
Abstract
Background:
Contemporarily, the use of innovative orthodontic appliances or their components has increased for safer, quicker results, and more comfort of the patient. But, researchers rarely highlight the potential demerits of accidental ingestion of these appliances. Thus, the present study aimed to investigate the evidence-based literature on the accidental swallowing of these appliances and their effect on the gastrointestinal tract (GIT) and airway.
Method:
An electronic search was performed on PubMed, Medline, Scopus, The Cochrane Library, and EMBASE until April 11, 2021. Methodological quality and synthesis of case series and case report tool (MQCC) was applied to determine the quality of these case reports and series. The outcome variable was to assess its effect on airway and GIT, and methods of removal of these foreign bodies. Meta-analysis was not performed as the study included case reports and case series in which no control groups were present.
Results:
Out of 113 case reports and series, 29 articles were included in this systematic review. Only 31% of articles have satisfied the MQCC scale and maintained as high-quality case reports, 43% of articles were medium to high quality, and 26% designated as low quality.
Conclusions:
Eighty percent of the accidental ingested orthodontic appliances that pass uneventfully through the gastrointestinal system require a fiber-rich diet and laxatives. A total of 10% to 20% lacerates oral, pharyngeal, and gastrointestinal mucosa result in pain, bleeding requires laryngoscope, endoscopically and laparoscopy with use of Magill’s forceps. Only 1% of cases have presented with a high morbidity and mortality alarming for surgical removal of ingested component. Thus, the precautions to be taken to overcome such incidences are tying silk thread to activation key, use of recent bonding method, use of contrast colors of removable appliances as the color merges with mucosal color, and operator position should be 7 O′ clock.
Introduction
Accidental ingestion of foreign body is more often seen in children and around 1,500 people die each year due to this. 1 Incidence of foreign body aspiration occurs in children (80%), elderly, mentally impaired, or alcoholic individuals and sometimes it may occur deliberately in prisoners or psychiatric patients.2-4
Commonly aspirated foreign objects are coins, meat boli, and button batteries; sewing needles, tooth picks, straightened paper clips, and razor blades; and dental objects. In most of the situations, these objects pass through the gastrointestinal tract (GIT) uneventfully, but 10% to 20% required endoscopic removal and 1% alarm for surgical removal.4-6
Kurkciyan et al (1996) 7 , Pavlidis et al (2008) 8 , and Dhandapani et al (2009) 9 have reported that the accidental swallowing of dental materials and other armamentarium or materials their product used in various dental procedures.7-9,10-14 The most often accidentally swallowed dental objects are the broken fragments of burs, posts, root pieces, teeth, impression materials, implant components, and restorations. Overall incidence of dental foreign body aspiration is 3.6% to 227.7% and higher in adult than in children.15-19 In prosthodontics, single crowns and loose dentures are more prone to swallowing in endodontics broaches and files, and also fragments of implants and other dental restorative materials are frequently swallowed.
Rohida and Bhad et al, Umesan et al, and Naragond et al have reported that during routine orthodontic treatment, chance of accidental aspiration of various orthodontic materials like bracket, wire fragment, activation key and fractured twin block, removable retention appliances and lingual retainers. However, these incidents are being managed successfully without medical emergency.18-23
The major manufacturing limitations of dental and orthodontic materials are their shape and size, smaller and made up of radiolucent materials, which make them easy to swallow and difficult to detect with radiographs. Hence, it alarms to use bronchoscopy/endoscopy or computed tomography for its localization.1-17,23,25-27 Although only 2% to 3.7% require emergency treatment as these foreign bodies obstruct GIT or respiratory tract, and the rest of the material pass GIT without complications. 28
This systematic review aimed to investigate the most frequent ingesting of the foreign body during orthodontic treatment, associated complications, and management from available evidence like case reports and case series.
The objective of this systematic review is to collect, compile, and review the data available on accidental ingestion of orthodontic materials during treatment from various published case reports and case series.
Focused question: What are the effects of accidentally swallowing an orthodontic appliance or part of a fixed orthodontic appliance to the airway and gastrointestinal tract?
Materials and Methods
This systematic review was conducted in agreement with the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The study has not been registered.
Eligibility Criteria
The inclusion and exclusion criteria were established according to the (population, intervention, control, and outcomes) PICO question reported above.
The included studies were case series and case reports published in English and regarding the accidental swallowing of orthodontic materials, associated complications, and their management. Also searched articles published in medical journals entitling on accidental swallow of dental or orthodontic materials.
Exclusion criteria: case reports, case series, and studies with orthodontic treatment in autism, Pica syndrome, geophagia, and subject with mouthing habit.
Information Sources
An electronic investigation was performed using PubMed, Medline, Scopus, PsycINFO, SciSearch, The Cochrane Library, EMBASE, HINARI, and EBSCO. The search was conducted until April 11, 2021. No restrictions were applied in time or language.
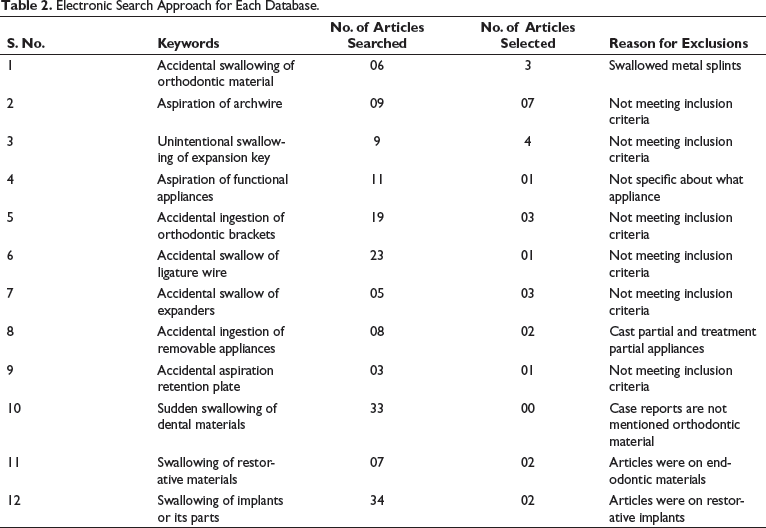
Search Strategy
Primary and Secondary Keywords.
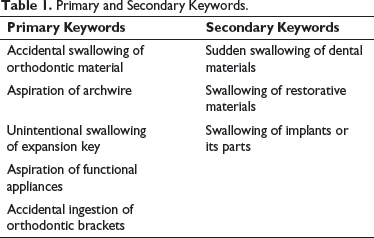
Electronic Search Approach for Each Database.
Study Selection
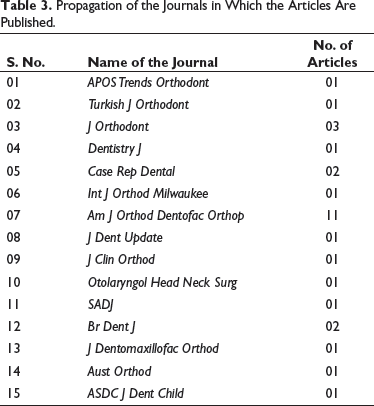
Propagation of the Journals in Which the Articles Are Published.
Data Collection Process
Evidence obtained from the selected articles were retrieved and exported to Excel sheet (Microsoft window 2010) organized according to methodological quality and synthesis of case series and case reports tool (MQCC) under following 4 domains:
Subjects Ascertainment Causality Reporting
Quality Assessment
Independent quality assessment of selected case reports and case series were conducted according to checklist provided by MQCC 28 under 4 domains by 2 reviewers (SS and SR). Any disagreement between the 2 authors was discussed and resolved by consensus or arbitration by the third reviewer (RR).
In this review, methodological quality and MQCC of Murad et al 28 was the modified tool of Bradford Hills and Newcastle Ottawa scale. In this Newcastle Ottawa scale’s, 8 items have converted into 4 domains: selection, ascertainment, causality, and reporting. Thus, the quality assessment of the case reports and series were evaluated assigning “stars” (Newcastle Ottawa scale). One “star” for an incomplete detail, two “star” for an acceptable, and three “star” for complete and alternate ways of accidental swallow.
Result
Selection of Case Reports and Case Series
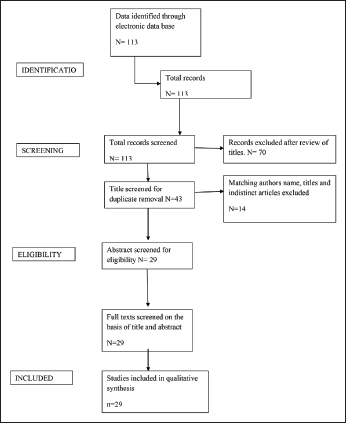
The electronic search conducted to identify case reports and case series depends on the title admissible in the systematic review. However, a sum of 113 case reports and case series retrieved from various dental and orthodontic, and medical emergency journals. A thorough screening was performed and 70 nonorthodontic dental case reports were removed; 43 case reports were being shortlisted to determine their compliance with the eligibility, and 14 case reports were excluded. Finally, 29 articles fulfilled the selection criteria and were included for qualitative analysis of the systematic review.
This comprised 58.7% of the total articles retrieved from the data search. The present study was conducted and reported following the PRISMA, the outline of which is illustrated in Figure 1.
PRISMA flow chart
Characteristics of Included Studies
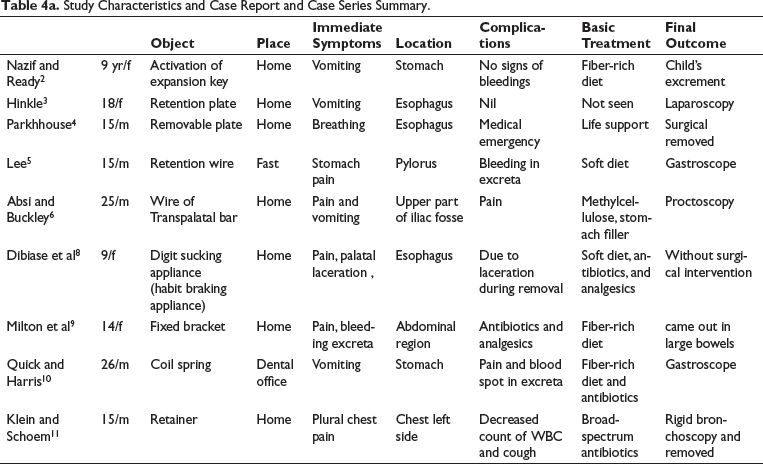
Study Characteristics and Case Report and Case Series Summary.
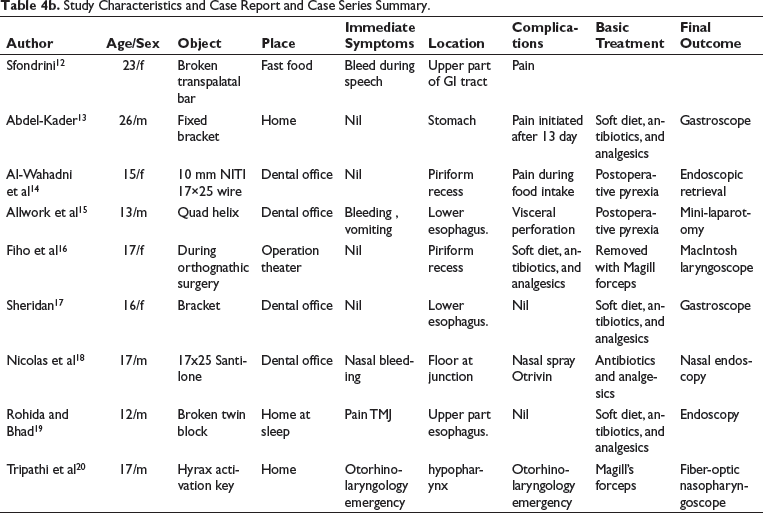
Study Characteristics and Case Report and Case Series Summary.
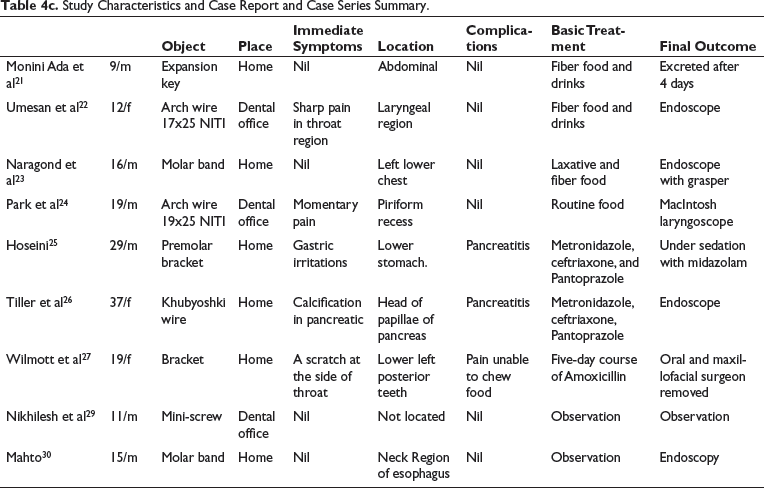
Study Characteristics and Case Report and Case Series Summary.
Quality Assessment
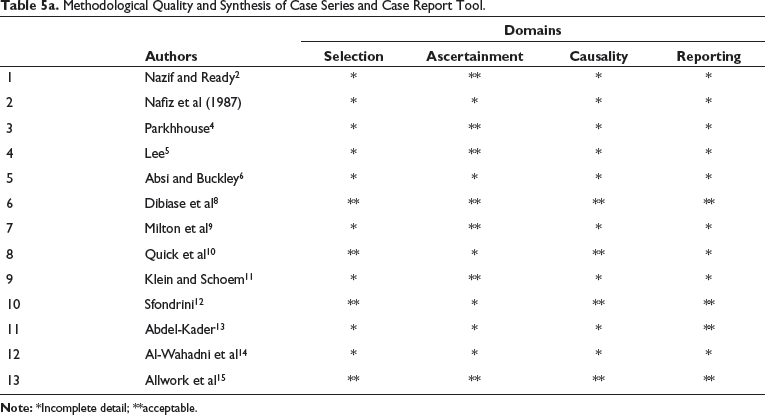
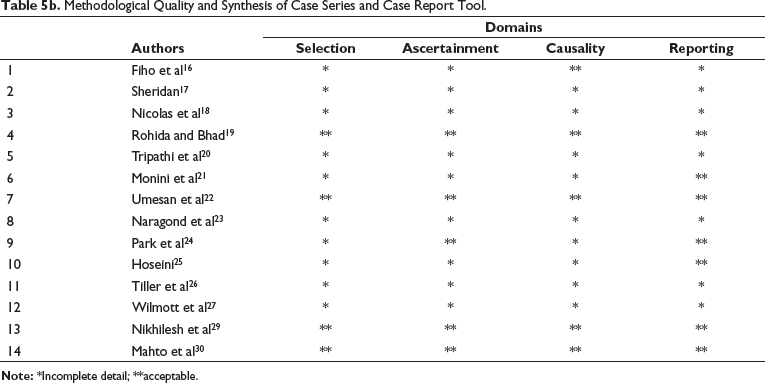
Methodological Quality and Synthesis of Case Series and Case Report Tool.
Methodological Quality and Synthesis of Case Series and Case Report Tool.
Risk of Bias Assessment
Methodological quality and synthesis of MQCC scale was applied to determine the quality of these case reports and series and is illustrated in Tables 5a and 5b.
Nineteen out of 29 were case reports and 10 case series, in which 74% of case reports have satisfactorily addressed the method of MQCC and its applicability to be the general population.
Synthesis of Results
Twenty-nine articles have published the unexpected swallow of orthodontic materials (archwire, segment of archwire, removable appliance, retainer, expanders, expansion key, and mini-screw). Nine out of 29 articles have been notified on incidental assimilate of the archwire, segment of archwire, and ligature wires; and 7 on expanders, and expansion key’s rest of the articles documented twin block, mini-screw, and removable appliances.
Discussion
Synthesis of Evidence
Case reports and case series are communicative studies that are prearranged for demonstrating novel, unusual, or atypical features recognized in subjects of medical, dental, and orthodontic practice, and they hypothetically create new research questions.26, 27 Most of the case reports and case series define and scrutinize the diagnosis and management of 1 or more than 3 patients; also from the base of the evidence-based pyramid. 28
Accidental Swallow of Expansion Key
Nafiz and Ready MA in 1983 have published two case reports on accidental aspiration of expansion key. This incident took place in the dental office while the operating subject turned head and slipped from the operator’s hand; as the patient’s position was the supine key was swallowed a fiber-rich diet was advised and after 4th week seen in excreta. 2
Tripathi et al 19 published a similar case report of the 17-year-old male (cleft lip and palate) patient; the incident occurred in a dental office as the patient turned up his head and the expansion key slipped from the operator’s hand. 19 This case was managed as a medical emergency, and the key was removed using “Magril force” with fiber-optic nasopharyngoscope. An exact case report was published by Monini Ada et al. 20
Archwire and Archwire Segments
Absi and Buckley 6 reported that a 25-year-old female had an accidental swallow of transpalatal bar made up of crescent-shaped piece of rigid stainless steel wire of 0.9 mm diameter and approximately 2.5 cm length, with a U-loop at both the ends. An abdominal radiograph located that wire was in the upper-right iliac fossa. She was given methylcellulose as bulk filler, and then it was located passing from small bowel to a large intestine, then the patient was discharged. Later, the patient complained of abdominal pain, now the wire was located at rectal region and removed with proctoscopy. Nicolas et al 17 published a case report of a 17-year-old male who came with the chief complaints of nasal bleeding and pain; nasal endoscopy was used to remove the wire fragment. Umesan et al 21 reported a 12-year-old girl’s case report of accidental ingestion of archwire (17X25 NITI) segment of 20-mm length in dental office during the routine visit. This incident occurred while cutting a posterior excess archwire with distal end cutter; wire was located at laryngeal region and was successfully removed using endoscopy.
Fixed Orthodontic Bracket
Milton et al 9 published a case report of a 19-year-old woman who visited with pain, cough, and scratchy throat. On clinical examination, premolar bracket was missing, and on the X-ray of the chest and stomach, location of an ingested foreign body was unidentified. The patient was encouraged with fiber food, more drinks, and amoxicillin tablets. Later, an orthopantomograph revealed that dislodge premolar bracket seen in a posterior second molar area was removed. Fiho et al 15 and Sheridan 16 reported that a 17-year-old girl, 32-year-old boy, and 29-year-old women respectively were the orthognathic patients post-surgery that found the missing second molar tube and brackets.
On X-ray, missing appliances were located at the piriform recess of the larynx, with the help of Macintosh laryngoscope, and removed using Magill forceps.
Removable Appliance, Retainer, and Twin Block
Park et al 23 published a case report of a 15-year-old boy who was given a tongue crib and was accidentally ingested during fast food eating. He later complained of stomach pain and bleeding spots in stools, and it was located at the pylorus region; managed with gastroscopy. Dibiase et al 8 reported an 18-year-old male with an accidental swallow of the removable plate. The immediate complaint was difficulty in breathing, and the appliance was at the esophagus region. This case was alarmed for a medical emergency and surgical removal. Rohida and Bhad 18 circulated a case report of 12-year-old male with accidental swallow of fracture twin block. The author reveals that the patient was using repaired piece of broken twin block, located at the esophagus and removed using endoscopy.
Orthodontic Band Material and Molar Bands
Naragond et al 22 reported through a case report of a 16-year-old male who accidentally engulfed a molar band during eating fast food. It was located at the lower-left region of the chest. No immediate or delayed symptoms were found and by using endoscopy with grasper, the foreign body was removed. Mahto et al 29 reported a similar incident that occurred in a 16-year-old cleft lip boy and was removed using endoscopy with a grasper.
Mini-Screw
Nikhilesh et al 30 published a case report of 11-year-old male patient who was getting treated with mini-screw-supported distalizing appliance. During the routine visit, one of the mini-screws was loose, and the operator wanted it to remove and reposition it. While removing, a patient turned his head, gave a push, and a mini-screw fell in the pharyngeal region. However, it was not located in the X-ray. The author concluded that the mini-screw might have expelled.
Management Protocol
The development of signs and symptoms depends upon the age of the subject (child or an adult), 75% of the case reports have revealed that the foreign body gets entrapped at the upper esophageal sphincter, and 30% at a lower level.1-5 The accidental ingested foreign body follows 4 levels with the specific sign and symptoms at each level such as, at oropharyngeal level drooling of saliva, inability to swallow; at an esophageal level in adults complaining of discomfort at the center of the chest or epigastric region, dysphagia and children clinically presents retching, neck, or throat pain, gagging, vomiting later may develop fever, recurrent aspiration pneumonitis/pneumonia.10,16,18,22,27,30 Similarly, if the foreign body entrapped at a suboesophageal level can present passing rectal blood and melena and few cases develop subacute intestinal obstruction, and if the appliance is sharp trapped in a GIT may present gastrointestinal perforation signs and symptoms as acute mediastinitis, chest pain, dyspnea, and signs of pneumonitis/pleural effusion.11, 12, 13, 25 In this situation, the patient should be calmed and careful examination should be performed; the location of foreign objects at each level is mandatory. Thus, abdominal and chest X-rays, endoscopy, and computed tomography scans of the thorax and abdomen are advised.12,14,16,20,21,26,29-31
Act quickly, keep the patient’s head low, and instruct to cough or if a foreign body is visible, remove it with small forceps or use the Heimlich maneuver method. Based on the location of the ingested foreign body-appropriate devices such as MacIntosh laryngoscope with Magill forceps, fiber-optic nasopharyngoscope is used to remove it.1,3,5,7,21,30
Wasundhara Bhad et al advised that the use of removable appliances should have contrast color of gastrointestinal (GI) tract that helps in locating the swallowed part of functional appliance. 18
Recommendations
Most of the accidental aspirated orthodontic foreign particles entering the oropharynx will pass through the alimentary canal uneventfully. Only 1% of the large and sharp object causes complication as they have impact in GI tract.1-6,9,10,17,20,22,27,30
Orthodontic wire segment, if impact at the level of 4th cervical vertebra and laryngeal impaction present with dysphagia and odynophagia can be managed with endoscopic retrieval. The use of a distal end cutter avoids the accidental swallow.3,10,17,21,25
Removable orthodontic appliance accidentally ingested and is located at esophageal area may present chest pain, drooling of saliva, and vomiting and if the appliance fragment lodged at ileocecal junction or at the sigmoid colon area, it presents with muscle incoordination, incessant twitching, and hematemesis causes.3,10,17,21,25,26,30 Later, patient presents with abdominal pain, fever, nausea, vomiting, and abdominal distension because of perforation of the ileocecal junction and the sigmoid colon. The use of Fiber-optic nasopharyngoscope to locate and remove the aspirated fragment or appliance.12,16,19,22 Use silk thread and tie a knot to labial bow or Adam’s clasp for immediate retrieval from the esophagus; use a contrast-colored appliance to identify at the time of removal.9,24,11,23,29-31
Strength of the Study
In the era of clinical trial and evidence-based practice, this systematic review withstands to describe hidden or undetected scientific observations for clinical trials. This also generates a hypothesis that provides an evidence-based orthodontic practice. This systematic review enlightens patient-centered clinical awareness of an individualized nature of contemporary patient care and can be used for teaching, review, and research purposes.
Weakness of the Study
This systematic review comprised of scanty evidence, deceptive, and no control group to compare outcomes, and has no statistical validity.
Conclusion
We conducted this systematic review to answer the question: “What are the effects of accidentally swallowing an orthodontic appliance or part of a fixed orthodontic appliance to the airway and gastrointestinal tract?”
Based on the meticulous search, 29 case reports and case series have published the accidental swallow of different orthodontic materials. To answer the research question, we have clubbed the case report and series reporting similar items of accidental swallow, and we have got the following conclusions.
Nine individual case reports were on accidental swallowing of wire segments in resident and subjects reported with abdominal pain; nasal bleeding and airway compromised. Seven case reports were reported on expanders and expansion keys, and patients reported with discomfort, drooling of saliva, and inability to swallow. One article reported a functional appliance swallow with a chief complaint of breathless with a severe cough. Most of the case reports could not satisfy the methodological evaluating domains. Clinician must warn the subject and parents before beginning with any orthodontic treatment. Activation key tied to silk thread and 7 O′ clock position of the operator can prevent its accidental ingestion
Footnotes
Acknowledgments
The authors would like to thank Dr. Wasundara Bhad and Dr Santosh Chavan for their moral support to complete this study.
Author Contributions
Dr Siddharth Sonwane: writing, design, compile, data collection, and analysis; Dr.Shweta.Kamble (sonwane): concept, supervision, and grammar.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.