
Abstract
Objective:
The aim of this study is to assess the influence of general attitude and attitude toward orthodontic treatment on bracket failure rate.
Methods and Materials:
The sample comprised 128 orthodontic patients of both genders (82 women and 46 men), divided into two groups—adolescents (12-18 years old) and adults (19-25 years old), who underwent fixed orthodontic treatment with metallic braces. Two questionnaires were handed out—one before beginning the treatment and, the second, 6 months after the start of treatment. Both the questionnaires consisted of 12 questions with 5 options each, in which the attitude was scored from 1 to 5.
Conclusion:
Patients with poor attitude scoring had higher bracket failure rate and vice versa.
Introduction
Malocclusion is defined as an irregularity of the teeth or a malrelationship of the dental arches beyond the range of what is accepted as normal. 1 Malocclusions can be managed effectively by the orthodontist with the use of various appliances that may be removable, fixed, or functional, which also results in the correction and improvement of dentofacial esthetics, function, and speech. To obtain a satisfactory result following fixed orthodontic treatment, the adhesion of brackets to the teeth as handles for applying force is absolutely essential.
One of the most common clinical problems encountered by an orthodontist, which can be frustrating during orthodontic treatment, is the accidental breakage of brackets. Clinical experience strongly suggests that some patients are more prone than others to bracket failures. Bracket failure increases chair-side time and inevitably compromises treatment time/results. Identification of factors contributing to treatment overruns is, therefore, extremely important to success in orthodontic practice. 2 There are various reasons that can be attributed to bracket failure among which are operator-related factors such as the bonding technique, patient cooperation and compliance with dietary and oral hygiene instructions, type of etchant or adhesive used, and bracket properties.3-10 Several studies have been carried out to evaluate the influence of age, gender, and diet on bracket failure rates.4,7,11-18
The motivation and cooperation of the patient for orthodontic treatment has been shown to be an important factor, especially when considering time and even quality of the results. It is in this context that we have carried out the present study to assess whether there was a correlation between the attitude of patients and bracket failure rate, which also include correlation of the general attitude of patients and attitude of patients toward the instructions given by the doctor and toward orthodontic treatment.
Material and Methods
This prospective study was conducted in the Department of Orthodontics and Dentofacial Orthopedics and was approved by the Institute Ethics Committee (No. IEC/MES/55/2017). The sample included 128 patients, 12 to 25 years old, who underwent fixed orthodontic treatment with metallic brackets.
Sample Selection
The methodology and protocols involved for the selection criteria of the patients have been outlined below.
Inclusion Criteria
Fixed appliance therapy of maxillary and mandibular arches using metal brackets.
Age between 12 years and 25 years.
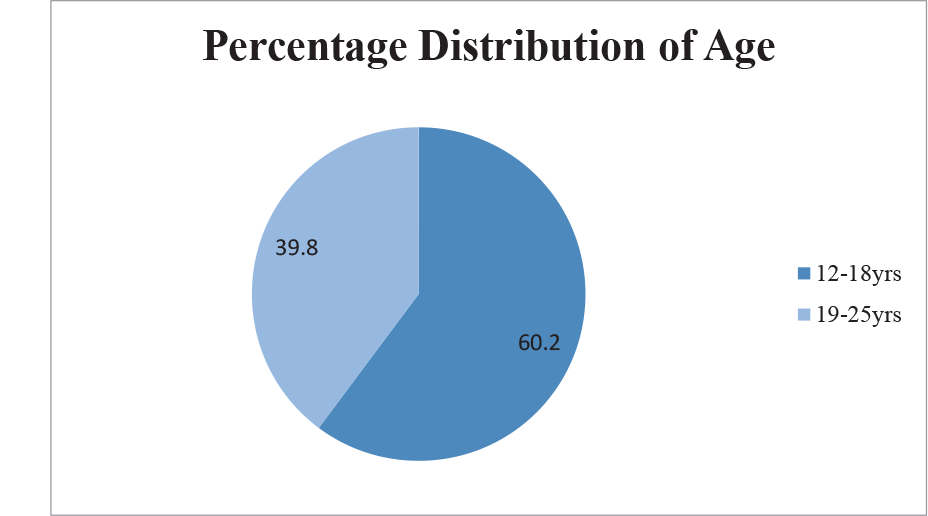
Patients were divided into two groups based on their age (Figure 1):
12 to 18 years—Adolescent group
19 to 25 years—Adult group
Exclusion Criteria
Craniofacial anomalies.
Patients with known history of behavioral problem.
Developmental defects involving enamel.
Patients who had undergone previous fixed orthodontic treatment.
Teeth with fillings, hypoplasia, white spots on the buccal surface, or a prosthetic crown.
Rebonded brackets.
Bracket failure during the placement of initial archwire.
Teeth which have vertical occlusal clearance of 2 mm or less were banded and, therefore, excluded from the study.
Molars were excluded from the study as they were banded.
Patients, whose treatment duration was 6 to 8 months, were not included in the study.
Sample Preparation
The brackets were bonded by three faculty of our department, who had a minimum of 5 years’ experience. Standard protocols of bonding were followed.
Percentage Distribution of Age Groups.
Orthodontic Brackets and Light Cure Composite Used in the Study.
Protocol for Bonding
A total of 2135 brackets bonded to the enamel surface of 128 patients were evaluated. Enamel surfaces of incisors, canines, and premolars were cleaned with fluoride-free pumice with a rubber polishing cup and were etched with 37% phosphoric acid (Anabond Stedman) for 20 seconds. After thorough washing for 60 seconds, the enamel surfaces were dried with compressed air. Primer (Transbond XT) was applied on the tooth surface (Figure 2). Composite (Transbond XT 3M UNITEK) was placed on the bracket base (ORMCO 022″ MBT prescription), and the bracket was positioned firmly on the tooth. Excess composite was removed from the tooth surface with a sharp probe before curing the material for 40 seconds (Koden Light Cure Unit). The usual choice of initial aligning archwire was 0.014-inch Nickel–Titanium (NiTi) wire, followed by progressively thicker NiTi wires, and finally 0.019 × 0.025-inch stainless steel wire. In case of crowded teeth, at the time of initial ligation, the NiTi wire was deflected only to a maximum of 2 mm to prevent excessive application of force, resulting in inadvertent bracket failure. Patients were instructed to report to the clinic as soon as a bond failure was noted by them.
During treatment, patients were given appointments at 4-week intervals. Bond failures were recorded accurately in the pro forma for later statistical analyses. The date of bond failure was identified as the date when detachment was observed by the patient/confirmed by clinician, whichever was earlier. The brackets were replaced immediately after bond failure was detected by the clinician. Rebonded brackets were excluded from the study because replacing a bracket could affect its bond strength. All patients were observed till the end of treatment.
Sample Collection
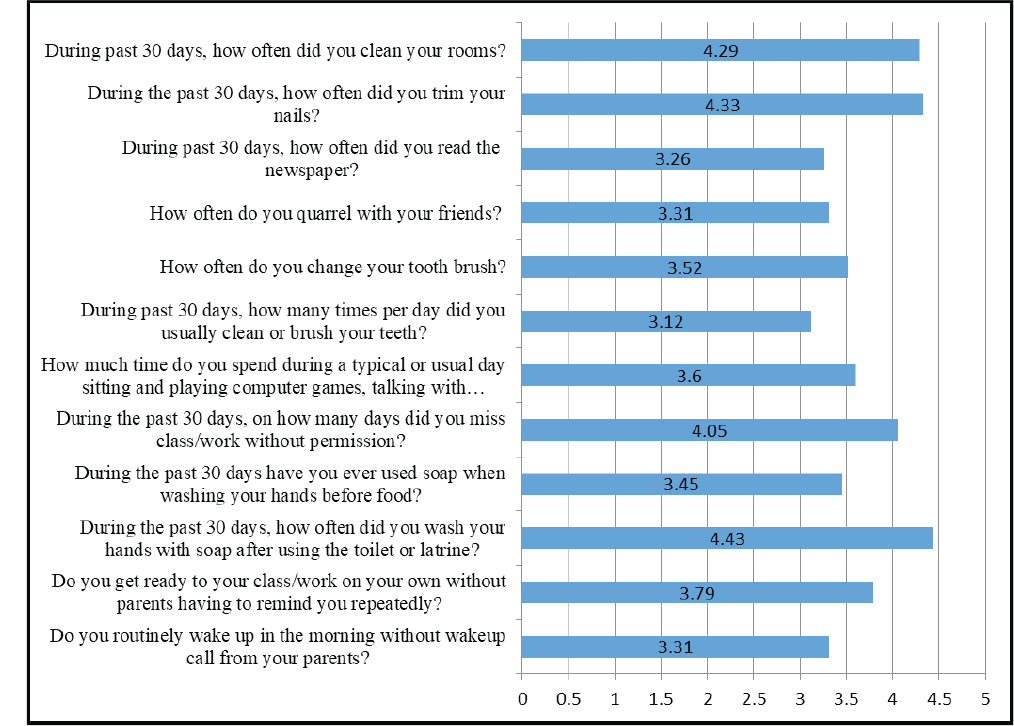
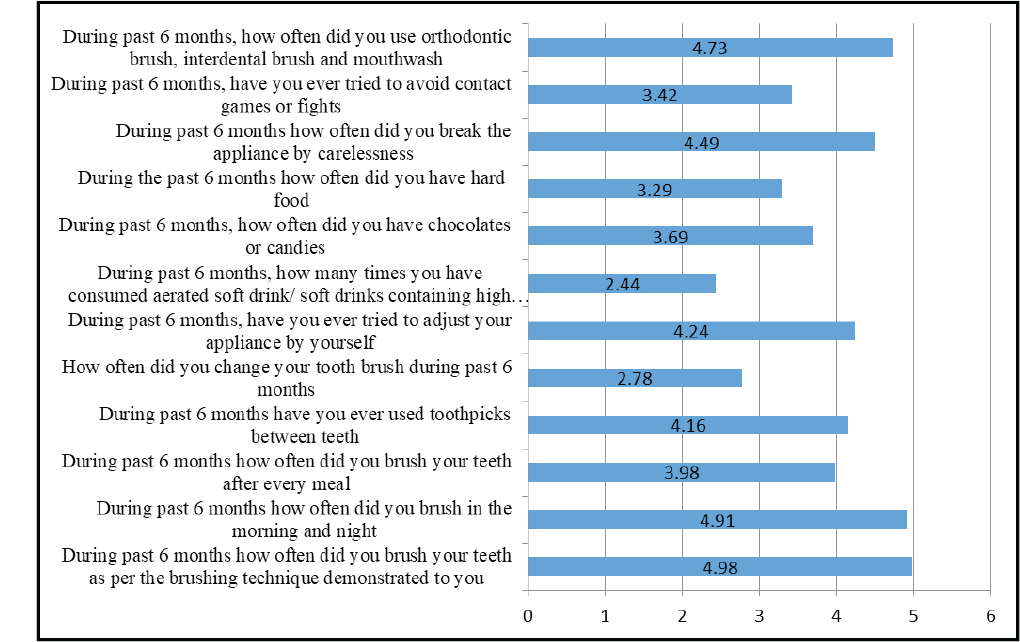
In this study, two different questionnaires were handed out to assess the attitude of patients—one at the beginning of the treatment and, the second, 6 months after the start of treatment. Both the questionnaires consisted of 12 questions with 5 options each, in which the attitude was scored from 1 to 5.
The following sociodemographic- and treatment-related information were recorded from each patient:
date of birth; sex; general attitude of the patient; date of bonding; and the fate of each bracket was recorded month-wise up to the end of treatment.
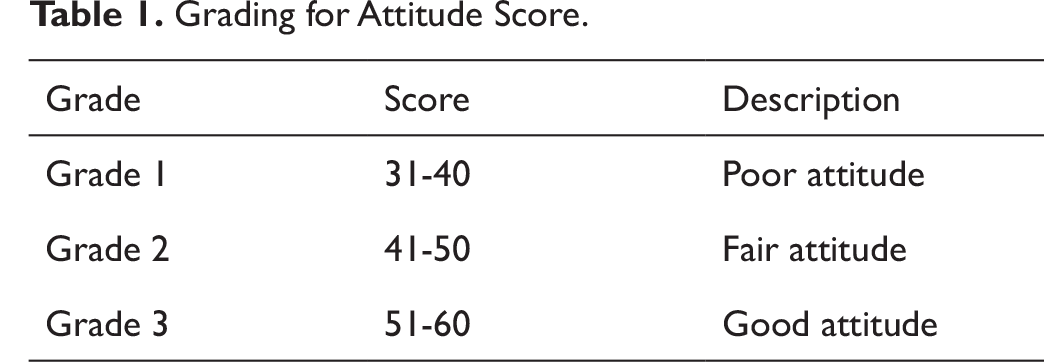
Date of birth, gender and general attitude of the patients were assessed by provided a set of questionnaires to the patients at the beginning of treatment. After the placement of the fixed orthodontic appliance, all patients were provided a set of postoperative instructions on maintenance of oral hygiene and appliance care, verbally and in writing. The second questionnaire was provided during the 6th month of treatment to assess the attitude of patients toward the treatment and also to assess whether the patient had really followed the instructions that were provided by the doctor at the start of treatment. The 6th month of treatment was chosen as, by that time, alignment would have been over and treatment would be in the retraction/space closure phase. After receiving the attitude scores, the patients were grouped into three grades (Table 1). A minimum score possible was 12 and a maximum score possible was 60 in each questionnaire.
Statistical Analysis
Data were entered in Microsoft Excel, and a statistical analysis was carried out with SPSS software version 16 (SPSS Inc., Chicago, IL, USA). Student t-test was used to compare mean and percentage failure of brackets between age and gender. Pearson correlation test was used to assess the correlation between bracket failure rates and attitude of patients. Confidence interval was set at 95%, power of the study at 80%, and probability of alpha error at 5%.
Results
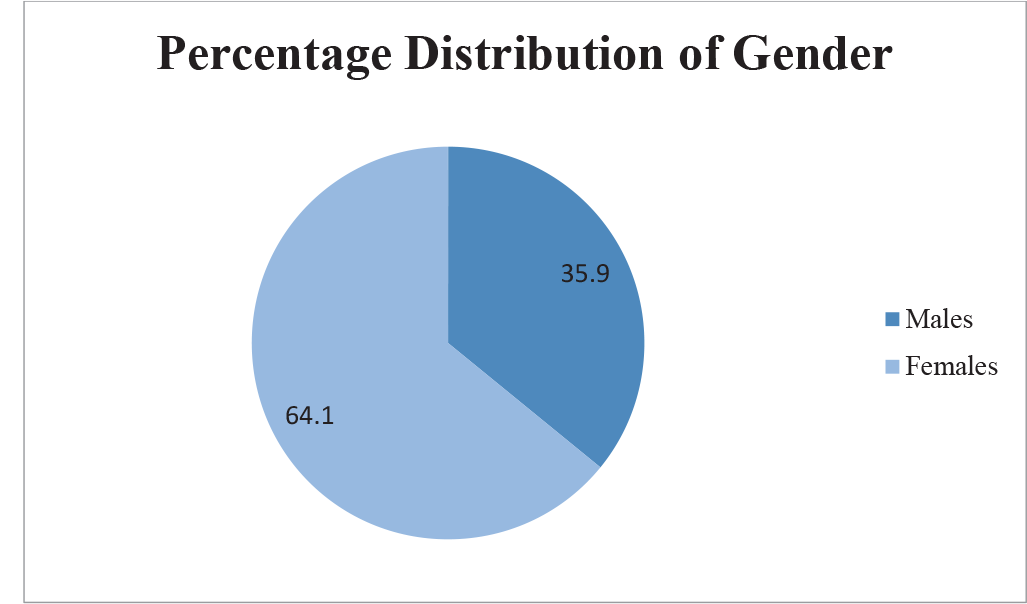
In the present study, a total of 128 patients having an age range of 12 to 25 years with a total of 2135 bonded attachments between them for their fixed orthodontic treatment were studied. Figures 1 and 3 show the age and gender distribution of the study sample.
Out of 2135 brackets bonded, 268 bracket failures were reported. The incidence of bracket failure in this study was found to be 12.55%, that is, 61% of patients reported with bracket failure. The incidence of anterior bracket failure was 5.6%, and posterior bracket failure was 29.2%.
Grading for Attitude Score.
Percentage Distribution of Gender.
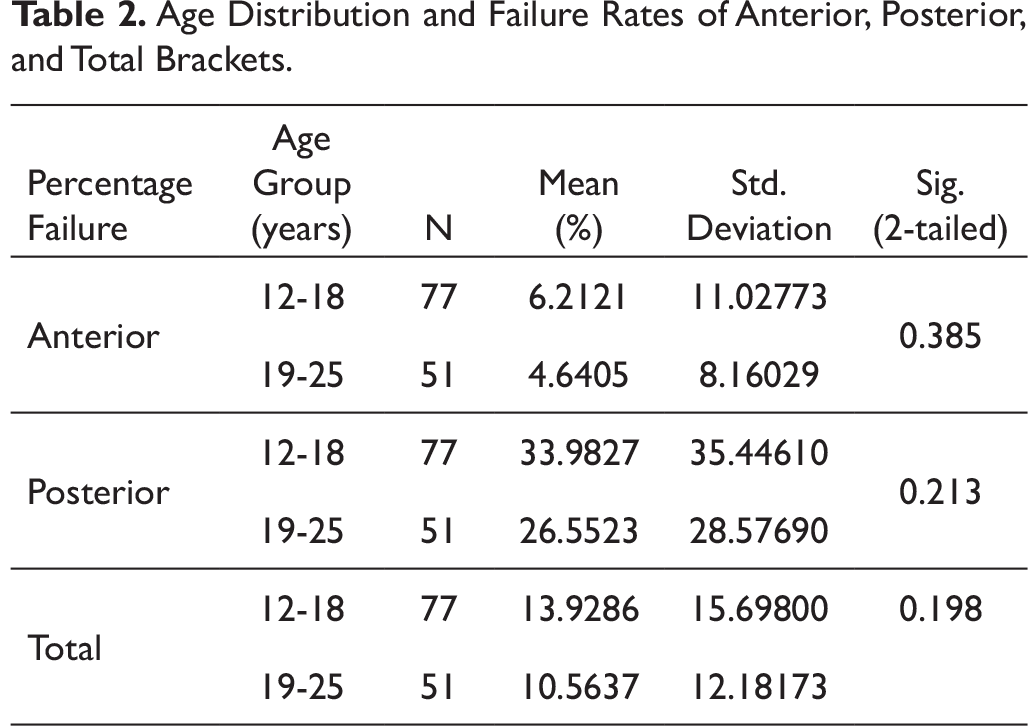
Age Distribution and Failure Rates of Anterior, Posterior, and Total Brackets.
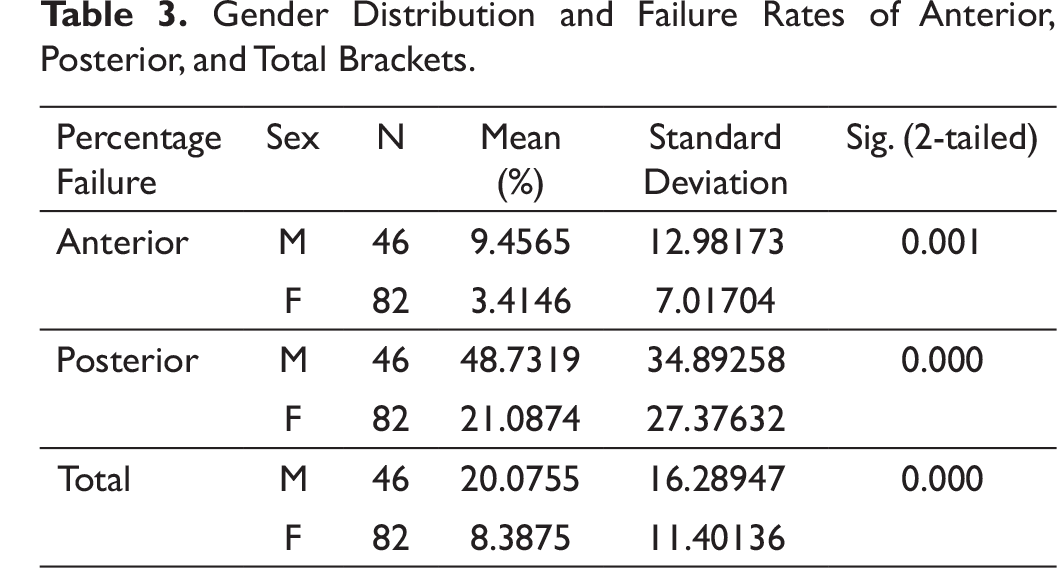
Gender Distribution and Failure Rates of Anterior, Posterior, and Total Brackets.
Frequency and Percentage Distribution of Patients with Poor, Fair, and Good Attitude.
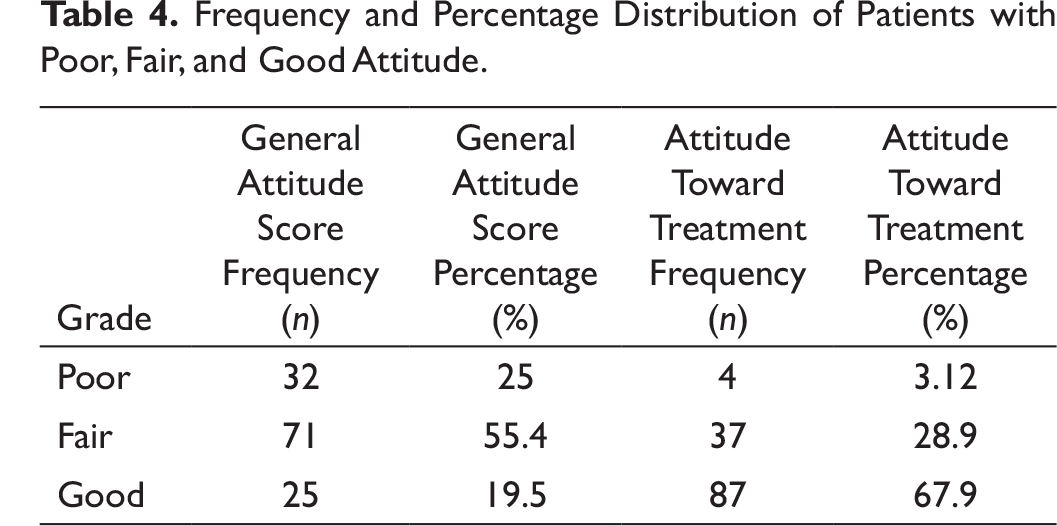
Table 3 shows the mean and standard deviation of percentage failure rates of anterior, posterior, and total brackets among males and females. In this study, it was found that there was a statistically significant difference between bracket failure rates and sex distribution; males had higher bracket failure rates (20%) when compared to females (8%) (P value < .001).
Mean Attitude scoring before treatment, signifying the general attitude of the patient, was found to be 45, and attitude scoring after 6 months of appliance placement was found to be 51 (Figures 4 and 5). Table 4 shows the frequency and percentage distribution of patients with poor, fair, and good attitude (general attitude and attitude toward treatment). It was observed that 19.5% of patients had good general attitude, and 25% of patients had poor general attitude. However, the 6-month mid-treatment evaluation revealed that 67.9% had good attitude toward treatment, and 3.12% of patients had poor attitude toward treatment.
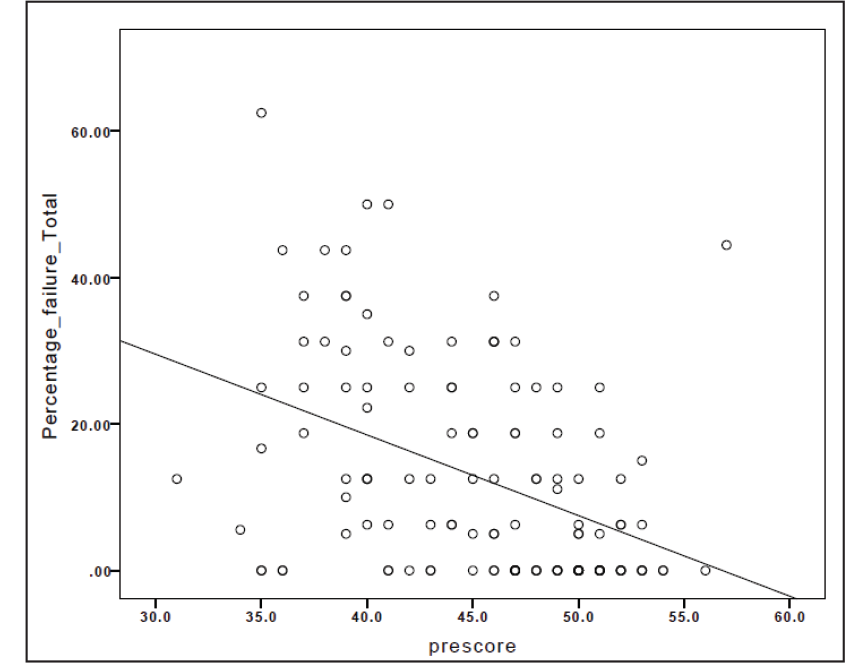
Statistically significant negative correlation was found between percentage of total number of failed brackets and pretreatment attitude scoring (P value < .000) as seen in Figure 6. A statistically significant (P value < .000) negative correlation between anterior and posterior bracket failure rates with pretreatment attitude scoring was observed, that is, as the attitude scoring increased, the bracket failure decreased and vice versa, or the patients who were considered having good attitude scoring had lesser debonding rates.
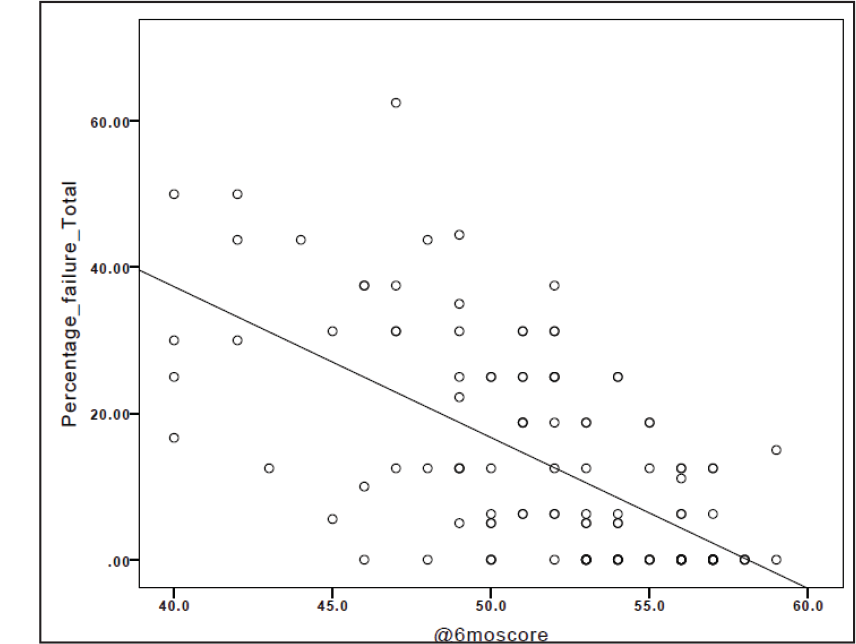
A statistically significant negative correlation was found between percentage failure rate of total number of brackets and mid-treatment attitude scoring (Figure 7) (P value < .000). Similarly, a statistically significant negative correlation was observed between percentage failure rates of anterior and posterior brackets with 6-month mid-treatment attitude scoring.
Pre-questionnaire Mean Statistics.
Mid-questionnaire Mean Statistics.
Moderate Negative Correlation Was Found Between Percentage of Total Number of Failed Brackets and Pretreatment Attitude Scoring.
Good Negative Correlation Between Percentage Failure Rate of Total Number of Brackets and Mid-treatment Attitude Scoring.
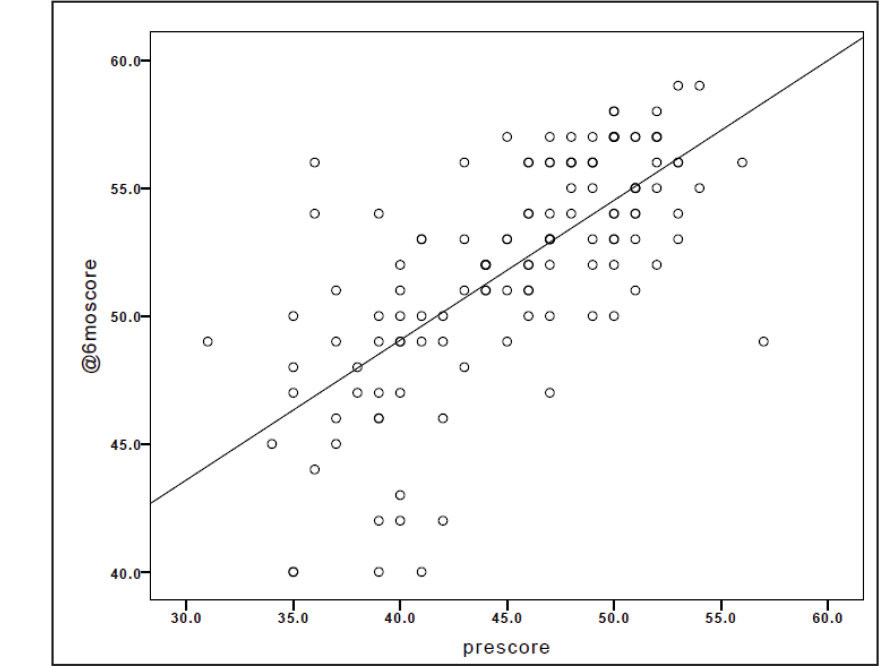
Correlation of the pretreatment and mid-treatment attitude scoring was carried out and was found to have statistically significant positive correlation between the two, signifying that the general attitude of the patient as well as the attitude toward orthodontic treatment were similar (Figure 8) (P value < .000).
Discussion
The incidence of bracket failure in the present study was found to be 12.55%. Literature reveals bracket failure rates ranging from 1.57% to 55.6%7,19-22 and can vary with age, gender, the particular tooth, side and location of the arch, and skeletal class. 23 A similar study was carried out by Aikins and Ututu, 4 where they found an incidence of 17.0%, which was lower than a study conducted by Moninuola et al 20 in South West Nigeria.
Good Positive Correlation Between Pretreatment and Mid-treatment Attitude Scoring
Bracket Failure and Age
In the present study, it was observed that the bracket failure rate between the adolescent and adult age groups was not statistically significant (P = .19). The bracket failure rate on the anterior and posterior teeth were assessed, and it was found that there was no actual difference in failure rate between the adolescent and adult groups (P = .385, P = .213). This was contrary to the findings of Ahangar and Shahamfar, 24 Bindayel et al, 25 and Bazargani et al, 26 who had reported that bracket failure incidence tended to decrease as the patients’ age increased. Al-Duliamy 5 observed similar results, in that a higher percentage of bond failure was found among younger-age patients. He attributed this to the fact that the younger age group, especially teenagers, took lesser care of their teeth and ate more sweets, which led to plaque accumulation and gingival inflammation, in turn, adversely affected the bonded bracket attachment.
Bracket Failure and Gender
The percentage failure rates of both anterior and posterior brackets were significantly higher for males. This result was supported by Adolfsson et al, 27 who explained that females were generally more careful than males, and that females tended to apply lighter masticatory forces. Aikins and Ututu 4 also reported that males had more bracket failure rate than females.
Bracket Failure Rate and Attitude of the Patients
A high level of motivation may decrease bracket failure.
Anxiety was reported before treatment in new dental patients and was found to be reduced, following the provision of an informative leaflet by Jackson and Lindsay. 28 However, in the study performed by Wright et al, 29 anxiety scores had fallen at 12 weeks, following commencement of fixed appliance therapy. These findings are in agreement with that of Sari et al, 30 who reported that patients undergoing orthodontic treatment for 12 months had lower anxiety levels than those about to begin the treatment. Lew 31 found that improvement in dentofacial appearance was the most important single factor motivating both patients and parents to seek orthodontic treatment.
In the present study, the scoring from the questionnaires revealed a statistically significant negative correlation between attitude (both pretreatment and 6-month mid treatment) and bracket failure rate (anterior, posterior and total) from which we can infer that patients with poor scoring for the attitude had a higher bracket failure rate and vice versa. A statistically significant positive correlation was observed between pretreatment attitude scoring and 6-month mid-treatment scoring from which one could infer that the patients’ general attitude and attitude toward orthodontic treatment were correlated.
In the final analysis of the data of this study, patient attitude and cooperation as observed in the pretreatment and mid-treatment attitude scoring showed that a lower scoring was observed in patients with greater bracket failure. Therefore, a positively motivated individual had lower bracket failure rate and vice versa. Satisfactory orthodontic treatment depends on the retention of brackets on the teeth for as long as the treatment is ongoing. Therefore, patients need to understand the importance of complying with instructions, and the orthodontist also should ensure that the bonding of brackets is carried out with adequate skill and expertise.
Conclusion
The incidence of bracket failure was found to be 12.55%.
Males had more bracket failure than females.
Age showed no significant relation with bracket failure rates.
A significant negative correlation was observed when comparing both general attitude and attitude toward treatment with the percentage failure of brackets—anterior, posterior, or total brackets. Therefore, a positively motivated individual had lower bracket failure rate and vice versa. A positive correlation was found between general attitude of the patient and attitude toward orthodontic treatment.
Footnotes
Acknowledgment
The authors would like to thank all the Staff and Post-graduate students, MES Dental College, Perinthalmanna and everyone involved in the compilation and analysis of data for the study. Kerala University of Health Sciences; MES Dental College, Perinthalmanna, Kerala.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.