
Abstract
Objective: To establish soft-tissue cephalometric norms of Kashmiri population and to compare them with European-American norms.
Material and Methods: A total of 102 subjects falling in the age group of 19 to 25 years were selected from random and representative sample of 5317. Reference lines were traced according to the definitions given by Holdaway, Rickett, Steiners, Merrifield, and nasiolabial angle. Thirteen linear and 4 angular measurements were analyzed on the lateral cephalogram of the sample.
Results: Significant differences were found between male and female subjects in measurements of the soft-tissue facial angle, upper lip thickness, upper lip strain, lower sulcus depth and soft-tissue chin thickness, and upper lip to S line and nasiolabial angle. Soft-tissue cephalometric norms of Kashmiri population that were measured in the present study when compared with the norms set by Holdaway’s parameters, Rickett’s E line, Merrifield Z angle, Steiner’s S line, and nasiolabial angle did not fall within the normal range. The facial angle was found to be greater by 1.36°, upper lip sulcus depth was greater by 0.53 mm, convexity at point A was greater by 2.43 mm, the H angle was greater by 5.64°, upper lip thickness and strain were greater by 2.30 and 2.36 mm, respectively, soft-tissue chin thickness was greater by 0.92 mm, upper lip to S line was greater by 0.60 mm, and lower lip was greater by 0.91 mm when compared with the standard European-American norms.
Conclusion: According to the present study, the measured soft-tissue cephalometric norms for Kashmiri population differed from the standard norms. When planning orthodontics treatment, it should be kept in mind that the profile may not necessarily be orthognathic.
Introduction
Orthodontics presents a philosophical challenge, in that both art and science are of equal importance. 1 The recorded human history and the archeological evidence show that mankind since the time memorable has been aware of facial esthetics, proportion, and beauty. From time to time, there has been a swing from one philosophy to another, latest being a shift toward a soft-tissue paradigm. 2 The soft-tissue influence on craniofacial growth has been widely known and accepted following the functional matrix hypothesis given by Dr Melvin L. Moss,3-6 and its relevance to the orthodontic diagnosis and the treatment planning cannot be overruled. The external appearance of an individual is the reflection of his or her soft tissue, thus a reflection of orthodontics treatment. Majority of the regions of the world follow the cephalometric standards that are based on sample population with European or American ancestors, and since patients in different parts of the world and many times within the same country have different racial and ethnic backgrounds, these standard norms, if followed, may not be appropriate for the diagnosis and treatment planning of these patients.
This has led to various reseraches7-28 being conducted for different ethnic and racial groups around the globe. These investigations have not only established the soft-tissue norms, but also shown that different ethnic and racial groups differ in their soft-tissue norms when compared to European or American population.
After a thorough review of literature, not even a single research paper describing the soft-tissue cephalometric norm of Kashmiri population was found. Kashmir is a province covering an area of 15520.3 km2 and has a population of 14.28 million with only 1 Dental College and Hospital that provides fixed orthodontic treatment to the general Kashmiri population. It becomes of utmost importance to come up with the norms for this population.
So, the aim of the current study undertaken was to establish soft-tissue cephalometric norms for a sample of Kashmiri population according to Holdaway’s parameters, Rickett’s E line, Merrifield Z angle, Steiner’s S line, and nasiolabial angle, and to compare them with those of standard European-American tissue norms.
The following null hypotheses were tested:
There was no difference between Kashmiri male and Kashmiri female soft-tissue norms. There was no difference between Kashmiri population and standard European-American soft-tissue norms.
Materials and Methods
Ethical Approval and Patient Consent
Ethical approval was obtained from the scientific committee of the institution. Consent was also sought by asking the patient to sign a form that explained the nature and purpose of the study. For the current study, the probability of type 1 error (α) was fixed at 5% and that of type 2 error (β) was fixed at 20%. The power of the study was set at 80%. The sample size for the study was determined scientifically, and using Cohen’s test, the sample size of minimum of 102 was established. The sample of 102 (51 female and 51 male subjects) was collected from the patients, students, and employees of this government-run institute. People from all over the region converge here for treatment, work, and education. So, the sample represents Kashmiri population from each district. All the patients reporting to the outpatient section of the hospital were also screened. Out of a sample of 5317 people, 102 who fulfilled the criteria were selected, with an age range of 18 to 32 years. The inclusion criteria were as follows: Kashmir subjects with both parents and both grandparents (maternal and paternal) of Kashmiri origin, Class I molar, canine, and incisor relationship, a balanced soft-tissue profile, a pleasant smile, no previous history of orthodontic treatment, and the presence of all permanent teeth, excluding third molars. Individuals who did not satisfy the above criteria were excluded from the study. These included patients with syndromes, patients who had undergone fixed orthodontic treatment in the past, and patients with deviation from Class I canine and molar relation.
For standardized cephalometric radiography, all radiographs were taken from the same X-ray machine with the subjects in natural head position, with their teeth in maximum intercuspation and lips at repose. All the lateral cephalometric radiographs were recorded by the same operator from a standardized Orthophos XG5 DSCEPH (SIRONA) on a standard Konica Minolta 8 × 10 inches film with an anode to the mid-subject distance of 5 feet by the same operator. Linear measurements were recorded with a measuring scale up to a precision of 0.5 mm. The same researcher performed all tracing and recorded all measurements. Not more than 5 radiographs were traced at 1 time to prevent examiner fatigue.
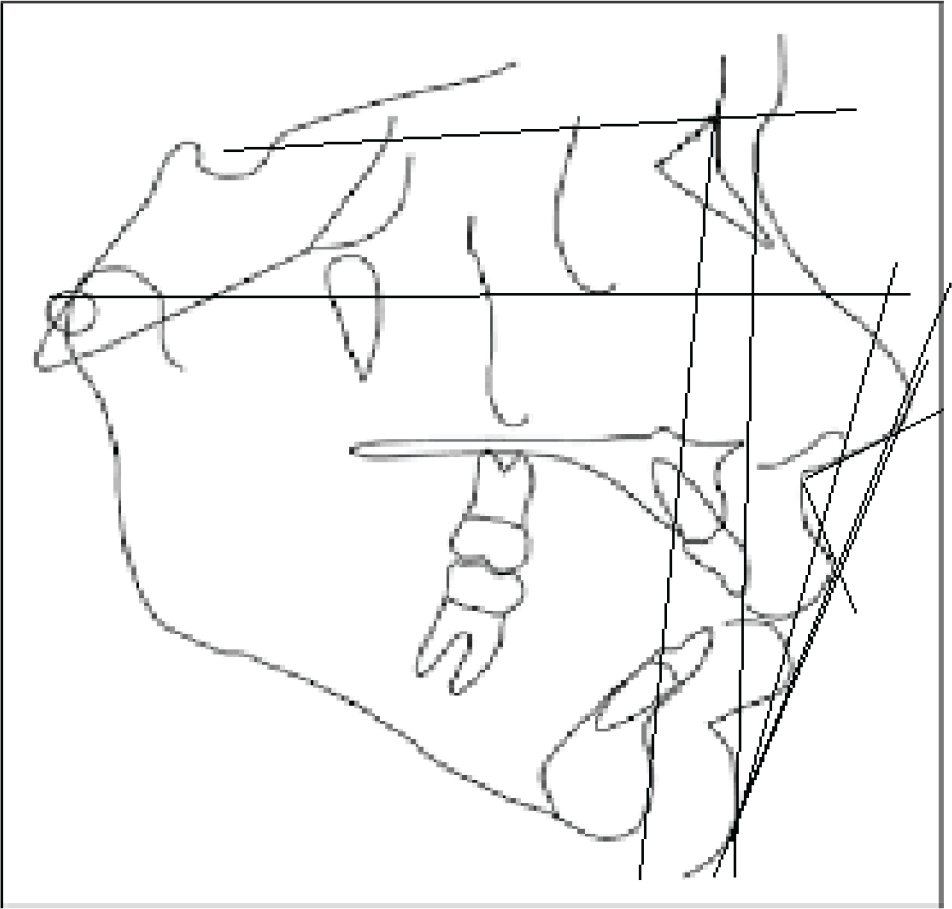
Seven reference planes were identified and traced (Figure 1) according to the definitions by Holdaway’s parameters, 29 Rickett’s E line, 30 Merrifeild Z angle, 31 Steiner’s S line, 32 and nasiolabial angle. A total of 13 linear (mm) and 4 angular (degree) measurements were analyzed.
Cephalometric Planes Used in the Study
Frankfort horizontal (FH) plane
Sella-nasion: a line connecting sella and nasion
Line connecting soft-tissue nasion to soft-tissue pogonion (N′ to Pog′)
Harmony (H) line: a line tangent to the chin and upper lip
Nasion to pogonion, N to Pog
Frankfort perpendicular (FP) line: a line perpendicular to FH and tangent to the vermillion border of the upper lip
Rickett’s E line: a line connecting the tip of the nose to soft-tissue pogonion
Pogonion to soft-tissue pogonion, Pog to Pog′
Soft-tissue pogonion to most protrusive point on lip
Tangent to the columella of the nose
Tangent to the upper lip
S line: a line extending from the soft-tissue contour of the chin to the middle of an S formed by the lower border of the nose.
Linear Measurements
Upper lip curvature: a perpendicular dropped from the FH tangent to the upper lip. From this line, the depth of the upper lip sulcus was measured.
Skeletal convexity at point A: skeletal convexity measured from point A to nasion-pogonion (skeletal).
Nose tip to the H line: tip of the nose to the H line.
Upper sulcus depth: measured from the H line.
Upper lip thickness: measured horizontally from a point on the other alveolar plate 2 mm below point A to the outer border of the upper lip.
Upper lip strain: measurement extends horizontally from the vermilion border of the upper lip to the labial surface of the maxillary central incisor.
Lower lip to the H line: measured from the most prominent outline of the lower lip.
Lower sulcus depth: measured at the point of deepest curvature between the lower lip to chin.
Soft-tissue chin thickness: measured as a distance between the bony and soft-tissue pogonion.
Upper lip to Rickett’s E line: measured horizontally from the upper lip to the E line.
Lower lip to Rickett’s E line: measured horizontally from the lower lip to the E line.
Upper lip to the S line: measured horizontally from the upper lip to the S line.
Lower lip to the S line: measured horizontally from the lower lip to the S line.
Comparison of Kashmiri Male and Female Soft-tissue Morphology
Angular Measurements
Facial angle: an angle formed by the intersection of the FH plane with the line extended from the soft-tissue nasion to pogonion.
H-angle: an angle formed between the H line and soft-tissue nasion-pogonion line (N′-Pog′).
Merrifield angle: an angle formed by the intersection of FH and a line connecting the soft-tissue chin (Pog′) and the most protrusive lip point (may be upper or lower).
Nasiolabial angle: an angle formed by 2 lines, namely a columella tangent and an upper lip tangent.
Results
Statistical software Statistical Product and Service Solutions version 20.0 (SPSS Inc., Chicago, IL, USA) was applied to carry out the statistical analysis of the data. 33 Data were analyzed by means of descriptive statistics, namely means and standard deviations. Student’s independent test was used to measure the difference between genders and the t-test for single mean was used to measure the difference between the soft-tissue cephalometric norms of Kashmiri sample and those of European-American. A P value of less than .05 was considered statistically significant. All P-values were 2 tailed.
Gender Differences
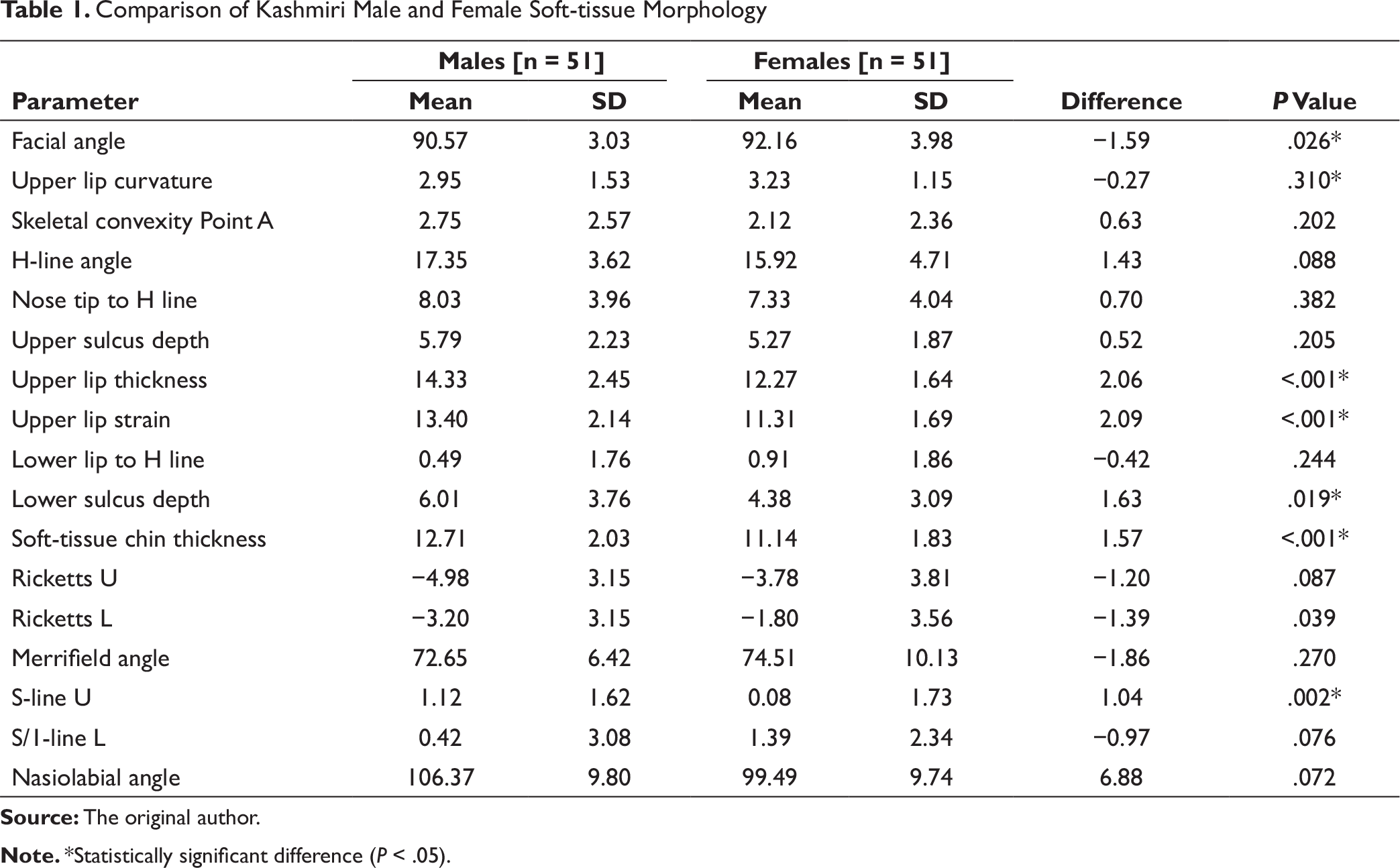
Table 1 illustrates the descriptive and comparative statistics between Kashmiri female and male subjects for soft-tissue morphology. Significant differences were found between male and female subjects in measurements of the soft-tissue facial angle, upper lip thickness, upper lip strain, lower sulcus depth and soft-tissue chin thickness, and upper lip to S line and nasiolabial angle (P < .05, Table 1).
Mean was calculated as a midpoint of the range, when not provided by the original author.
The soft-tissue facial angle of female subjects was 1.59° greater than that of male subjects; upper lip thickness was greater by 2.06 mm in male subjects that of female subjects. Similar results were found when upper lip strain was compared; upper lip strain was found to be 2.09 mm more in male subjects than that in female subjects. Lower sulcus depth and soft-tissue thickness were found to be less in female subjects than those in male subjects by 1.63 and 1.57 mm, respectively. The nasiolabial angle was fund greater by 6.88° in male subjects than that in female subjects. The upper lip S line in female subjects was found to be retrusive when compared with that of male subjects.
Mean calculated as a midpoint of the range, when not provided by the original author.
Comparison of Kashmiri Soft-tissue Norms with European-American Norms
$: Range not provided by the original author.
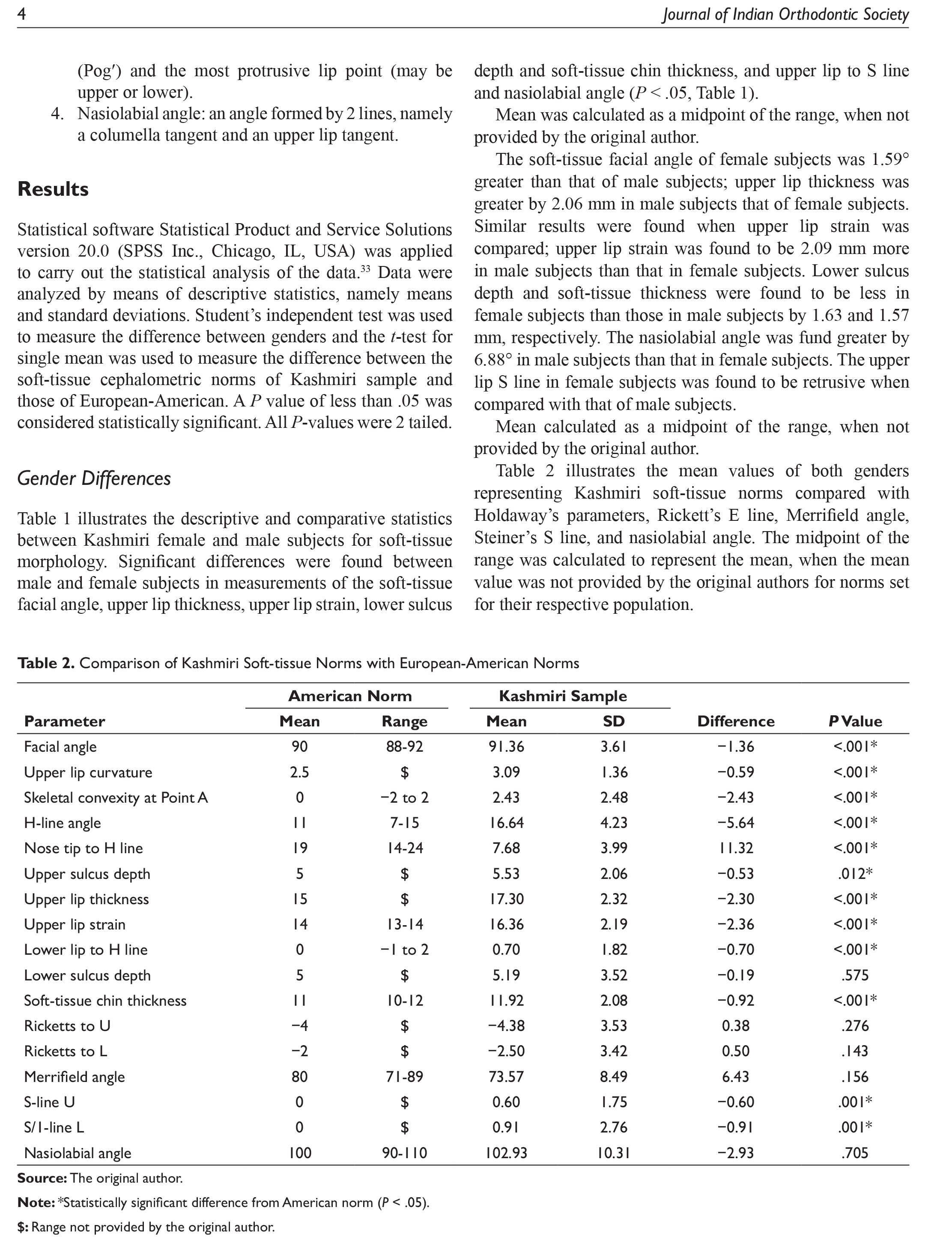
Table 2 shows that majority of the Kashmiri norms measured in the present study were statistically significant when compared with the norms set by Holdaway’s parameters, Rickett’s E line, Merrifield angle, Steiner’s S line, and nasiolabial angle, and did not fall within the normal range, with lower sulcus depth, upper and lower lips to E line and nasiolabial angle being exceptions that fell within the normal range.
The facial angle was found to be greater by 1.36°, upper lip sulcus depth was greater by 0.53 mm, convexity at point A by 2.43 mm, H angle by 5.64°, soft-tissue chin thickness by 0.92 mm, upper lip to S line by 0.60 mm, and lower lip greater by 0.91 mm than European-American norms. All the above-stated values were found to be statistically significant.
The nose tip to H line was less than Holdaway’s value by 11.32 mm; similarly, upper lip thickness and upper lip strain were found to be less by 2.30 and 2.36 mm, respectively. The Merrifield angle was found to be less than 6.43° but was not statistically significant.
Discussion
India is a country with a large number of racial/ethnic groups. Each region of country not only differs in cultural backgrounds but also has a different ethnicity and exhibit considerable variability in facial esthetics and profile from each other and rest of the world. Various studies have been conducted in Indian population and around the world in various ethnic groups and compared to the standard norms set by various authors. These researchers have shown statistically significant differences when compared to the standard norms.
Comparison Between Male and Female Soft-Tissue Morphology
In the current study, the facial angle was 1.59° greater in female than that in male subjects, indicating a prominent chin in female subjects (Table 1). Upper lip thickness and upper lip strain were found to be greater in male subjects; this could be attributed to morphological differences in soft-tissue between males and females, in general. Lower sulcus depth and soft-tissue chin thickness were found to be less in female subjects. The H angle was not found to be statistically significant.
Similar results between gender were found by Basciftci et al 34 and Hwang et al 35 for Anatolian Turkish, and Korean and European-American adults, respectively. The upper lip of Kashmiri female subjects was found to be more retrusive in relation to chin and the base of nose than the norms described by Steiner, which can be related to the presence of more prominent chin in female subjects and thinner lips. The same could be explained for the nasiolabial angle which we found to be smaller in female subjects.
Comparison of Norms for Kashmiri Population and Other Ethnic Groups
Majority of Kashmiri norms determined by the current study were statistically significant and differed from European-American norms. The facial angle was greater by 1.3°. The soft-tissue facial angle helps us to determine the degree of chin prominence. The mean value is found to be greater in Kashmiri population, indicating that this population has a well-defined chin of adequate thickness. Also, the upper lip curvature of population is more than ideal, indicating thick lips. Similar results were found in study conducted on Malabar population.
The H angle was greater than Holdaway’s value by 5.64°. The H angle was also found to be greater in Antolian Turkish, 34 Korean 35 , and Japanese 36 adults; these studies found similar deviations.
The ideal H angle for the present study sample with skeletal convexity at point A (2.43 mm) should be 13°, indicating that the upper lip was excessively prominent in relation to the overall soft-tissue profile. Valianthan et al 37 and Purushothaman et al 38 have shown similar results where the H angle was found to be higher in Kerala population and Malabar population, respectively.
In comparison with Caucasians, upper lip thickness was found to be more in Indo-Aryans, 39 Yemini, 40 and Hyderabadi 41 population. Similar results were found in our study.
The lower lip to H line was prominent by 0.70 mm when compared with Holdaway’s value. This indicates that Kashmiri population has a protrusive profile when compared with Caucasian population as indicated by an increase in the value of the lower lip to the H line, skeletal convexity, and H angle.
The relationship between the upper and lower lips of Kashmiri adults to the E line was the same as that described by Rickett’s E line for North American population.
Conversely, the lips of Anatolian Turkish subjects were more retrusive to the E line, while those of Korean 35 and Japenese 36 subjects were more protrusive.
The position of the upper and lower lips with respect to the S line is slightly protrusive, but this finding is not statistically significant.
The Merrifield angle was greater by 6.43° in Kashmiri subjects than the standard norms, but it is not statistically significant.
Thus, the null hypothesis was rejected, and it was concluded that Kashmiri ethnic soft-tissue norms differ in majority of the parameters when compared with the ideal norms set by Holdaway’s parameters, Rickett’s E line, Merrifield angle, Steiner’s S line, and nasiolabial angle. This should be considered while planning orthodontic treatment for these patients. It should be kept in mind that it is not necessary to have an orthognathic profile in mind; a slightly protrusive profile may sometimes be acceptable.
Conclusion
The following conclusions can be drawn from the present study:
Female subjects had more prominent chin than male subjects in Kashmiri population. The lips of the female subjects were considerably more retrusive in relation to base of the nose and chin, while those of male subjects were slightly more protrusive. Majority of the soft-tissue parameters undertaken in the present study in Kashmiri population were found to be statistically different than those of the European-American norms. Facial angle, convexity at point A, H angle, upper sulcus depth, lower lip to H line, and soft-tissue chin thickness were found to be greater in Kashmiri population, whereas the nose tip, H line, upper lip thickness, and upper lip strain were found to be less. While diagnosis and treatment planning, separate norms should be set for different ethnic groups and patient should be treated keeping their ethnic background in mind.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.