
Abstract
Objective:
The objective of this study was to evaluate the effects of the four first premolars extraction compared with a non-extraction treated control group on the lower anterior facial height.
Methods:
Electronic search was conducted on PubMed, Cochrane, Scopus, Lilacs, Scielo, clinical trials, and opengrey.eu databases; only article published in English were included. The eligibility criteria were extraction of four first premolars compared with a non-extraction control group treated with fixed mechanotherapy. Anterior Nasal Spine to Menton (ANS-Me) (mm) was taken as the primary outcome; Frankfurt mandibular plane angle (FMA) and Nasion to Menton (N-Me) were selected as secondary outcomes. Non-randomized Studies-of Intervention (ROBINS-I) tool was used for the quality assessment and risk of bias. Heterogeneity was analyzed using statistical tests, including chi-squared-based Q-statistic, tau-square, and I-squared statistics. Review Manager was used for quantitative assessment and meta-analysis.
Results:
Five retrospective studies were included for quantitative assessment and three were included in the meta-analysis due to certain missing data. Extraction of four first premolars did not affect both primary and secondary outcomes with P = .65, P = .93, and P = .91, respectively, for ANS-Me, FMA, and N-Me.
Conclusion:
This review and meta-analysis concluded that there was no statistically significant effect of extraction of four first premolars on lower anterior facial height.
Keywords
Introduction
To establish good facial esthetics during orthodontic treatment, facial balance plays a key role and is commonly defined by anterior and posterior facial height. Usually, anterior facial height is less developed than posterior facial height in a normal growth pattern.1, 2
These dimensions establish the changes in mandibular rotation. Although, it remains a controversial topic among well-known orthodontics authors; whether to extract a tooth or not, especially in the border-line cases.
Extractions are usually recommended in a patient with crowding, increased facial height, steep mandibular plane, and minor dentoskeletal disharmony. To simply understand this concept, assume that our dentoskeletal component and posterior teeth are present in a form of an occlusal wedge, and when these teeth move in the anterior direction or in the posterior direction, it will close the bite or open the bite, accordingly.3-5 Thus, it is a belief that extraction of posterior teeth provides upward and forward movement of molars, and mandible rotates counterclockwise and aids in reducing lower anterior facial height as well as close the bite of the patients.3, 6-9 However, this concept is not relatable with skeletal anchorage (temporary anchorage device (TAD)-assisted retraction), as molars remain in their position. Some published studies have demonstrated that extraction of premolars may not reduce lower anterior facial height,10-12 but it may further increase it.13-15 However, some studies also concluded that the extraction of tooth does not improve facial height.9, 16, 17
Therefore, it is necessary to conduct a highly specific systematic review and meta-analysis to evaluate these changes. Thus, this study aimed to evaluate the effects of the four first premolars extraction when compared with a non-extraction treated control group on the lower anterior facial height.
Material and Methods
Registration and Protocol
This systematic review and meta-analysis is conducted according to the Cochrane Handbook of Systematic Review 18 and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. 19 Registration of this review was carried out under The International Prospective Register of Systematic Reviews (PROSPERO) with a registration number CRD42020202472.
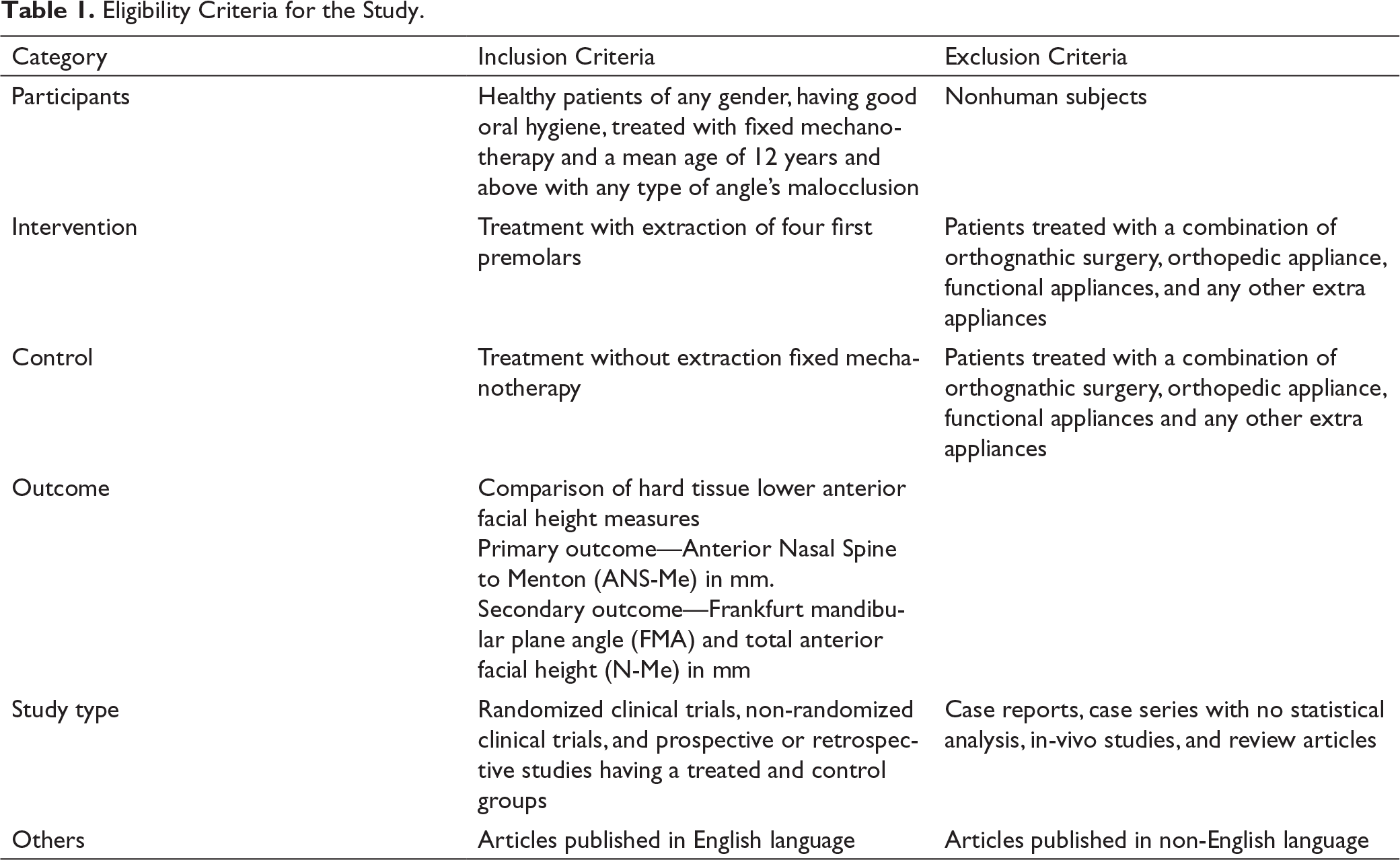
Eligibility Criteria
Eligibility Criteria for the Study.
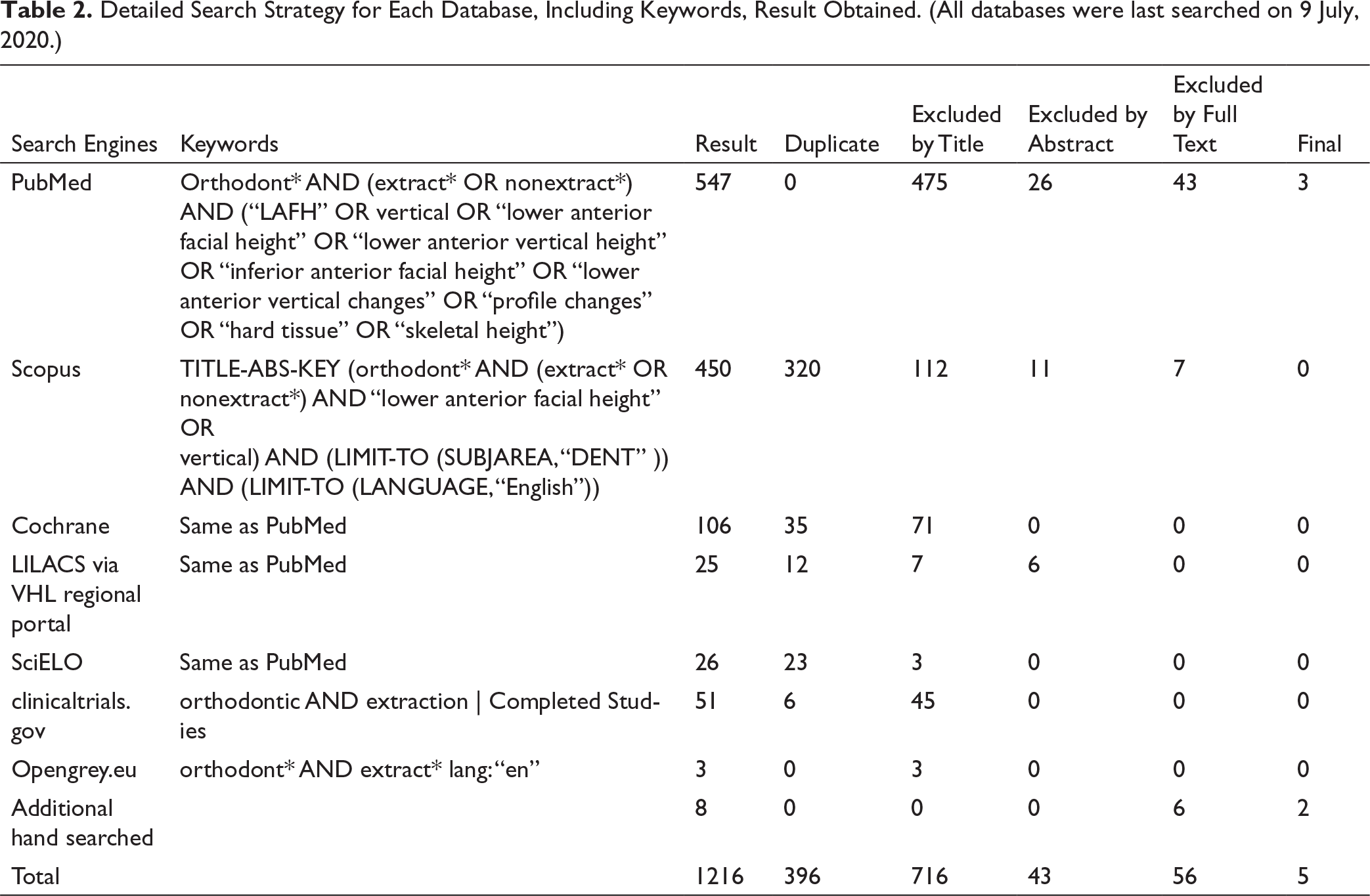
Information Sources and Search Strategy
Electronic database search was last conducted on July 9, 2020 with no limitation of publication year. Following databases were searched: PubMed, Scopus, Cochrane (CENTRAL), Latin American and Caribbean health sciences (lilacs) via Virtual Health Library (VHL) regional portal, and Scientific Electronic Library Online (sciELO); Additional search for unpublished studies was conducted electronically through OpenGrey (opengrey.eu), and Clinical Trials (clinicaltrials.gov) databases. We also performed hand screening of the references of relevant articles for additional studies.
Detailed Search Strategy for Each Database, Including Keywords, Result Obtained. (All databases were last searched on 9 July, 2020.)
Study Selection and Data Collection
The recognized studies from the databases’ search were sequentially assessed in two stages. The title and abstract of studies were screened in the first stage, followed by the second stage in which the full-text assessment was carried out for final selection and suitability. This process was performed independently by one author (ADJ) and, in duplicate, checked against the criteria by another author (SK). Any conflicts were resolved by detailed discussion and agreement of a third author (SM). These authors were not blinded.
Data collection was performed using the same protocol and authors on a customized data extraction sheet. The extraction sheet included the names of authors, publication year, study design, details of each extraction group and non-extraction group (the type of malocclusion, number of participants, mean age, gender, intervention, and duration of treatment), assessment method, outcome, and magnification control. Numerical data of included studies were also collected using a customized sheet for both primary and secondary outcomes, separately. Secondary data were obtained only from included studies for the primary outcome.
Risk of Bias in Each Study and Quality Measurement
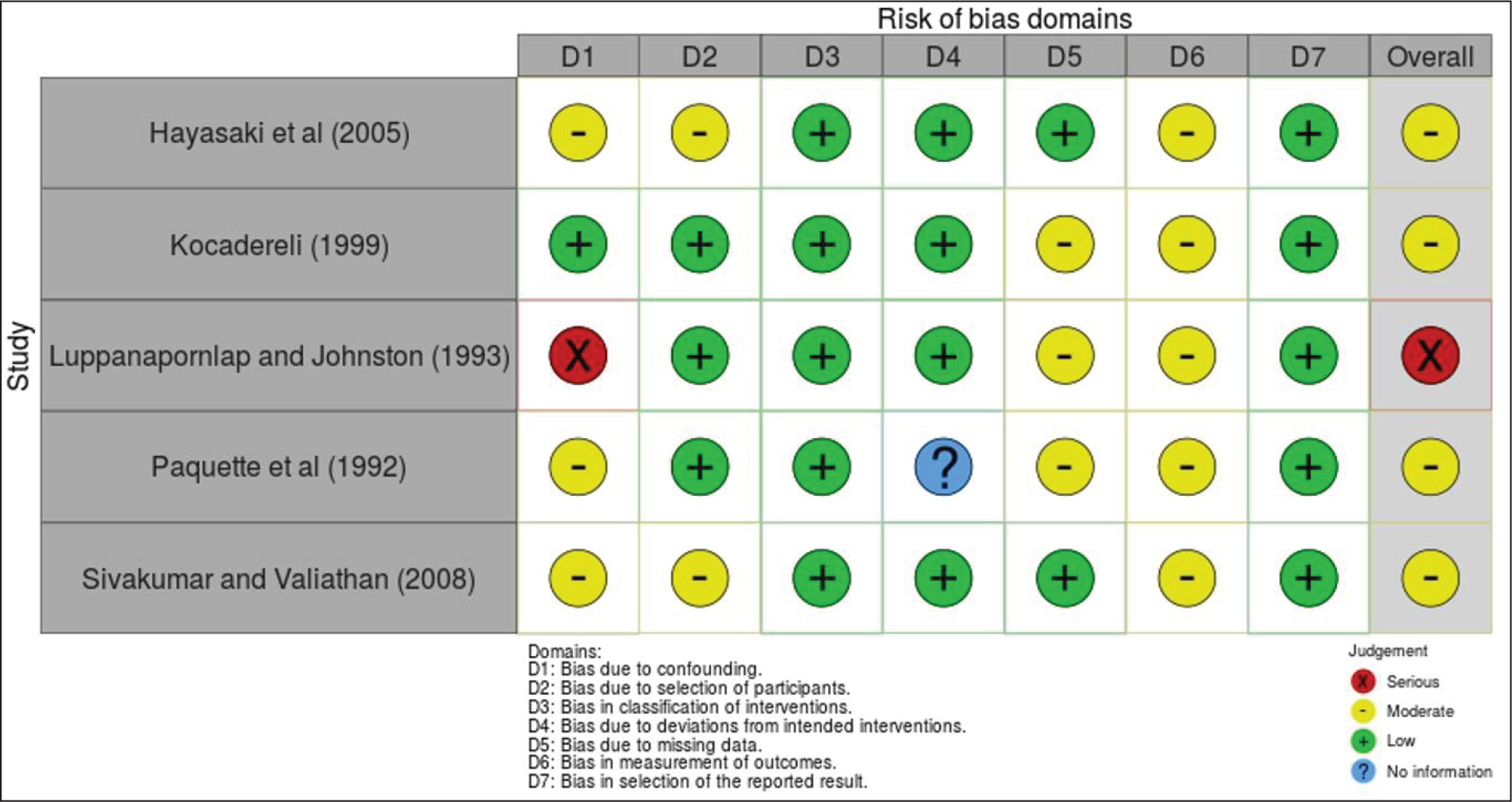
The Cochrane risk of bias (ROB) tool was used to investigate the risk of bias in each study with the help of Risk Of Bias In Non-randomized Studies-of Intervention (ROBINS-I) tool, 20 which evaluates seven domains (Ds) of bias in each study. Besides, an overall bias assessment is also made in the form of critical, serious, moderate, and low. 21 Risk-of-bias Visualization (robvis) 22 tool was used to design a traffic signal light plot and weighed plot for each study included in this review. Data obtained from the ROBINS-I tool were used to create both plots in which each study was given equal weight (1) for the weighed plot.
Risk of Bias Across Studies
Assessment of reporting biases across studies was planned for this appraisal but could not be conducted owing to the restricted number of included studies.
A standard funnel plot could also be drawn if it included more than 10 studies in the meta-analysis.
Summary Measures and Data Synthesis
The primary and secondary data of each included study were summarized separately. Secondary outcomes were observed only for those studies that had a primary outcome. Studies with either complete or incomplete data were included in this analysis, according to the need for quantitative and qualitative assessment. When necessary, data were omitted, if possible; it was either calculated from the existing data, or the corresponding author was contacted for further details.
Statistical heterogeneity was evaluated using tests including chi-squared-based Q-statistic, tau-squared, and I-squared statistics for within-study, absolute, and relative heterogeneity, respectively. 23 I-square statistic was reported to judge heterogeneity as high, moderate, and low, corresponding to values of 75%, 50%, and 25%. Fixed-effects model was used if I-square was <50%, and random-effects model was used if I-square was >50%. 24
Original data from primary studies were quantified using Review Manager 5.4 (RevMan) software. Considering that the included studies have several variables such as the patient’s age, appliance used, gender, and operator, a random-effects model was adopted to estimate the average distribution. Standard mean difference (SMD) at a 95% confidence interval (CI) was calculated for meta-analysis. Also, subgroups of Class I and Class II were formed in forest plots for both primary and secondary outcomes.
Results
Study Selection
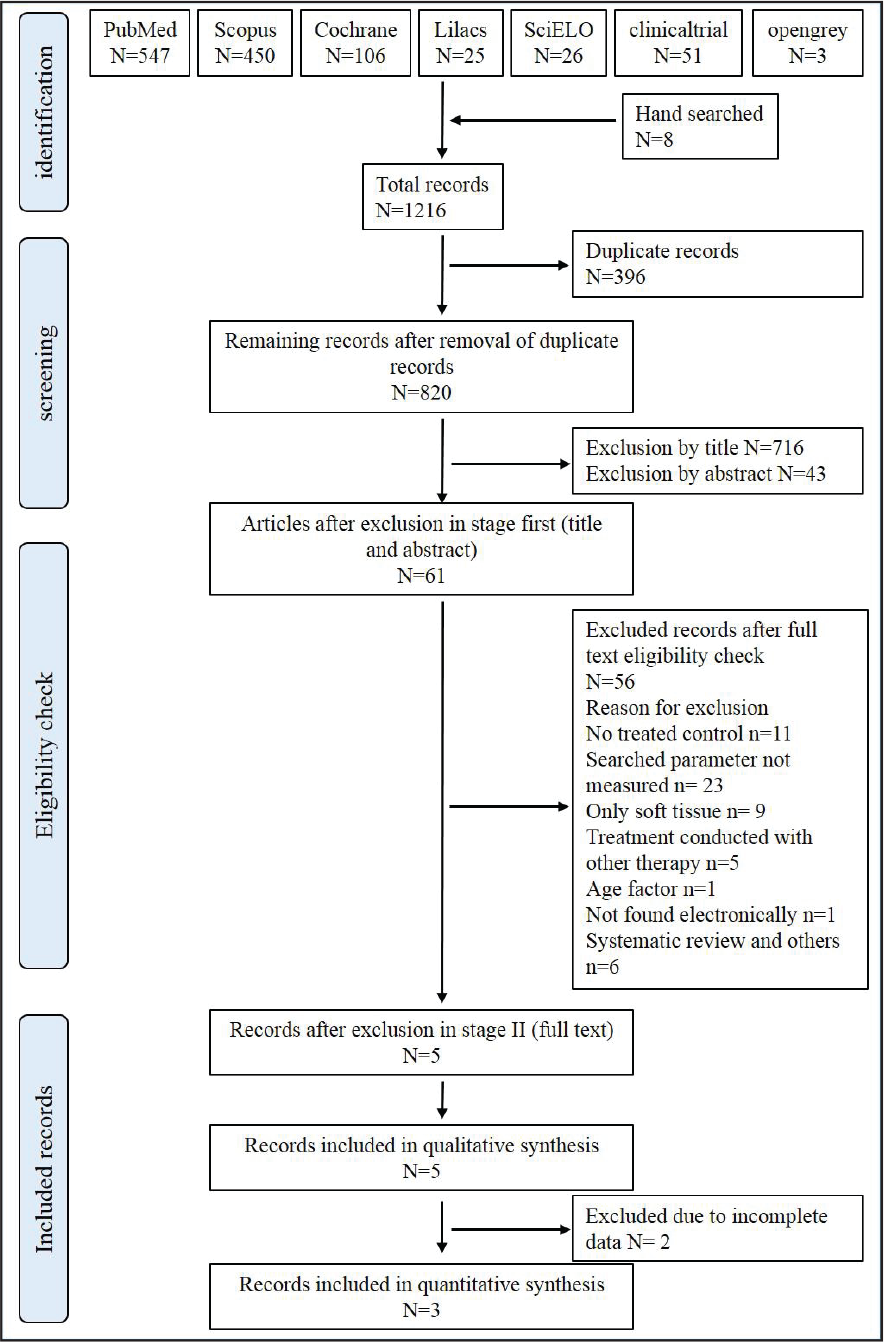
A total of 1,216 records, including 396 duplicates, were found during the literature search. A detailed study selection protocol is presented in Figure 1. After conducting stage 1 screening, 716 records were excluded based on the title, and 43 records were excluded based on the abstract. The remaining 61 records were then screened for stage 2. After applying inclusion and exclusion criteria on full-text reading, only five records25-29 were selected for qualitative evaluation, and only 3 articles27-29 were considered suitable for quantitative analysis, as the other two studies25, 26 had missing data.
PRISMA Flow Diagram for Identification and Retrieval of Studies.
Study Characteristics
Study Design, Intervention, and Outcome Assessment of all Included Studies for Qualitative Data Synthesis.
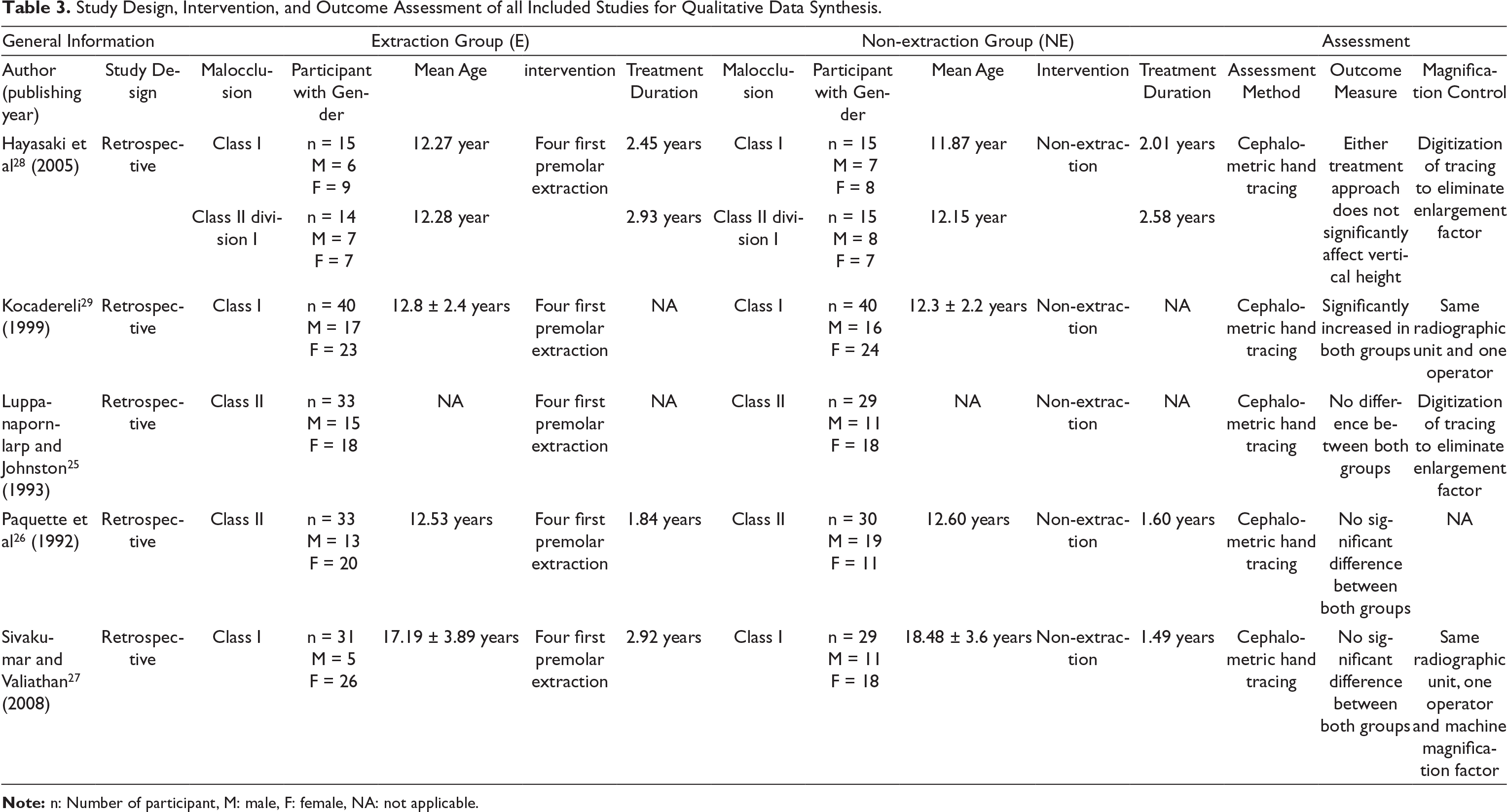
Note: n: Number of participant, M: male, F: female, NA: not applicable.
These five studies25-29 included a total number of 166 patients in the extraction group and 158 patients in the non-extraction group. The male to female ratio was not divided equally into any of the included studies, except for one study 28 that had a considerable same ratio. Three studies26, 28, 29 had reported a mean age of 12 years in both treatment groups. Age distribution was not given for one study 25 and another study 27 had a mean age of 17.5 years.
Among all included studies, only one study 28 had evaluated changes for both Class I and Class II malocclusion separately. Effects of either treatment on Class I malocclusion and Class II malocclusion were evaluated independently in studies carried out by Sivakumar and Valiathan 27 and Kocadereli, 29 and studies carried out by Luppanapornlarp and Johnston 25 and Paquette et al, 26 respectively. The average treatment duration was different among all the studies. Treatment outcomes in all studies25-29 were measured using pre- and post-lateral cephalograms, and hand tracings were performed to record primary and secondary outcomes. Most importantly, magnification control was achieved by the digitization of the tracing to eliminate radiographic enlargement in two studies,25, 28 but the other two studies had used the same radiographic machine, and one operator for the assessment, so that uncertainty could be minimized.27, 30 Only one study did not report any magnification control. 26
Risk of Bias Within Studies
As mentioned earlier, ROB was assessed using the ROBINS-I tool for non-randomized studies, and seven domains for every included study were assessed. Four studies were categorized at moderate risk,26-29 and one was at serious risk (Figure 2, Table 4). 25
Risk of Bias Summary Using Traffic Signal Light Plot Designed via Robvis Tool for Individual Study.
Summary of Risk of Bias of Included Studies Using ROBINS-I Cochrane Collaborated Tool.
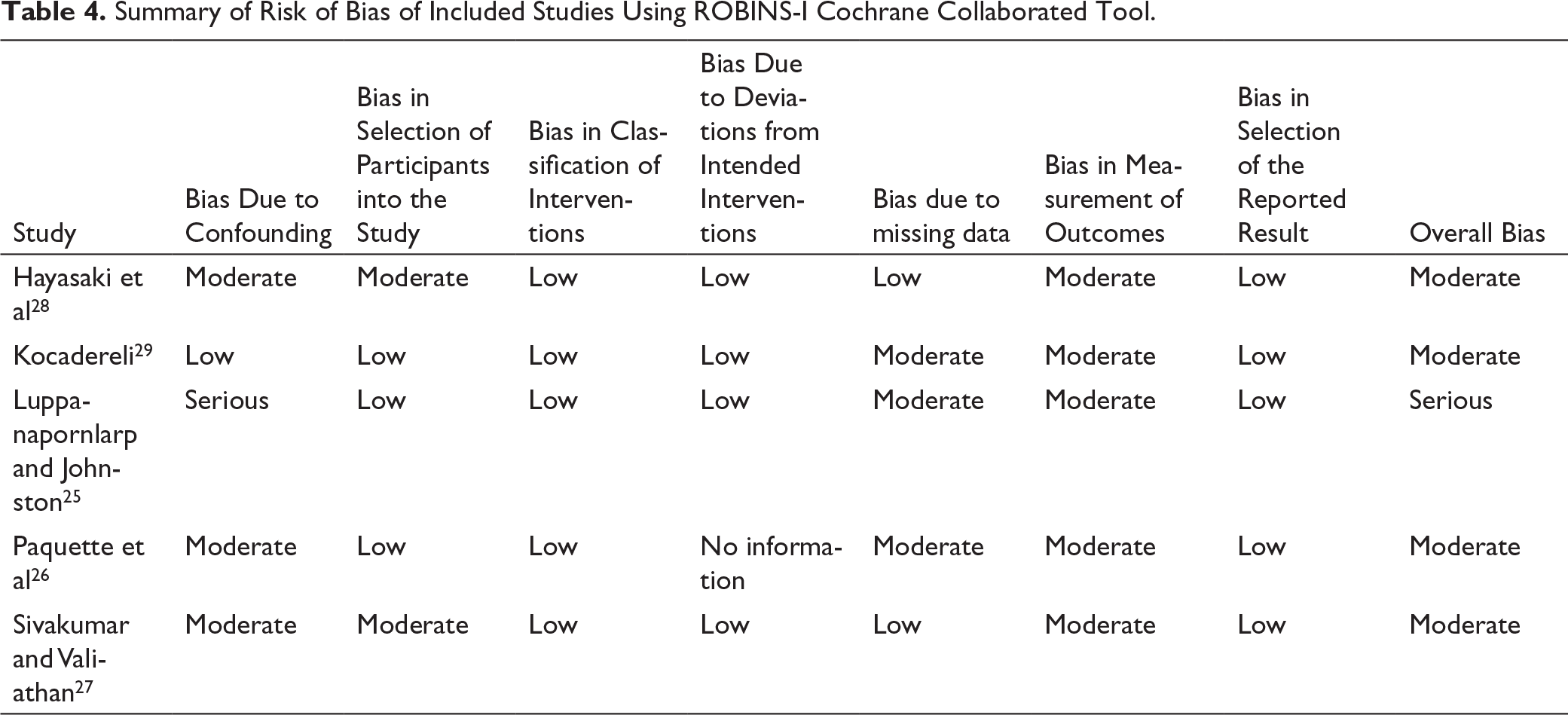
Bias due to confounding was serious in one study 25 due to different group characteristics but moderate for two studies.26, 28 Classification of intervention and selection of reported result biases were at low risk, and measurement of outcome bias was at moderate risk for all included studies25-29 because blinding of the operator was not possible. A detailed form of ROB is presented in Table 5, and a traffic signal light plot and weighted plot for each study are presented in Figures 2 and 3, respectively, for the evaluation of the ROB within the included studies.
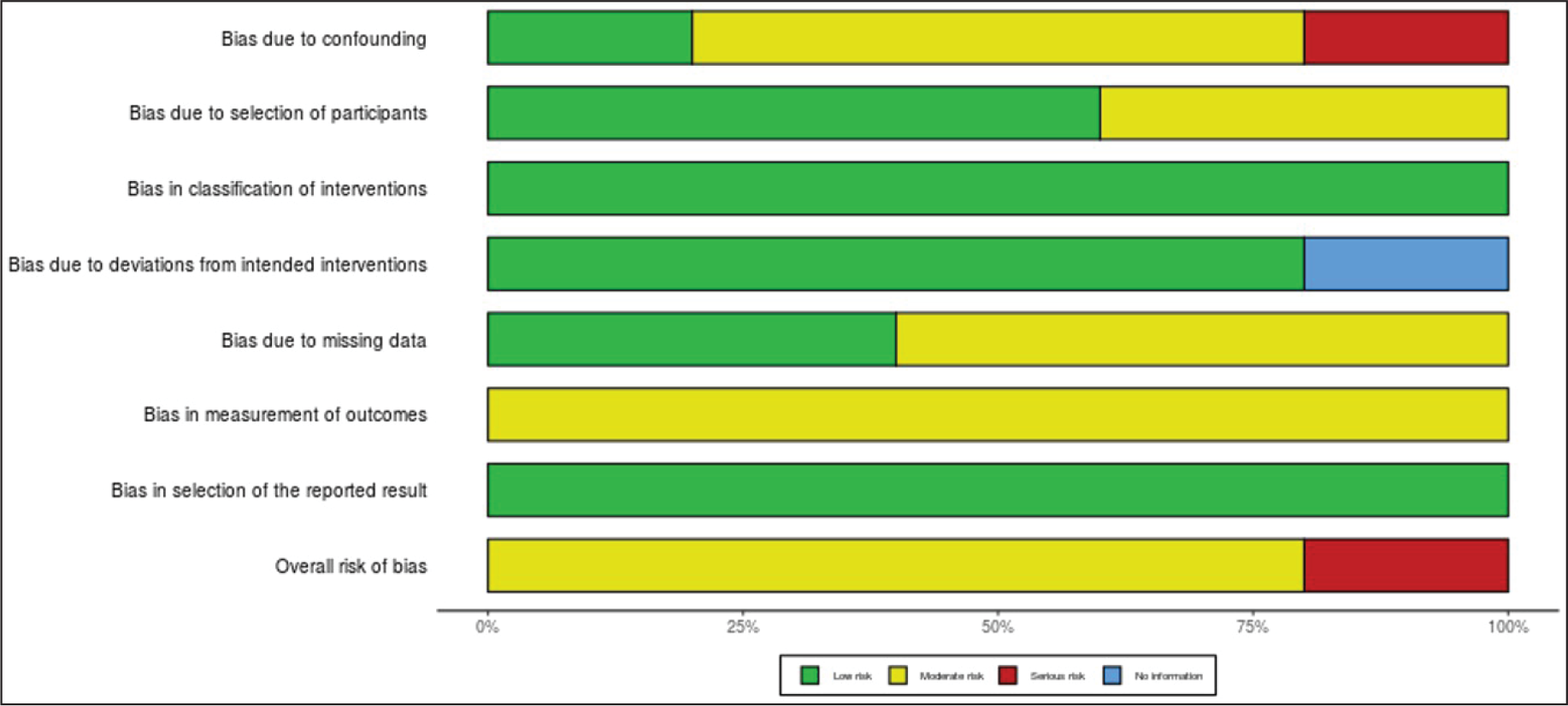
Risk of Bias Summary Using Weighted Plot Designed via Robvis Tool. All Studies Were Given Equal Weight for Qualitative Assessment.
Statistical Outcome Summary of ANS-Me for Each Included Study for Both Qualitative and Quantitative Analysis.
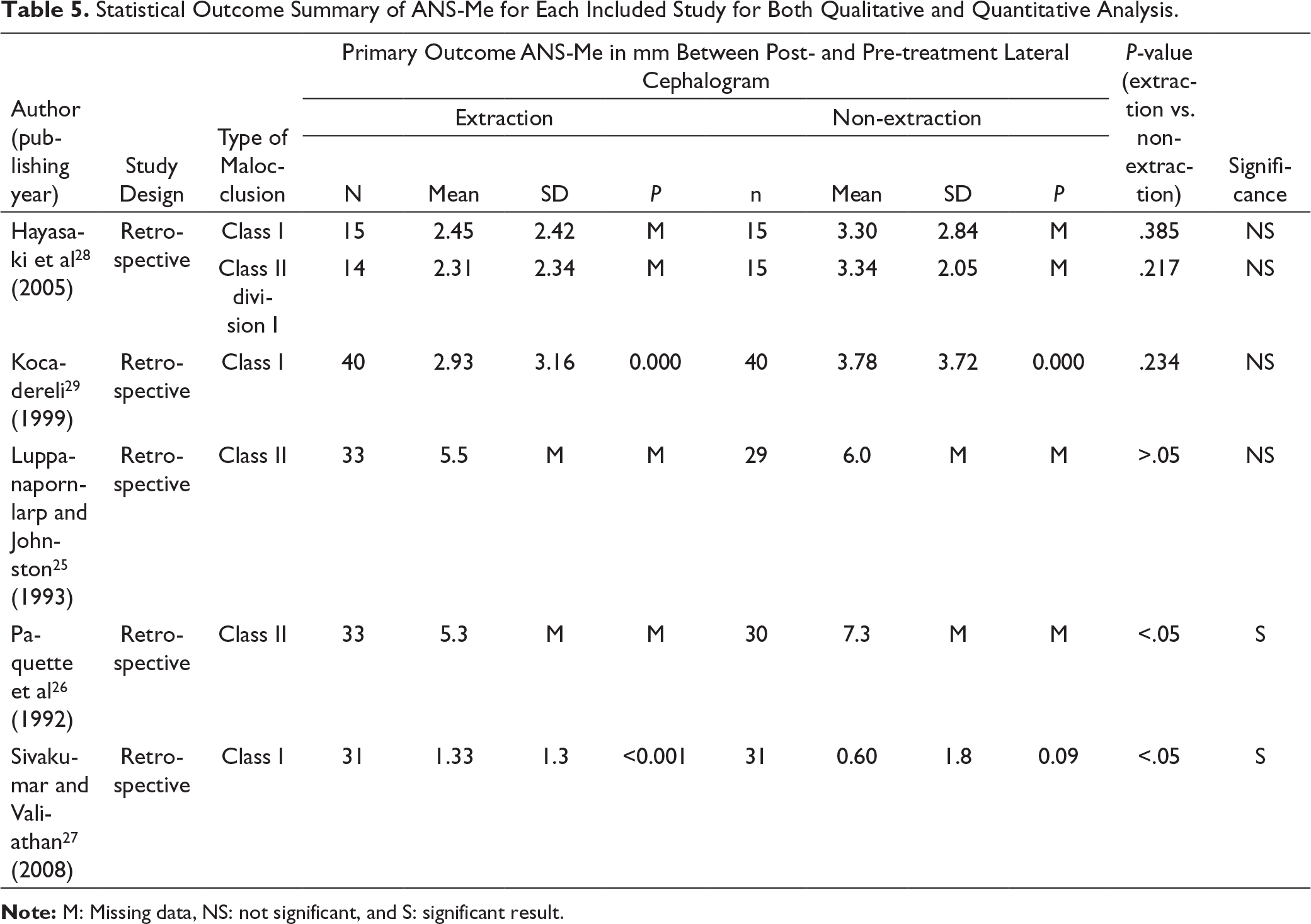
Note: M: Missing data, NS: not significant, and S: significant result.
Results of Individual Studies and Meta-analysis
Statistical results of each included study for both primary and secondary outcomes are listed in Tables 5 to 7. Extraction of all four first premolars was carried out in the experimental group, and relevant changes were compared with a non-extraction group for estimate changes in the parameter of lower anterior facial height.
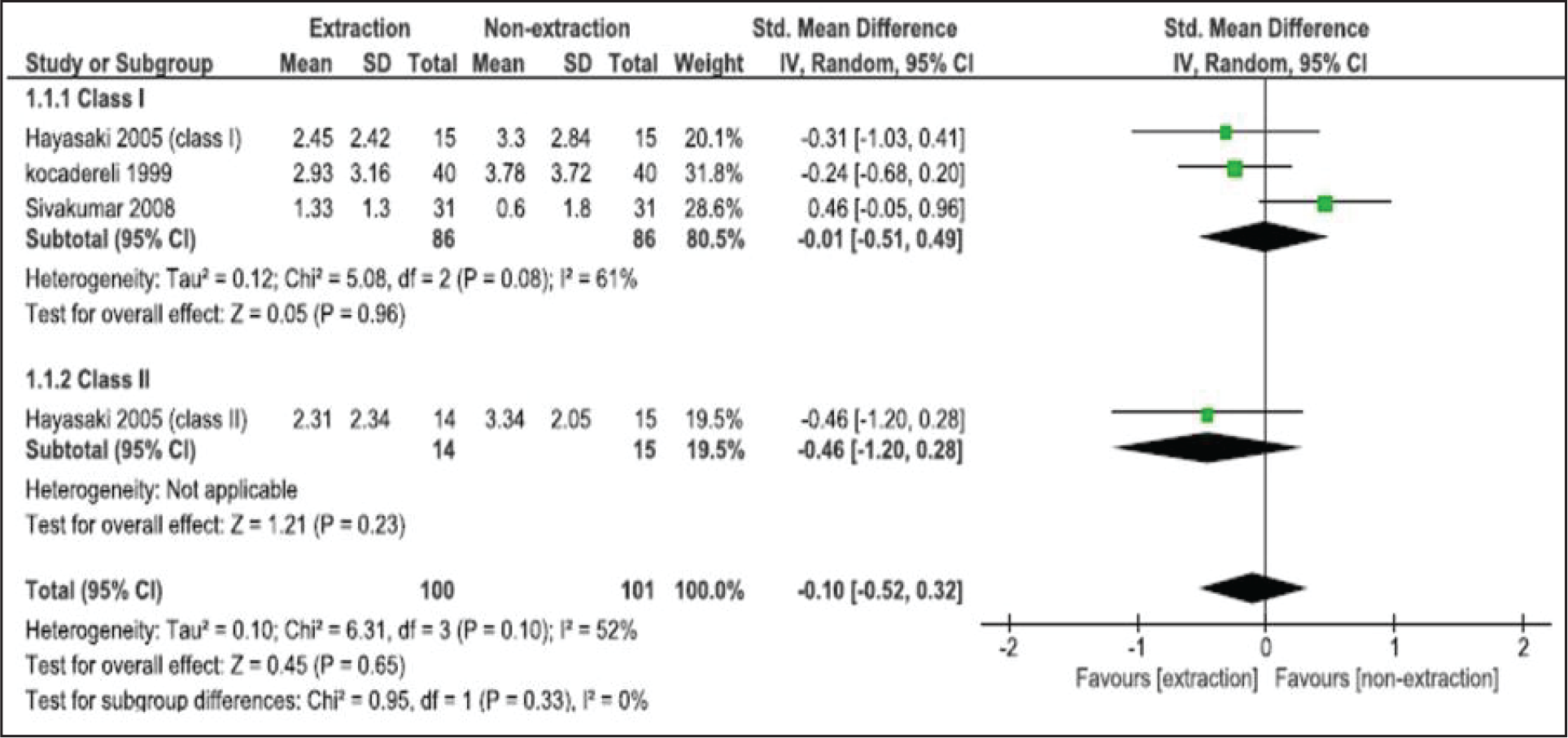
Primary Outcome: Lower Anterior Face Height (ANS-Me) in Millimeter
The effect on Lower Anterior Face Height (LAFH) from Anterior Nasal Spine to Menton (ANS-Me) was measured in all 5 included studies as the primary outcome for qualitative analysis. Two out of the 5 included studies favored statistical changes of LAFH between both groups (P < .05).26, 27 Although three studies estimated that extraction of four first premolars did not have any effect on LAFH (P > .05; Table 5).25, 28, 29
Only three studies were included for quantitative analysis (meta-analysis),27-29 and the other two studies were excluded from meta-analysis, owing to the lack of data.25, 26 Class I and class II subgroups were also created in the forest plot. The SMD found by Hayasaki et al 28 for Class I was −0.31 mm with 95% CI of −1.03 to 0.41 and for Class II was −0.24 mm with 95% CI of −0.68 to 0.20; by Kocadereli, 29 it was −0.24 mm with 95% CI of −0.68 to 0.20; and by Sivakumar and Valiathan, 27 it was 0.46 mm with 95% CI of −0.05 to 0.96. From these three studies, a heterogeneity (I 2 ) of 52% was reported, and an overall pooled estimate of −0.10 mm with 95% CI of −0.52 to 0.32 overlapped the line of no difference with P = .65, indicating that the extraction of four first premolars do not affect LAFH with regard to ANS to Me (Figure 4).
Meta-analysis and Forest Plot of Included Studies for ANS-Me.
Secondary Outcomes
Statistical Outcome Summary of N-Me for Each Included Study for Both Qualitative and Quantitative Analysis.
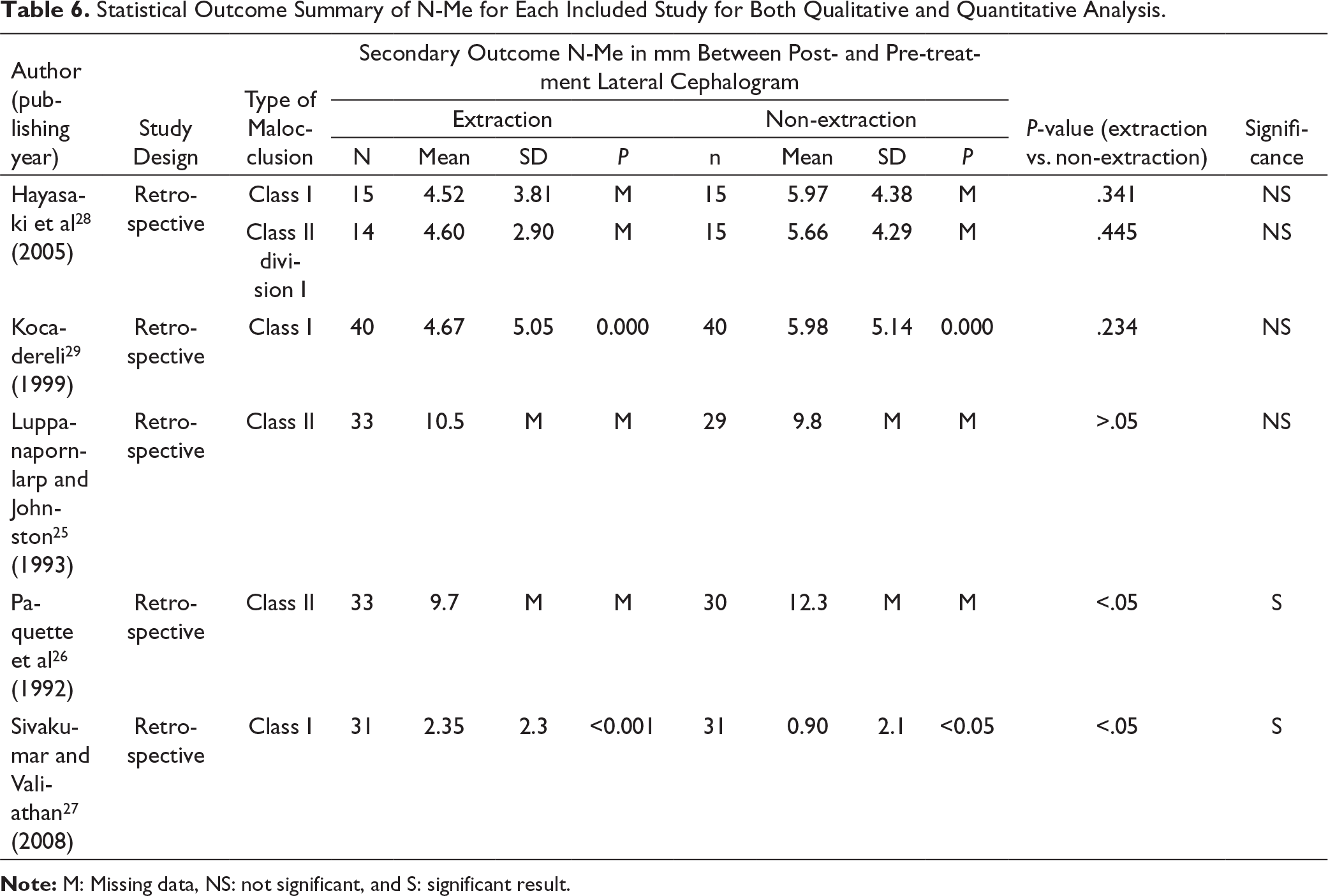
Note: M: Missing data, NS: not significant, and S: significant result.
Statistical Outcome Summary of FMA for Each Included Study for Both Qualitative and Quantitative Analysis.
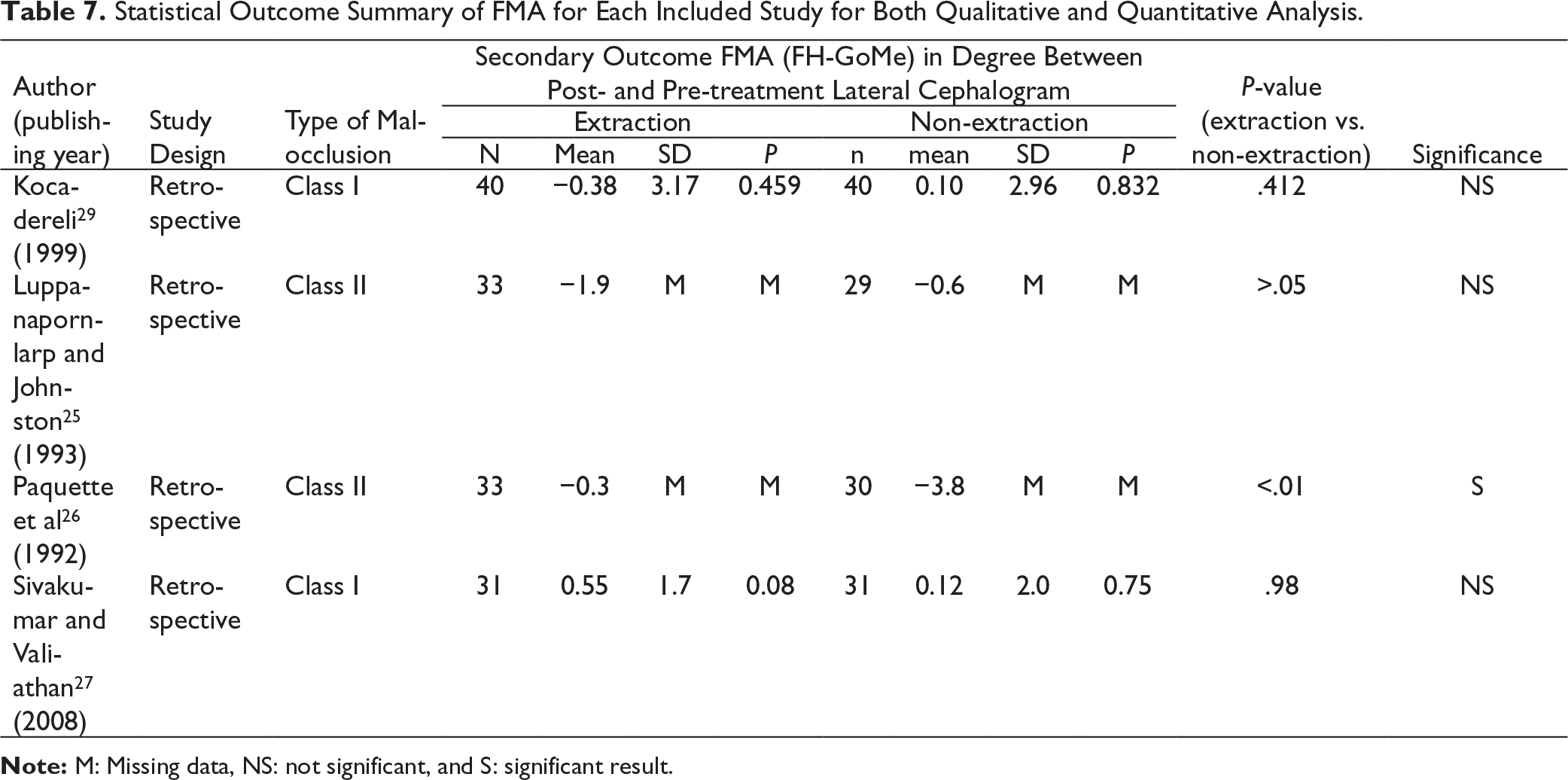
Note: M: Missing data, NS: not significant, and S: significant result.
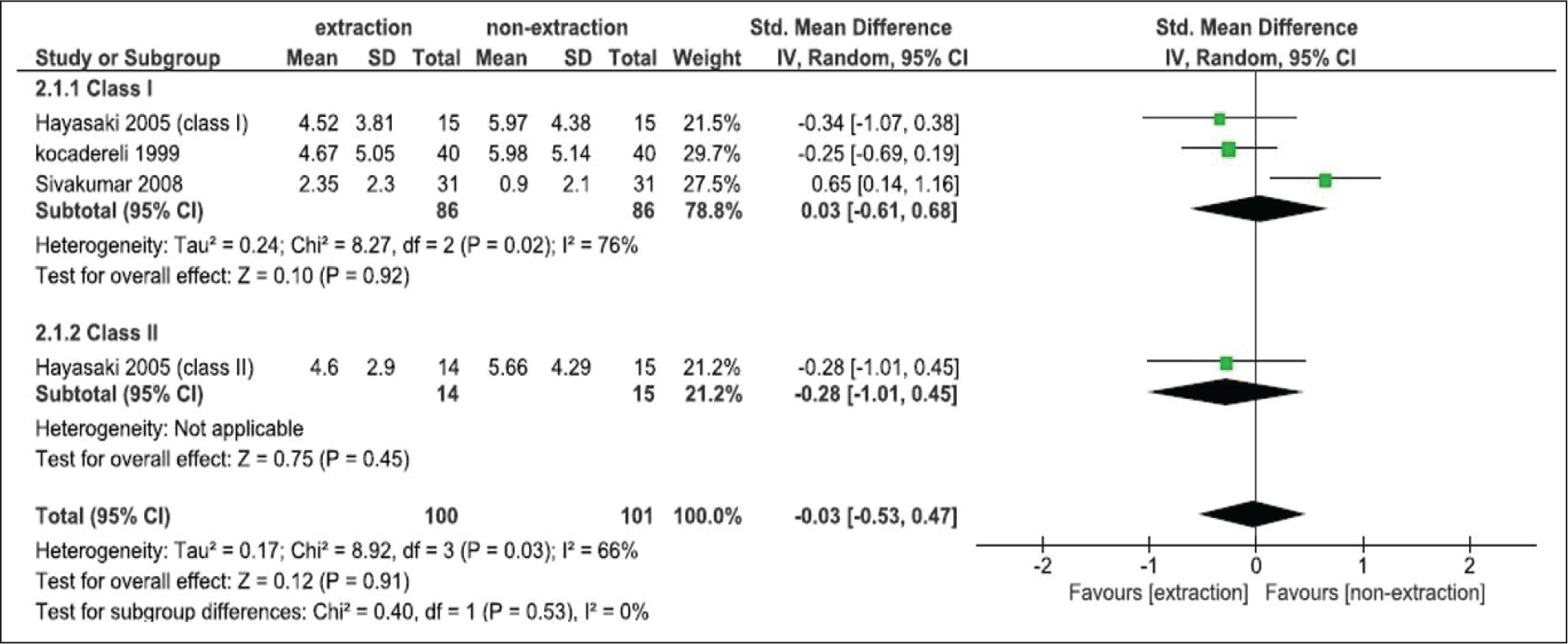
Three studies were included for quantitative analysis (meta-analysis)27-29 for TAFH, and only two were included for FMA.27, 29 Other studies were excluded from the meta-analysis for both outcomes, owing to lack of data. The SMD for TAFH found by Hayasaki et al 28 for class I was −0.34 mm with 95% CI of −1.07 to 0.38, for class II was −0.28 mm with 95%CI of −1.01 to 0.45; by Kocadereli 29 was −0.25 mm with 95% CI of −0.69 to 0.19; and by Sivakumar and Valiathan 27 was 0.65 mm with 95% CI of 0.14 to 1.16. From these three studies, heterogeneity (I 2 ) of 66% was reported and an overall pooled estimate of −0.03 mm with 95% CI of −0.53 to 0.47 overlapped the vertical line of no difference with P = .91 indicated that extraction of four first premolars do not affect TAFH in regards of N-Me (Figure 5).
Meta-analysis and Forest Plot of Included Studies for N-Me.
Although the SMD for FMA was −0.16 mm (95% CI, −0.59 to 0.28) by Kocadereli 29 and 0.23 mm (95% CI, −0.27 to 0.73) by Sivakumar and Valiathan 27 , a heterogeneity (I 2 ) of 22% and pooled estimate of 0.02 mm (95% CI, −0.36 to 0.39) overlapping the line of no difference with P = .93 indicated that the result was not in favor of either treatment (Figure 6).
Meta-analysis and Forest Plot of Included Studies for FMA.

Discussion
Whether the extraction of premolars left any effect on the lower anterior facial height has remained a debatable topic for several authors for many decades. A pearl of current wisdom has developed that extraction in hyperdivergent patients helps us to control increasing vertical direction, and it should be avoided in hypodivergent patients to avoid the closure of facial height.8, 31
As per our knowledge, this meta-analysis was the first to precisely address the effects of extraction of four first premolar on lower anterior facial height. However, a systematic review 32 on the effect of four premolar extraction and non-extraction treatment was recently published. Previous studies were conducted to check the effect of four premolars extraction on the vertical dimension, regardless of which premolar had been extracted. Also, these studies had not mentioned any specific appliance used for treating the subjects; extraoral appliances were also considered. The search terms for this review were also different from the previous one; this describes the variances in the numbers of the article retrieved. In our study, we focused only on subjects treated with fixed mechanotherapy and four first premolars extraction rather than any other extraction pattern. This explains the differences between inclusion and exclusion criteria of the studies, making this study more precise. Unlike other studies, we included articles published only in the English language. Moreover, the previous studies did not conduct any meta-analysis because of their inclusion criteria, and selected studies might produce biased results.
Nevertheless, we retrieved a total number of 1,216 articles with our search terms and ending up with five articles.25-29 One was the basis of the desired primary outcome for the synthesis of qualitative review, and three articles27-29 for meta-analysis, owing to lack of respective data. This article summarizes results from retrospective clinical studies on the effect of the first four premolars extraction on the lower anterior face height and strictly follows our inclusion and exclusion criteria. The level of evidence was III, as all included studies were retrospective.
While a detailed aspect of the treatment protocol for both extraction and non-extraction groups was not noted in any of the included studies, only extraction pattern and appliance used were given. This may produce a certain level of heterogeneity. The method for evaluating LAFH was almost similar and measured on pre- and post-treatment lateral cephalograms for all studies. These studies followed their protocol to control radiographic error; Hayasaki et al 28 and Luppanapornlarp and Johnston 25 preferred to analyze digitized hand tracing with Dentofacial Planner 7.02 software (Dentofacial Software, Toronto, Ontario, Canada), Kocadereli 29 and Sivakumar and Valiathan 27 used the same radiographic units and single operator, and no such processes were used by Paquette et al 26 to control radiographic error.
A meta-analysis of three included studies indicates that the extraction of four first premolars do not have any effect on LAHF, statistically, among all the outcomes with an effect estimate of −0.10 mm, −0.03 mm, and 0.02 mm for ANS-Me, N-Me, and FMA, respectively. Similar findings were also reported for secondary outcomes. A study carried out by Sivakumar and Valiathan 27 do slightly favor non-extraction group with an SMD of 0.46 mm (95% CI, −0.05 to 0.96), 0.65 mm (95% CI, 0.14 to 1.16), and 0.23 mm (95% CI, −0.27 to 0.73) corresponding to ANS-Me, N-Me, and FMA.
Limitations
Language restriction was applied for this study, studies published in the English language were included; thus, certain evidence might be missing, owing to them being published in other languages. A detailed treatment protocol was also missing from all studies (like the amount of crowding, methods of closing space), which could help us in synthesizing a more potent review. Secondary outcomes were evaluated only from studies included in this review and could be separately reviewed as primary outcomes. Moreover, all included studies are retrospective and are more prone to different types of biases (especially selection bias). Although it is difficult to conduct a prospective study or a randomized control trial for such a treatment protocol, selection bias will be a limitation and can be minimized by including borderline cases. More importantly, using a modern digital platform for cephalometric measurement would help to reduce radiological error, and would be beneficial for further studies.
Conclusion
From the existing evidence of this study, the following conclusions can be drawn: The meta-analysis of included studies showed that there is no specific effect of extraction of four first premolars treatment as compared with the non-extraction treatment carried out with fixed mechanotherapy on the lower anterior facial height and its different measures. It is not justified to extract or not to extract four first premolar teeth to control or reduce anterior facial height.