
Abstract
Introduction:
Respiratory function has a direct relationship with the pharyngeal airway dimension and mandibular morphology. The objective of the present study was to compare and correlate pharyngeal airway, mandibular morphology, and tongue position in hyperdivergent and normodivergent patterns using standard cephalometric radiographs.
Materials and Methods:
A total of 130 individuals with age 13 to 19 years, with no craniofacial skeletal abnormalities, were taken. The individuals were divided into 2 groups based on their Frankfort mandibular angle (FMA). Group I consist of 65 hyperdivergent individuals (34 males, 31 females) with FMA >28. Group II consisted of 65 normodivergent individuals (28 males, 37 females) with FMA >25 to <28. For statistical analysis, variables were analyzed by unpaired t-test, with P value <.05. Correlation between the pharyngeal space and the other variables was analyzed with the Pearson correlation test.
Results:
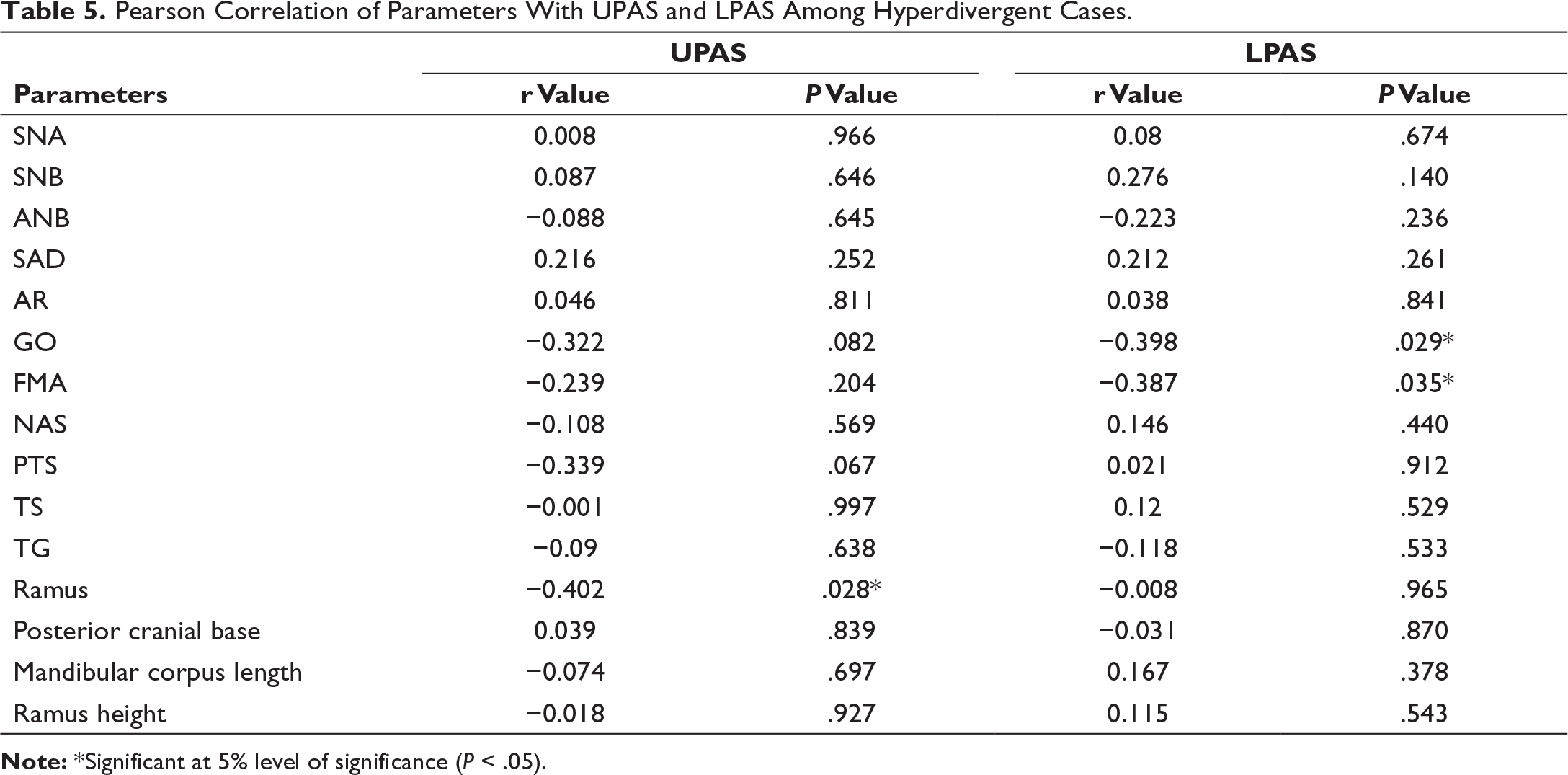
Upper pharyngeal airway space in hyperdivergent growth pattern exhibited a significant negative correlation with ramus width (r = −0.02 and P = .028). Gonial angle showed a statistically significant inverse correlation with lower pharyngeal airway space (r = −0.398 and P = .029). A-point-nasion-B-point (ANB), saddle angle, posterior tongue space, tongue gap, and pharyngeal airway among normodivergent subjects, showed a statistically significant negative correlation.
Conclusion:
The present study showed a significant relationship between pharyngeal airway space, craniofacial morphology, and tongue position suggesting that narrower airway space may be a causative factor for altered dentofacial skeletal patterns. Reduced ramus width, lowered tongue, and narrower posterior pharyngeal wall might be a balancing mechanism set for morphological imbalance in hyperdivergent pattern.
Introduction
In orthodontic diagnosis and treatment planning, functional examination of the respiratory system of the patient plays an important role. The upper airway spaces which include the hypopharynx, nasopharynx, and oropharynx play a significant role in the process of deglutition and respiration. 1 Abnormal nasorespiratory function is related with inadequacy airway which can precipitate to mouth breathing habit. 2
According to Solow’s hypothesis, oral and pharyngeal soft tissues could be influenced by a change in head, jaw, or tongue posture. This altered breathing pattern results in the downward movement of the mandible and the tongue and an extended head posture 3 ; altered head posture could result in stretching of the soft tissue musculature which in turn leads to the overall rotation of the mandible in backward direction. 4
Another important factor in maintaining the airway and head posture is the relative position of the hyoid bone to the mandible and cranial base. When the tongue posture is lowered, the geniohyoid muscle may increase the mandibular load that had a direct impact on the developing craniofacial structures. 5
According to Enlow’s counterpart principle, another factor that influences pharyngeal space is the middle cranial fossa which is the counterpart to ramus width. 6 Trenouth and Timms stated that there exists a correlation among functions of oropharyngeal airway and craniofacial morphology and showed a significant correlation between mandibular length and oropharyngeal airway. 7 Parkkinen et al, 8 confirmed in their study that dimensions of the retropalatal region and nasopharynx can be measured from lateral cephalogram with much validity.
Although studies have shown that cephalometric measurements give 2-dimensional information of 3-dimensional objects, they also considered it as a reliable screening tool for evaluation and estimation of airway, adenoids, and tongue.8, 9 Cephalometric analysis by using software enables a quick, user-friendly, and time-saving method when compared to manual tracing. 10 As there is a direct correlation between the pharynx, mandible, and tongue, any orthodontic intervention may influence the pharyngeal airway space; a detailed knowledge of these structures would help in orthodontic diagnosis and treatment planning. 11
Previous studies2, 4, 5, 7 attempting to measure pharyngeal airway space did not take into account the correlation between the oropharynx, mandibular morphology, and tongue position. Thus, the present study aimed to evaluate the oropharynx of the individuals with normal nasorespiratory functions and also to correlate oropharyngeal airway dimensions, mandibular morphology, and tongue in hyperdivergent and normodivergent individuals on standard cephalometric radiographs.
Materials and Methods
A total of 130 individuals were selected from the patient database of Orthodontic Department of Al-Badar Dental College, Kalaburagi, Karnataka. Standard digital pretreatment lateral cephalograms (CS IMAGING TECHNIQUE CS 8100) with an age of 13 to 19 years were taken with the Frankfort horizontal plane parallel to the floor, and subjects should be in centric occlusion/centric relation during the expiratory phase. The subjects were advised to place the tongue in a relaxed posture and to breathe normally. A piece of lead foil was fixed with glass ionomer cement on the tip of the tongue and a coating of barium paste was applied over the tongue (Figure 1). 5
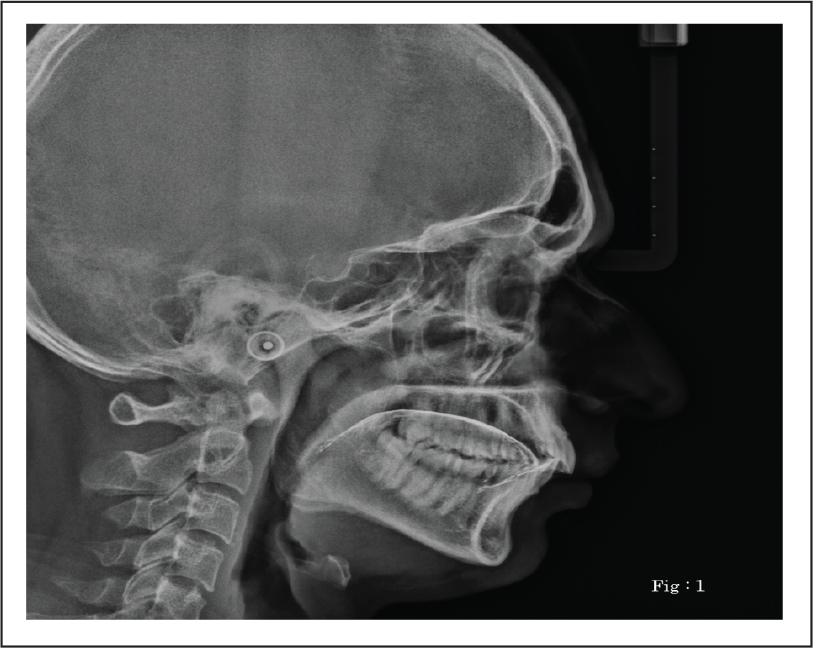
Lateral Cephalogram Showing Tongue Outline with Barium Coating and Lead Foil Fixed on the Tip of the Tongue.
Before digitization of the landmark with the Facad software (3.10.1 Swedish company), calibration of the films was done by digitizing 2 points on the ruler within the cassette. Digital images (DICOM format) were assessed for linear and angular measurements using Facad software (3.10.1). Once the set landmarks has been digitized, the variables are generated automatically by the program. Exclusion criteria included patients, who had orthognathic surgery, nasal obstruction, history of enlarged adenoids or ear-nose-throat infections, or surgery, cleft, mouth breathing habits, tongue thrusting habit, and obstructive sleep apnea (OSA). 12 OSA subjects were eliminated based on the history of snoring, daytime sleepiness, pauses in breathing during sleep or choking, and nocturnal awakening. The diagnostic criteria set for inclusion of OSA by International Classification of Sleep Disorders includes the presence of at least one of the mentioned symptoms. 12
The power of sample size was analyzed by the formula n = f (α/2, β) × 2 × σ2/(µ1 − µ2)2
where µ1 and µ2 are mean outcomes and σ is the standard deviation.
From this formula, it was determined that a total of 130 individuals would be needed to conduct a study with 90% power (α = 0.001).
The 130 individuals (age 13-19 years) were categorized into 2 groups. Each group consisted of 65 individuals, group I consisted of 34 males, 31 females as hyperdivergent (Frankfort mandibular angle [FMA] >28) and group II consisted of 28 males, 37 females as a control group or normodivergent (FMA >25 to <28) according to previous studies.13, 14
The examiner executed all measurements 5 times, with a gap of 1 day, to have a high level of reproducibility of the method and to maximize the intraexaminer reliability. The intraclass correlation coefficient was evaluated to assess the reproducibility of the measurements by the examiner.
The following variables were assessed in the study.
Craniofacial Analysis
Airway Space and Tongue Measurement (Figures 2–3)
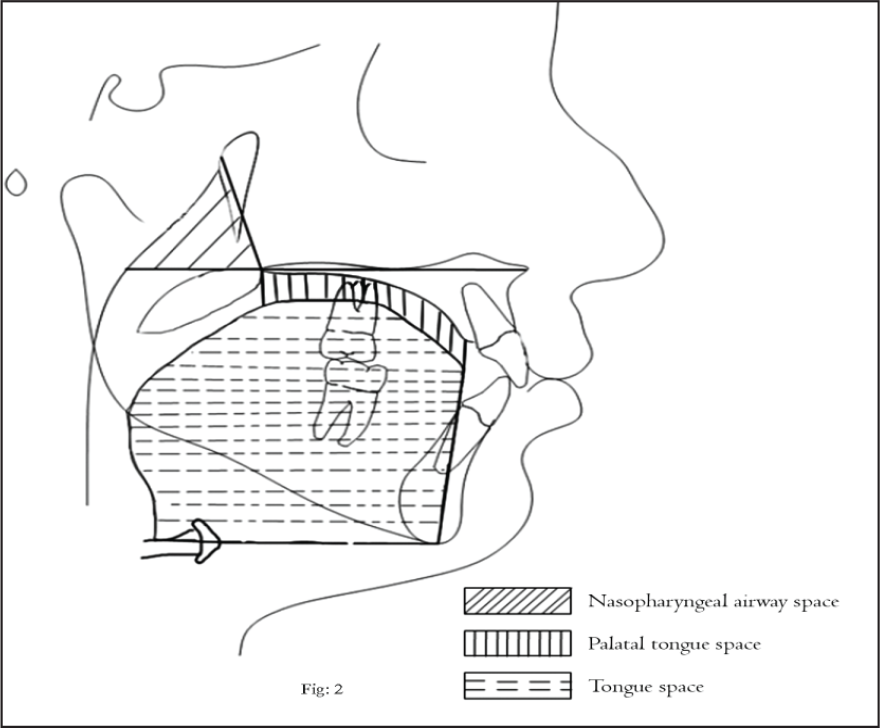
Cephalometric Landmarks for Nasopharyngeal Airway Space and Tongue: Formed by Palatal Plane and the Pt-PNS Posterior Nasopharyngeal Line. Palatal Tongue Space: Space Between Tongue and Palate From the Line Perpendicular to the Palatal Plane at the Incisive Foramen to the Line Perpendicular to the Palatal Plane at the PNS. Tongue Space: Area Formed by Superior and Posterior Borders of the Tongue and T, Me, H1, and H2.
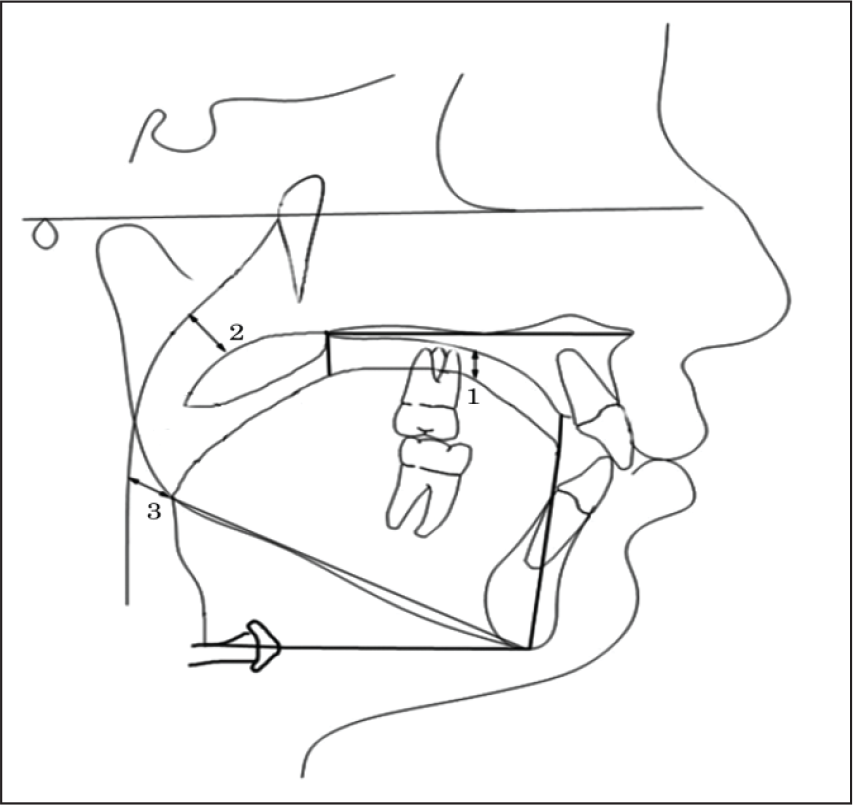
(1) Tongue Gap; (2) Upper Pharyngeal Airway Space; and (3) Lower Pharyngeal Airway Space.
Angular Measurement (Figure 4)
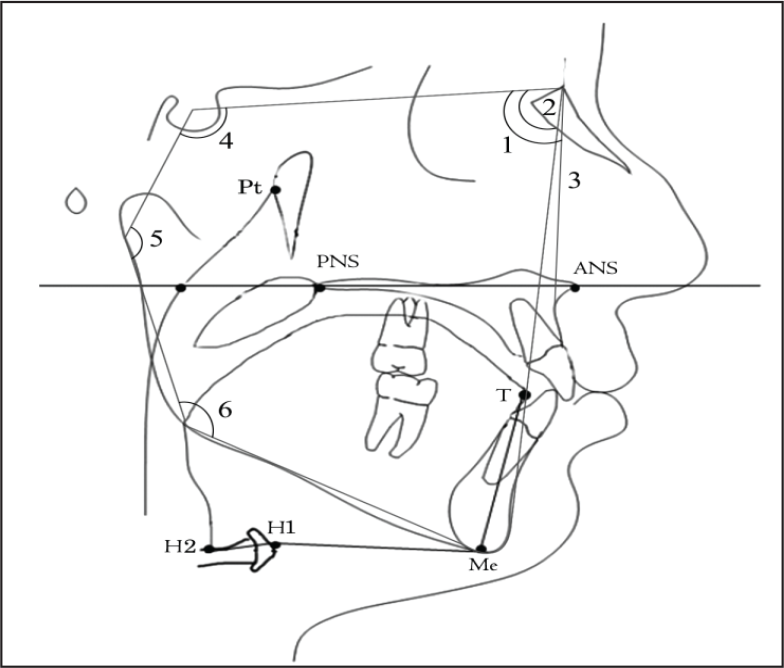
Various Cephalometric Landmarks and Linear and Angular Parameters for the Measurement of Pharyangeal Airway Space: Among Normodivergent and Hyperdivergent Growth Pattern. ANS (anterior nasal spine), Anterior Point of the Maxilla; PNS (posterior nasal spine), Posterior Point of the Palatine Bone; Me (Menton), the Inferior Point of the Symphysis; Pt (pterygoid point), the Posterior Point of the Pterygopalatine Fossa; T, the Most Anterior Point of the Outline of the Tongue; Palatal Plane, a Line Passing Through the ANS and PNS; H1, the Intersection Between the Posterior Border of the Tongue and the Hyoid Bone; H2, the Most Anterior Point of the Hyoid Bone; (1) SNA; (2) SNB; (3) ANB; (4) SN-Ar; (5)S-Ar-Go; and (6) Ar-Go/MP.
Linear Measurements (Figure 4)
Statistical Analysis
SPSS IBM Version 22 was used for data analysis with data represented in the form of mean and standard deviation. The difference between the means of variables between groups was tested by an unpaired t-test, with P value <.05 considered statistically significant. The correlation between the pharyngeal airway space and the other variables was analyzed using the Pearson correlation test.
Results
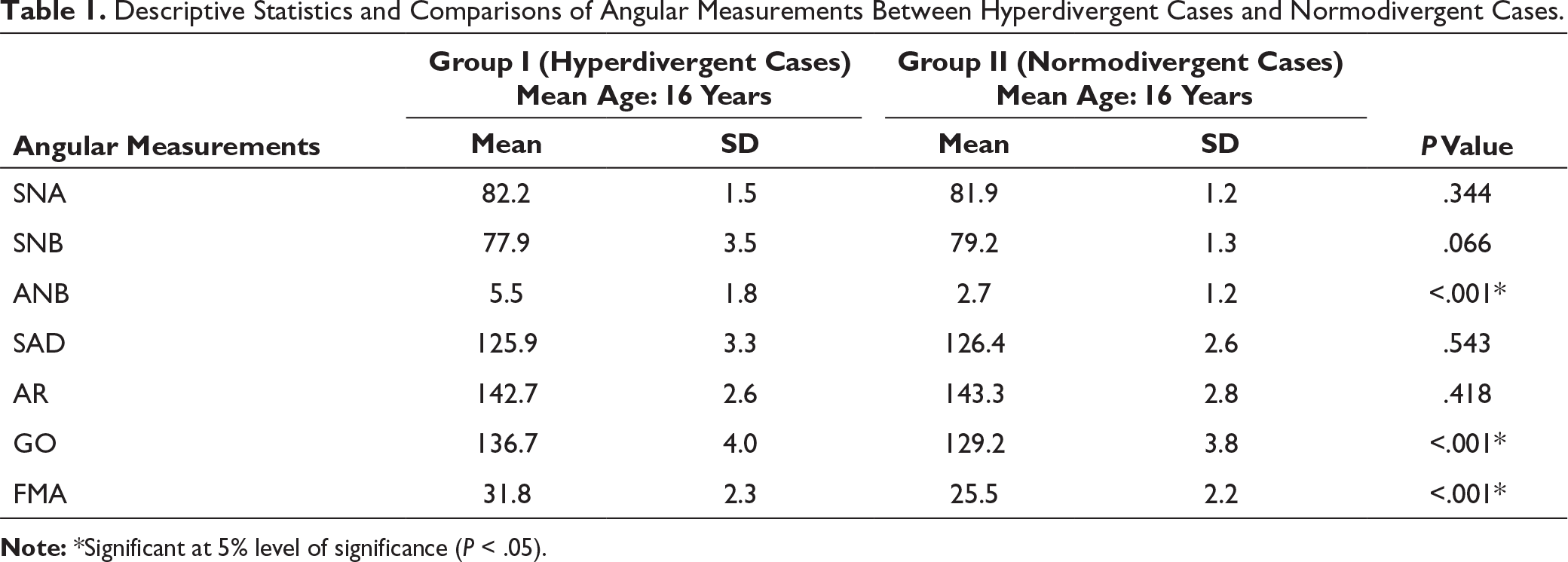
Descriptive Statistics and Comparisons of Angular Measurements Between Hyperdivergent Cases and Normodivergent Cases.
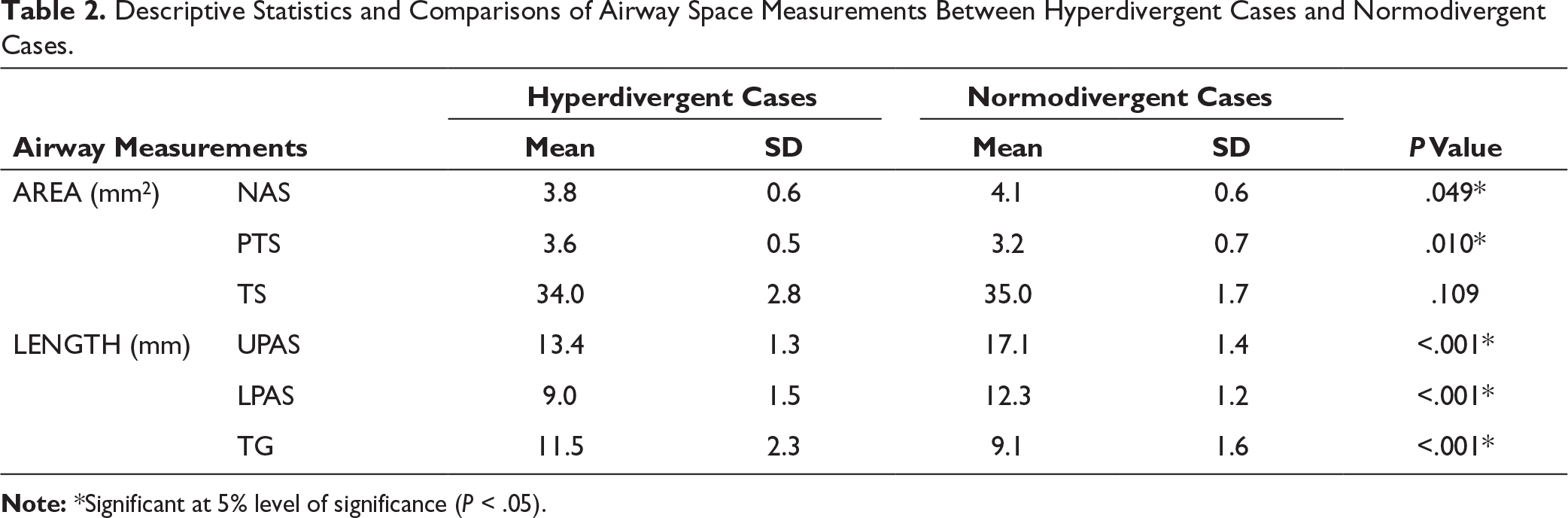
Descriptive Statistics and Comparisons of Airway Space Measurements Between Hyperdivergent Cases and Normodivergent Cases.
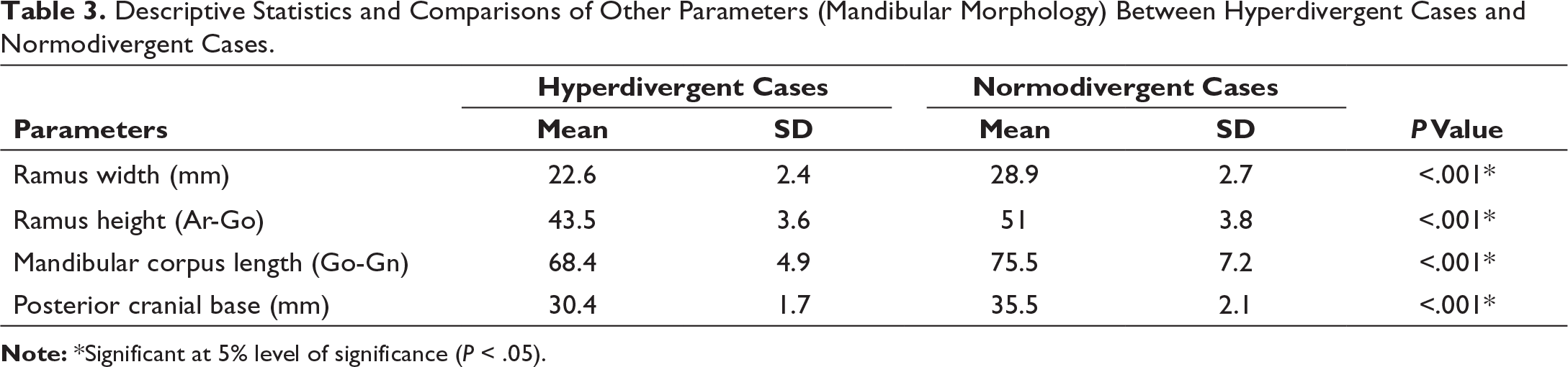
Descriptive Statistics and Comparisons of Other Parameters (Mandibular Morphology) Between Hyperdivergent Cases and Normodivergent Cases.
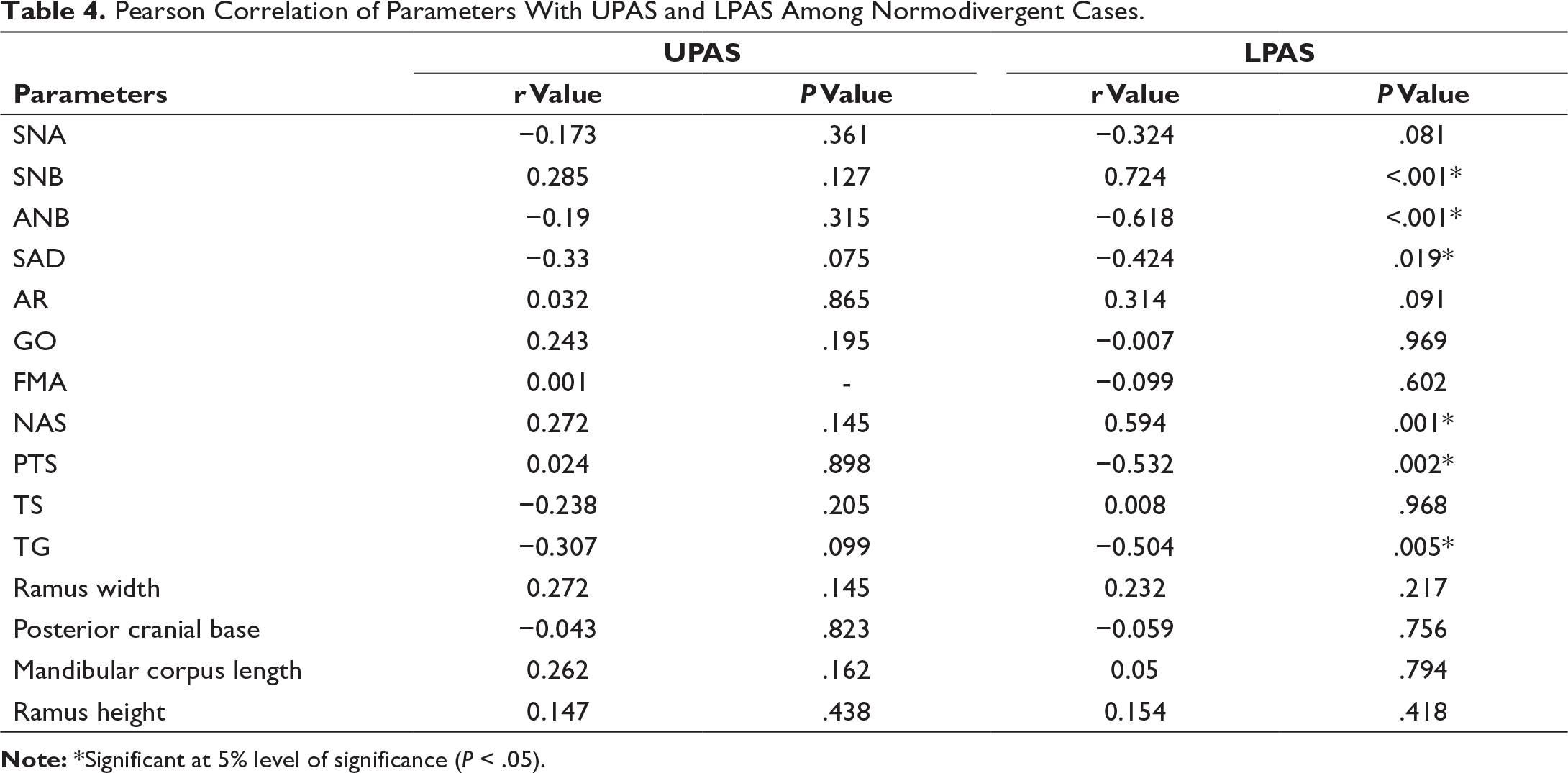
Pearson Correlation of Parameters With UPAS and LPAS Among Normodivergent Cases.
Pearson Correlation of Parameters With UPAS and LPAS Among Hyperdivergent Cases.
Discussion
The pharyngeal airway space allows to pass the inspired air from the nasal cavity to the glottis, and the expired air to pass from the glottis to the nasal cavity. 11 Assessment of the airway and its impact on craniofacial structures, and the inverse correlation among the 2 are one of the controversial and conflicting topics in the field of orthodontics.
According to Major et al, 15 the lateral cephalogram can be considered as a reliable initial screening tool for airway obstruction. Malkoc et al 9 stated that lateral cephalogram has a very high reproducibility for the assessment of airway dimensions, tongue position, and hyoid bone at natural head posture. 9 Naoumova and Lindman 16 concluded that manual tracing and digital tracing (FACAD) is comparable and reliable. 16
Analyzing the result of our study, it can be inferred that upper pharyngeal airway width had a significant impact on the craniofacial growth pattern, as stated in previous studies.17-19 However, few studies reported a weak correlation between pharyngeal airway, craniofacial morphology, and growth pattern. These studies were in discordance with the present study because they determined the influence of pharyngeal airway on facial form and occlusion. 20
Jean et al 21 concluded that rapid increase in nasopharyngeal airway area occurs till 13 years of age. Vilella et al, 22 in his study, reported that from 8 to 11 years, increase in bony nasopharyngeal depth occurs by 1.86 mm, whereas the thickness of adenoidal tissue increases by only 0.5 mm; also, nasopharygeal growth relates to downward displacement of hard palate, resulting in airway adequacy and even the thickness of the adenoidal tissue is increasing. The study by Fujioka et al 23 reported the largest adenoid/NP airway ratio at 4.5 years in absence or presence of snoring. Previous studies8, 24, 25 have assessed adenoids in children without respiratory symptoms and demonstrated a rapid growth of adenoids from 3 to 5 years of age. According to Linder-Aronson and Leighton, 25 adenoid tissues do not follow Scammon’s growth curve. Papaioannou et al 26 explained that at 8 year of age in majority of the children, the lymphoid tissue in the pharyngeal region restricts the lumen of airway to varying degrees. Thereafter, adenotonsillar overgrowth resolves in children without snoring. Because the subjects involved in the present study are in age range of 13 to 19 years, we can assume that the sagittal measurements were more stable.
From the cephalometric anatomy of the pharyngeal airway of this study, it was observed that there is a marked difference between hyperdivergent and normodivergent growth pattern. From this study, it was observed that the pharyngeal airway in hyperdivergent growth pattern was significantly narrower than the normodivergent growth pattern. Our finding was in agreement with the previous studies conducted by Joseph et al 27 and Ucar et al. 28 However, they concluded that this differentiation was attributed to the associated bimaxillary retrusion showed in the vertical growth pattern.
From the result of our study, it is evident that the ANB angle is larger in hyperdivergent subjects compared to normodivergent subjects and was statistically significant. Ceylan and Oktay 1 stated that the larger the ANB angle, the smaller will be the nasopharyngeal airway size. Akcam et al 29 estimated a reduction in upper airway dimension in individuals who had backward mandibular rotation which could lead to positioning the tongue more posteriorly and inferiorly. The present study showed statistically significant high mandibular plane angle, larger TG, larger PTS, and larger gonial angle in hyperdivergent subjects which was following Ucar et al. 28 According to Moss, 30 the gonial angle is influenced by the functional matrix of the muscle-like medial pterygoid and masseter. When the function of these muscles is altered, the morphology of the gonial angle is altered. 30
Dunn et al, 30 Ricketts et al, 31 and Linder-Aronson et al 32 reported that nasal obstruction results in mouth breathing habit that was associated with the nasopharyngeal width; the smaller or restricted the nasopharynx, the less adenoidal tissue enlargement was needed to obstruct the pharyngeal airway, thus explaining the prevalence of mouth breathing in individuals with hyperdivergent growth patterns.
When comparing craniofacial morphology among hyperdivergent and normodivergent, it is evident from our study that ramus width, ramus height, corpus length, and posterior cranial base length all variables were shorter in hyperdivergent subjects and were statistically significant.
According to Opdebeeck and Bell, in their study of long and short face subjects stated that short ramus in adenoid facies/long face syndrome was due to decreased cross-section of the hyoid bone and lower positioning of the pharynx closer to the cervical spine. 33
Buschang et al 34 stated that decreased force of masticatory muscle provided the excellent explanations for the predominance of hyperdivergent retrognathic phenotype and size of the masticatory muscle was directly related to ramus breath and bizygomatic width. This might be the reason for shorter ramus width in hyperdivergent individuals when compared to normodivergent individuals in our study.
According to the study of Damera et al, 35 the mean ramus width in males is about 31.0275 ± 3.54567; in females, it is 30.5625 ± 2.92309 mm in a normal individual, whereas our study showed the marked reduction of ramus width with a mean of 22.6 ± 2.4 mm in hyperdivergent individuals.
In this study, we correlated the relationship between the widths of ramus to pharyngeal airway space; according to counterpart principle, ramus width and middle cranial fossa (posterior cranial base) are the counterpart to each other which in turn was a counterpart to pharyngeal space. 6 Ramus width exhibited a highly significant positive correlation to upper nasopharyngeal airway, that is, as the ramus width decreases there is a reduction in upper pharyngeal airway in hyperdivergent subjects. From counterpart principle of Enlow, the skeletal function of the ramus width was to bridge the pharyngeal airway space and the middle cranial fossa so that the mandible can relate with the maxilla in correct anatomic position. If ramus width was too narrow, it positions the mandible too retrusive and vice versa to compensate for the morphogenic imbalance. 6
Mandibular corpus length is shorter in hyperdivergent subjects and it also showed a negative correlation with UPAS but it is not statistically significant. Our finding were not in agreement with Kim et al 36 which showed a significant association between mandibular corpus and total airway. Variation between studies may be attributed to difference in methodologies like different sampling methods and ethnic factors. Gonial angle and FMA also indicated a statistically significant inverse correlation to lower pharyngeal airway in hyperdivergent subjects. Low mandibular posture and tongue results in gonial angle area encroaching more on the muscles of the pharynx, this would add to the functional matrix of the gonial angle area resulting in constricted pharyngeal airway space. 30
Navarro et al 31 stated that backward rotation of the mandible occurs as a result of reduced muscle function, and provides the only supporting evidence for a direct association between masticatory muscle forces and mandibular posture. 37 A correlation between the normodivergent individuals and pharyngeal airway showed a highly significant and direct correlation with SNB, NAS, and LPAS. A significant inverse correlation was between ANB, Saddle angle, PTS, and TG. A study done by Solow et al 3 stated that inadequate pharyngeal airway space was related with an increased craniocervical angulation.
The study by El and Palomo 38 concluded that the mandibular posture with the base of the cranium contributes to the dimensions of the oropharynx. Head posture plays a major role in maintaining sufficient airway. The head posture differs variably depending on the severity of OSA. Korkmaz et al 39 in his study indicated no significant variation in craniocervical angulation/head posture between obese and nonobese individuals without OSA, which might probably influence the head posture, according to BMI. As the present cephalometric study excluded the patient of OSA, there is no significant effect of BMI on the pharyngeal airway.
The limiting factor of this study was that it was done with 2-dimensional cephalometric head films to estimate pharyngeal airway measurements; despite its limitation especially in the transverse plane, it can indicate the need for referral to an otolaryngologist for more comprehensive tests. Additionally, it would be interesting to consider respiration phase, head position, body types, and all 3 facial patterns with a CBCT volumetric calculation as evaluation of pharyngeal airway necessitates a more composite and dynamic 3-dimensional evaluation.9, 10 The factors put forward in this article highlighted the interrelated and compensatory morphological pattern of the pharynx, mandible, and tongue providing the clinical significance of their neuromuscular adaptation as data regarding this will expand our knowledge in diagnosis and treatment planning of orthodontics.
Conclusion
Following conclusions can be made from the present study:
Hyperdivergent subjects had reduced pharyngeal airway space when compared to normodivergent subjects. As there was a direct correlation among pharyngeal airway space, morphology of mandible and tongue was shown. Ramus width, Gonial angle, and FMA variations are inversely related to pharyngeal airway size in hyperdivegent subjects. Saddle angle, ANB angle, and tongue posture showed an inverse relationship with pharyngeal airway size in normodivergent subjects. Narrower airway space may be a causative factor for altered dentofacial skeletal patterns.
To provide stable orthodontic treatment outcomes, the orthodontist should have an excellent knowledge of pharyngeal airway morphologies during orthodontic diagnosis and treatment planning.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.