
Abstract
Crowding, protrusion, and class II or end-on occlusion are malocclusions frequently associated with a narrow transverse dimension. The goal of expansion is to reduce the need for extractions in permanent dentition through elimination of arch length discrepancies as well as correction of bony base imbalances. Gaining arch length makes the subsequent fixed appliance treatment easier and shorter. Palatal expansion is usually achieved by using fixed rapid maxillary expansion, but because of the complexity, cost, and increased laboratory steps, this step is sometimes omitted. We have modified the design and screw activation protocol of the removable Schwarz plate in such a way that it gives efficient and stable expansion as well as arch perimeter gain with simpler mechanics. We present the long-term results of 10 such cases treated with this modified expander followed by fixed appliances.
Introduction
This article shows how maxillary transverse discrepancies can be corrected by using a modified removable screw plate to increase the arch perimeter and gain space. Most of the cases with crowding are treated with extraction therapy or other approaches like rapid maxillary expansion (RME). A modified butterfly expander to increase anterior arch length has also been mentioned in the literature. 1 To the best of our knowledge, there is no literature that shows how the expansion is managed 2–3 years after retention with semi-rapid expansion protocol using a removable appliance. Modification of conventional Schwarz plates as well as screw activation protocol can bring about a lot of difference in end results. This appliance is simple and easy to use, does not cause pain or trauma, and gives long-term stable results. We present 10 cases of maxillary arch length discrepancies treated by such a modified expansion plate, which makes this approach of treating patients unique.
Case Report
Diagnosis and Treatment Plan
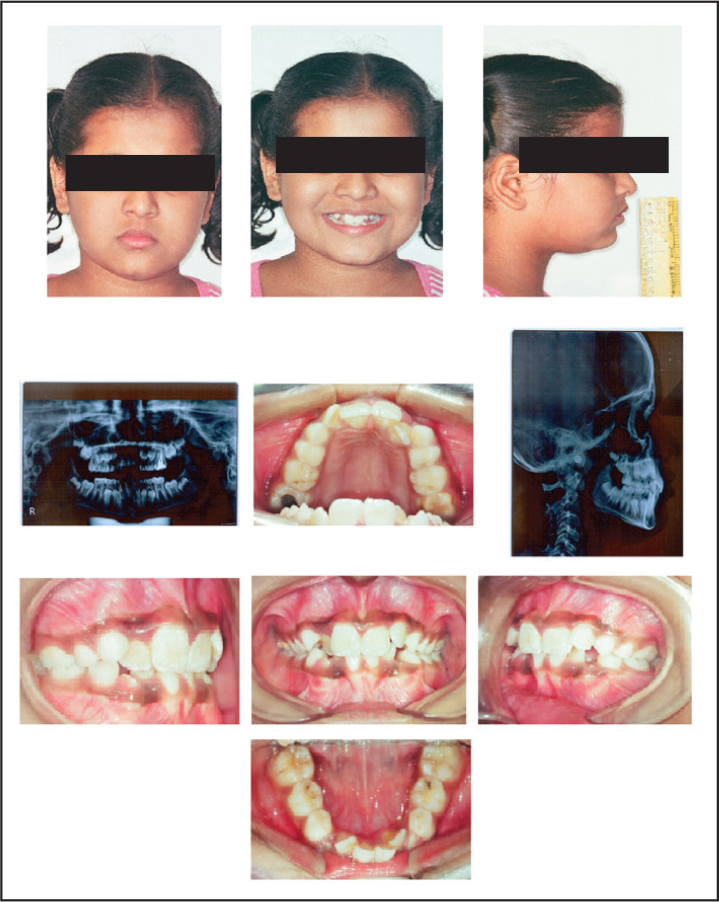
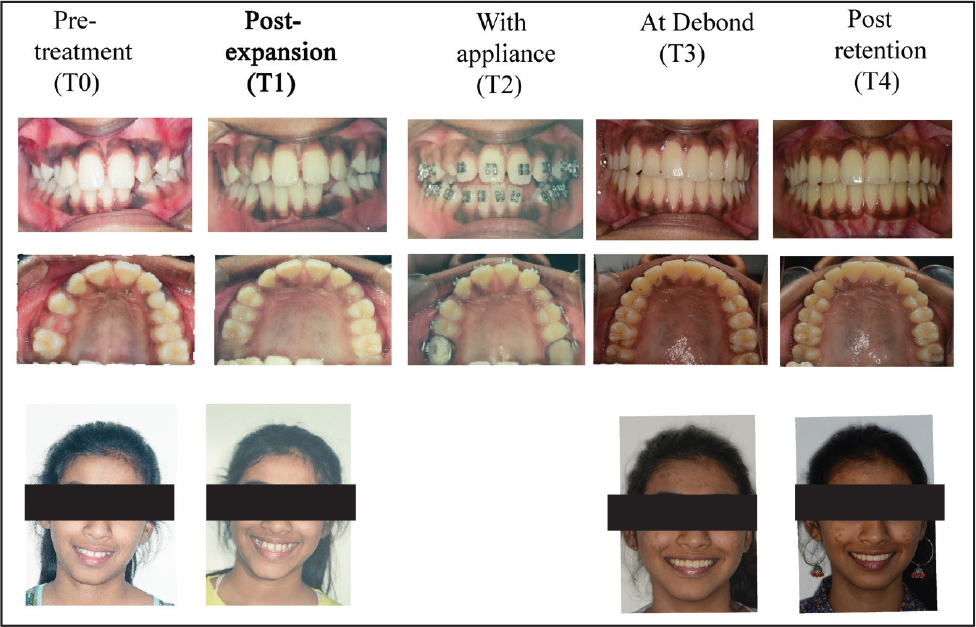
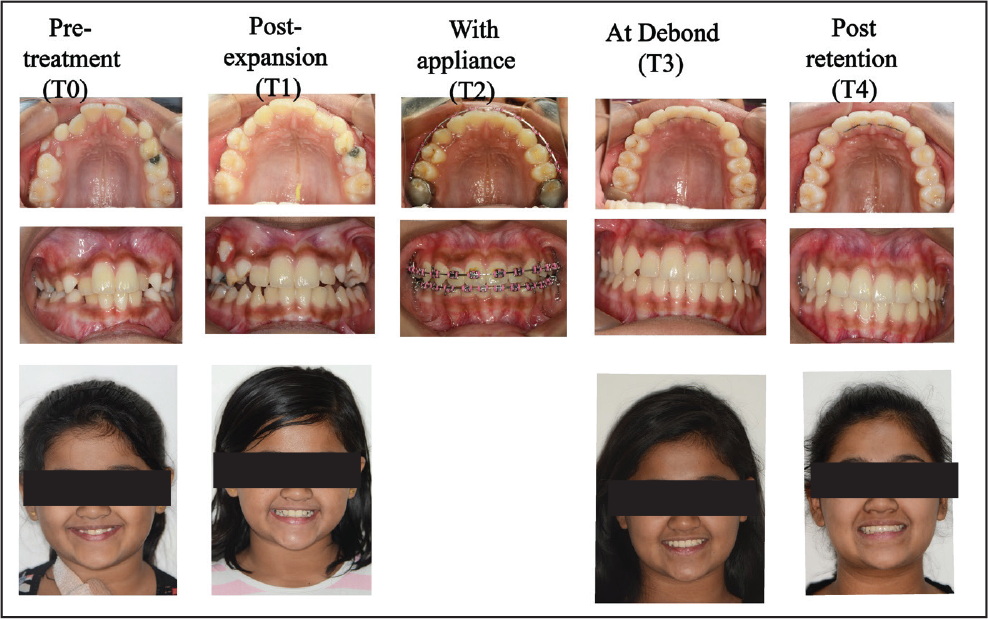
Ten patients in the age group of 12 to 15 years who presented with the chief complaint of crowded teeth were selected. The clinical evaluation showed relatively normal profile and Class 1 molar relationships. Using our earlier hypothesis, 2 it was found that all the patients had narrow maxillary arches with anterior crowding. None of the cases presented with a cross bite. The patients were given the modified screw plate and instructions on activation protocol were given. After 3 to 4 months, the patients were immediately put on fixed appliances (0.022 slot, pre-adjusted) without any retention protocols. Photographic records were taken at T0 (pre treatment), T1 (post expansion), T2 (mid-fixed appliance treatment), T3 (de bonding), and T4 (post retention). The radiographic records were taken at T0, T1, and T3 only.
Treatment Progress
Description of Appliance
Appliance design: A simple removable plate was devised as the mode for expansion. An appliance (Figure 1) was constructed with the jackscrew placed at the deepest part of the vault along with six well-fitting Adam’s clasps (on lateral incisors, first premolars or primary deciduous first molars, and 1st molars). It was assumed that with the force of activation closer to the center of resistance (touching the deepest part of the vault), and the tight adaptation of the appliance, there would be more lateral translation of the 2 maxillary halves and less of dento-alveolar tipping. 3 The 6 Adam’s clasps ensured even distribution of force anteriorly as well as posteriorly and prevented excessive dental tipping. The acrylic plate and wires of the clasps passing over the teeth unlocked the occlusion and allowed for easier expansion. The appliance used an 11 mm expansion jackscrew (Dentaurum, Ispringen, Germany) with activations of a full turn equivalent to a 0.8 mm expansion.
Expansion protocol: The rate and rhythm of screw activation was 1/8th turn (0.8 mm per full turn) 6 days a week (every day except Sunday). The screw was not turned for 1 day per week to allow for dissipation of accumulated forces and biophysical stress build up during expansion. Thus, an expansion of 0.6 mm per week was given. It has been hypothesized that a rapid activation of more than 2 to 4 mm per week is likely to cause tissue damage, while slow activation will not provide enough force to open the suture.4–6
Instruction to patients:
Modified Removable Expansion Appliance

Treatment Outcomes
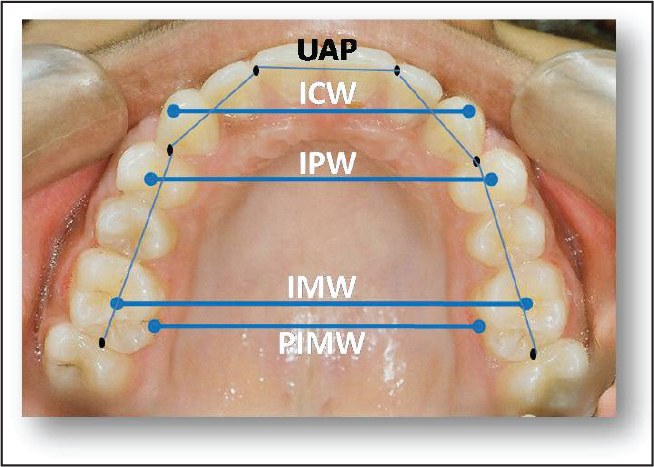
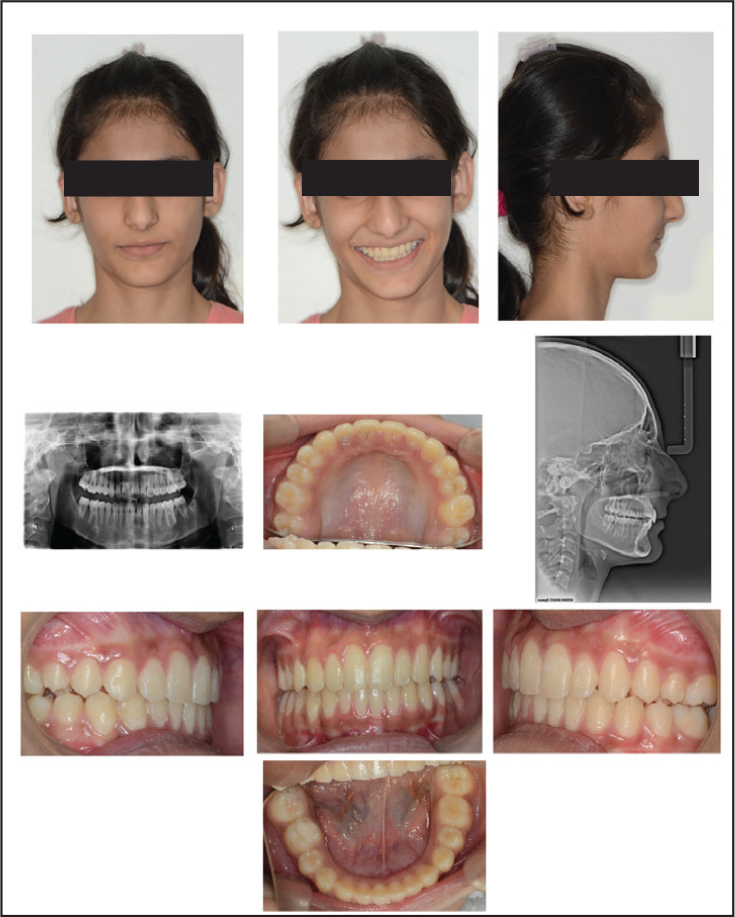
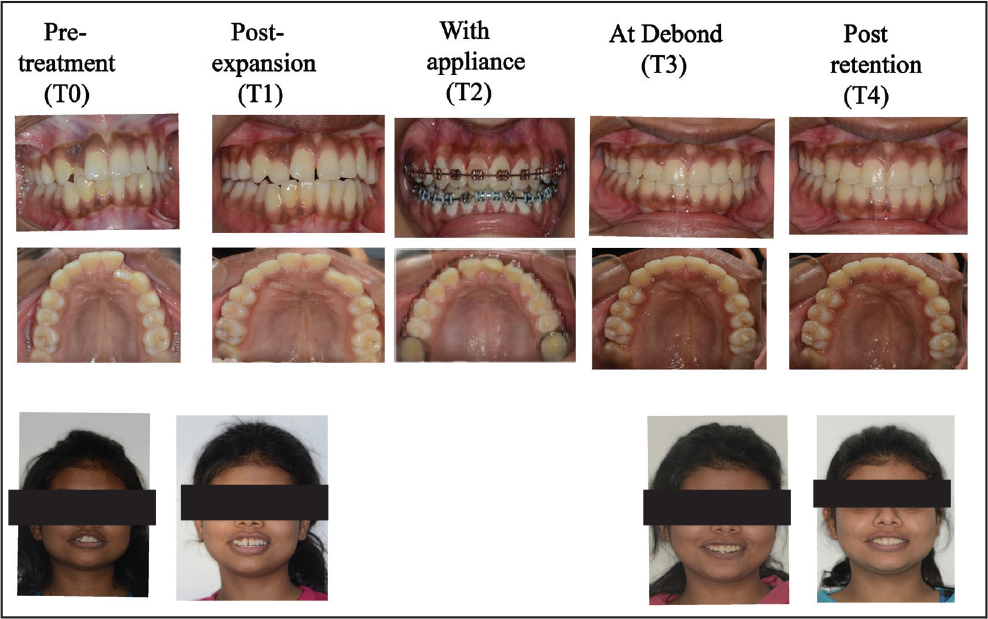
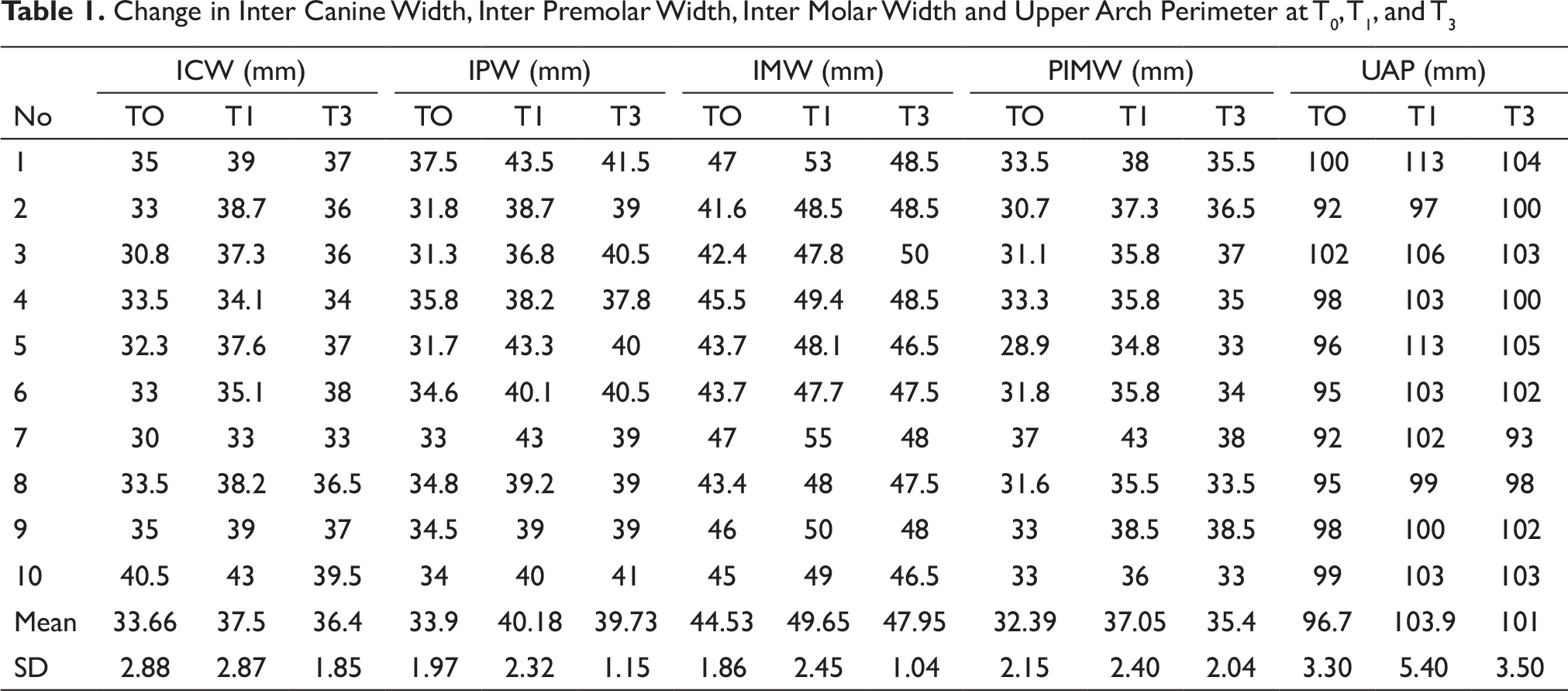
Measurements were taken on models at three time points: T0, T1, and T3 as seen in Figure 2. All the cases were followed till 2 years post retention (Figures 3[a]–12]. It was found that all parameters showed increase in distances from T0 to T1; and decrease from T1 to T3; with a net gain at T3 as compared to T0. There was an average gain in upper arch perimeter (UAP) of 4.3 mm from T0 to T3 (Table 1).
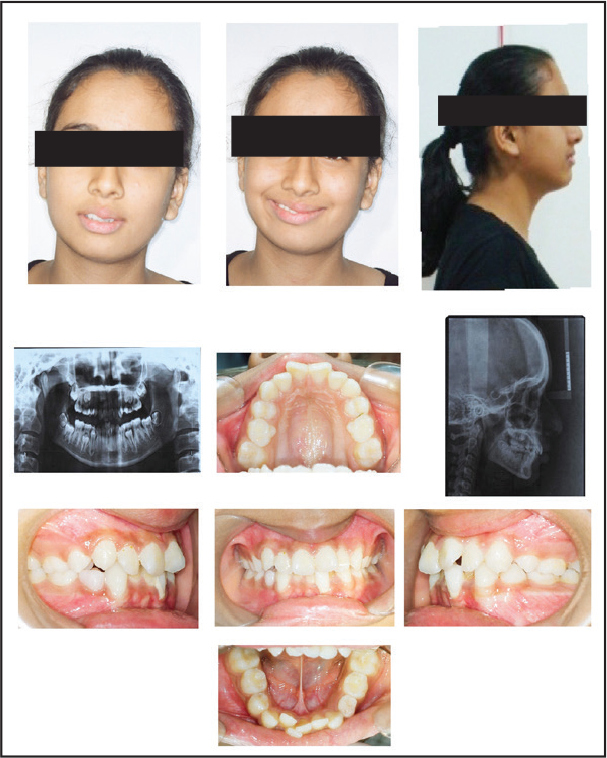
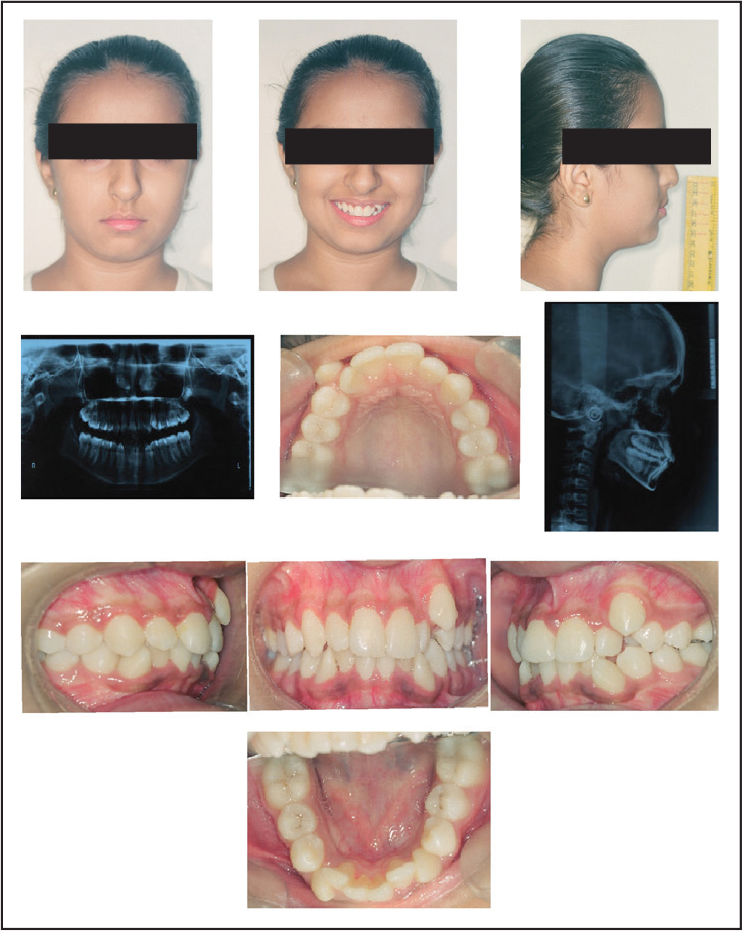
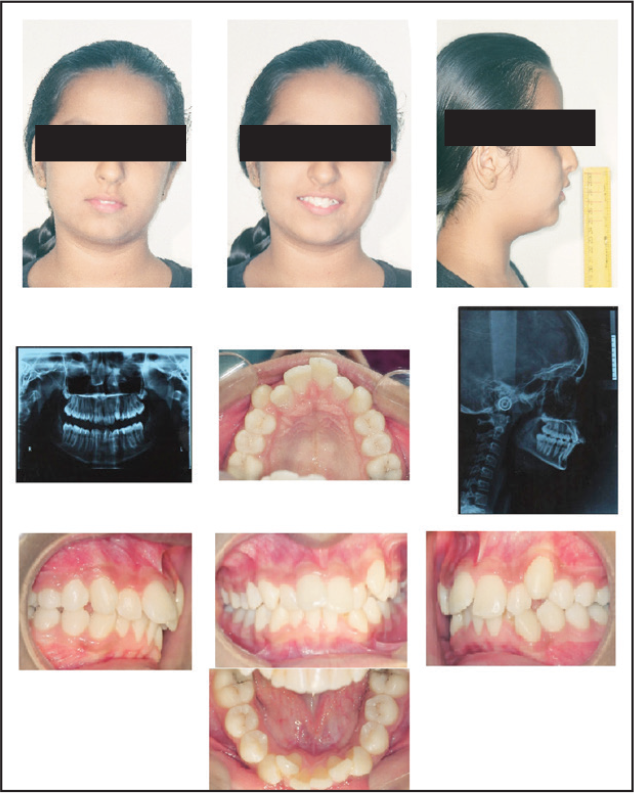
Case 1: Pre Treatment (T0)
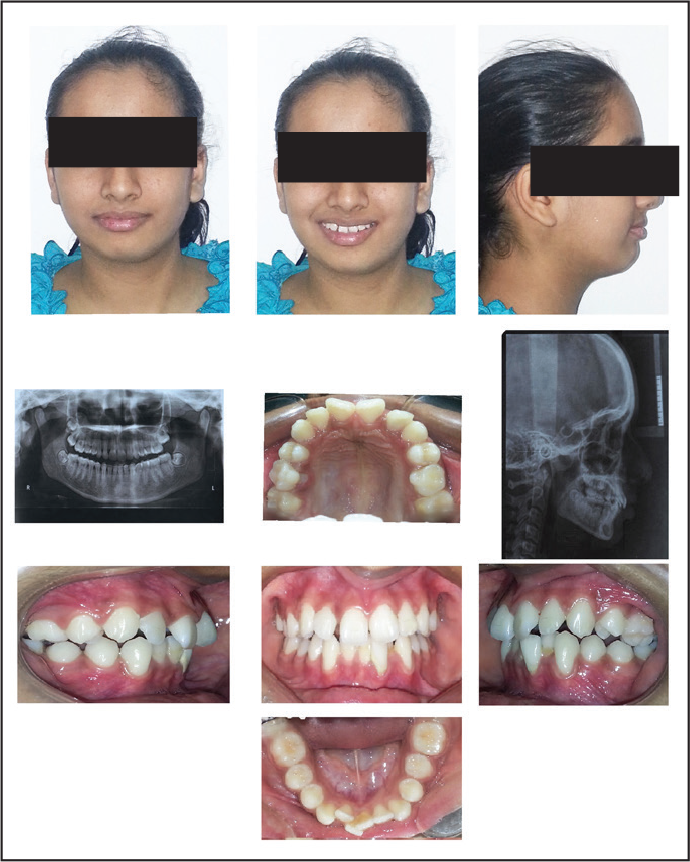
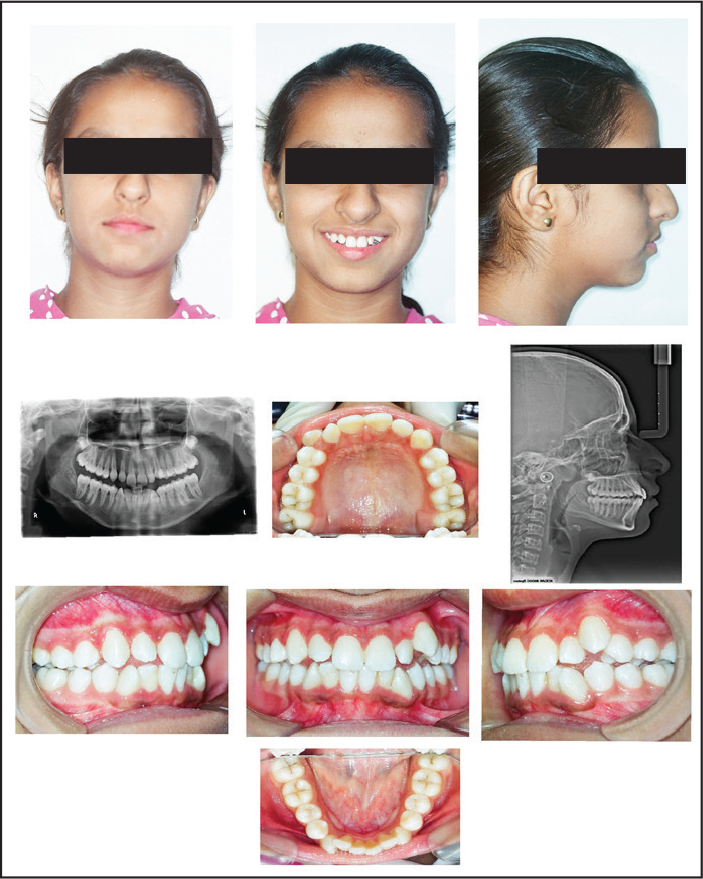
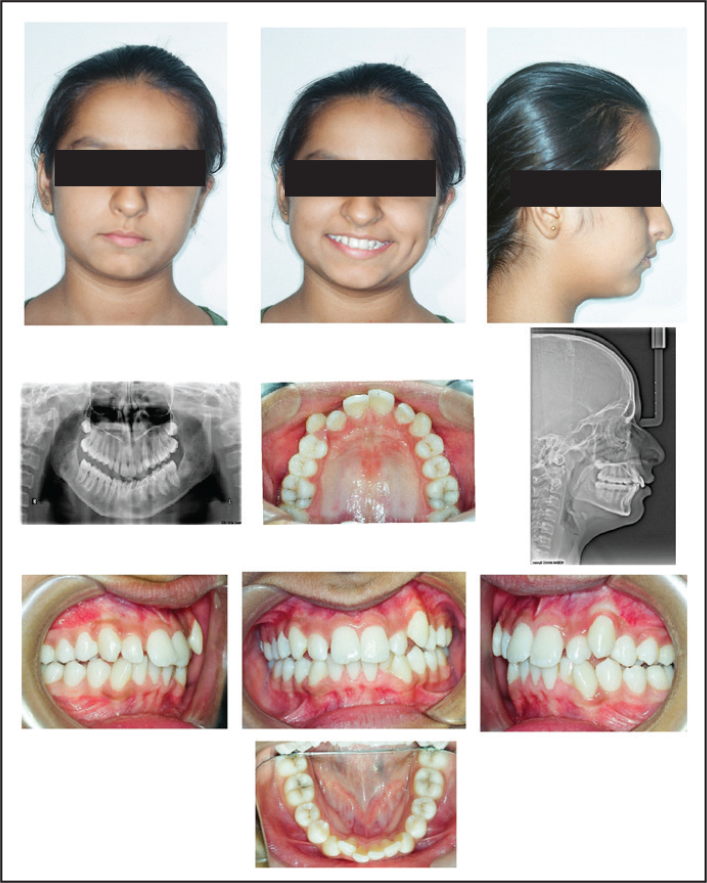
Case 1: Post Expansion (T1)
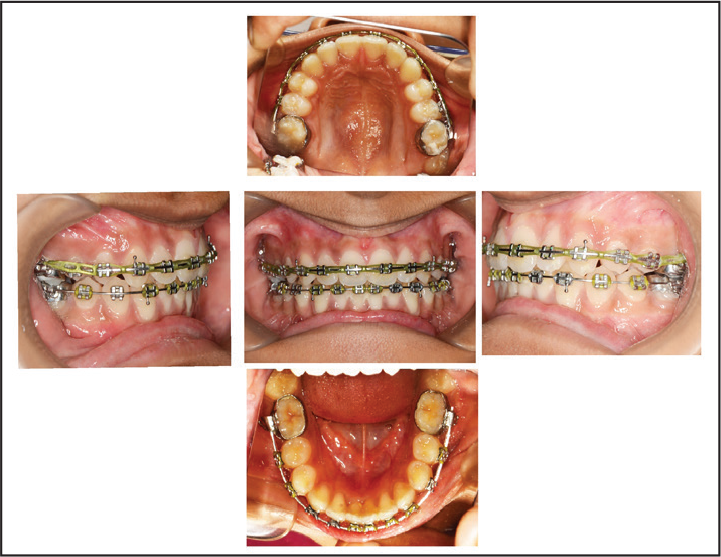
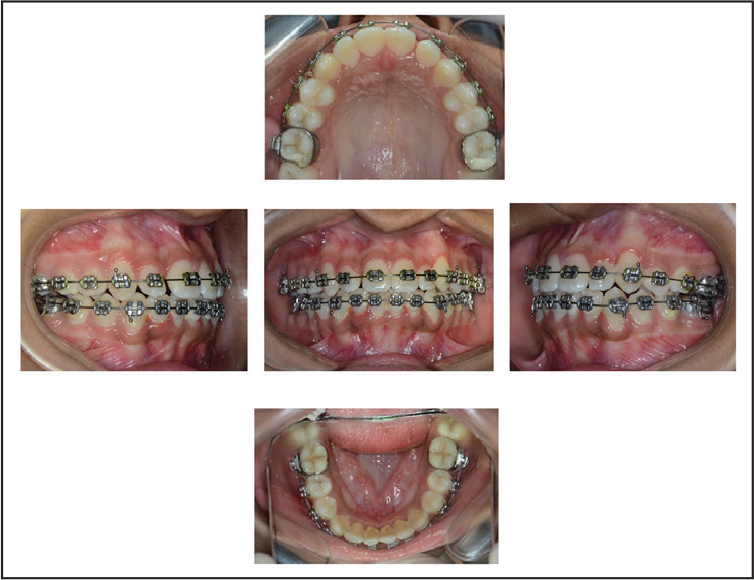
Case 1: With Appliance (T2)
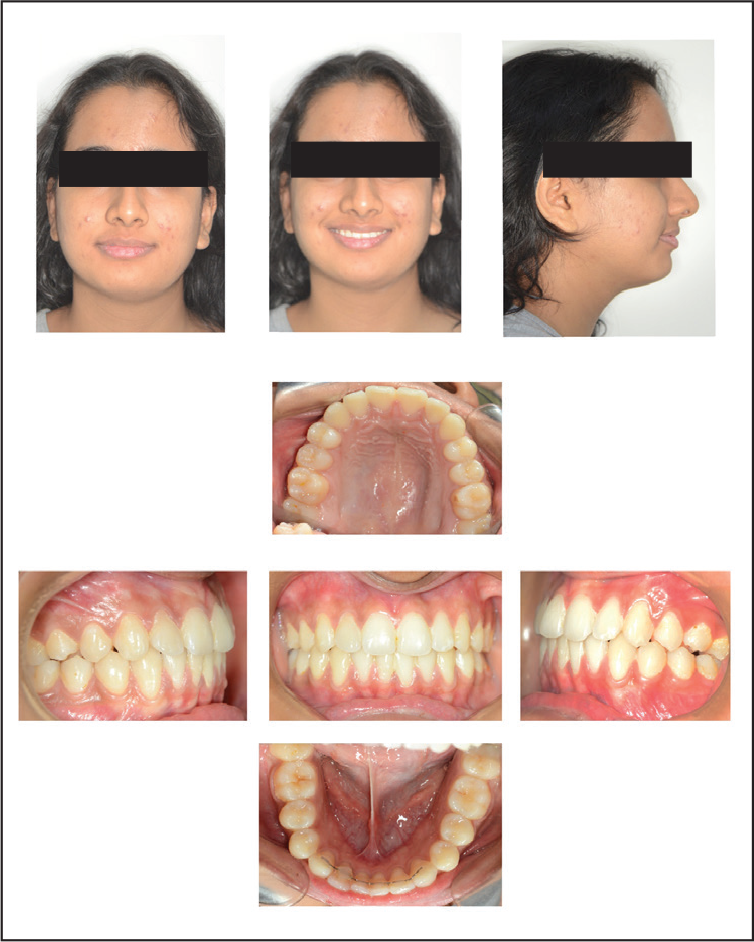
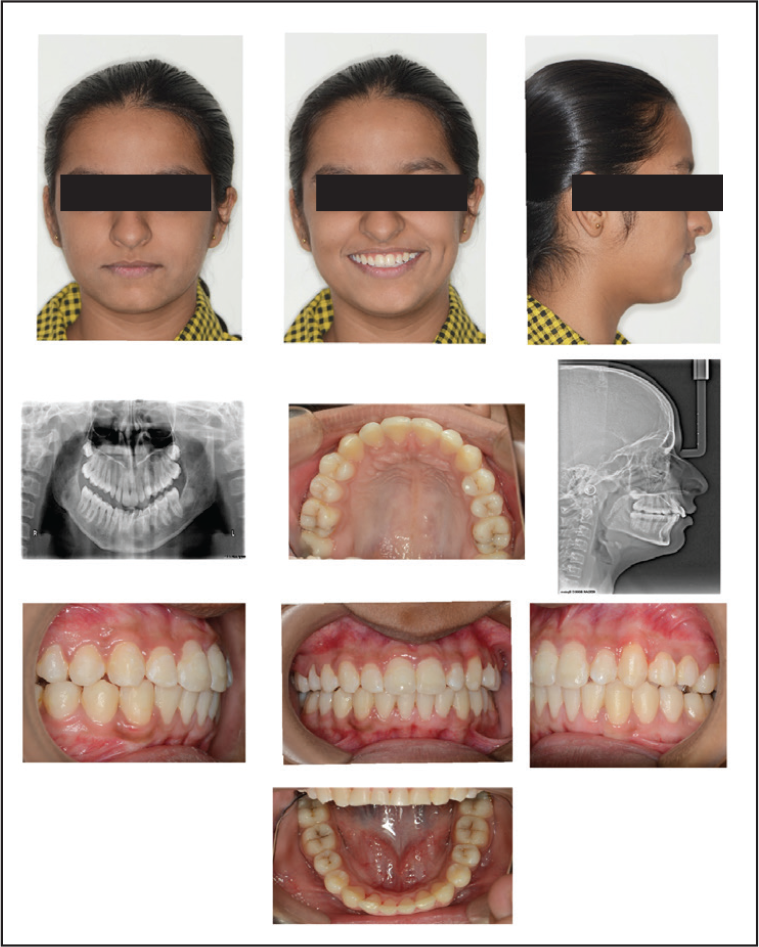
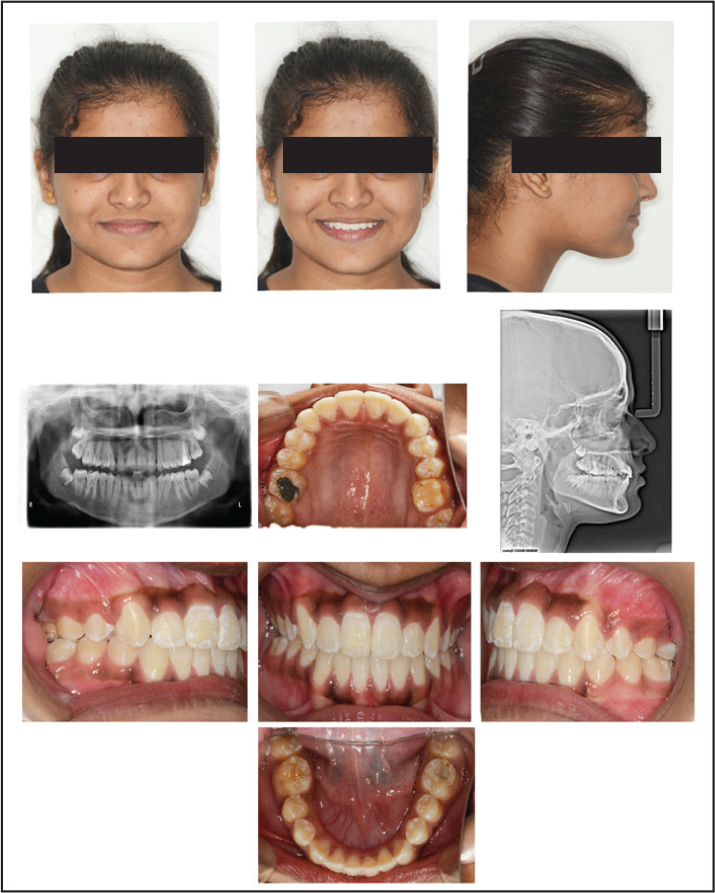
Case 1: At Debond (T3)

Case 1: Post Retention (T4)
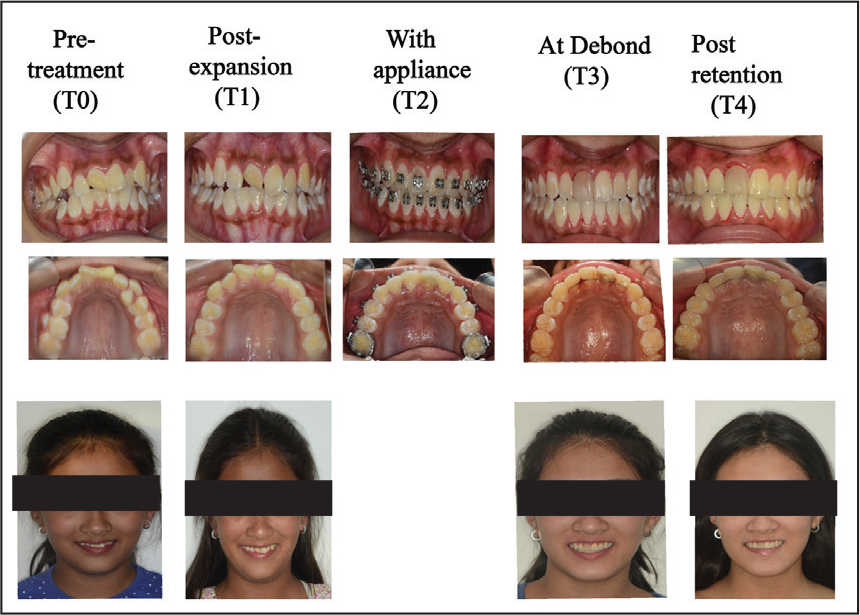
Case 2: Pre Treatment (T0)
Case 2: Post Expansion (T1)
Case 2: With Appliance (T2)
Case 2: At Debond (T3)

Case 2: Post Retention (T4)

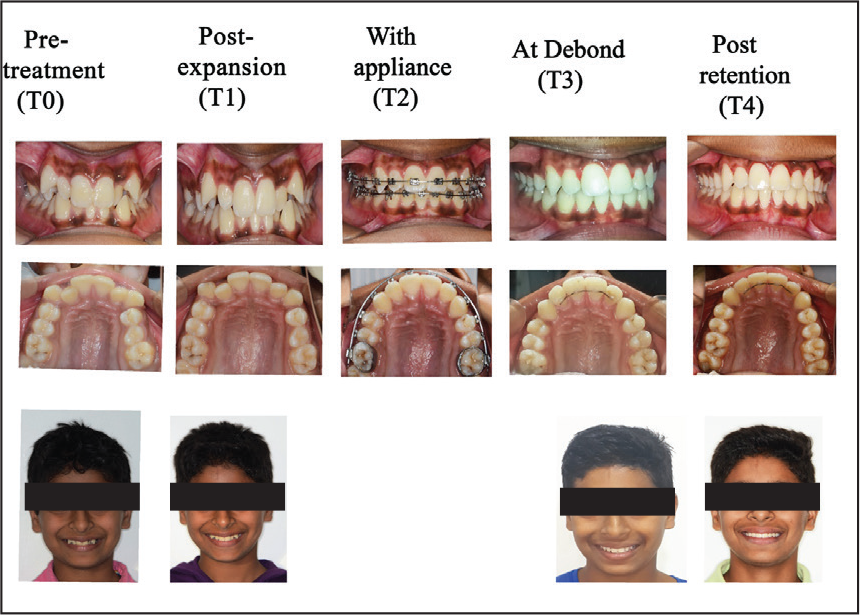
Case 3: Pre Treatment (T0)
Case 3: Post Expansion (T1)
Case 3: With Appliance (T2)

Case 3: At Debond (T3)
Case 3: Post Retention (T4)

Case 4: Pre Treatment (T0)

Case 4: Post Expansion (T2)

Case 4: With Appliance (T3)

Case 4: At Debond (T3)
Case 4: Post Retention (T4)

Case 5: Pre Treatment (T0)
Case 5: After Expansion (T1)

Case 5: With Appliance (T2)

Case 5: At Debond (T3)
Case 5: Post Retention (T4)

Case 6 (T0–T4)
Case 7 (T0–T4)
Case 8 (T0–T4)
Case 9 (T0–T4)
Case 10 (T0–T4)
Change in Inter Canine Width, Inter Premolar Width, Inter Molar Width and Upper Arch Perimeter at T0, T1, and T3
Discussion
The use of the modified expansion appliance allowed space gain by increase in arch perimeter. The advantage of this method is ease of insertion and removal of the appliance as compared to fixed expanders. Minimum laboratory steps are required to fabricate the appliance. The activation of the screw was easy as it was done outside the mouth. The patients found it easy to maintain oral hygiene. There were no reports of pain or discomfort and there were no emergencies reported. We found that the expansion was stable with minimum tipping and was maintained till the end of retention period as can be seen in photographs. The subsequent treatment with fixed appliances was simpler and the treatment time was shorter due to the space gained through the use of the modified expander. We found this appliance simple and easy to use, cost effective, as well as efficient. Studies have shown an approximate net gain of 4–6 mm in upper arch perimeter using fixed rapid maxillary expansion appliances.7,8 In our cases, we achieved a mean gain of 4.3 mm in arch perimeter using semi-rapid expansion protocol with a removable appliance. Along with the arch perimeter, increase in arch width was also noted in all the cases.
Conclusion
Adequate and stable increase in arch perimeter and arch width was achieved by using a modified removable screw plate appliance. There are many ways to expand the palate. This method can be one more tool that can be added to the armamentarium of the clinician.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.