
Abstract
Mini-implant or temporary anchorage device (TAD) have now become an important aspect in the Orthodontic practice worldwide. It has increased the envelope of discrepancy for Orthodontic correction, as more anchorage can be harnessed owing to TAD’s. Placement of mini-screw in particular has to be very precise in order to get maximum anchorage without hampering adjacent structures like tooth root and periodontal ligament. Angulation of the screw with respect to bone is of equal importance to gain biomechanical advantage and achieve necessary stability. We have developed a 3-D mini-implant guide, called MIG-20 using basic orthodontic material and then its final design was casted. Placement and working of MIG-20 is explained in this article. Design of MIG-20 has been patented by the authors and the working is been copyrighted. A study has been conducted to evaluate the accuracy of MIG-20 on patients. It has proven to give accurate results in mini-screw placement.
Introduction
Mini-implants have now become an integral part of orthodontic therapy as they provide absolute anchorage during orthodontic treatment. It can increase a patient’s treatment options and improve the functional outcomes of treatment. Root contact and marginal bone location are considered to be the main risk factors for screw failure. It is seen that when marginal bone and the mini-screw are separated by less than 1 mm, the stability of the mini-implant is grossly affected.1, 2 It is recommended that a 2D radiograph, accompanied by a mini-screw guide, is compulsory for placing the temporary anchorage device accurately. 3 Numerous researchers have proposed different designs of mini-implant guides to help ensure precise positioning during mini-implant placement. 4
This article describes a 3D guide, the Mini-implant Placement Guiding Device (MIG-20), which was innovated by us in our department and patented by the Indian Patent Office. The placement of a mini-screw using this MIG-20 is explained in this article. Approval from the ethical committee was obtained before using this on patients.
Components
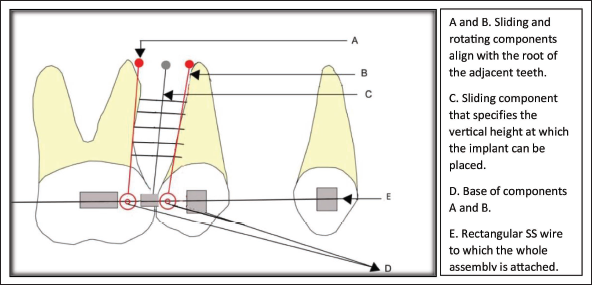
MIG-20 is made up of three sliding and rotating components:
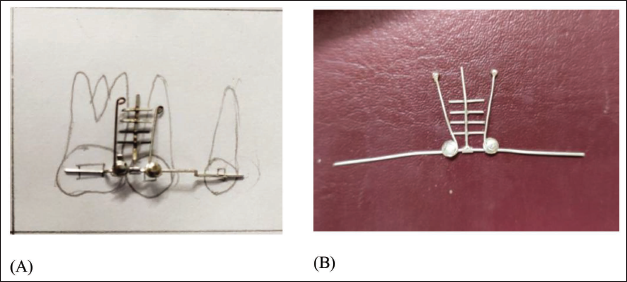
Two-wire components are at the side, which are used to accurately locate the long axis of the adjacent root of the teeth (Figure 1A and C). Thus, it considers the axial inclination of the tooth root and can be adjusted according to root angulation. The wire component in the center (Figure 1B) is used to determine the appropriate vertical height at which the mini-implant should be placed. This ensures that the adjacent root structures remain untouched while placing the mini-implant. Figure 1D is the base of the sliding component (Figure 1A and C). Figure 1D was initially made using a short crimpable hook and a lingual button (orthodontic attachments). The crimpable hook was loosely crimped to the rectangular SS wire; this allowed sliding of the component on the SS wire, onto which the lingual button was soldered. Figure 1A and C were loosely tied with ligature wire to the lingual button, thus making it feasible to rotate and slide. Figure 1E is the piece of orthodontic rectangular wire to which all the components are attached. The whole assembly of MIG-20 was initially made out of small orthodontic metal components, which have been soldered and welded (Figure 2A). Later on, the final design was cast (Figure 2B).
Design of the Appliance. (A) Initially Fabricated Using Orthodontic Material. (B) Final Design Cast.
Placement
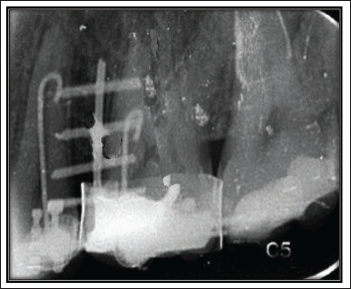
The mini-implant guide, that is, MIG-20, is positioned in the patient’s mouth as shown in Figure 3. The whole assembly is on the piece of orthodontic rectangular arch wire; one end is placed in the molar tube, and the other end is placed in the canine bracket. (The clinician needs to remove any base arch wire previously placed in order to use the assembly.) A clinical assessment is performed, positioning Part A near the mesial root surface of the first molar and Part C near the distal surface of the second premolar. Part B is adjusted to slide between these two teeth. A radiovisiography (RVG) is then captured for evaluation (Figure 4). If the radiograph confirms the accuracy of the clinical positioning, as illustrated in Figure 3, the clinician can use this setup as a guide. Parts A and C help prevent contact with the adjacent root surfaces, while Part B determines the appropriate vertical placement of the implant. Using this approach, the mini-implant can be accurately placed with the assistance of MIG-20.

Clinical Application
A study titled “Comparative Evaluation of the Stability of Orthodontic Temporary Anchorage Device With and Without the Use of Implant Placement Guide in Adults—An In-Vivo Study” was conducted and suggests that the MIG-20 guide facilitates precise placement of mini-implants by improving accuracy in the mesiodistal and vertical dimensions as well as angulation. It also contributes to better primary stability, which is essential for enhancing the success rate of orthodontic implants. 5 These factors are the primary objectives necessary for increasing the success of orthodontic implants.
Recognitions
MIG-20 has been granted a patent by the Indian Patent Office on March 3rd, 2020.
A device for mini-implant placement guiding has been registered in the Registers of Patents by the Commissioner of Patents, Patent Office, Australia.
MIG-20 has been nominated for the state-level research awards in the category of Padma Vibhushan Professor Dr. R.A. Mashelkar Award for Best Patent in Oral Healthcare.
The idea of MIG-20 has been honored with an award of appreciation by the local branch of the Indian Dental Association.
A copyright has been published explaining the “Protocol for the use of Mini-Implant Guide (MIG-20).”
Conclusion
MIG-20 is made up of stainless-steel components that can be placed into the already fitted fixed orthodontic appliance to take radiographs. A single implant guide can be used in all patients and all four quadrants without being modified for the same. It is autoclavable as well as radio-opaque. An exciting feature about MIG-20 is that it is completely made with routinely used orthodontic material. Thus, it is cost-effective.
Footnotes
Acknowledgments
The author (Shriya Prakash Murarka) acknowledges the contribution of guide, Dr. Sunita Shrivastav, ma’am, in enlightening on the subject and encouraging innovation of MIG-20. The author is thankful to the Department of Orthodontics, DMIHER, for providing the necessary amenities to carry out research in the subject. The author acknowledges the assistance of colleagues during the development of this equipment. The author acknowledges the guidance received from the Research House, DMIHER, in article preparation and submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical consent was obtained from the Institutional Ethical Committee, DMIHER, before employing the device in the patient.
The procedure of using the device was explained to the patient, and informed consent was obtained before starting.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.