral et al 34 showed wavy and curved types as the most common types of rugae patterns in all groups (class I, class II, class III). This could be due to the difference in the races included in the study. Fatima et al 46 concluded that the pattern of palatal rugae was found to be significantly different among the malocclusion groups with the curved pattern showing the highest frequency. However, the result in the present study, of the straight rugae pattern having the most predominance, was not consistence with these studies.
The most consistent parameter among the 3 is the fingerprint pattern. Several studies have shown a significant correlation between the fingerprints and the malocclusion as both follow a hereditary pattern. They follow a polygenic pattern of inheritance. Like many other complex traits, studies suggest that both genetic and environmental factors play a role in the formation of dermal ridge derivatives. Studies on the genetic inheritance of dermatoglyphic patterns to investigate the embryogenesis of dermatoglyphic patterns reported a genetic basis and no alteration in the structure of ridge patterns after birth. Also, the heterogenic nature of the fingerprints can aid in assessing complex genetic traits in the future and also help in differentiating between the different malocclusions related to skeletal discrepancy. Also reflecting its heterogenic nature, fingerprint measuring patterns are wide like counting the frequency of ridges in a particular pattern, and the disposition of triradii (the junctional area where 3 sets of parallel ridges meet). Also, the basic classification of arches, whorls, and loops can be further divided into many distinct patterns like the tented arch, radial loop, ulnar loop, and double pocket loop. Central pocket loop, double whorl, and composite whorl patterns.
When compared to the other patterns like the lip prints and the palatal rugae, the collection of fingerprints is more accurate than the other two. A digital image of the palm can be obtained using scanners which makes the analysis accurate. Lip print collection is technique sensitive when collected using the cellophane paper method and analyzing them becomes difficult if not stored properly which leads to smudging of the lip print patterns. Although a digital scan of the palatal rugae patterns can be obtained, the results of the present study did not show any statistically significant results in all the rugae patterns whereas finger and lip print patterns showed statistically significant differences in the various patterns.
Dermatoglyphic patterns can be easily visualized and their ease and inexpensiveness to record them can act as a major factor in mass screening tests. Combining digital technologies for their recording can increase its reliability as a screening tool. Based on the literature and the results of the present study it is established that dermatoglyphics may be associated significantly with malocclusions related to skeletal discrepancies.
The simplicity, inexpensiveness, and heterogeneous nature of the dermatoglyphics when combined with other clinical and other investigative features may be used as a screening device and as a non-invasive marker as an adjunctive diagnostic tool to predict or detect the early development of malocclusions with skeletal discrepancies when there is no access to advanced diagnostic aids so that preventive and interceptive treatment can be planned which remains one of the main goals of Orthodontists.
The present study had some limitations. This was a cross-sectional study as the subjects recruited were those who visited the hospital for treatment purposes. To establish an association between dermatoglyphic patterns and sagittal discrepancies, observations should be made on a larger sample that is representative of the entire population. Lip print collection is technique sensitive. The use of the cellophane paper method, although, is a universal method used for the collection of lip prints which poses a problem in that it is difficult to record the whole pattern of lip print if not collected properly. There is also a long-term complication of the collected lip prints fading away if not stored properly. Ethnic, racial variations, congenital, environmental, and local factors are some of the many factors influencing the development of malocclusions. Further longitudinal studies on large sample sizes, according to their racial and ethnic background using digital analysis, can be undertaken to warrant an accurate result.
Conclusion
The following conclusions can be drawn from the following study.
Class I malocclusion with no skeletal discrepancy showed a statistically significant difference in the loop fingerprint patterns on all fingers except the first finger on the right and left hand, branched lip pattern, and straight palatal rugae pattern in primary rugae 1 and 4. Class II malocclusion related to skeletal discrepancy showed a statistically significant difference in the loop pattern on all fingers except in the fourth finger of the right hand which showed a whorl pattern, branched lip pattern, and straight palatal rugae pattern in primary rugae 1, 4, and 5. Class III malocclusion related to skeletal discrepancy showed a statistically significant difference in the loop pattern on all fingers except in the fourth finger of the right hand which showed an absence of arch pattern, vertical lip print pattern, and straight palatal rugae pattern in primary rugae 1.
From the present study results, it can be inferred that there is a statistically significant association present between dermatoglyphic-like patterns and malocclusions. It could be used as an easily accessible and noninvasive marker for the prediction of malocclusions with skeletal discrepancies which might offer important practical and or clinical implications for preventive and interceptive orthodontics. Further longitudinal studies on each of these groups in large sample sizes, according to their racial and ethnic backgrounds, are necessary.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The ethical clearance from the institution was obtained (IEC No: PMVIDS&RC/IEC/ORTHO/DN/0237-2018).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.