
Abstract
The improvement of facial aesthetics is one of the main reasons why patients with a class II division 1 malocclusion seek orthodontic treatment. There are various techniques available to treat class II malocclusions, one of which is a two-phase approach that includes functional jaw orthopedics as well as fixed orthodontic treatment. The following case report describes the case of a 12-year-old growing female patient AK with a severe class II division 1 malocclusion. The patient was treated initially with Haas-type rapid maxillary expansion. Pre-functional orthodontics was followed with a removable twin block functional appliance and a combination pull headgear for growth modification and correction of her overjet and profile. Thereafter, a fixed, pre-adjusted MBT (McLaughlin Bennet Trevsi) prescription orthodontic appliance was utilized following the extractions of the maxillary first premolars and two lower incisors in the final phase, to ensure well-aligned arches and improved aesthetics and function.
Case Report (Indian Board of Orthodontics Examination)
Management of a skeletal class II malocclusion using multiphase treatment with maxillary expansion and a twin block appliance with a combination pull headgear, followed by extractions and fixed mechanotherapy.
Introduction
Class II division 1 malocclusion cases are complicated due to a skeletal discrepancy involving both the maxilla and the mandible. It can be the result of a retrusive mandible and/or a protrusive maxilla. 1 The most prevalent feature of this malocclusion in growing patients is the mandibular retrusion. 2 Treatment of skeletal class II cases depends on growth, age, compliance, and the severity of the malocclusion. 3
There are various ways to treat class II division 1 malocclusions, with treatment options including both removable and fixed appliances. Rapid maxillary expansion followed using a functional appliance is essential in cases with narrow arches with extreme crowding. There are alternative fixed options available, which include fixed class II correctors and fixed orthodontic treatment in conjunction with inter-arch elastics and/or extractions and/or skeletal anchorage and/or orthognathic surgery, depending on the severity of the case.
In patients with psychosocial problems due to compromised facial aesthetics and an enlarged overjet, a two-phase or early management approach can be followed, where the patient starts treatment in the late mixed dentition by making use of functional appliances, followed by a second phase where fixed appliances are used to finish the treatment in the permanent dentition. The use of the single-phase or late treatment is advocated in cases where the patient has finished growing and treatment only commences in the permanent dentition with the fixed appliance treatment. 4 Various types of functional appliances exist and are designed to alter the activity of the various muscle groups that influence the position and function of the mandible. By altering the vertical and sagittal positions of the mandible, the muscle forces can result in orthodontic and orthopedic changes in the dentition. 5
Pretreatment Assessment
AK, a 12-year-old female, came with a chief complaint of forwardly placed upper front teeth and presented with an Angle’s class II division 1 relation on a class II skeletal jaw base and normodivergent vertical relation. She had a convex profile with incompetent and everted lips and a positive VTO (visual treatment objective).
Diagnosis
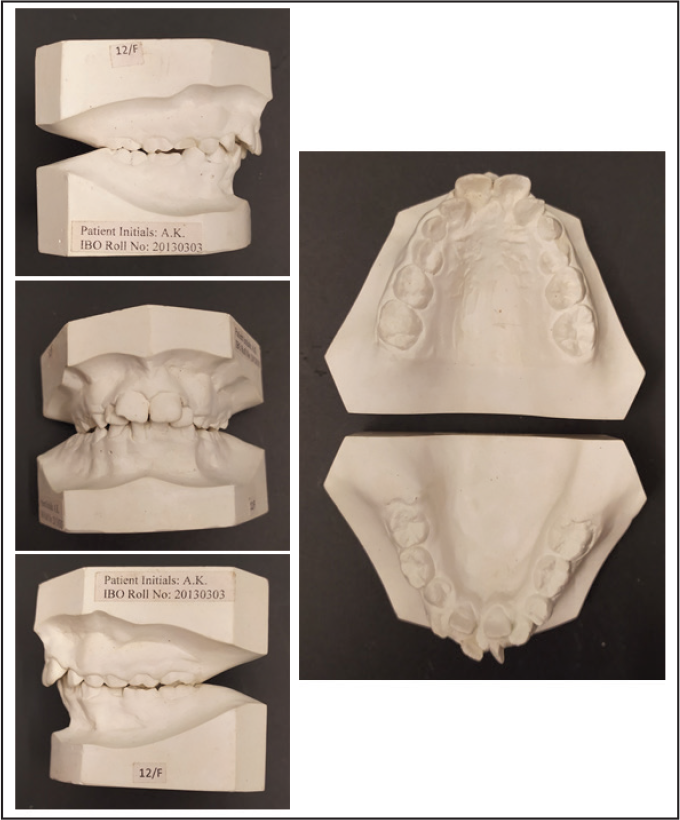
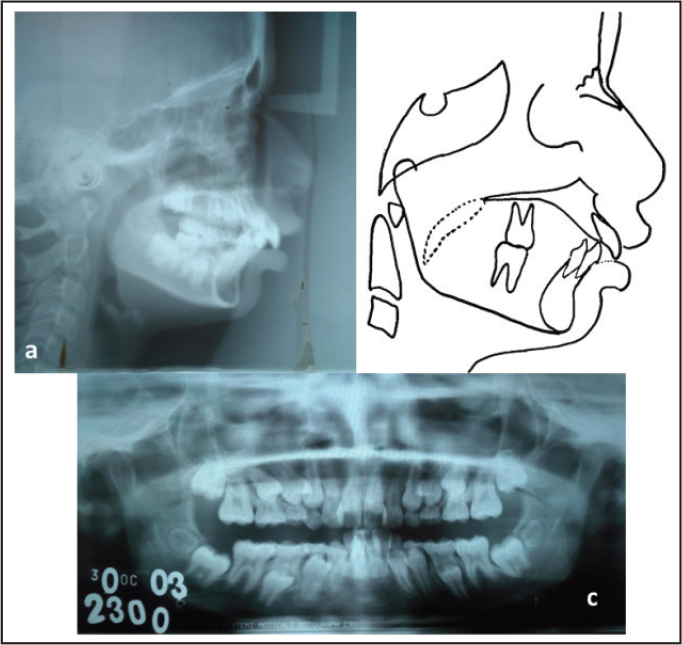
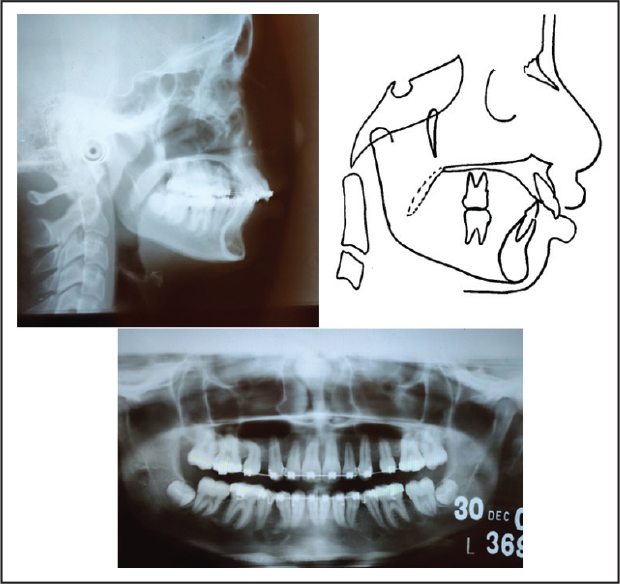
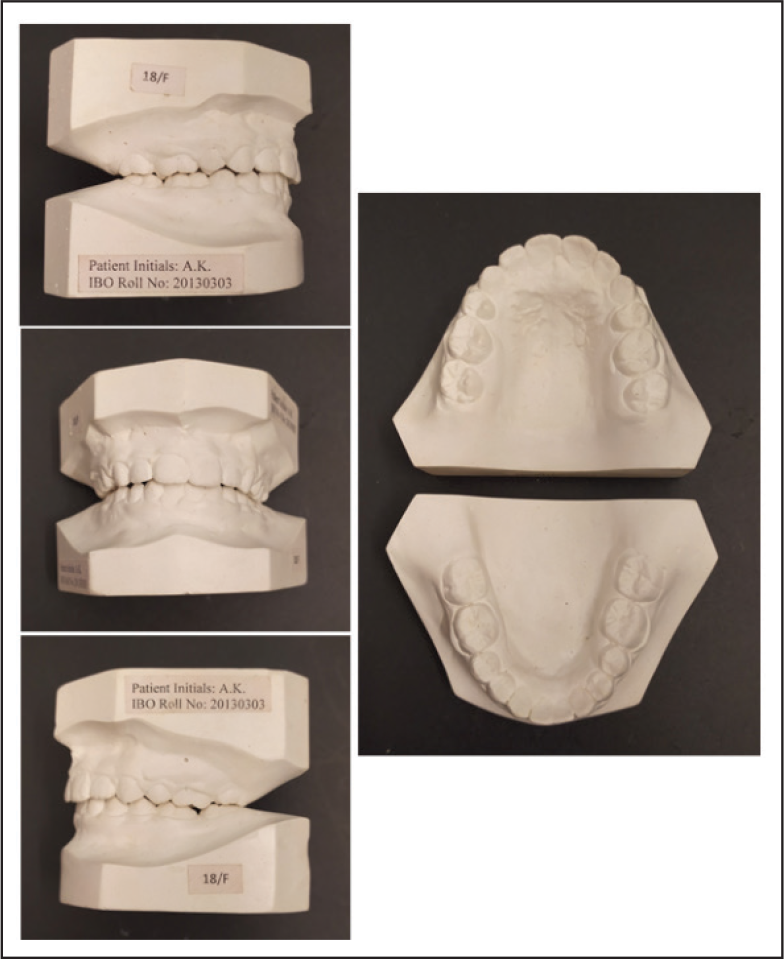
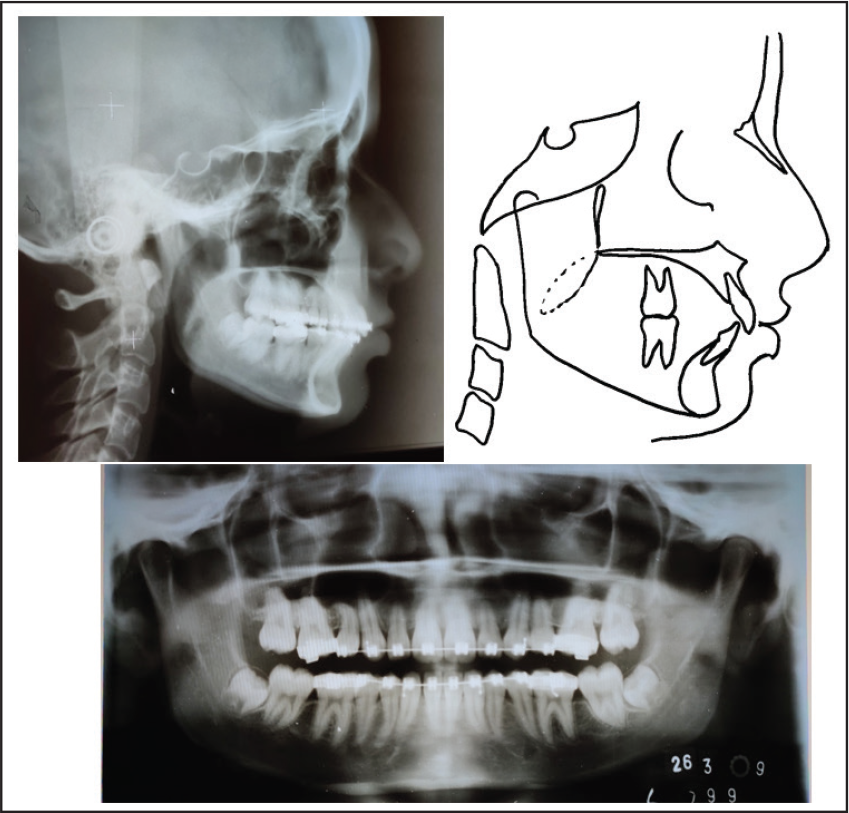
The 12-year-old female patient AK presented to the orthodontic clinic with a complaint that her teeth were sticking out and she was unhappy with her appearance. She was healthy, with no contributing medical history. The pretreatment extraoral clinical photographs (Figure 1) showed a convex lateral profile, with a potential lip trap and a class II division 1 incisor relationship. She had incompetent lips and an increased upper incisor show at rest. The pretreatment intraoral photographs (Figure 1) showed a severe maxillary protrusion with a large overjet and deep overbite dental arches. The pretreatment dental cast (Figure 2) showed crowding in the upper arch and the lower arch, a large overjet of 8 mm, and an overbite of 6 mm. She was in the mixed dentition stage, as shown in the panoramic radiograph (Figure 3[c]). Tanaka–Johnston mixed dentition analysis revealed adequate leeway space available in the upper arch and inadequate leeway space in the lower arch; an additional space of 3.5 mm was required on either side.
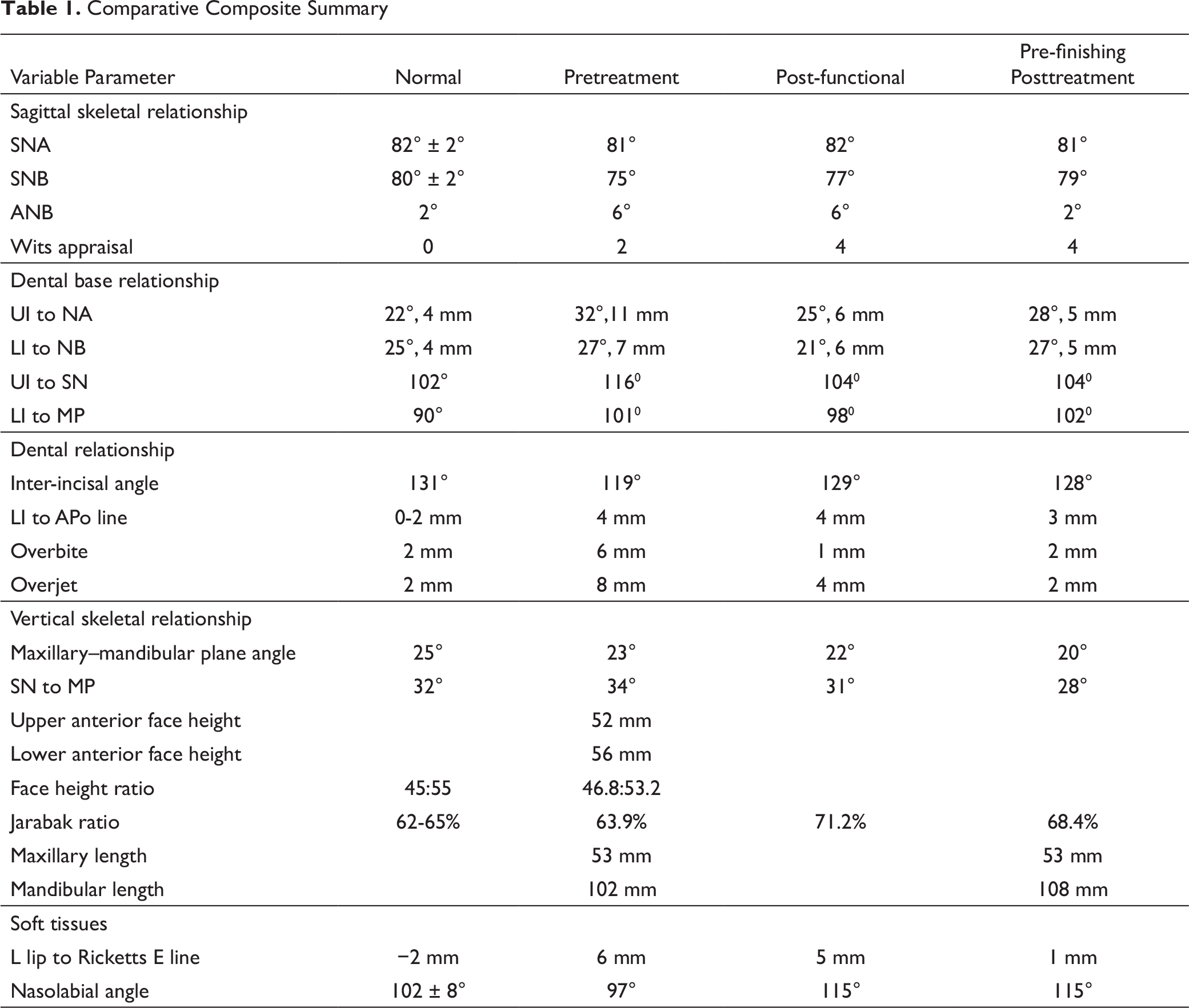
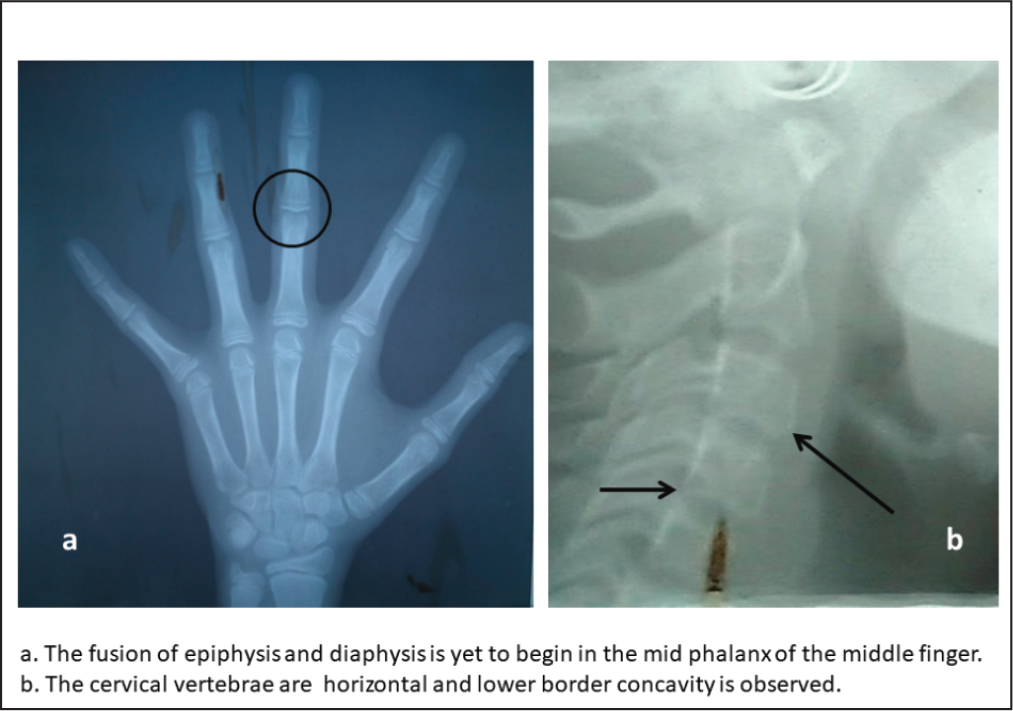
The pretreatment cephalometric radiograph (Figures 3[a] and [b]) and the analysis (Table 1) demonstrated a moderate skeletal type II (ANB [Anterior point on Maxilla Nasion Anterior point on Mandible] angle 6°). The SNA (Sella Nasion Anterior point on Maxilla) angle of 81° indicated an orthognathic maxilla compared with the cranial base, and the SNB (Sella Nasion Anterior point on Mandible) angle of 75° reflected a retrognathic mandible compared with the cranial base. Her MP-PP (Mandibular Plane Palatal Plane) angle of 23° revealed an acceptable vertical skeletal relationship. Regarding growth status, hand and wrist radiographs depicted that the patient was in the FG (Stages in Mid Phalanx evaluation) stage as per the third middle phalanx, and in the lateral cephalometric radiographs, the cervical vertebral maturation 6 demonstrated remaining skeletal growth in the CS3 (Cervical Maturity stage 3) stage, which indicated that a considerable amount of growth could be expected in the year following treatment (Figures 4[a] and [b]).
Pretreatment Extraoral and Intraoral Photographs

Pretreatment Models
Pretreatment Radiographs
Comparative Composite Summary
Skeletal Maturity Assessment With Wrist and Cervical Vertebrae Radiographs
The problem list indicated a marginally increased size of maxilla, decreased size of mandibular corpus, dorsal placement of condyle, Angle’s class II division 1 subdivision on the right side, proclined upper and lower anteriors, moderate crowding with upper anteriors and severe crowding with lower anteriors, increased overjet, deep bite, rotations, convex profile, acute nasolabial angle, potentially competent lips, lip trap, normal mentolabial sulcus, and a receding chin.
The treatment objectives to deal with the patient’s complaints were (a) to create a more balanced, aesthetic face by reducing the apparent intermaxillary anteroposterior discrepancy and reducing the patient’s convex facial profile with improved smile aesthetics; and (b) to achieve the ideal intermaxillary incisor overbite and overjet relationships, as well as to reduce the Curve of Spee through alignment and leveling of the teeth in both arches to establish good intercuspation.
Treatment Start and Progress
The following options based on functional/orthopedic/orthodontic camouflaging were presented to the patient:
Rapid maxillary expansion followed by pre-functional orthodontics; Twin block with high-pull headgear; and Extraction of the maxillary first bicuspids and mandibular incisors in the next stage for getting the space required.
This would require maximum posterior maxillary dentoalveolar anchorage combined with class II intermaxillary elastics correcting the excessive maxillary anterior overjet and leveling of the mandibular arch Curve of Spee.
Stage I
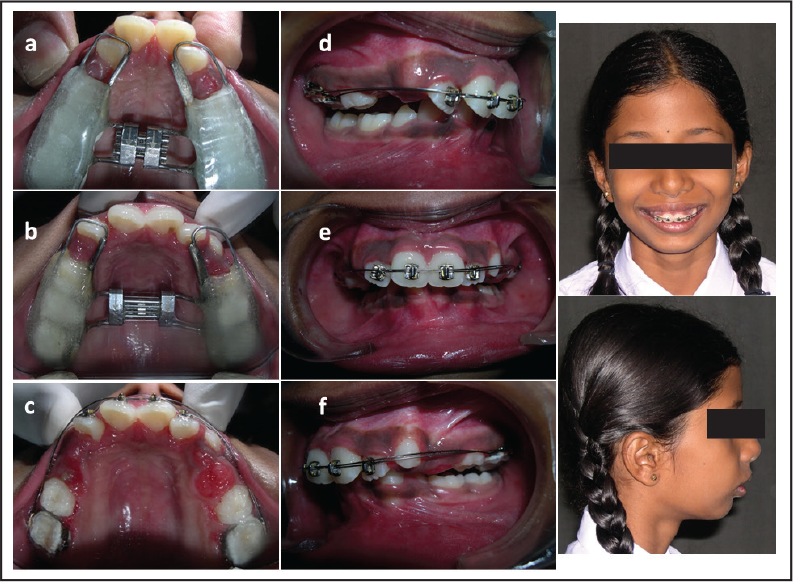
Maxillary expansion was conducted with a Haas type of appliance. The maxillary arch in most class II division 1 cases is constricted and requires expansion. This expansion is also necessary to ensure that bilateral posterior crossbites do not develop with the forward positioning of the mandible. The standard protocol of 180° in the morning and evening was followed by a holding phase for 3 months. (Figures 5[a] to [c]). Following the expansion, the maxillary incisors were aligned to facilitate mandibular advancement using a functional appliance. The pre-functional orthodontic correction was achieved with Mulligan’s 2 × 4 appliance using Begg brackets on the maxillary incisors and round tubes in the cemented molar bands. Simultaneously, a 0.014″ nickel–titanium (NiTi) archwire and 0.016″ stainless steel (SS) wire with a 30° anchor bend were employed to achieve the pre-functional correction (Figures 5[d] to [f]).
Stage II
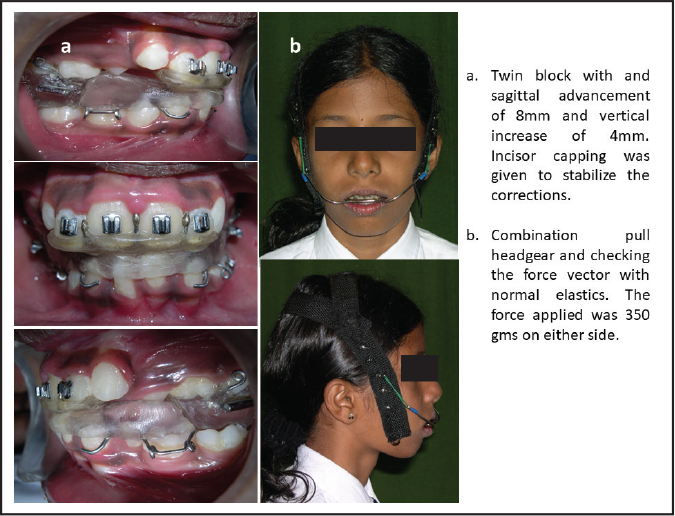
The initial placement of the twin block with the posturing of the mandible showed early improvement in the patient’s profile and appearance and motivated her to wear the appliance. There was soft-tissue strain present, with a large amount of posturing necessary to position the mandible better, when the appliance was first placed (Figure 6[a]). The amount of soft-tissue strain becomes normal after the initial twin block placement in a severe class II case with a severe overjet. The strain improves with the dentoalveolar retrusion of the maxillary and the protrusion of the mandibular anterior teeth throughout treatment. The lower component of Twin block appliance was incorporated with incisal coverage to inhibit any further proclination of the mandibular incisors. The combination pull headgear was employed to restrict the entire maxillary growth without affecting any rotations. The force applied was 350 g on either side, and the patient, with the force vector coinciding to pass along the ptergomaxillary fissure, was advised to change elastics every alternate day (Figure 6[b]). The patient was instructed to wear the twin block at all times and to only remove it in order to clean. The patient struggled with the twin block appliance at first but showed excellent compliance and persisted in wearing the appliance for the rest of the first phase of treatment. The total treatment time of the twin block was 12 months. The molar relation was corrected, and the facial aesthetics improved considerably. The overjet, the proclination of the upper incisors, and the crowding in the lower anteriors were the next problems to be addressed. After the cephalometric assessment and model analysis, an extraction plan was finalized to complete the treatment (Figure 7).
(a) Rapid Maxillary Expansion; (b) 2 × 4 Mulligan’s Pre-functional Orthodontics
Twin Block Appliance and Combination Pull Headgear
Post-functional Radiographs
Stage III
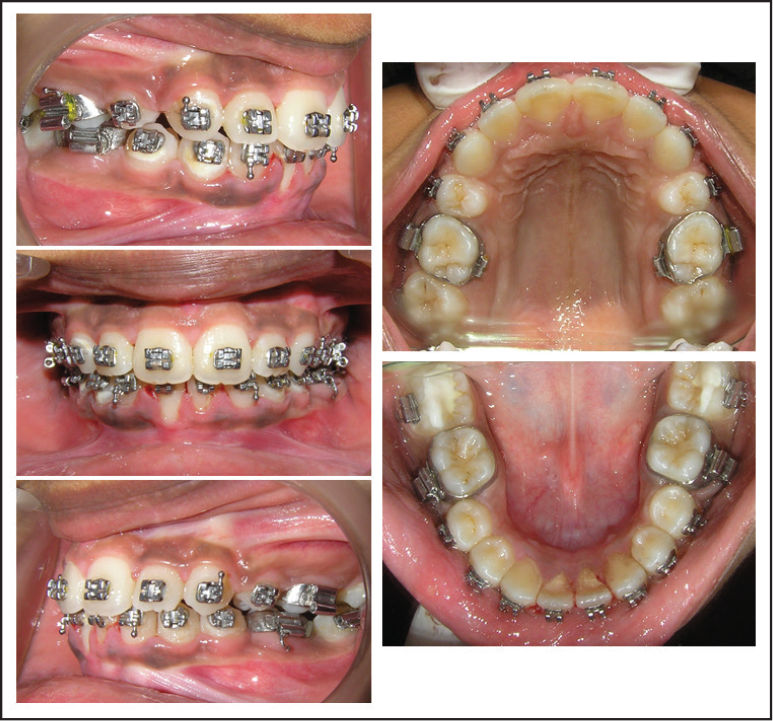
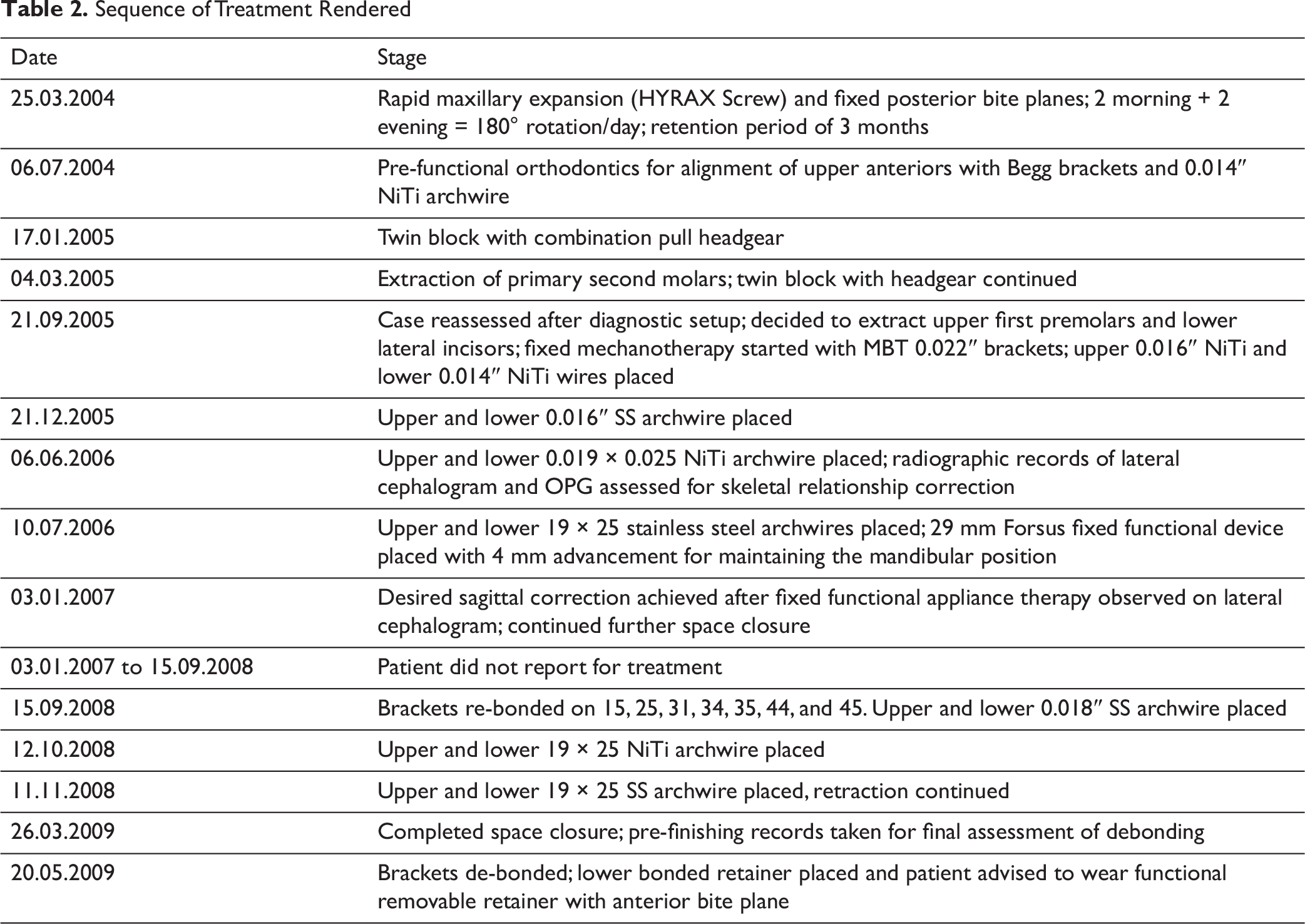
Fixed-appliance treatment was started after the removal of the Begg brackets followed by the extraction of the maxillary first bicuspids and mandibular lateral incisors. The MBT 0.022″-slot pre-adjusted orthodontic system was used to conduct the third phase of the treatment (Figure 8). Alignment was done using NiTi archwires, and the case was finished on SS and titanium molybdenum alloy (TMA) wires. The archwire sequences used are shown in Table 2. The final archwire for the lower arch was a 0.019″ × 0.025″ SS wire. A further increase in torque would have resulted in an even smaller interincisal angle with the already proclined lower incisors. Clinically, the torque of the maxillary incisors was evaluated and thought to be adequate. Inter-arch class II elastics were used during the second/fixed orthodontic phase of the treatment. The patient had a stable class I bite from the end of the first phase throughout the rest of the treatment. This proved that the correction seen after the first phase was not due to posturing and that a new occlusal relationship had been established that was stable and reproducible without any strain. Also, the elastics used were for settling the teeth in their new positions. This was done for the last 2 weeks prior to the removal of the braces. The sequence of wire changes is described in Table 2.
Pre-finishing Intraoral Photographs
Sequence of Treatment Rendered
Treatment Results
The posttreatment facial photographs showed an improvement in the facial profile (Figure 9). The intraoral dental casts and photographs (Figure 10) showed satisfactory dental alignment, bilateral class I canine relationships, and an ideal overjet and overbite. Good buccal interdigitation was achieved. Mandibular alignment was completed, and dental midlines had matched with the facial midline. Canine guidance was present on the left and right during lateral excursions, and incisal guidance was present on protrusion. There were no nonworking side interferences during functional movements. The cephalometric analysis between pretreatment and posttreatment cephalometric radiographs (Table 1) showed that sagittal skeletal relationship type II was changed to type I (ANB was reduced from 6° to 2°) and the maxillary incisors were retroclined and positioned backward (UI–NA was retracted from 32° and 11 mm to 28° and 5 mm; UI–SN was decreased from 116° to 104°). In terms of soft-tissue changes, an acceptable facial profile was achieved, and the nasolabial angle increased from 97° to 115°. These represented the changes from a skeletal class II pattern to a skeletal class I pattern. The Bolton ratio was a challenge that required interproximal reduction to match the canine relationship. A total reduction of 3.2 mm was required and equally done with 0.4 mm reductions on each side of the mandibular canine and premolar bilaterally.
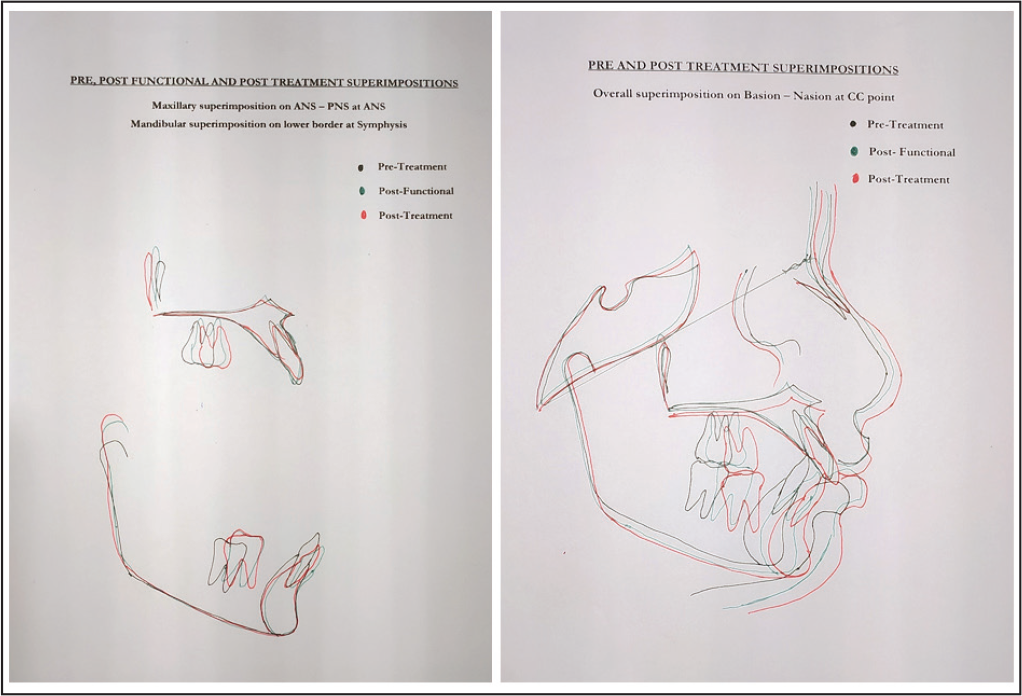
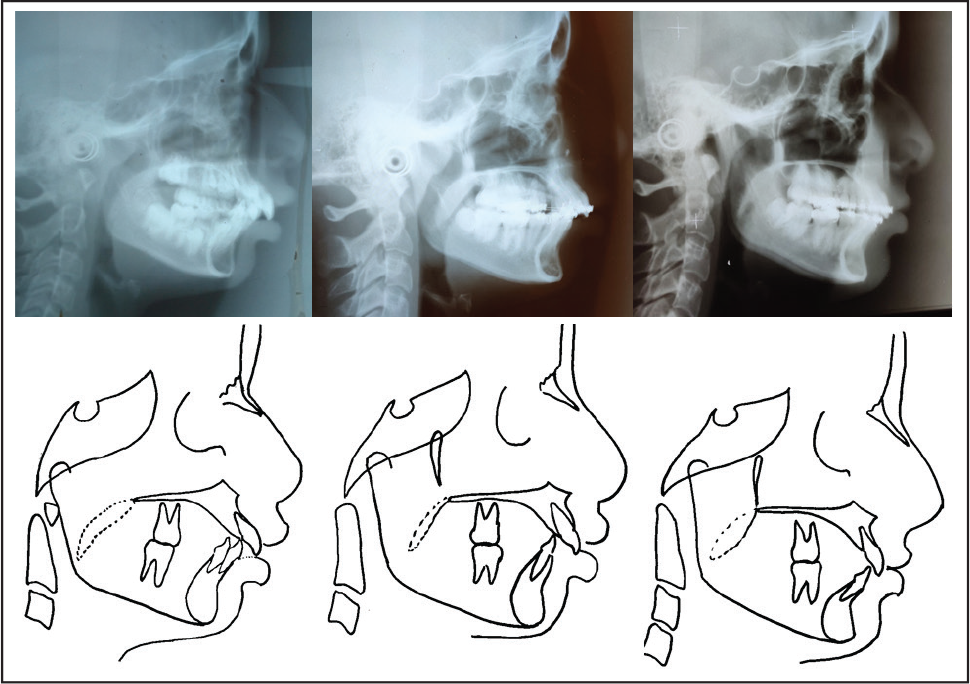
The pre-finishing panoramic radiograph (Figure 11) showed that all extraction spaces were closed, and the roots had been paralleled. The pre-finishing intraoral photographs revealed all the minor corrections needed to finish the treatment ideally (Figure 8). The fixed orthodontic treatment time was 2 years and 6 months. Upper and lower wraparound retainers were used to maintain alignment. The retention period was designed for 1 year full-time and then gradually decreased. Lateral cephalometric superimposition (Figure 12) showed intrusion of the upper and lower anterior teeth and extrusion of the lower posterior teeth, as well as correction of the Curve of Spee. Retraction of the upper anterior teeth corrected the protrusion of the maxillary anterior teeth. The facial convexity and upper lip protrusion were reduced. The nasolabial angle was more obtuse. There was harmonization of the upper and lower lips and an improvement in lip incompetence. Maxillary superimposition of the pretreatment and posttreatment cephalometric radiographs (Figure 12) along the palatal plane registered on the best fit of internal palatal structure, lingual contour of the oral part of the palate, and at the pterygomaxillary fissure revealed a movement of 3 mm at the A point in results from the treatment effect of the change in upper-anterior-teeth inclination. The upper first molars were moved forward by 2 mm. The upper incisors were tipped palatally and intruded as the incisal edge moved backward by 7 mm.
Posttreatment Photographs

Posttreatment Models
Pre-finishing Radiographs
Superimpositions
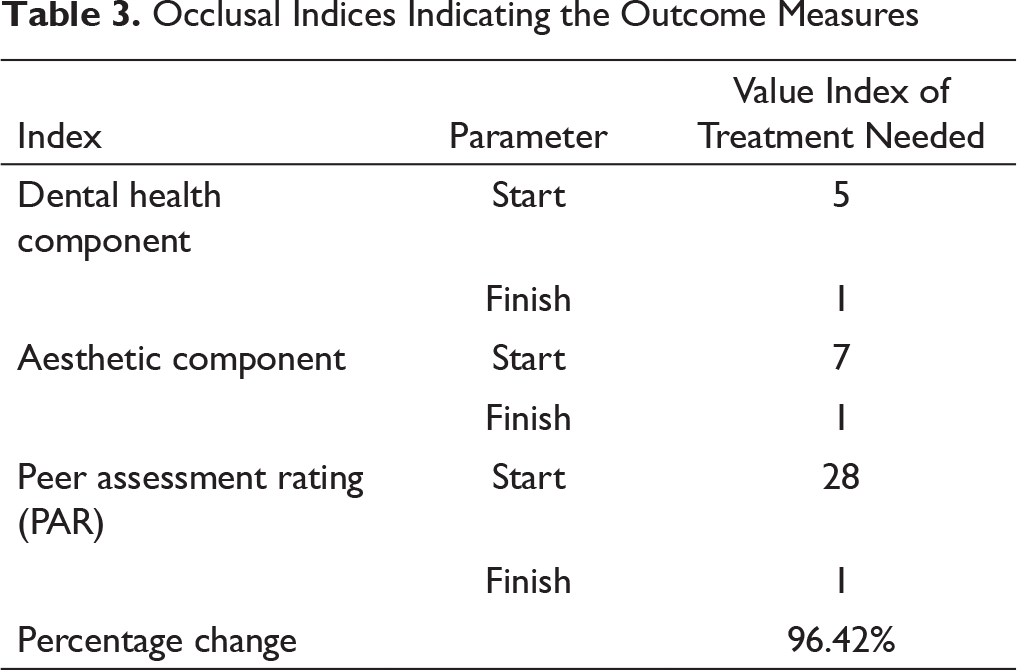
Occlusal Indices Indicating the Outcome Measures
Discussion
If the class II problem was due to protrusive upper anterior teeth, the treatment had to be focused on upper anterior teeth retraction, with or without extractions. If, the problem was deemed to be largely due to mandibular retrusion, the treatment was chosen with the aim to advance the mandible by functional appliance and facilitating the mandibular symphyseal prominence.
A satisfactory outcome could be expected with still-growing patients through adopting a camouflage approach with upper first bicuspid extractions. The changes observed in the occlusal indices are presented in Table 3.
Conclusion
This case report describes the case of a 12-year-old female patient who presented with a convex lateral profile, a class II division 1 incisor relationship, and skeletal type II with orthognathic maxilla and retrognathic mandible. The treatment achieved the patient’s profile and aesthetic goals regarding the nasolabial angle, lip posture, and perioral protrusion, as well as intraoral normal overjet and overbite with adequate interdigitation of canine and molar relationships. The entire treatment lasted for 4 years and 6 months, and occlusion was effectively improved with good posttreatment stability. The treatment resulted in a well-balanced and aesthetically pleasing profile as depicted in the comparative photographs and radiographs (Figures 13 and 14).
Critical Appraisal
The challenge in this case was the age of the patient. The severity of malocclusion and the amount of growth remaining were the factors considered in treating this case. The initial decision to use rapid maxillary expansion to relieve crowding was insufficient due to the severity. Sufficient expansion was achieved for the canines to erupt. The post-expansion phase was still in mixed dentition, and hence the case was treated with a twin block and combination pull headgear.
Stagewise Comparative Radiographs
Stagewise Comparative Facial Photographs

After 2 years of active treatment, the changes were minimal and the protrusion of the upper jaw persisted. The diagnostic setup revealed that extractions were essential, and hence the lower laterals were extracted to reduce the torqueing requirement in the later stages of the treatment.
The extended length of the treatment plan was a hindrance for the family, which was transferred to another city. The patient was unable to keep the appointments for more than a year. The appearance of the orthodontic scars and white spot lesions in the lower right buccal region were always serious concerns.
The maxillary anteriors experienced root resorption. This external apical root resorption amounting from 2 mm to less than one-third of the original root length could have been reduced if lighter and continuous force levels and/or segmental mechanics were used. Nevertheless, for en masse anterior intrusion, about 75 g of force was used. 7
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.