
Abstract
Aims and Objectives:
To evaluate the influence of the two adhesion boosters (assure universal bonding resin and enhance adhesion booster) on the shear bond strengths of indirectly bonded lingual brackets.
Materials and Methods:
A total of 120 extracted human teeth were randomly divided into 3 groups (n = 40), each group contained equal number of anterior and posterior teeth (anterior = 20, posterior = 20), and their lingual surfaces were etched by using 37% phosphoric acid. The bracket was bonded indirectly without using adhesion booster in group 1 (control group). In group 2, the adhesion booster A (enhance adhesion booster) and adhesion booster B (assure universal bonding resin) in group 3 were applied, respectively, before the bonding. The universal testing machine was used to measure the maximum bond strength. Student’s t-test followed by the one-way analysis of variance was used to compare shear bond strength among the groups.
Results:
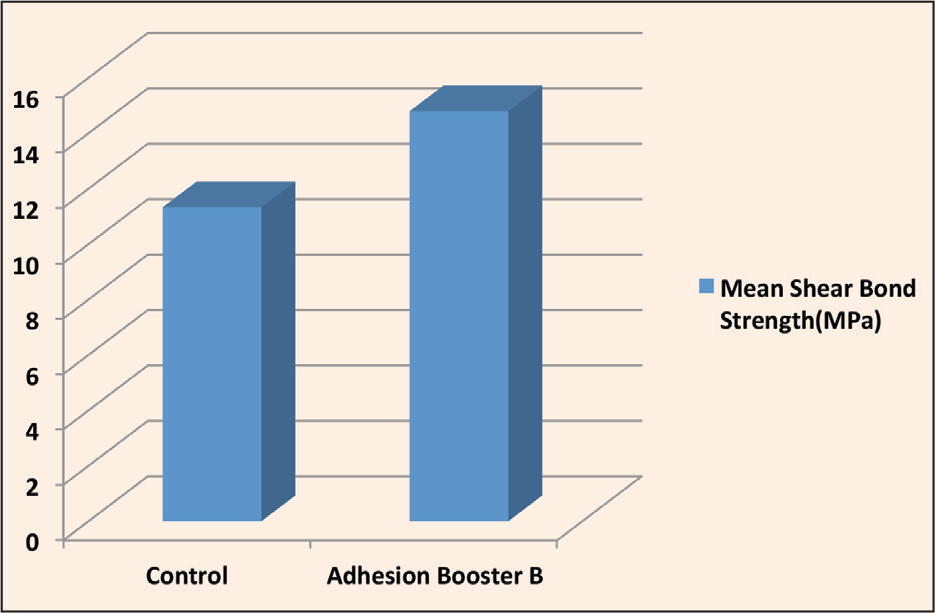
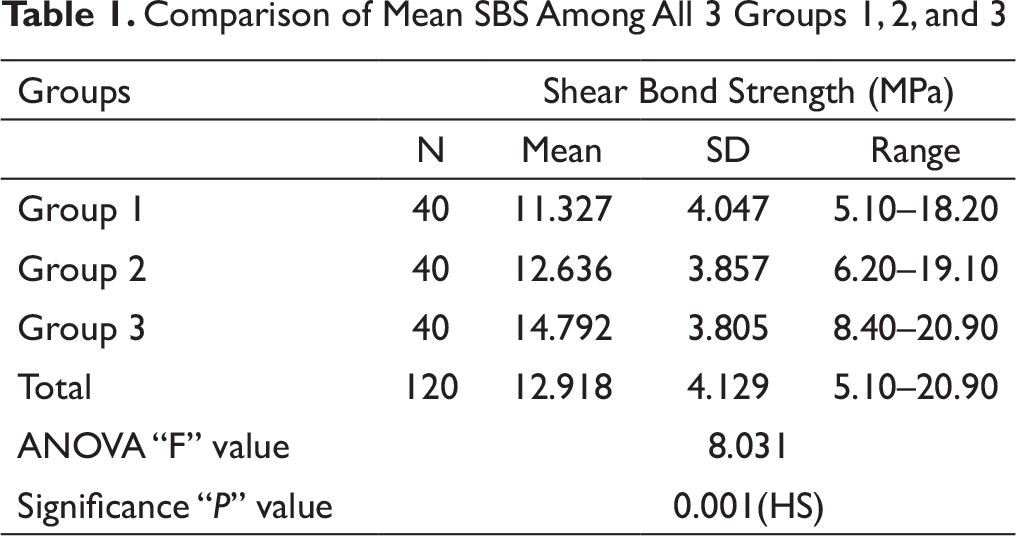
The shear bond strength was found to be highest in group 3, followed by group 2, and it was least in controls. There were highly significant differences statistically in shear bond strength among the groups 1, 2, and 3 (P = .001).
Conclusion:
Shear bond strength was admissible in all the groups. The application of the assure universal bonding resin significantly increased the bond strength of lingual brackets in indirect bonding.
Introduction
In recent years, due to rise in the esthetic expectations by the patients, there has been a growing demand for lingual orthodontic appliances. Increasingly, adult patients are seeking orthodontic treatment, and many of them are unwilling to wear the labial appliance, which is immediately visible. Hence, lingual appliance is the invisible treatment protocol and has become an obvious choice for these patients.
Lingual orthodontics, apart from offering the esthetic benefits, also provide several mechanical advantages over the conventional labial mechanics, such as the active intrusive forces on the anterior dentition, bodily movement of the tooth, distal tipping during molar distalizations, and remarkable dentoalveolar expansions. Since its inception in the 1970s, great advances have been made in this modality. 1
The benefits of the successful orthodontic treatment are well known today. While the esthetic is the common motivator to seek the orthodontic therapy, a harmonious smile is often accompanied with the achievement of good relationship between the hard and the soft tissues. The efficiency of obtaining treatment goals depends on how well a clinician controls the tooth movement during the treatment.
Among various types of the appliance used, the brackets are currently the most utilized and most recognizable features of the orthodontic treatment. When brackets lose their attachment from the tooth structures during the treatment, the clinician does not have control over the tooth movement, and the reattachment of the brackets is often necessary. It is often difficult to obtain efficient results if such interruptions take place in the course of the treatment. Thus, there is always a need for a standard bonding system, which can prevent or reduce the frequency of bond failure during the course of treatment paving the way to achieve planned and efficient treatment results.
For the past 60 years, after the introduction of the acid-etching technique by Buonocor2, 3 in 1955, major improvements have been achieved in bonding bracket to the teeth. In 1964, Newman4, 5 first tried to bond orthodontic brackets to the teeth using the acid-etching technique and an epoxy-derived resin. Weisser 6 and Silverman et al, 7 in 1973, used acid etching and BisGMA resin for direct bonding of orthodontic brackets.
The indirect-bonding method was first introduced in 1974 by Silverman and Cohen. 8 The adhesive used to attach the plastic brackets to the cast models in the laboratory was methyl methacrylate. Between the previously placed adhesive and etched enamel, an adhesive layer of an unfilled BisGMA resin was used.
In 1979, Thomas introduced a simple and efficient way of bonding the brackets indirectly to the tooth surface. 9 In this technique, the laboratory procedure involved the placement of a filled BisGMA resin on bracket base. After hardening of bracket with filled resin, a flexible transfer tray was used to carry the bracket to the mouth. For bonding the bracket, the bracket base was applied with a base resin and the etched enamel surface was applied with a liquid catalyst resin. The tray was removed when the polymerization was completed.
The Advantages of the Indirect Bonding
There are some significant advantages to the indirect bonding9-14:
accurate bracket positioning; reduced chair-side time; avoiding bands on the posterior teeth; no need for separator; enhanced ability to bond posterior teeth; and enhanced patient comfort and hygiene.
In Orthodontics, bond failure occurs at 4.7% to 6.0% for a variety of reasons such as poor operator technique, moisture contamination, and excessive masticatory forces. 15 It has been suggested that values between 5.9 Mpa and 9.7 MPa of the shear Bond strength (SBS) are sufficient for the effective bonding clinically. 16 When bonding is performed in uncontrolled humidity or on irregular enamel surfaces such as deciduous teeth, hypocalcified enamel, and fluoridated enamel surfaces, the frequency of bond failure is increased.
To decrease the bond failure rates, there have been many strategies, including the new innovation in bracket base designs, new adhesive materials, sandblasting techniques, and enamel-etching procedures. A relatively new method to enhance the bond strength of orthodontic brackets is the use of adhesion boosters, which was developed to reduce the bond failure rate. They incorporated hydrophilic monomers and other adhesion enhancers into the primer. 17 The addition of hydrophilic monomer to the adhesive systems facilitates the resin infiltrations into the etched enamel; this reduces the interfacial porosity and the adhesive defects, hence, resulting in the better bond strength after the polymerization. 18
Several studies have been carried out on the effects of the adhesion booster on the direct bracket bonding technique and the rebonding.17-23 Some studies have showed an increase in SBS, and others found no differences.
However, the effects of these products on indirect bracket bonding with lingual brackets have not been studied. Therefore, this study was carried out to evaluate the effects of two adhesion boosters (assure universal bonding resin and enhance adhesion booster) on the SBS of lingual brackets in indirect bonding.
Materials and Methods
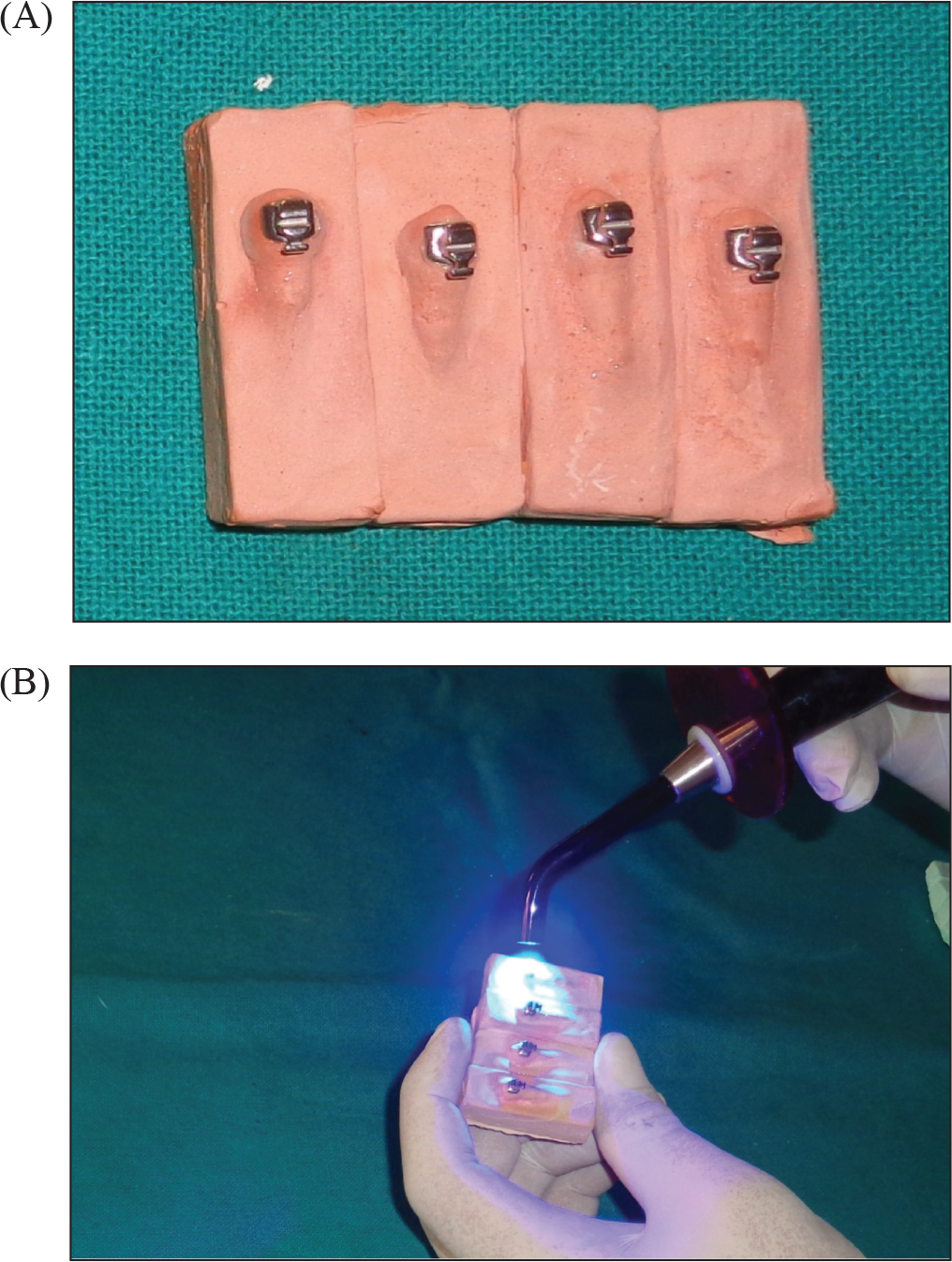
A total of 120 extracted human teeth, free of caries, wear, fracture, or any other visible defects, were selected and stored in distilled water until the beginning of the experiment. To prepare specimens, the teeth were mounted using the chemically cured resin, so that lingual/palatal surface was above the acrylic and was placed parallel to the base. Impressions of the specimen were taken using condensation silicone, and types III and IV dental plasters were poured. The plaster models were left to dry for 24 hours. A layer of insulating agent, that was diluted with water at 1:1 ratio, was applied to the model, and was allowed to dry for 20 minutes. Next, the base of the lingual bracket was sandblasted for 1 second with the compressed air jet and 50 µm aluminum oxide. A small amount of light-cure resin was applied to the metal mesh of the brackets before placing at the center of the lingual/palatal surfaces of the teeth model. The excess material was then removed with a scaler. The bracket was then light-cured for 40 seconds (10 seconds per side) at a distance of 2 to 3 mm with a light-emitting diode lamp and at a light intensity of 1300 to 1600 mw/cm 2 (Figure 1).
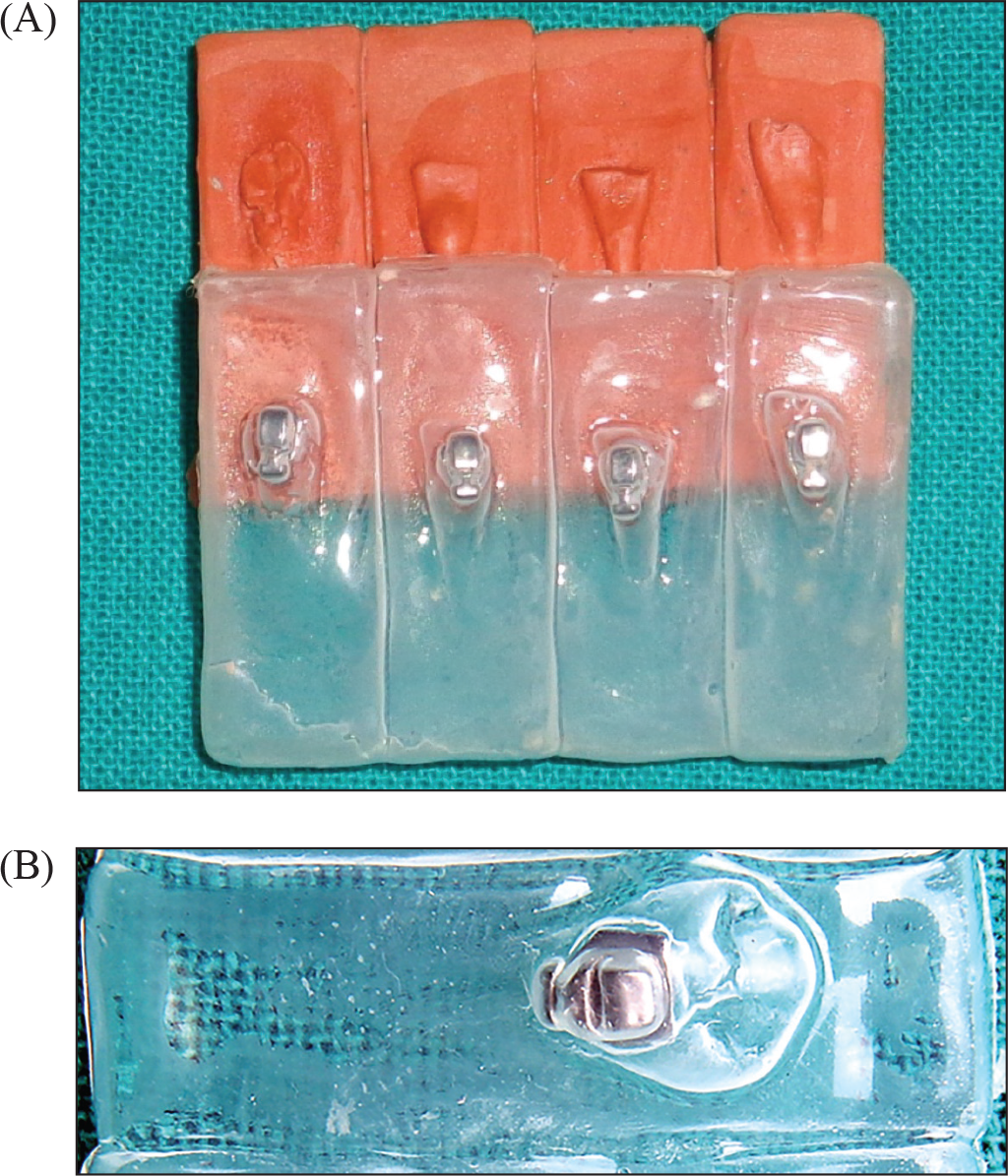
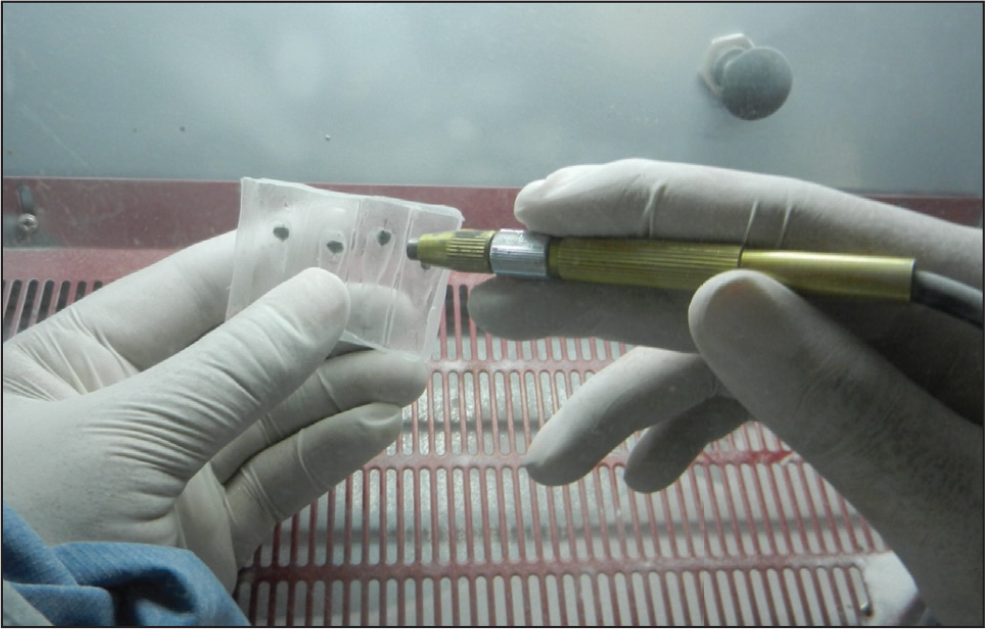
Thermoplastic resin with 1 mm thickness was used to prepare transfer trays in vacuum-forming machine (Figure 2). The transfer trays were then trimmed 3 mm below the upper margin of the models and placed in water for 30 minutes (Figure 3). The trays were then removed from the models (Figure 4), and the custom resin base were photopolymerized for 20 seconds. This custom resin base produced clinically effective torque in lingual brackets. Following this, the custom bases were sandblasted for 1 second to remove possible remnants (Figure 5). Enamel cleaning was carried out using a rubber cup and pumice powder. Immediately after this, enamel conditioning was carried out with 37% phosphoric acid for 30 seconds, rinsed with water, and dried with compressed air until the enamel acquired a chalky white appearance.
(A and B) Bracket Placement on Models and Curing With Light-Emitting Diode Lamp
(A and B) Transfer Tray Fabrication With Vacuum-Forming Machine

Immersion in Water

The specimens were divided into 3 equal groups randomly, each group containing equal number of anterior and posterior (anterior = 20, posterior = 20), and a different bonding protocol was used for each group.
Group 1 (control): Indirect bonding of brackets was carried out using the Transbond XT adhesive and the 3M Unitek primer according to the manufacturer’s instructions. The transfer tray was positioned in the teeth, slightly pressed, and light-cured for 40 seconds (10 seconds per side) at a distance of 2 to 3 mm with light-emitting diode lamp. The transfer trays were then carefully removed.
Group 2: Two layers of the adhesion booster A (enhance adhesion booster: Reliance orthodontic Product Inc, Itasca, IL, USA ) were applied to the enamel, and one layer was applied to the custom base, followed by a brief application of the compressed air. After 60 seconds, the brackets were bonded using the Transbond XT adhesive, as in the control group.
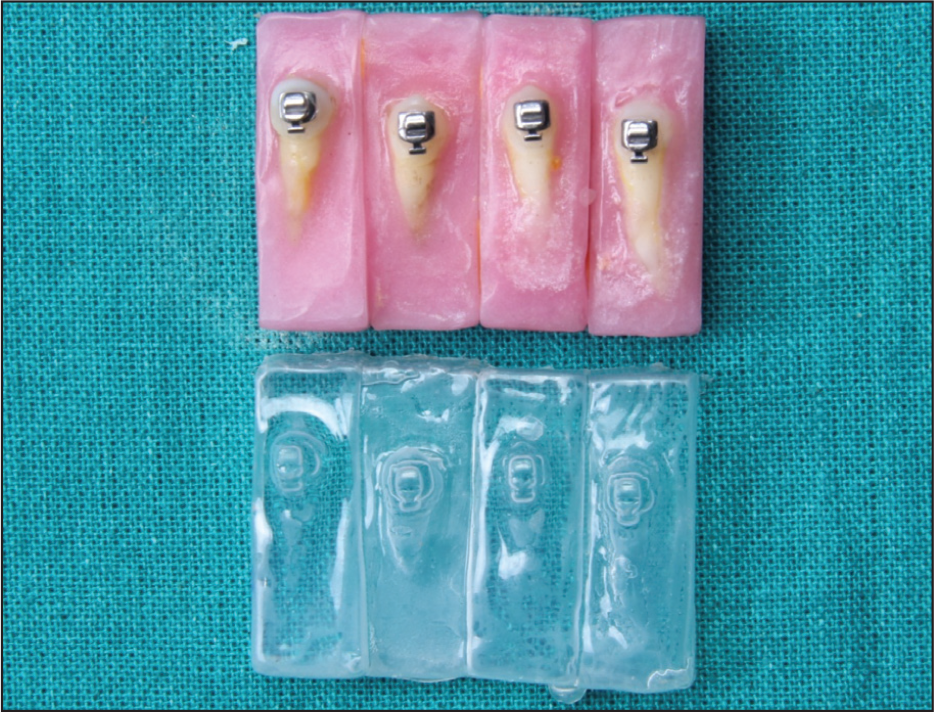
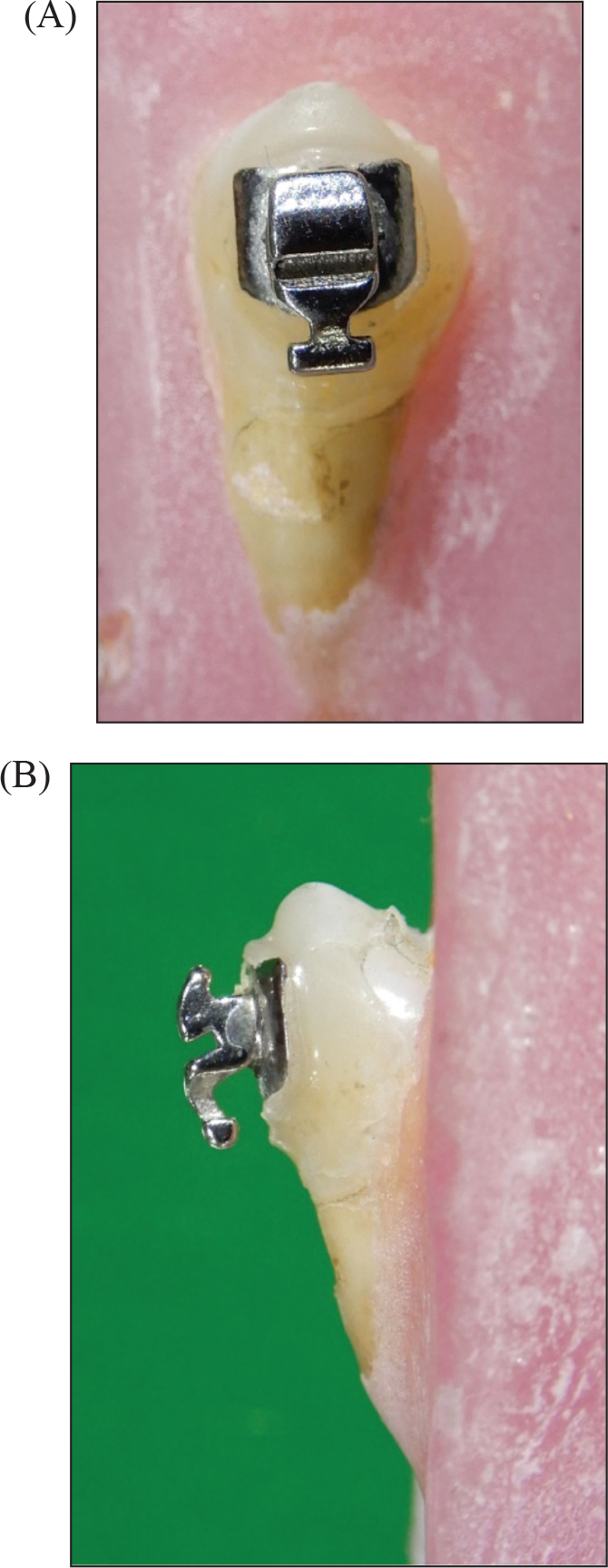
Group 3: Two layers of the adhesion booster B (assure universal bonding resin: Reliance orthodontic Product Inc, Itasca, IL, USA) were applied to the enamel, and one layer was applied to the custom base, followed by the application of the compressed air. After 60 seconds, the brackets were bonded using the Transbond XT adhesive, as in the control group (Figures 6 and 7).
(A and B) Removal of Transfer Tray
Sandblasting
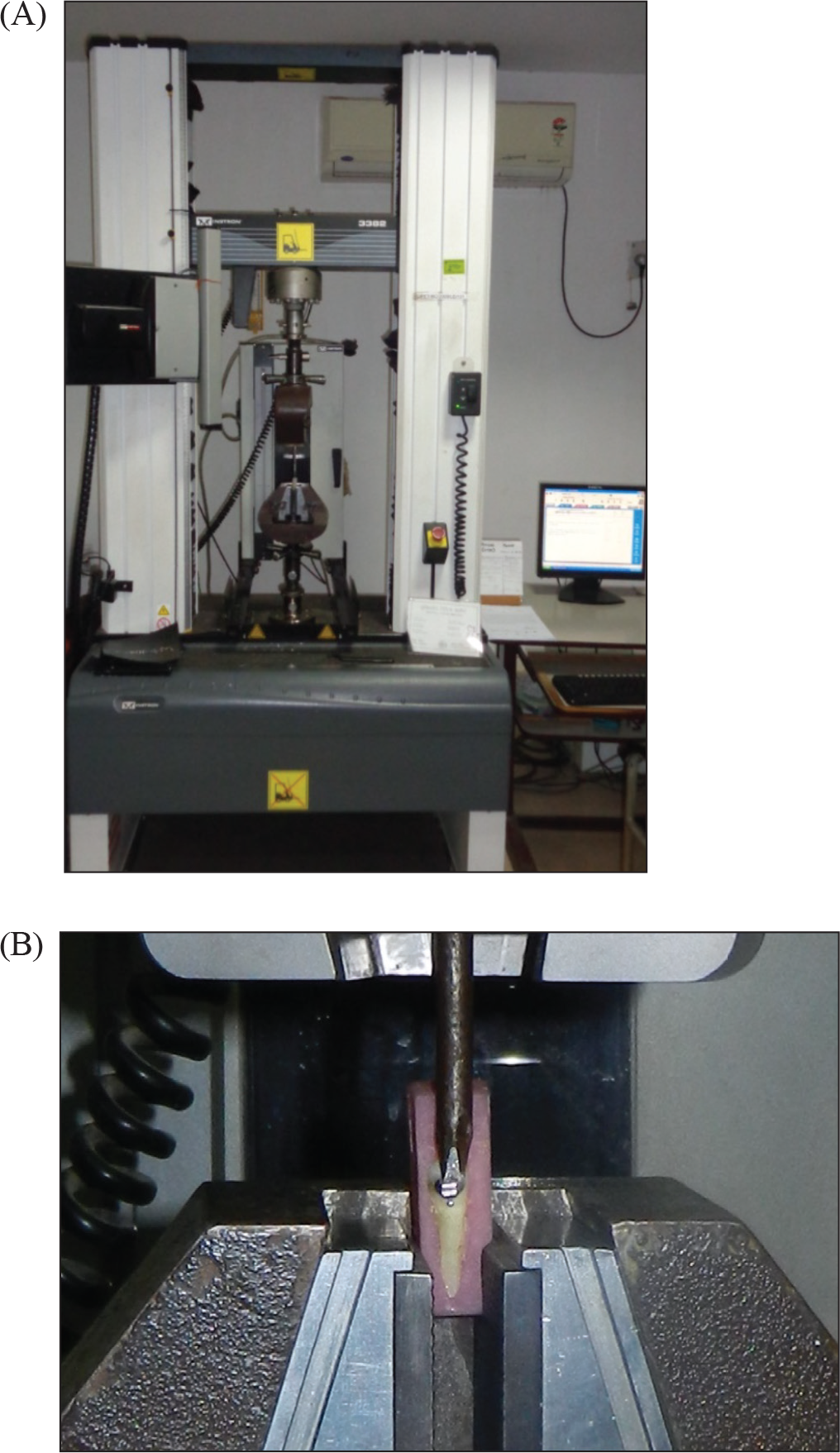
After bonding, the teeth were stored in distilled water at room temperature for the next 24 h. Then the specimens underwent a thermocycling procedure, involving 500 cycles, at 5°C and 55°C to simulate the oral environment. All specimens were sent for SBS testing. A mechanical testing machine was used to evaluate the shear strength of the brackets with a 1 kN load and 0.5 mm/min speed (Figure 8). The chisel was placed at tooth/bracket base interface in such a way that the force applied was parallel to the bracket base. The SBS in megapascals (MPa) was estimated by using the following formula: SBS (MPa) = force (N)/area of the bracket base.
Transfer of Brackets and Bonding
(A and B) Frontal and Lateral View of Bonded Lingual Bracket
(A and B) Debonding Setup of Universal Testing Machine
Comparison of Mean SBS Among All 3 Groups 1, 2, and 3
Comparison of Mean SBS Among Groups 1 and 2
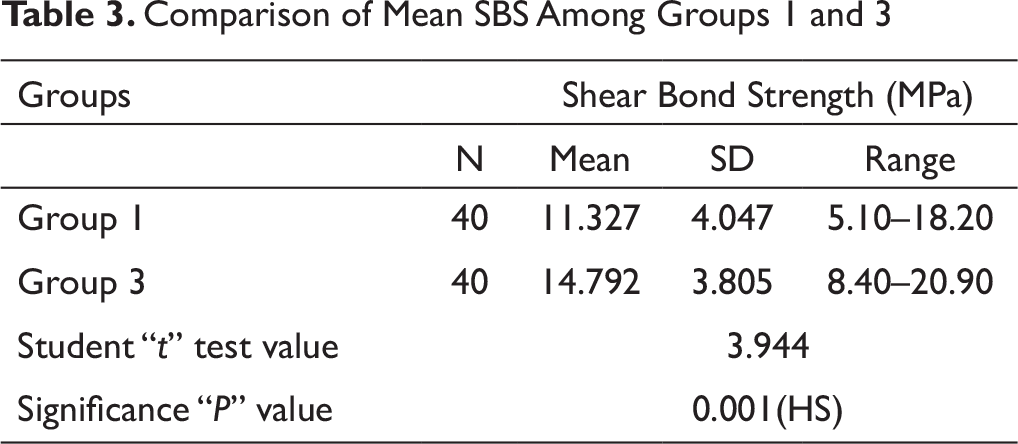
Comparison of Mean SBS Among Groups 1 and 3
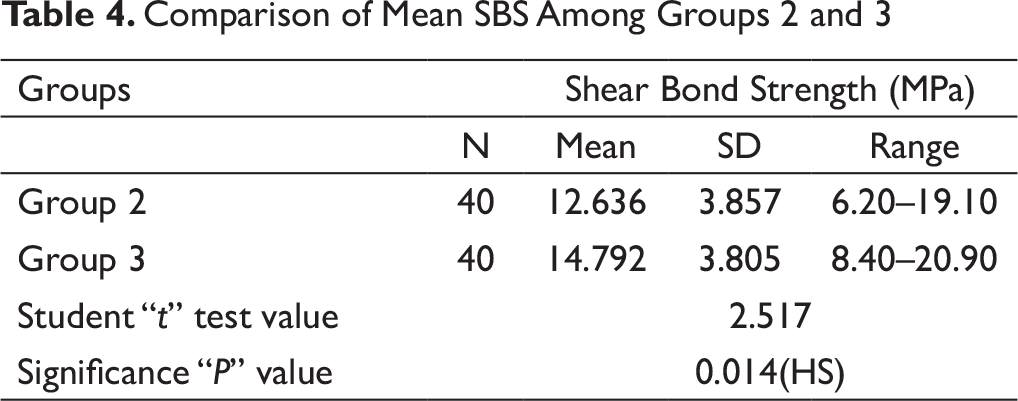
Comparison of Mean SBS Among Groups 2 and 3
Statistical Analysis
Mean SBS, standard deviations (SDs), and minimum and maximum values were calculated for each group. The data obtained were subjected to statistical analysis with the help of a statistician.
Statistical analysis was carried out using the Statistical Package of Social Science (SPSS Version 20; Chicago Inc., USA). Data comparison was carried out by applying specific statistical tests to find out the statistical significance of the comparisons. Significance level was fixed at P < .05. Statistical tests employed for the obtained data in our study were Student’s t-test and Analysis of the Variance (ANOVA).
Results
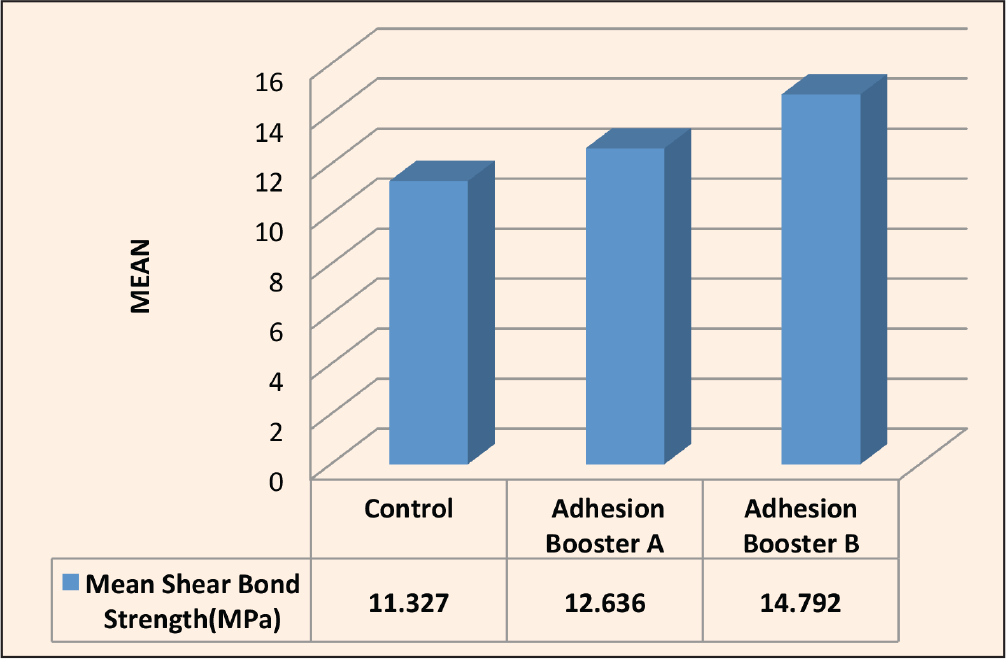
Comparison of Mean Shear Bond Strength Among All Three Groups 1, 2, and 3 (Table 1, Figure 9)
Comparison of Mean SBS Among All 3 Groups 1, 2, and 3
Comparison of Mean SBS Among Groups 1 and 2
Comparison of Mean SBS Among Groups 1 and 3
Comparison of Mean SBS Among Groups 2 and 3
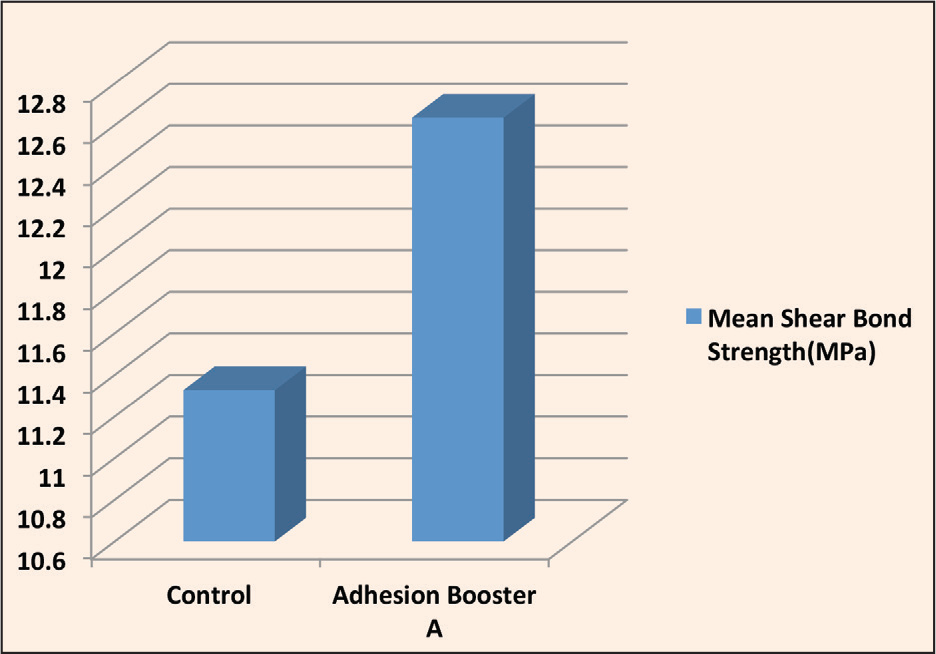
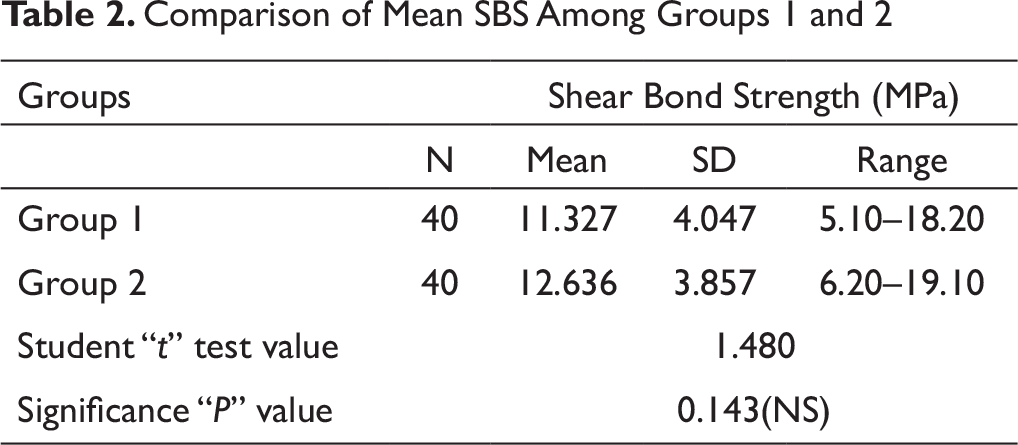
Comparison of Mean Shear Bond Strength Among Groups 1 and 2 (Table 2, Figure 10)
SBS was slightly more in group 2 samples as compared to controls. There was statistically no significant difference in SBS among groups 1 and 2 (P = .143)
Comparison of Mean Shear Bond Strength Among Groups 1 and 3 (Table 3, Figure 11)
SBS was more in group 3 samples as compared to Group 1. There was statistically significant difference in SBS among groups 1 and 3 (P = .001).
Comparison of Mean Shear Bond Strength Among Groups 2 and 3 (Table 4, Figure 12)
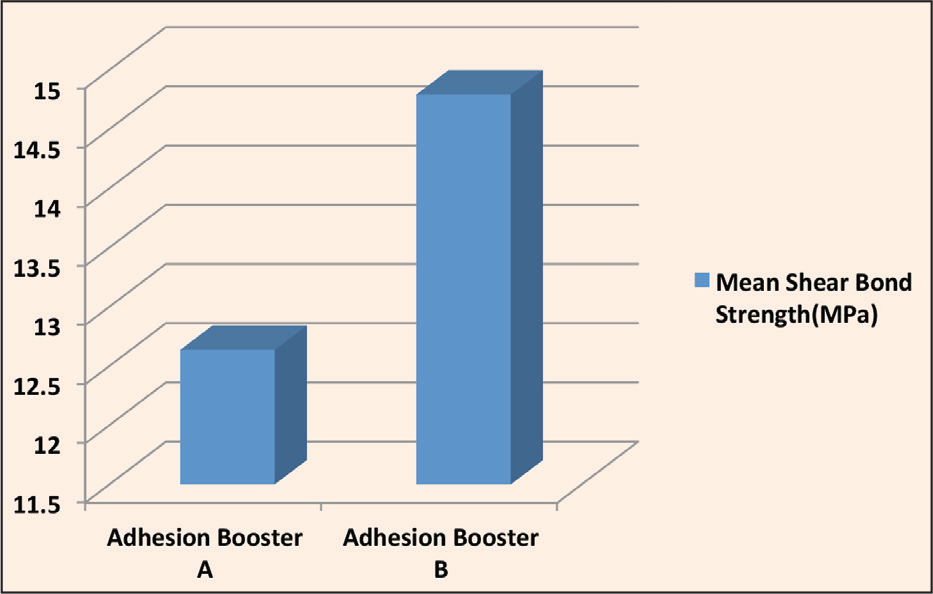
SBS was more in group 3 samples as compared to Group 2. There was statistically significant difference in SBS among groups 2 and 3 (P = .014).
Discussion
Greenlaw et al and Reynolds have advised that bond strengths of 5.9 to 9.7 MPa are appropriate for orthodontic treatments.16, 24 The mean bond strength obtained in vitro in the 3 groups in this study ranged from 11.33 MPa to 14.79 MPa, values that would be appropriate for orthodontic treatment according to several authors.16, 24
Egan et al evaluated the efficacy of enhance adhesion booster along with a conditioner that contained methyl methacrylate (Plastic Conditioner, Reliance Products Inc, Itasca, IL, USA) for direct bracket bonding. They did not find any increase in the bond strength of re-bonded brackets. 22 In the present study, when adhesion booster B was used (group 3), there was a significant increase (P = .001) in SBS in comparison with the control group (group 1) and the other group that received the adhesion booster A (group 2).
Several studies evaluated the effect of the booster on direct and indirect bracket bonding and found that adhesion boosters produced adequate bond strength under humid and dry conditions.21, 25-27 The present study was carried out on the lingual bracket using indirect bonding technique under dry conditions, and the results of our study have indicated that the adhesion booster B is capable of increasing the SBS (P = .001).
Although the manufacturer claimed that both adhesion boosters evaluated in this study can improve adhesion for indirect bracket bonding with the Thomas technique, 28 the differences in SBS may be due to differences in their composition.23, 29
O’Brien et al concluded that the SBS is affected by the type of adhesive material used. 29 Adhesion booster A is composed of Na-N-tolyglycine glycidyl methacrylate and biphenyl dimethacrylate, which increases the adhesion of adhesive material to a different surface, such as resin and enamel. In contrast, adhesion booster B is composed of hydrophilic primers that contain biphenyl dimethacrylate and hydroxyethyl methacrylate, which is used to increase the adhesion to enamel, dentin, metal, and resin surfaces. In the present study, group 1 did not receive any booster in bonding, while groups 2 and 3 received adhesion booster A and adhesion booster B, respectively. SBS was found highest in group 3, followed by group 2, and it was least in controls. It was 14.792 ± 3.80 among group 3 samples, 12.636 ± 3.85 among group 2 samples, and 11.327 ± 4.047 among controls.
In the present study, greater bond strength was required for lingual brackets; hence, the adhesion booster was used. However, there are several factors that may affect the bracket bonding in the patients. These factors are difficult to reproduce in the laboratory, and this in vitro study therefore cannot be considered as the comprehensive representation of the clinical cases. In the oral cavity, bonded brackets are exposed to the variations in temperature and humidity. These variations may lead to the stress on the brackets and on the adhesive, which may affect the bond strength. 30 Therefore, thermocycling was performed to produce a better simulation of the intraoral conditions.
The mean bond strength obtained in vitro in the 3 groups in this study ranged from 11.33 MPa to 14.79 MPa, which was well above the suggested values of 5.9 MPa and 9.7 MPa of SBS as sufficient for clinically effective bonding. 16 However, while in vitro studies allow for more standardized procedures by limiting variables, caution should be taken when interpreting absolute magnitudes of SBS of an artificial test environment and applying them to clinical settings. The substrate storage, length of storage, extraoral bonding process, lack of periodontal ligament, crosshead speed, point of application, direction, and magnitude of force are among the many artificial variables not experienced in vivo.
The main disadvantage of the in vitro orthodontic bonding is that the complete replication of the in vivo condition has not been possible yet. 31 It should be pointed out that while in vivo randomized control trials can provide the most clinically relevant information, in vitro studies still hold great value for initial screening of products to be tested in a clinical setting, as well as actual measurement of SBS of adhesive products.
The storage solution in this study was distilled water. The samples used in this study had varying times of storage duration in distilled water (1 to 4 months). The reason behind this discrepancy was the periodic but irregular collection of samples from multiple sources throughout Bhopal. Williams and Svare found that there were no significant differences in SBS when bonding composite to enamel for specimens stored at 24 hours, 3 months, and 5 years. 32
It is important to note that the history of the tooth samples is unknown. Unless it was obvious to the investigator, the samples used for this study may contain teeth with a previous history of orthodontic bonding. Bonding to these teeth may more accurately represent the re-bonding scenario. It has been shown that the re-bonded teeth have a significantly lower and inconsistent SBS compared to new teeth. 33 In addition, teeth that were extracted may have abnormally high stresses applied to the enamel during the extraction process; this may explain why a higher amount of enamel fractures were seen when debonding than what might be observed clinically. 34
Most orthodontic SBS tests in vitro have used very slow crosshead speeds to accurately and consistently collect data. It must be stressed that these crosshead speeds lack correspondence to clinical conditions. In this present study, a constant, unidirectional force of 0.5 mm/min was applied to each sample. While some of the investigators found that crosshead speed variation between 0.1 and 5 mm/min does not significantly influence SBS, 35 a systematic review found that each millimeter per minute of greater crosshead speed increased bond strength by 1.3 MPa. 36 Regardless of the speed chosen for SBS tests, caution must be taken when drawing clinical conclusions from in vitro models.
Conclusion
The findings indicate that shear bond strength was admissible in all the groups.
The application of assure universal bonding resin significantly increases the bond strength of lingual brackets in indirect bonding.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.