
Abstract
This case report was presented at the Indian Board of Orthodontics examination under category I in September 2021. It demonstrates fixed orthodontic treatment of a 13-year-old female presenting with Angle’s Class I malocclusion on Class I skeletal base with an average growth pattern. This was complicated by a 7 mm overjet with proclination and crowding of the upper and lower labial segments. She also presented a reduced overbite and a centerline discrepancy of 1.5 mm. Lips were protruded and incompetent at rest with decreased nasolabial angle. Treatment involved extraction of all first premolars followed by fixed orthodontic mechanotherapy with preadjusted edgewise appliance (0.022 × 0.028” slot with MBT–McLaughlin Bennett and Trevisi prescription). Anchorage reinforcement in the upper arch was provided with mini-screw implants.
Introduction
Anchorage control is one of the most important factors for the successful outcome of orthodontic treatment. Although various extraoral anchorage devices can be used to augment anchorage during retraction of anterior teeth, the patient’s acceptability and compliance are always an issue because of esthetic and social concerns. 1 This lack of compliance can result in anchorage loss and poor orthodontic results. Over the years, various temporary anchorage devices have been introduced, which can be placed intraorally and used well without relying on the patient cooperation. Mini-implants, 2 miniplates, 3 mini-screws,4-6 endosseous implants, 7 infra-zygomatic crests, and buccal shelf screws 8 can be used as a source of anchorage. Among those, mini-screws or mini-implants have the advantage of easy insertion and removal, placement at various anatomic locations, immediate loading, and a low cost.
In the case presented below, mini-screws were used for en masse retraction of maxillary anterior teeth. Maximum anchorage was maintained throughout the retraction, and the desired results were achieved without any anchorage loss.
Pretreatment Assessment
Patient Details
R.S., a 13 years 9 months old female patient, reported with the chief complaint of “irregularly placed upper and lower front teeth.”
Clinical Examination: Extraoral Features
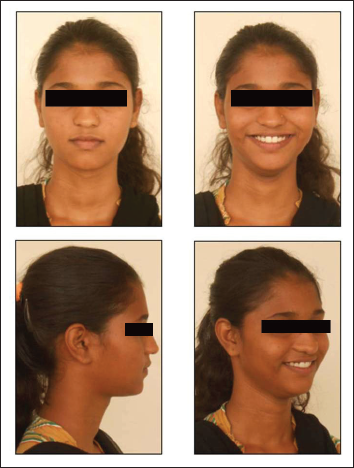
The skeletal assessment showed class l skeletal pattern with convex facial profile (Figure 1). Vertically normal lower anterior face height proportions were noted. Acceptable facial symmetry and balance were observed on frontal examination.
Pre-treatent Extra-oral Pictures

On soft tissue assessment, lips were protrusive and incompetent at rest with pronounced mentalis muscle activity. Decreased nasolabial angle was also present because of the proclinaton of upper anterior teeth.
Ptosis of left upper eyelid was present since birth, but the patient did not seek treatment for the same.
Clinical Examination: Intraoral Features
R.S. was well motivated and demonstrated fair oral hygiene with good gingival health. Hyperpigmentation of gingiva was evident (Figure 2). All the teeth up to second molars were present in each quadrant. Areas of plaque accumulation were present around gingival margins. Occlusal composite restorations were seen in mandibular first and second molars bilaterally.
Pre-treatent Intra-oral Pictures

Crowding/Spacing
Occlusal Features
Incisor relationship was class ll division 1 with an overjet of 7 mm and decreased overbite (10%), with upper incisors overlapping less than one-third of lower incisors. Buccal segments were in class l relationship bilaterally. The upper centerline coincided with facial midline. The lower centerline was shifted to right by 1.5 mm from midpoint of chin.
Individual tooth displacements were seen with palatally displaced upper lateral incisors and lingually displaced mandibular right lateral incisor.
General Radiographic Examination
Pretreatment Radiographs Taken
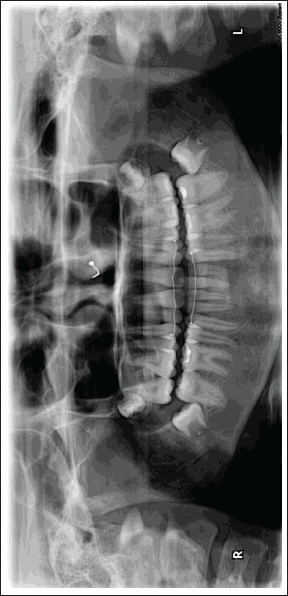
Dental panoramic tomogram - Figure 3 (September 1, 2018)
Pre-treatent Dental Panoramic Tomogram

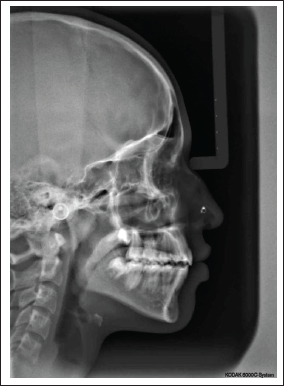
Lateral cephalogram - Figure 4 (September 1, 2018)
Pre-treatent Lateral Cephalogram

Relevant Radiographic Findings
The normal complement of permanent teeth was present with no abnormalities in tooth forms and the surrounding structures. Upper and lower third molars were in the development stages. The bone level was normal.
Cephalometric Interpretation
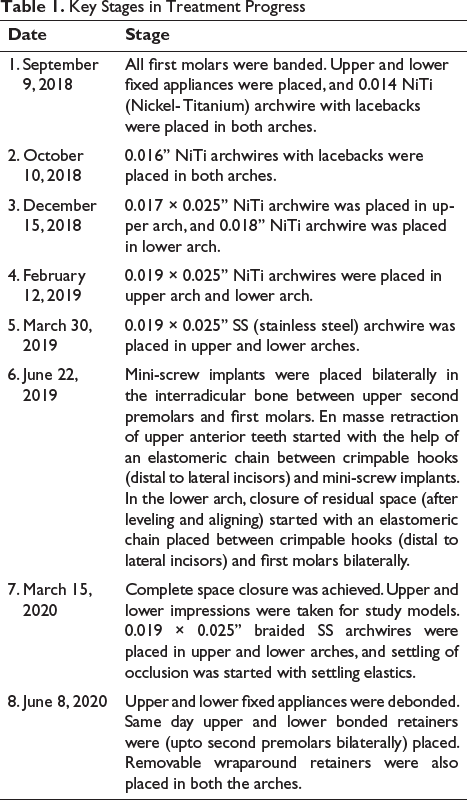
Key Stages in Treatment Progress
Skeletal
Cephalometric Assessment.
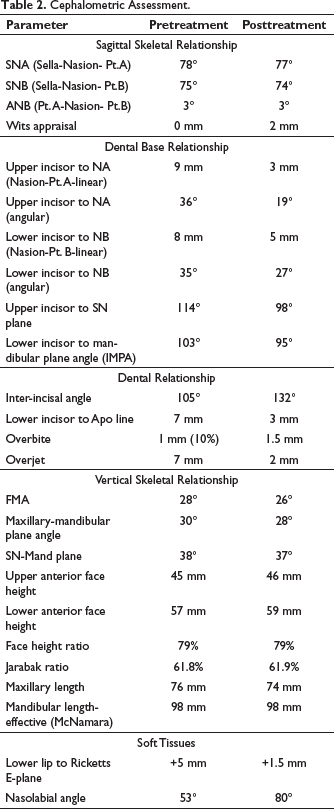
The vertical proportions assessed by FMA (Frankfurt Mandibular Plane angle), maxillo-mandibular plane angle, and face-height ratio were on the higher side of the normal range showing an average growth pattern and supporting the clinical findings.
Dental
Upper and lower incisors were proclined. As a result, the interincisal angle was reduced to 105°. Lower incisal edge was positioned anteriorly relative to point A-Pog line (+7 mm), consistent with lower anterior proclination.
Soft Tissues
Both upper and lower lips were protrusive relative to Ricketts E plane. Upper lip showed decreased nasolabial angle.
Diagnostic Summary
R.S., a 13-year-old female, presented with the chief complaint of irregularly placed upper and lower front teeth. On examination and analysis of relevant records, she was diagnosed with Angle’s class I malocclusion on class I skeletal base with an average growth pattern. This was complicated by a 7 mm overjet with proclination and crowding of upper and lower labial segments (Figure 1 and 2). She also presented a reduced overbite and a centerline discrepancy of 1.5 mm. Lips were protruded and incompetent at rest with decreased nasolabial angle. The dental health component of IOTN (Index of Orthodontic Treatment Need) was recorded as
Problem List
Areas of plaque accumulation
Incompetent and protrusive lips
7 mm overjet
Upper and lower labial segments crowding
Bimaxillary proclination
Reduced overbite
1.5 mm centerline discrepancy
Aims and Objectives of Treatment
Plaque removal
Relief of crowding
Level, align, and coordinate the dental arches
Reduce the overjet and achieve competent lips at rest
Correct the overbite
Correct centerline discrepancy
Maintain class l molar relationship and achieve class l incisor relationship
Retain corrected results
Treatment Plan
Treatment plan included extraction of all first premolars for relieving crowding. Upper and lower preadjusted edgewise fixed appliances (0.022 × 0.028” slot) with MBT - McLaughlin Bennett and Trevisi prescription was used.
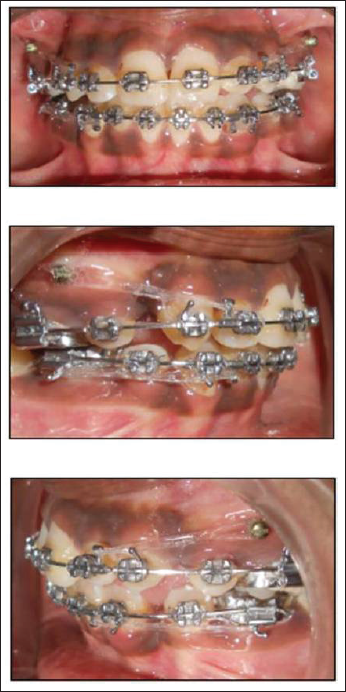
To maintain high anchorage during space closure, mini-screw implants were placed in the upper arch in the interradicular area between second premolar and first molar bilaterally and a lingual arch in the lower arch for anchorage reinforcement.
Proposed retention strategy: upper and lower bonded retainers (upto second premolar bilaterally) along with removable upper and lower wraparound retainers.
Prognosis for stability: provided that the general arch form was maintained and a good occlusal interdigitation was achieved, the long-term stability of the treatment changes was considered good. In order to maximize the stability of overjet correction, it was important to retract the upper incisors within the control of the lower lip. However, owing to the large contact point displacements in the maxillary and mandibular labial segment, upper and lower bonded retainers along with removable wraparound retainers were considered appropriate.
Treatment
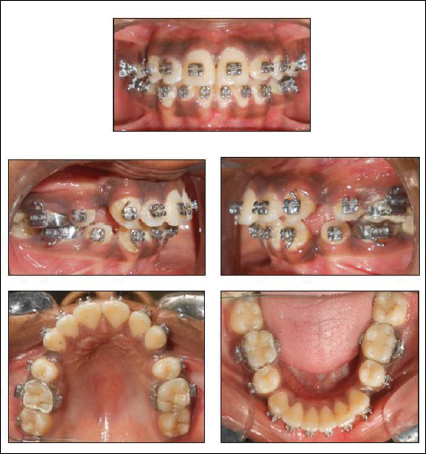
Fixed orthodontic treatment started after extraction of all first premolars. Treatment Progress is depicted in figures 5-6 and table 1.
Intra-oral pictures after Leveling and Alignment
Space closure with Mini-screw Implant anchorage
Age at start of active treatment: 13 years 9 months
Age at end of active treatment: 15 years 6 months
Post-treatment Assessment
Occlusal Features
After treatment, the incisor relationship was class I with an overjet of 1.5 mm and normal overbite (Figures 7 and 8). The maxillary and mandibular centerlines coincided with each other and the facial midline. The buccal segment relationship was maintained in a class l relationship bilaterally. No individual tooth displacements were present after the treatment. Mutually protected occlusion was achieved with the orthodontic treatment.
Post-treatment Extra-oral pictures
Post-treatment Intra-oral pictures

Complications Encountered During Treatment
Treatment progress was hindered by 3 broken brace appointments. All were related to debonding of brackets from lower incisors.
Occlusal Indices
IOTN dental health component improved from 4d to 1, and aesthetic component improved from score 7 to 1. Peer assessment rating also improved by “100%” (from score 52 to 0).
Radiographs Taken at End of Treatment
DPT (Dental Panoramic Tomogram) - Figure 9 (June 8, 2020)
Lateral Cephalogram - Figure 10 (June 8, 2020)
Post-treatment Dental Panoramic Tomogram
Post-treatment Lateral Cephalogram
Relevant Findings
No obvious pathology was noted.
No change in root length of upper and lower teeth was observed.
Good root parallelism was achieved.
Interpretation of Cephalometric Changes Skeletal
The SNA (Sella-Nasion- Pt.A) and SNB (Sella-Nasion- Pt.B) values were reduced by 1° suggesting posterior remodeling of A and B points, respectively, because of upper and lower anterior retraction (Table 2).
Vertical growth continued throughout the treatment as confirmed by a 3 mm increase in overall anterior face height. But vertical proportions did not change significantly. Angular measurements were recorded to be within the normal range.
Dental
The upper incisor to SN (Sella-Nasion) plane angle was reduced by 16° (from 114° to 98°) following the retraction of upper anterior. The lower incisor to mandibular plane was reduced by 8° (from 103° to 95°) following retraction of lower anterior.
The upper and lower molars moved minimally in an anteroposterior direction, as confirmed in superimposition (Figure 11).
Superimpositions
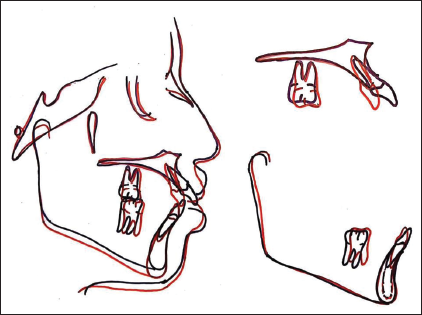
The lower incisal edge moved back by 4 mm (7 mm to 3 mm) relative to A-Pog line.
Soft Tissues
Nasolabial angle increased by 27° (from 53° to 80°). Lower lip position relative to Ricketts E plane was reduced by 3.5 mm. Both can be explained by the change in upper and lower incisor position during orthodontic treatment.
Section 4: Critical Appraisal
R.S. was successfully treated by orthodontic treatment over 21 months. The original treatment aims were accomplished, and the patient’s presenting complaint was addressed. R.S. was notably pleased with the treatment outcome. A good occlusal and aesthetic result was achieved, and this was reflected in the PAR (PeerAssessment Rating) and IOTN (Index of Orthodontic Treatment Need) scores.
Skeletal
Posterior repositioning of A and B points was seen with upper and lower incisor retraction, respectively, without any change in the skeletal relationship between upper and lower jaws. Vertical skeletal growth continued throughout treatment without significant change in the vertical relationship of the upper and lower jaw.
Dental
The 7 mm overjet was successfully reduced within normal limits. The overbite was also increased to normal limits. The final occlusal fit was good.
The marginal gingival contour was irregular with the upper left central incisor, for which gingival recontouring was advised. But the patient did not agree to the same.
Soft Tissues
The favorable soft tissue drape facilitated orthodontic treatment without detriment to dentofacial appearance. Lips were competent at the end of treatment, with the upper incisors under the control of the lower lip. These are favorable features for long-term stability of overjet correction. However, owing to the extent of the pretreatment contact point displacements in the maxillary and mandibular anterior teeth, upper and lower bonded retainers along with removable wraparound retainers were placed.
Iatrogenic
The posttreatment radiographs identified no change in root length of the upper and lower anteriors. Enamel decalcifications were evident on removal of the fixed appliances. Oral hygiene instructions were given, and topical fluoride application in the form of mouth rinse was prescribed. A mild apical shift of the marginal gingival was observed in relation to upper left central incisor and lower right and left central incisors.
Conclusion
This case report demonstrates the ability of mini-screws to maintain maximum anchorage during retraction in severe dentoalveolar protrusion.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.