
Abstract
Abstract
Aim & Objectives: To evaluate using CBCT, the condylar changes taking place in retrognathic, hyperdivergent Class II adult patients following maxillary intrusion using miniscrew assembly. Materials and methods: In this prospective study design, 20 class II div I high angle cases in the age group of 20-25 years with Class II molar and canine relationship; Overjet > 5mm; ANB angle > 4°; FMA angle >25°; SNGoGn > 35°; Jaraback ratio< 60° and Lower Gonial angle>75° were taken. Each patient had a miniscrew assembly in the maxilla through which intrusive force was applied to the maxilla. Two additional miniscrews were placed between the first mandibular molars and second premolars to prevent extrusion of lower molars. CBCT images were taken at the beginning of the treatment (T1) and at the end of 6-9 months of molar intrusion (T2). Statistical analysis was carried out using student T- test. Results: Prior to treatment, the patients showed significant mandibular retrusion associated with increased maxillary posterior heights. Following maxillary intrusion with miniscrew assembly, CBCT evaluation revealed that the distance from the centre of condyle to the posterior border of the external auditory meatus was 19.2±1.67 mm on right side and 18.1±1.54mm on left side in T1 which increased to 19.6±1.45mm on right side and 18.5±1.36mm on left side in T2. The average forward displacement of condyle was .5mm which was statistically significant. The distance from the centre of condyle to superior border of external acoustic meatus was 3.1±1.7 mm on right side and 3.5 ±1.8 mm on left side in T 1 which increased to 3.8±1.9 mm on right side and 4.1 ±1.3mm on left side in T 2. The average downward displacement was .7mm which was statistically significant. Conclusion: Significant Maxillary intrusion can be achieved using miniscrews/ miniplate in adult hyperdivergent skeletal class II patients.
Introduction
Class II malocclusions are the most frequently encountered malocclusions in North Indian population. 1 Prior to the 1950s, retruded mandibles and convex profiles were highly accepted and appreciated but with increased awareness over a period of time worldwide, there is an increasing trend towards straighter profiles. This has led to an increase in class II patients seeking orthodontic treatment. 2
Convex profiles in class II patients with horizontal growth pattern are easier to treat as it involves correction of single jaw. But, class II malocclusions associated with vertical growth patterns are complex cases in which both the jaws are involved and the treatment plan should be directed toward correction of both the maxillary and mandibular jaw bases. 3
It is the increased posterior maxillary dimensions with subsequent backward rotation of mandible which worsens the profile in class II high-angle cases. Therefore, control of posterior maxillary heights is of utmost importance in treating such cases as mandibular advancement alone will not be sufficient to produce desirable changes in profile. As a result, it is important to control vertical growth of the maxilla and eruption of the upper and lower posterior teeth in the treating class II high-angle cases. A myriad of appliances are available to control maxillary growth such as headgear alone, functional appliances with headgear, posterior bite blocks, and vertical pull chin cups. 4
The effectiveness of these appliances is limited to growing patients only and results are highly unpredictable as they rely on patient’s compliance and growth.
For adult class II hyperdivergent patients, treatment options are limited. Not many patients opt for surgical approach as it involves increased morbidity, mortality, and increased cost. 5
With the advent of miniscrews, the envelope of discrepancy has expanded to include miniscrews for treatment of such severe cases which could earlier be treated by surgery alone. It is now possible to apply light continuous forces for molar intrusion using temporary anchorage devices (TADs) eliminating chances of root resorption and dependence on patient compliance. The study was designed to evaluate changes in the condylar position after intrusion using miniscrew implants. A forward rotation of mandible and condylar remodeling can be expected by intruding maxillary teeth and holding the mandibular molars.
Burke et al studies on condylar position and morphology in hyperdivergent patients have revealed more superiorly positioned condyle with reduced superior joint space. Maxillary intrusion in hyperdivergent cases is likely to cause mandibular autorotation and subsequent improvement in the condylar position. 6
For evaluation of bony and positional condylar changes in temporomandibular joints (TMJ), cone beam computed tomography (CBCT) is the best treatment modality which provides valuable information about glenoid fossa and its remodeling after maxillary intrusion.6-10
The objective of this study was to evaluate the positional condylar changes compared to its original position in class II hyperdivergent patients after maxillary intrusion with miniscrew assembly.
Material and Methods
In this prospective study design, to achieve statistically significant results, 20 subjects were chosen which would give 80% power to the study. The sample consisted of 40 CBCT scans taken before (T1) and at the end of 6 months of molar intrusion (T2) of 20 hyperdivergent patients, with equal number of 10 patients in each sex presenting with class II division 1 malocclusion, in the mean age group of 20 to 25 years reporting for orthodontic treatment. Ethical clearance was taken prior to conducting the study.
The parameters included in the study were:
Nonsyndromic with good oral health; Class II molar and canine relationship; Overjet > 5 mm; ANB angle > 4°; FMA angle >25°; SN to GoGn > 35° Jaraback ratio < 60° Lower Gonial angle > 75° Distinct step between anterior and posterior segments seen with increased distance between nasal floor and upper first molar (as determined by cephalometrics for orthognathic surgery [COGS]).
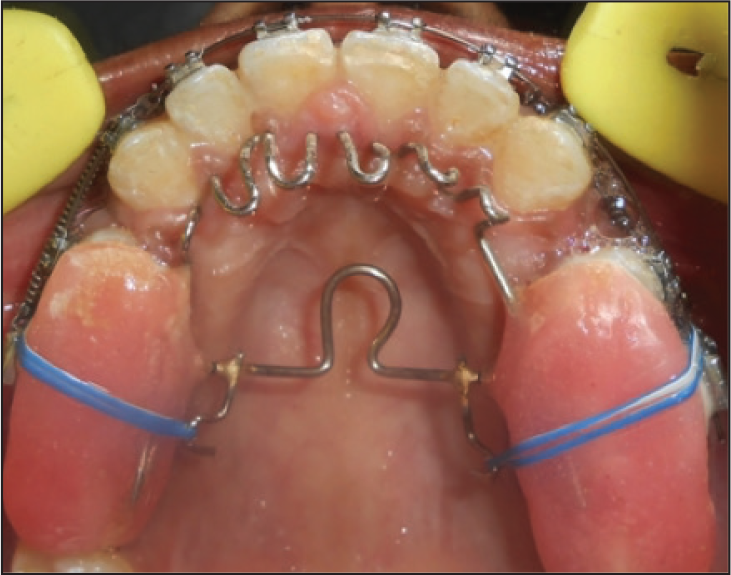
Face bow transfer was taken to rule out centric relation to centic occlusion (CR-CO) discrepancy prior to the initiation of treatment. The appliance used for skeletal anchorage was an assembly in the maxillary arch incorporating low transpalatal arch, posterior bite blocks, anterior tongue crib, and soldered hook through which force was applied to the miniscrews placed in the region of second premolar and first molar on the buccal side (Figure 9). TOMAS miniscrews with diameter of 1.6 mm and length of 8 mm were used in the study and force was calibrated to 150 Gms using dontrix gauge. A prefabricated jig was used for implant placement. TOMAS miniscrews were also placed in the lower arch in the same region. The patients were instructed to use chlorhexidine for rinsing before and few days after the procedure. The patients were anesthetized with local infiltration prior to the procedure.
The lower first molars were stabilized with these microscrews. Second molars in both the arches were included right from the beginning and all the third molars were extracted prior to molar intrusion. When we had achieved proper leveling of anterior and posterior occlusal planes, the amount of intrusion was determined cephalometrically by measuring the distance between the palatal plane and the upper first molar. The maxillary posterior teeth were then bracketed.
The assembly was taken off only after the active orthodontic phase was over.
CBCT scans Carestream CS9300 (Carestrean Health INC., Verona Street, Rochester, NY) machine was used to obtain CBCT scan in the present study according to the standard protocol (120 kvp; 4-5 mA; field of view, 13 × 17 mm; voxel, 0.3 mm; and scan time 25 seconds). The condylar changes were studied in the axial and sagittal section. The landmarks used in the study were: (a) the center of condyle; (b) line passing through the posterior border of external acoustic meatus perpendicular to true horizontal; (c) line passing through the superior border of external acoustic meatus perpendicular to the first line.
Center of condyle: From the axial view, largest lateromedial and anteroposterior dimensions of condyle were taken. Then, the center of the condyle was taken at the intersection of lines passing through these largest dimensions.
The distance from the center of the condyle to the superior border of external acoustic meatus was determined before (T1) and after treatment (T2) to evaluate the vertical displacement of the condyle on right and left side. Similarly, to evaluate sagittal displacement of the condyle, distance from the center of the condyle to posterior border of external acoustic meatus was determined before (T1) and after treatment (T2).
For accuracy of results, all measurements for this study were made by the same radiographer which were repeated twice with a span of 7 days between measurements.
Paired Student t test was used for statistical analysis of data. The effect size for the study is 0.8. No statistically significant difference was seen amongst different sexes.
Treatment Results and Discussion
Results
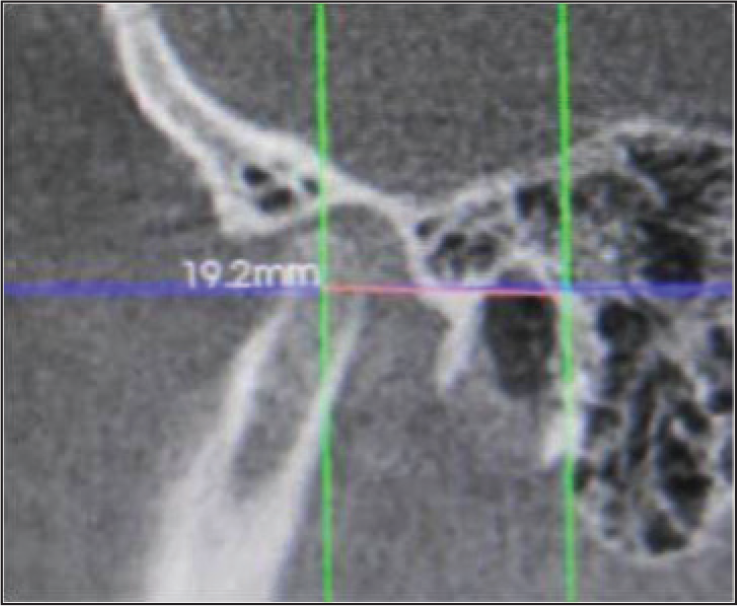
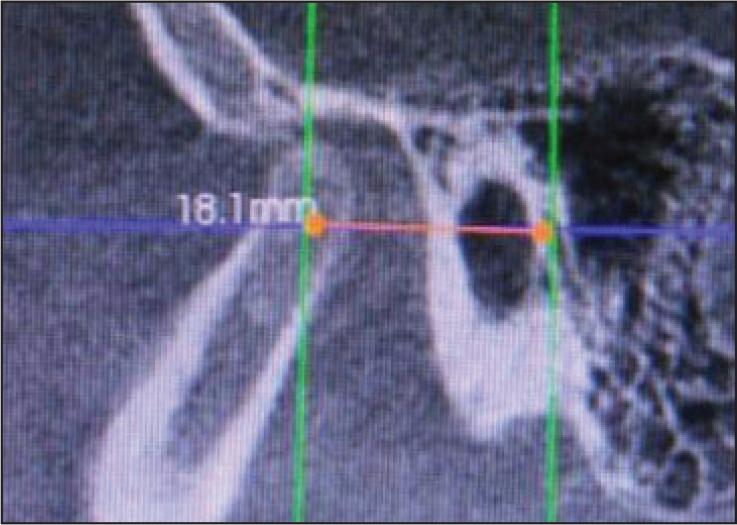
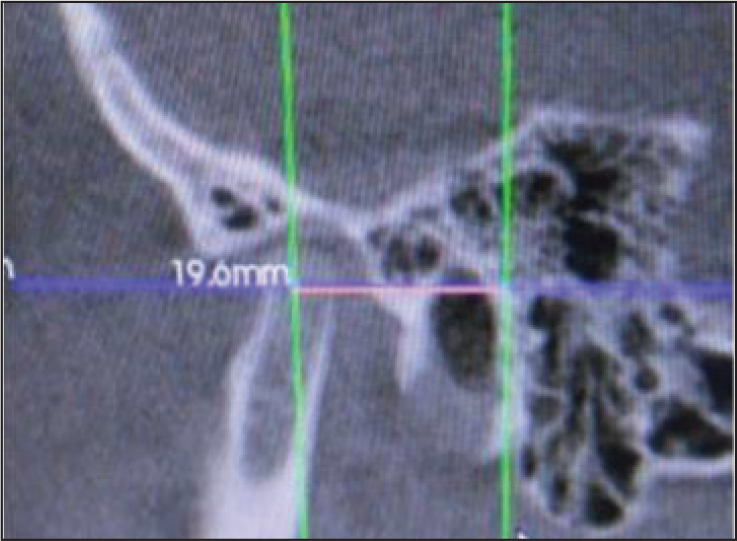
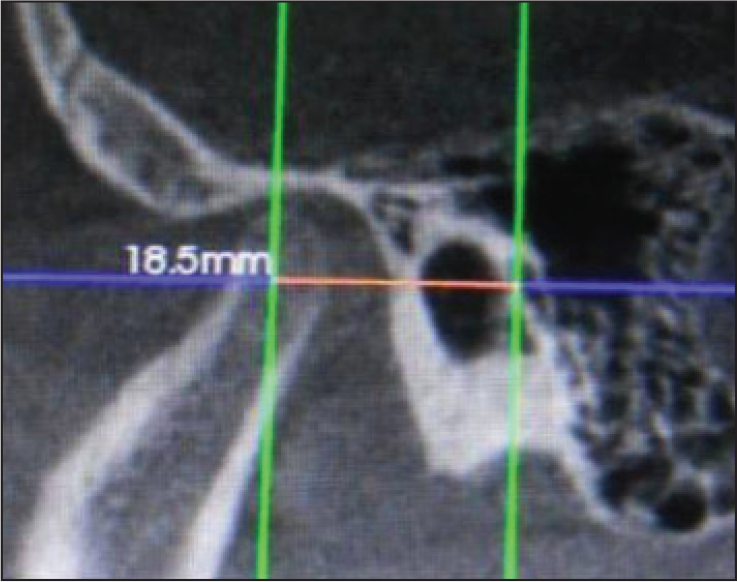
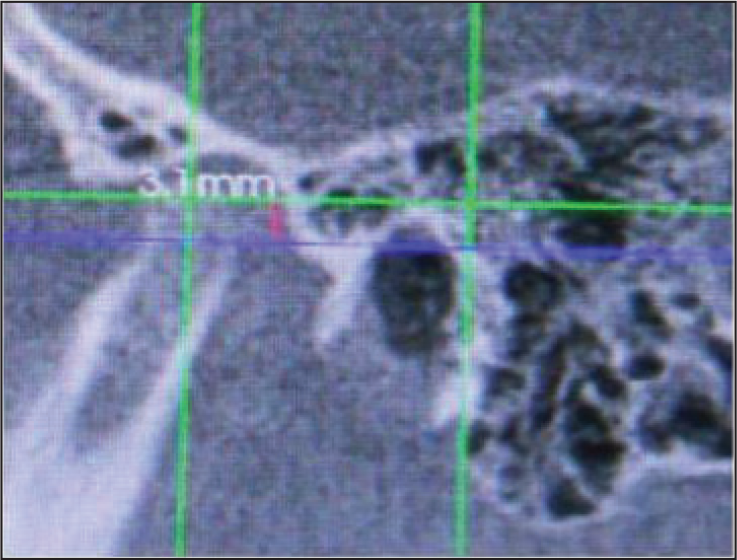
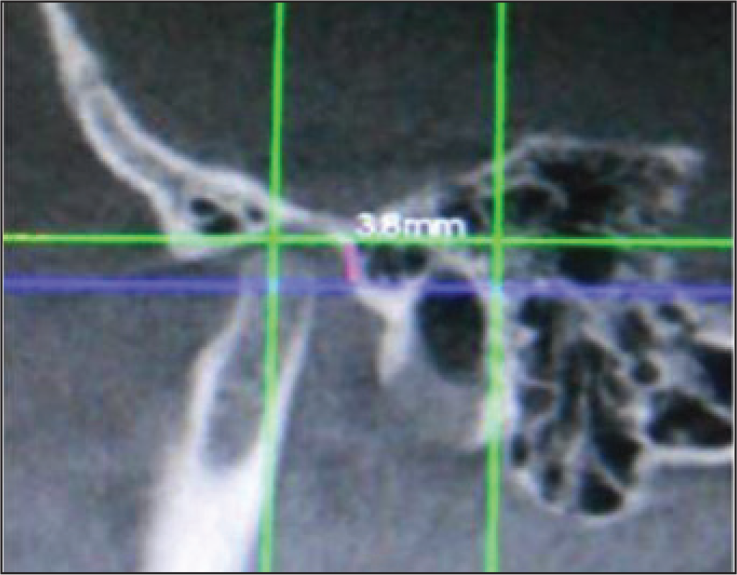
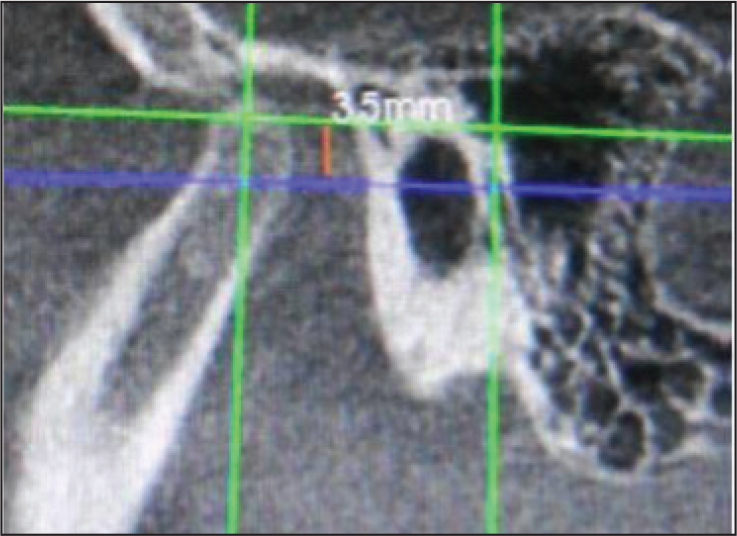
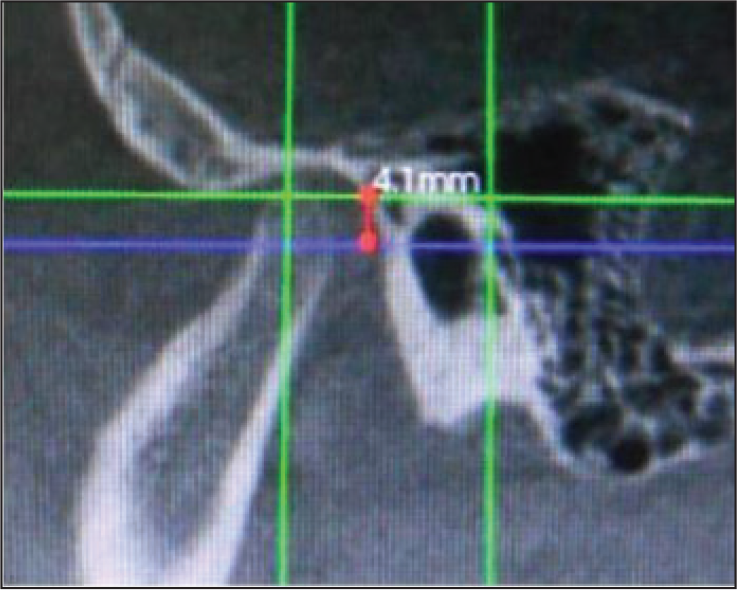
CBCT evaluation revealed that the distance from center of condyle to the posterior border of the external auditory meatus was 19.2 ± 1.67 mm (right side) and 18.1 ± 1.54 mm (left side) in T1 which increased to 19.6 ± 1.45 mm (right side) and 18.5 ± 1.36 mm (left side) in T2. Average forward displacement of condyle was .5 mm which was statistically significant. The distance from the center of condyle to superior border of external acoustic meatus was 3.1 ± 1.7 mm (right side) and 3.5 ± 1.8 mm (left side) in T1 which increased to 3.8 ± 1.9 mm (right side) and 4.1 ± 1.3 mm (left side) in T2. The average downward displacement was .7 mm which was statistically significant (Table 1, Figures 1-8).
Slight variation in the right and left side of condyle may be due to anatomical variation, positional error, or inter-examiner variability.
Discussion
For obtaining optimal functional esthetic balance and post treatment stability, it is extremely important to control the vertical facial dimensions during orthodontic treatment.11, 13
The literature is flooded with controversies in regard to different appliances being used for vertical control aiming towards correction of extrusion of maxillary molars, increased inclination of mandibular plane, and ante-inclination of maxillary plane.
The changes in mandible due to functional appliances have been extensively documented. In growing patients, with the help of orthopedic appliances, it is possible to bring about changes in mandibular position and condylar remodeling.11-13 But little is known about the mandibular response to maxillary intrusion and its consequent effects on the condyle in adults.
It is possible to orthodontically intrude the maxillary molars and correct class II high-angle cases presenting with or without open bite. 14 Superior positioning of maxilla in such cases may lead to autorotation of mandible which will help in correcting mandibular retognathism or retropositioning. It has been shown that mandible moves forwards and chin advances in 1:1 ratio following this autorotation. 15
Despite the small sample size, statistically significant results were obtained and the sagittal discrepancy was shown to be corrected which was consistent with the results of other authors.16-20 The positive treatment effects exhibited by majority of the subjects were primarily because of true intrusion of maxillary molars or due to holding of vertical dimension (relative intrusion).
A study conducted by Park et al 21 comparing condylar position in different vertical skeletal patterns suggested a posterior condylar positioning and reduced joint space in hyperdivergent patterns. A forward condylar positioning following maxillary intrusion as shown in our study may significantly improve the joint space and prevent temporomandibular disorders (TMD) problems in future.
A significant and higher condylar translation has been noted in hyperdivergent patients compared to the hypodivergent group in the studies conducted by Giradot Jr et al and Poluha et al.22, 23
CBCT Evaluation of Condylar Changes

Pre-treatment Right Side Horizontal
Pre-treatment Left Side Horizontal
Post-treatment Right Side Horizontal
Post-treatment Left Side Horizontal
. Pre-treatment Right Side Vertical
Post-treatment Right Side Vertical
Pre-treatment Left Side Vertical
Post-treatment Left Side Vertical
Miniscrew Assisted Intrusion Assembly
Conclusion
According to the methodology used and the results obtained, it was concluded that there was significant condylar changes in downward and forward direction indicating forward rotation of mandible following maxillary intrusion using miniscrews/miniplates in adult hyperdivergent skeletal class II patients.
The study shows significant downward and forward mandibular autorotation with miniscrews and thus can be considered a viable option in comparison to surgery in adult class II hyperdivergent patients. Though CBCT is an effective tool for 3D imaging of TMJ, the study is not without limitations such as the need of repeat CBCT after 6 months. The amount of autorotation was not calculated which can be done in a future follow-up study. The accuracy of the results can further be improved by a precise 3D head positioning device.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.