
Abstract
This case report was submitted to the board under category II for the Indian Board of Orthodontics examination in November 2017. This case report illustrated the treatment of class II division 1 malocclusion by pre-adjusted appliance along with Forsus Fatigue Resistance Device (FRD) fixed functional appliance (single-phase treatment) in a 13.6 year-old female patient whose growth was about to cease. The summary of the treatment, various records, treatment progress, and critical appraisal are reprinted here with minimal editing and reformatting, and hence, the presentation resembles the actual documents submitted to the board.
Keywords
Introduction
Class II malocclusion is a frequently encountered problem in orthodontic patients. The presence of skeletal class II malocclusion in adult patients is challenging, and patients often have high expectations regarding results. According to McNamara, 1 the most common characteristic of class II malocclusion is mandibular retrognathism rather than maxillary protrusion. 1 Functional orthopedic appliances are mostly used to treat class II malocclusion originated from mandibular retrusion.2, 3 Choice of appliance whether removable or fixed depends on existing anteroposterior discrepancy, growth period, and compliance of patient. Patients with class II mandibular retrusion in whom growth is about to cease are mostly treated with fixed functional appliances which do not require patient’s compliance.4-6
The following case report illustrates the treatment of class II division 1 malocclusion using fixed functional appliance (Forsus Fatigue Resistance Device [FRD]) in a 13.6 year-old female patient.
Case Report
AV, a 13-year 6-month-old female, presented with the chief complaint of forwardly placed upper front teeth. She presented with convex profile, class II skeletal base with retrognathic mandible, horizontal growth pattern, Class II molar and canine relation on right and left side, with mild crowding in lower anteriors. Model analysis revealed a space availability of 1.5 mm in the maxillary arch and space requirement of 1.5 mm in the mandibular arch. The patient was treated with non-extraction by fixed functional appliance—Forsus Fatigue Resistance Device (FRD) as a single-phase treatment. The appliance used was pre-adjusted edgewise appliance with slot size 0.018″ × 0.025″, MBT (3M orthodontics).
Section 1: Pretreatment Assessment Details
Initials: AV
Sex: Female
Date of birth: December 5, 2002
Age at start of treatment: 13 years, 6 months
Patient’s complaints: A 13.6 year-old female reported with a chief complaint of forwardly placed upper front teeth.
She had not given any significant medical, family, and dental history.
Clinical Examination: Extra-Oral Features
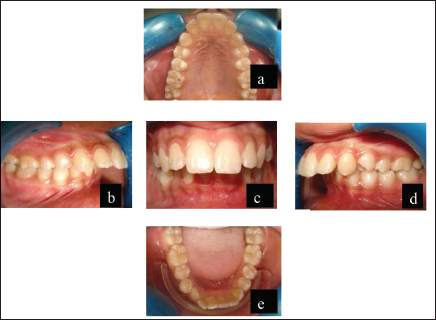
Extra-oral examination revealed good general health of patient with mesomorphic body type and mesoprosopic facial type. Patient was having orthognathic maxilla, retrognathic mandible, decreased mandibular plane angle, convex facial profile, and upward tipped nose with incompetent lips. Mentolabial sulcus and chin was found average. Pretreatment extra-oral photographs are shown in Figure 1.
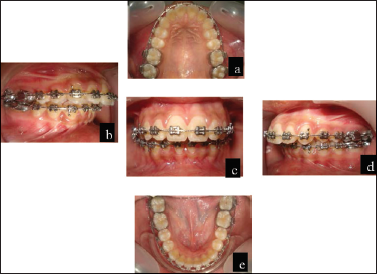
Clinical Examination : Intraoral Features
Pretreatment intraoral photographs are shown in Figure 2.
Soft tissues: No abnormality detected Oral hygiene: Good Erupted teeth present: General dental condition: Good dental and periodontal health.
Crowding/Spacing
Maxillary arch: V-shaped symmetrical arch with proclined upper anteriors along with mild spacing present between lateral incisor and canine bilaterally
Mandibular arch: U-shaped asymmetrical arch with mild crowding in the anterior region with rotated canines and second premolars bilaterally

Occlusal Features
Incisor relationship: Class II division 1
Overjet (mm): 14 mm
Overbite: 7 mm
Centre lines: Lower dental midline shifted toward right side.
Left buccal segment relationship: Class II molar relation, class II canine relation
Right buccal segment relationship: Class II molar relation, class II canine relation
Cross bite: Scissor bite: 14, 24
Rotations: Distobuccal rotation with both lower second premolar and distolingual rotation with both lower canines
Curve of Spee: Exaggerated
Model Analysis: Ashley Howe’s analysis indicated that this was a borderline case; Carey’s analysis indicated that this was a non-extraction case; Pont’s analysis indicated that expansion was required in premolar and molar regions; and Bolton’s analysis showed overall maxillary excess by 1.08 mm and anterior maxillary excess by 0.66 mm.
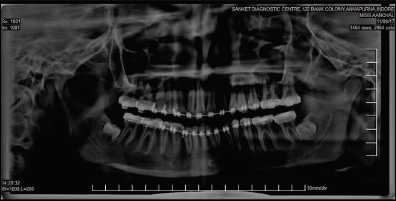
General Radiographic Examination
Pre-treatment radiographs taken
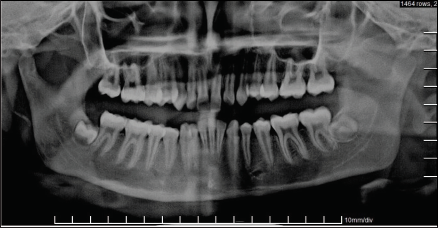
Relevant Radiographic Findings
The normal complement of permanent teeth was present with no abnormalities of the surrounding structures and regions; additionally, there were no abnormalities in the tooth form. The third molars in maxillary arch were congenitally absent and were unerupted in mandibular arch. The alveolar crestal bone level of the teeth present was within the normal limits of the cemento-enamel junction (CEJ).
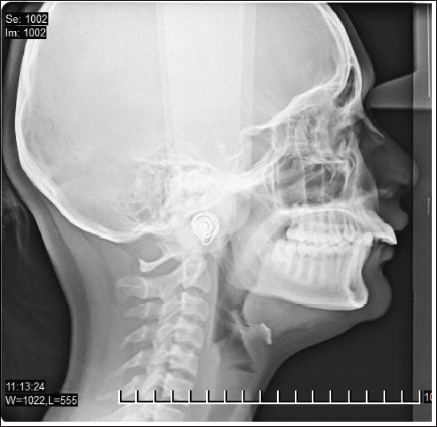
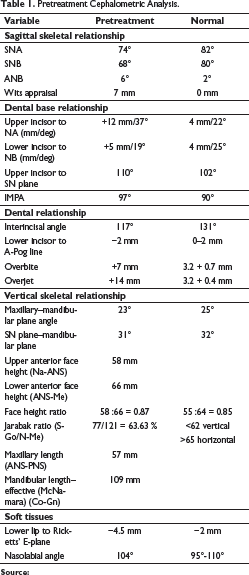
Pretreatment Cephalometric Interpretation
Pretreatment cephalometric values are given in Table 1.
Skeletal class II base with retrognathic maxilla and retrognathic mandible Horizontal growth pattern Convex profile Incompetent lips.
Pretreatment Cephalometric Analysis.
Source:
Diagnostic Summary
The skeletal and dental relationships confirm a Class II skeletal base malocclusion due to retrognathic mandible along with Class II molar and canine relation on right and left side with proclinated upper anteriors and mildly crowded lower anteriors. In model analysis, Bolton ratio showed minimal excess of maxillary tooth material. Cephalometric analysis revealed skeletal class II base with retrognathic maxilla, retrognathic mandible with horizontal growth pattern. Overall diagnosis was Class II skeletal bases with retrognathic maxilla, retrognathic mandible, horizontal growth pattern, Class II molar relation on right and left side with proclined upper anteriors and mild crowding in lower arch, and convex profile with incompetent lips.
Problem List
Skeletal class II base due to retrognathic mandible
Proclined upper anteriors and mild crowding in
lower arch
Class II molar and canine relation on right and
left side
Increased overjet
Deep bite
Incompetent lips.
Aims and Objectives of Treatment
Correction of the class II skeletal base
To improve profile and smile
To correct proclination of upper anteriors
To relieve crowding in lower arch
To achieve class I molar and canine relation on
both sides
To reduce overjet
To correct deep bite
To establish functional occlusion
To ensure long-term stability.
Treatment Plan
The case was treated with non-extraction using a fixed functional appliance like Forsus FRD along with a pre-adjusted edgewise appliance with slot size 0.018″ × 0.025″, MBT (3M Orthodontics).
Proposed retention strategy: Long-term upper Hawley’s retainer with reverse anterior inclined plane and lower bonded retainer from canine to canine.
Prognosis for stability: Good.
Section 2: Treatment
Treatment Progress
Start of active treatment: June 2, 2016
Age at start of active treatment: 13 years 6 months
End of active treatment: November 9, 2017
Active treatment time: 17 months
End of retention: Long-term upper Hawley’s retainer with reverse anterior inclined plane and lower bonded retainer from canine to canine.
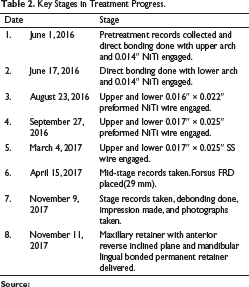
Key Stages in Treatment Progress
Key stages in treatment progress of this patient are given in Table 2.
Mid-treatment extra-oral and intraoral photographs are shown in Figures 5 and 6.
Key Stages in Treatment Progress.
Source:

Source: Patient records.
Source: Patient records.

Source: Patient records.

Source: Patient records.
Section 3: Post-treatment Assessment
Post-treatment extra-oral and intraoral photographs are shown in Figures 9 and 10.
Occlusal Features
Incisor relationship: Class I
Overjet (mm): 2 mm
Overbite: 2 mm
Centre lines: Almost coinciding
Left buccal segment relationship: Canine class I and molar class I relation
Right buccal segment relationship: Canine class I and molar class I relation
Crossbites: Scissor bite with 14, 24 corrected
Functional occlusal features: No functional Shift and TMJ functions with full range of mandibular movements
Other occlusal features: Curve of Spee leveled.
Complications Encountered During Treatment
No complications were encountered during the entire treatment.
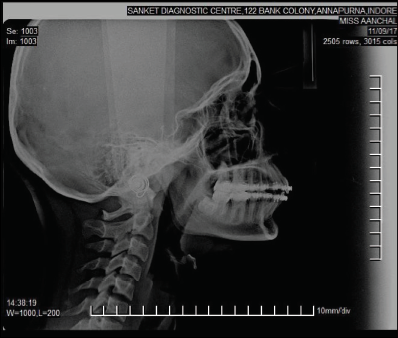
Radiographs Taken Toward/at the End of Treatment
Orthopantomogram (November 9, 2017) (Figure 11)
Lateral cephalogram (November 9, 2017) (Figure 12)

Source: Patient records.

Source: Patient records.
Source: Patient records.
Source: Patient records.
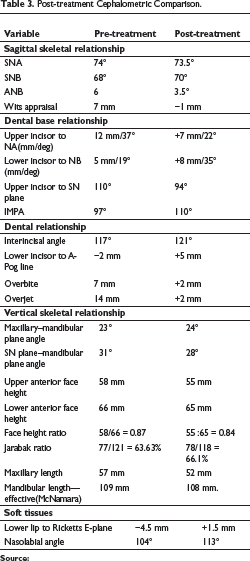
Post-treatment Cephalometric Interpretation
Post-treatment cephalometric comparison is given in Table 3.
Skeletal Effects: Maxillary–mandibular relation was improved.
Dental effects: Ideal overjet and overbite were achieved.
Class I molar and canine relationship was achieved.
Midline almost coinciding
Soft tissue effects: Profile showed a marked improvement.
Lip competency achieved.
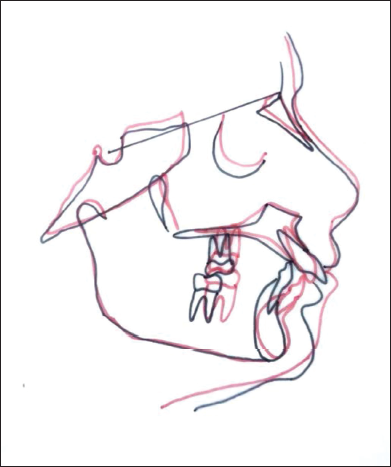
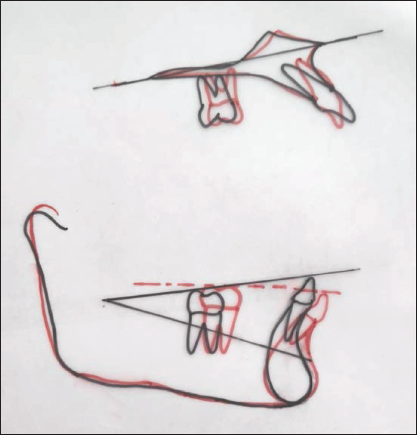
Cephalometric Superimpositions
Cephalometric superimpositions are shown in Figures 13 and 14.
Section 4: Critical Appraisal
Post-treatment Cephalometric Comparison.
Source:
Skeletal base relationship was improved.
Ideal overjet and overbite was achieved.
Class I molar and canine relation was achieved.
Profile was improved markedly.
Lip competency was achieved.
Good functional occlusion was achieved.
Footnotes
Declaration of Patient Consent
The other clarify that they have obtained all appropriate patient forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patient understands that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Declaration of Conflicting of Interests
Funding
The author received no financial support for research, authorship and/or publication of this article.