
Abstract
Objective: To assess skeletal, dentoalveolar, and soft-tissue effects of fixed functional appliances (FFAs), alone or in combination with multibracket appliances (comprehensive treatment), on Class II malocclusion in postpubertal patients.
Data Sources: Literature survey was conducted using the Medline, SCOPUS, Latin American and Caribbean Health Sciences, and Scientific Electronic Library Online databases and the Cochrane Library, and through a manual search. No restrictions were set regarding the type of fixed appliance, treatment length, or to the cephalometric analysis used. Data extraction was mostly predefined at the protocol stage by 2 authors.
Study Selection: Only double-blind randomized controlled trials (RCTs) of Class II skeletal cases treated by any FFA that had assessed specific skeletal, dental, or soft-tissue parameters were included.
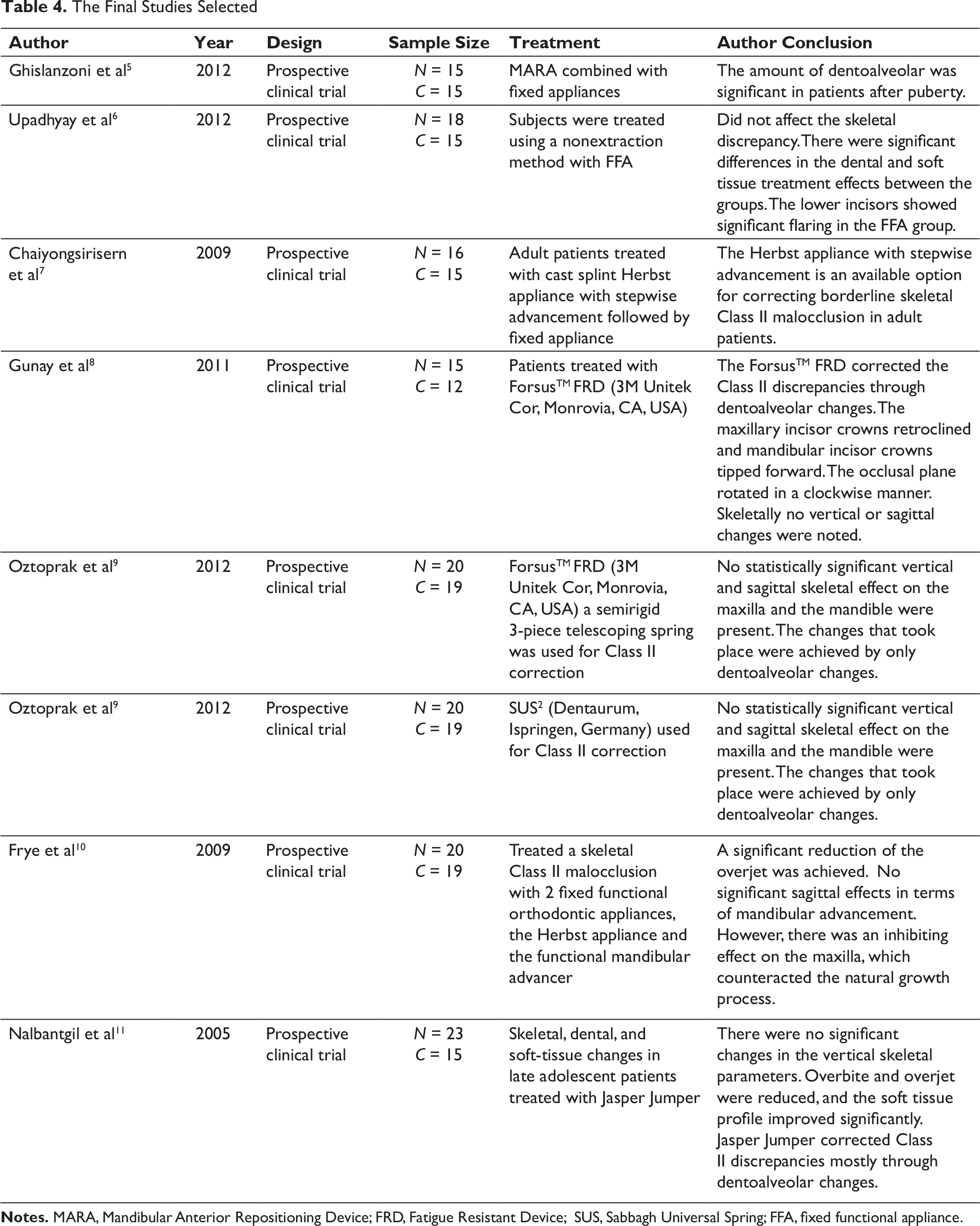
Data Synthesis: A total of 8 articles qualified for the final analysis. The studies were composed of late-adolescent or adult patients who were at the end of their postpubertal growth period. This meta-analysis included data from 271 subjects (142 Class II patients and 129 untreated individuals) and 8 RCTs, which assessed linear as well as angular cephalometric changes induced by Class II treatment with FFAs.
Conclusions: Based on the data available on postpubertal patients, it was concluded that the fixed functional treatment is effective in Class II malocclusion and shows changes in skeletal, dental, as well as soft tissue.
Introduction
Skeletal Class II malocclusion is one of the most common malocclusions in the general population. It occurs in about 25% to 30% of the general population. Moreover, mandibular retrognathism has been seen to be the most common causative factor for skeletal Class II malocclusion. 1 Fixed functional appliance (FFA) was introduced first in dentistry by Dr Emil Herbst of Germany at the 5th International Dental Congress in Berlin in 1909. In 1979, Pancherz et al 2 popularly investigated the effect of continuous bite jumping on the masticatory muscle activity using electromyography records, in Class II Division 1 malocclusion, treated with the Herbst appliance. This helped support the effectiveness of these appliances. James J. Jasper in 1987 introduced a relatively new type of flexible, fixed and tooth-borne functional appliance that allowed lateral movements as well. Hence, gradually new options as well as varieties were added to the family of FFAs.
The various treatment options for Class II correction apart from myofunctional/FFAs include orthopedic appliances like headgears, camouflage line of treatment by extractions of premolars, distalization of the maxillary arch or the surgical correction of the underlying skeletal discrepancy when growth has completed. FFAs are the most commonly used appliance to correct skeletal discrepancy in a growing stage, but still its enhancement effect on mandibular growth has been questionable. All these FFAs correct the skeletal Class II malocclusion by the combined effects of skeletal and dental changes, including the advancement of mandible, restrict the growth of maxilla, fanning the lower anterior, and retroclination of the maxillary anterior. Various studies support FFAs as an effective treatment option in treating Class II malocclusion occurring due to skeletal discrepancy, specifically when used during the pubertal growth phase, but unfortunately very few data are available on postpubertal patients. 3 Rarely any reviews have as such focused attention on how effective it is in treating early adult patients; moreover, they have shown substantial variability in the results reported. Therefore, this systematic review with a meta-analysis aims to assess the core skeletal, dentoalveolar, and soft-tissue changes seen after the use of FFAs, with or without the conjunctive use of fixed multibracket appliances, for treating adult Class II malocclusions.
Materials and Methods
Search Strategy
The following meta-analysis abides by the statements provided by the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) statement. 4 A PROSPERO registration was done during the initial steps of the review (http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42019126955).
This review and meta-analysis were written following the Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. The articles were sought and selected through a thorough literature survey from the following databases: (a) The Cochrane Library, (b) PubMed (c) SCOPUS, (d) Scientific Electronic Library Online, and (e) Latin American and Caribbean Health Sciences. Additionally, a manual search was also performed by further examining the intrastudy references as well as the titles of the articles published in the last 2 decades in various journals. Two blinded authors were assigned the responsibility of performing the eligibility assessment as well as data-collection processes of the articles. In the case of occasional conflicts, a thorough discussion was carried out on each article until reaching a conclusion.
PICO
Patient, Population, or Problem: Class II postpubertal cases/late adolescent/adult cases
Intervention, Prognostic Factor, or Exposure: Treatment done by myofunctional appliances (no limitation to the types of appliances used)
Comparison or Intervention: Compare Class II malocclusion treated with myofunctional appliance (experimental group) with those treated without myofunctional appliances (control group)
Outcome: Changes brought about in skeletal, dental, and soft-tissue cephalometric parameters after treatment of the experimental and the control groups.
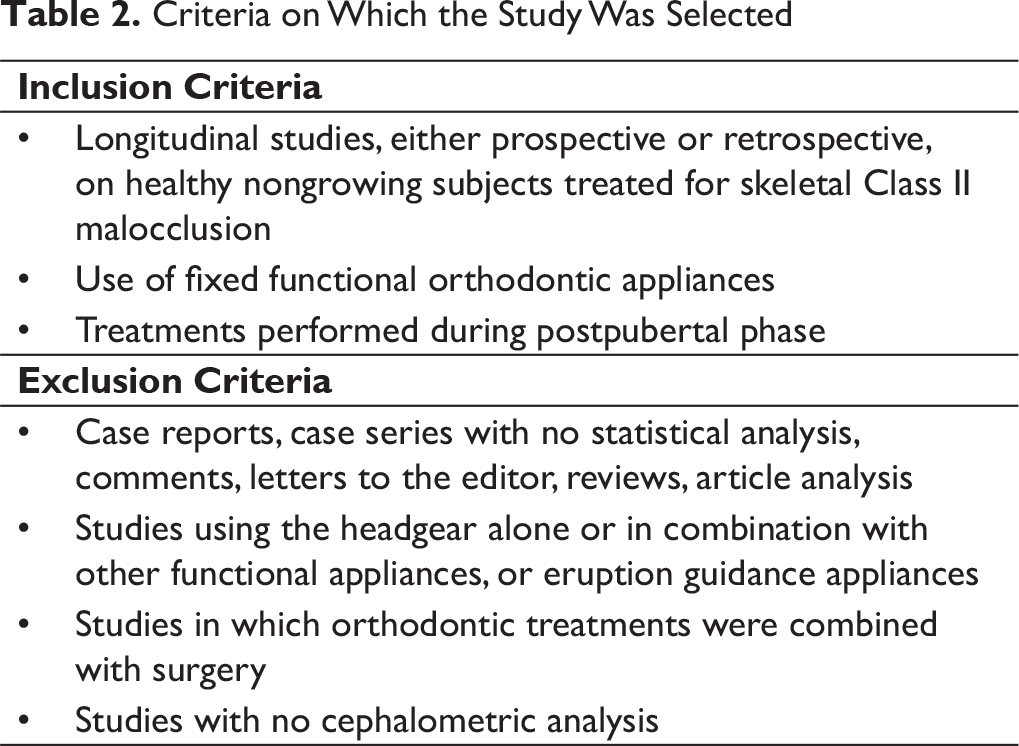
Eligibility Criteria
The selected studies were either randomized controlled trials (RCTs) or prospective or retrospective controlled clinical trials. It was a compulsion for them to include only healthy patients treated in their postpubertal growth phase. These studies must investigate the skeletal, dentoalveolar effects, and/or soft-tissue changes based on the types of parameters set prior to the start of the survey. Also, no restrictions were put concerning the type of fixed appliance used or the length of treatment. Studies not mentioning a reliable indicator of the growth phase (like the hand-and-wrist maturation method or the cervical vertebral maturation method) were excluded from our selected list of studies.
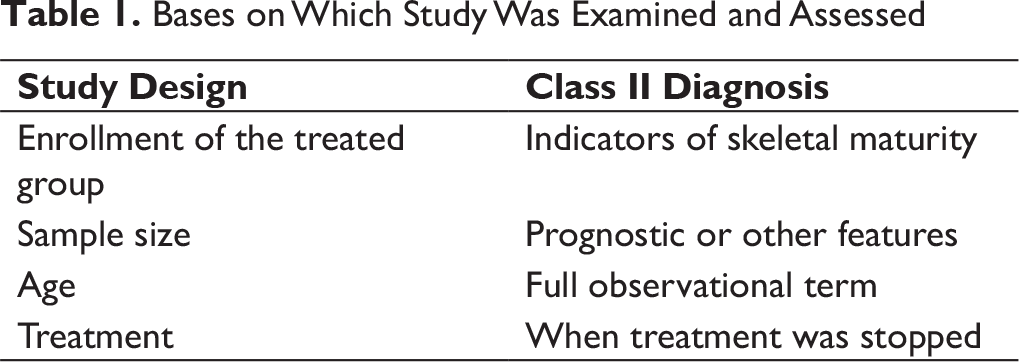
Data Items
The data shown in Table 1 were obtained independently by 2 authors keeping in mind the article’s inclusion and exclusion criteria.
Bases on Which Study Was Examined and Assessed
Criteria on Which the Study Was Selected
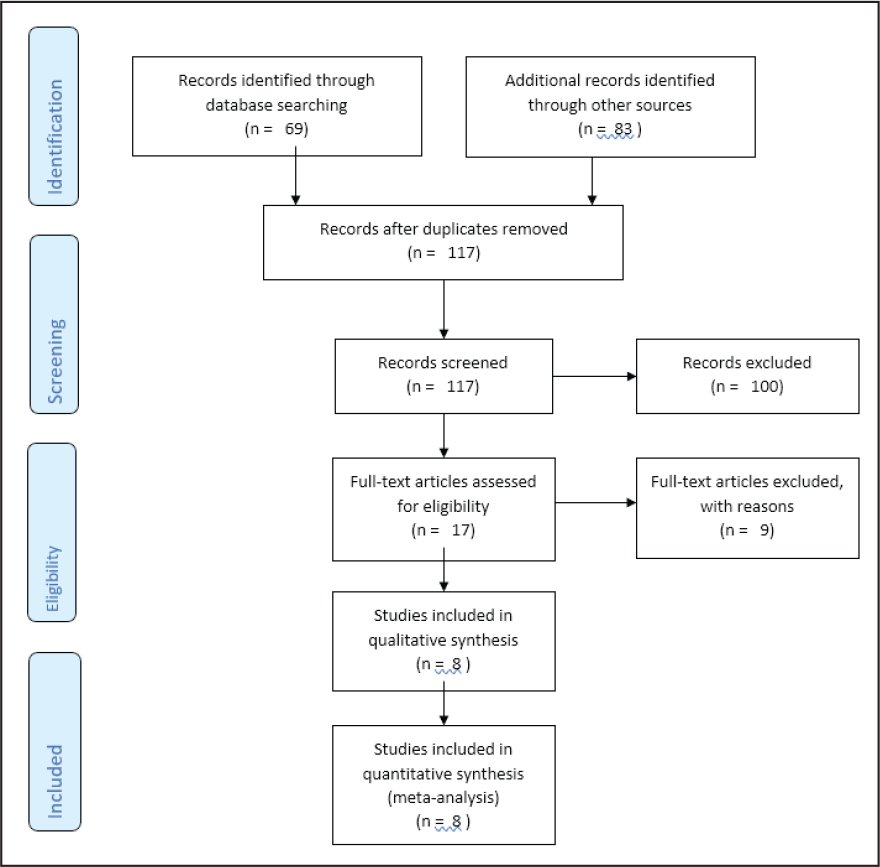
Article Selection and Elimination Flowchart
Statistical Analysis
The data thus obtained were subjected to statistical analysis using the forest plot. Descriptive statistical test like the standard mean difference on the 95% confidence interval was done using the RevMan software. Χ2-based Q-statistic method and i2 index were used to detect and assess the heterogeneity, but due to Q-statistic moderate insensitivity, only an i2 index of 50% was considered to be related to considerable heterogeneity amongst studies.
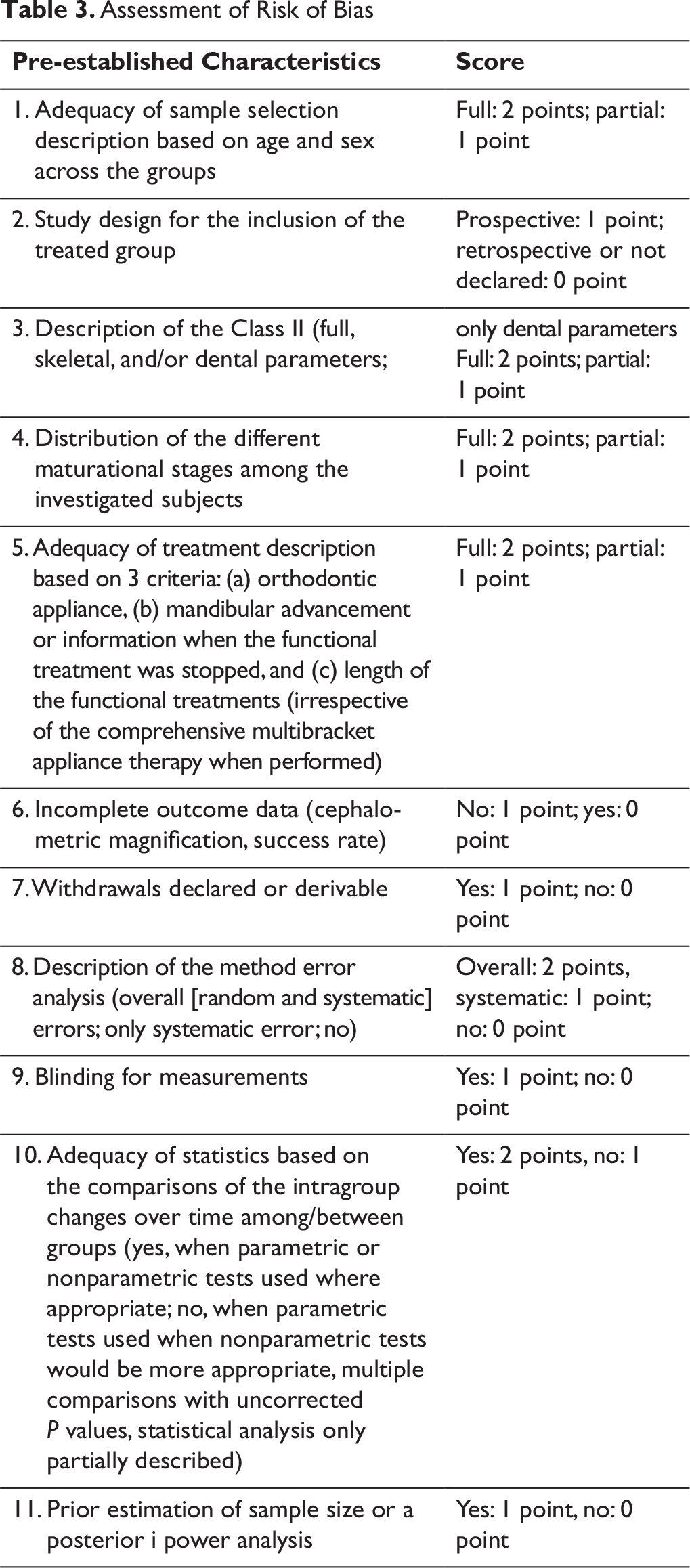
Assessment of Risk of Bias in Individual Studies and Across Studies
Heterogeneity was evaluated using the x2-based Q-statistic method and i2 index; however, due to the partial insensitivity of the Q-statistic, only an i2 index of 50% was treated as associated with a considerable heterogeneity. The χ2 was also calculated for the same. Risk of bias for individual studies was appraised (independently by 2 authors) following pre-established characteristics, along with the scores that were allocated to the individual retrieved articles mentioned in Table 3. The quality of the studies, with a maximum possible score of 17, was considered as follows:
Low: final score ≤7 Medium: final score >7 and ≤10 Medium/high: final score >10 and ≤14 High: final score >14.
Assessment of Risk of Bias
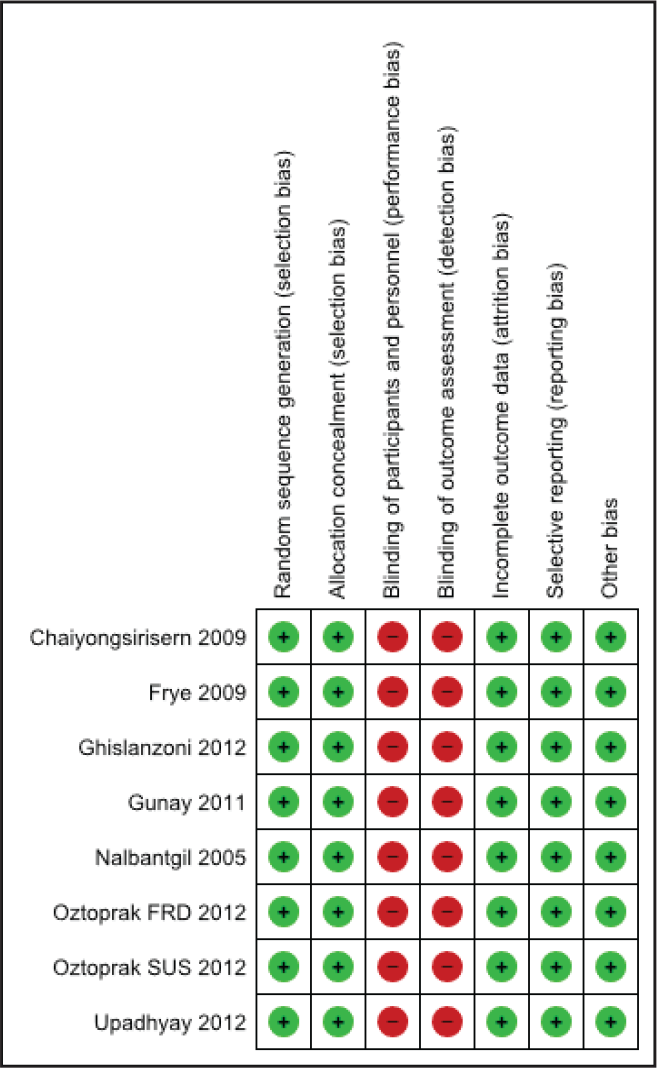
The evaluated fields are as follows: sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data addressed (attrition bias), selective outcome reporting (reporting bias), and other bias.
Risk of Bias Table According to the Review Manager by Cochrane Community
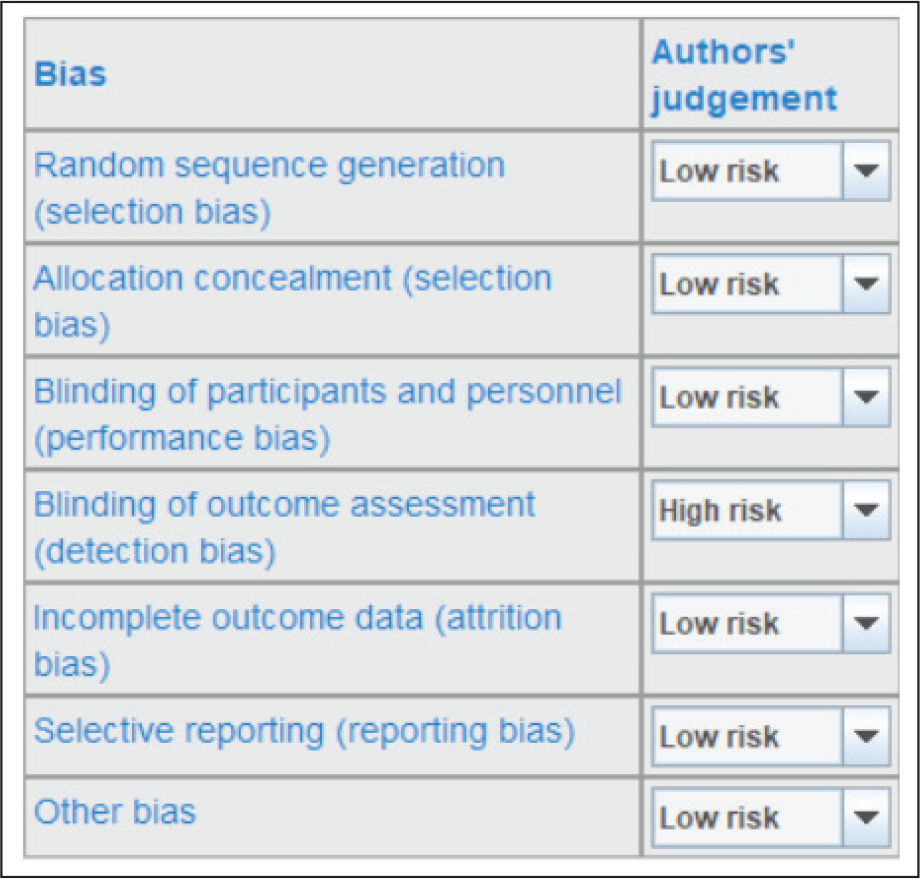
The overall risk of bias of the included trials was assessed according to the following: low risk of bias: if all fields were evaluated as at low risk of bias (bias improbable to change the results critically); unclear risk of bias: if at least 1 or more fields were assessed as at unclear risk of bias (bias carries some doubt about the results); and high risk of bias: if at least 1 or more fields were evaluated as at high risk of bias (bias critically affects the results) (excluded from the primary analysis). This risk bias is displayed in Figure 3 with color coding (green: low risk; yellow: unclear risk; and red: high risk).
Assessment of Risk of Bias by RevMan
The Final Studies Selected
Results
The changes brought about by the FFA was evaluated broadly in the following 3 categories:
Skeletal Dental Soft tissue.
The skeletal changes were evaluated based on the changes brought about in the following cephalometric parameters:
Sella-Nasion-Point A (SNA) angle Sella-Nasion-Point B (SNB) angle Point A-Nasion-Point B (ANB) angle Sella-Nasion-mandibular plane (SN-MP) angle Palatal plane-mandibular plane (PP-MP) angle
The dental changes were evaluated based on the changes brought about in the following cephalometric parameters:
Incisor mandibular plane angle (IMPA) Interincisal angle Overjet Overbite Li-NB (mm)
The soft-tissue changes were evaluated based on the changes brought about in the following cephalometric parameters:
H angle Nasolabial angle E line to upper lip E line to lower lip N-A-Pog
Following are the respective forest plots with their respective tables of data (Figures 4-18 and Tables 5-19).
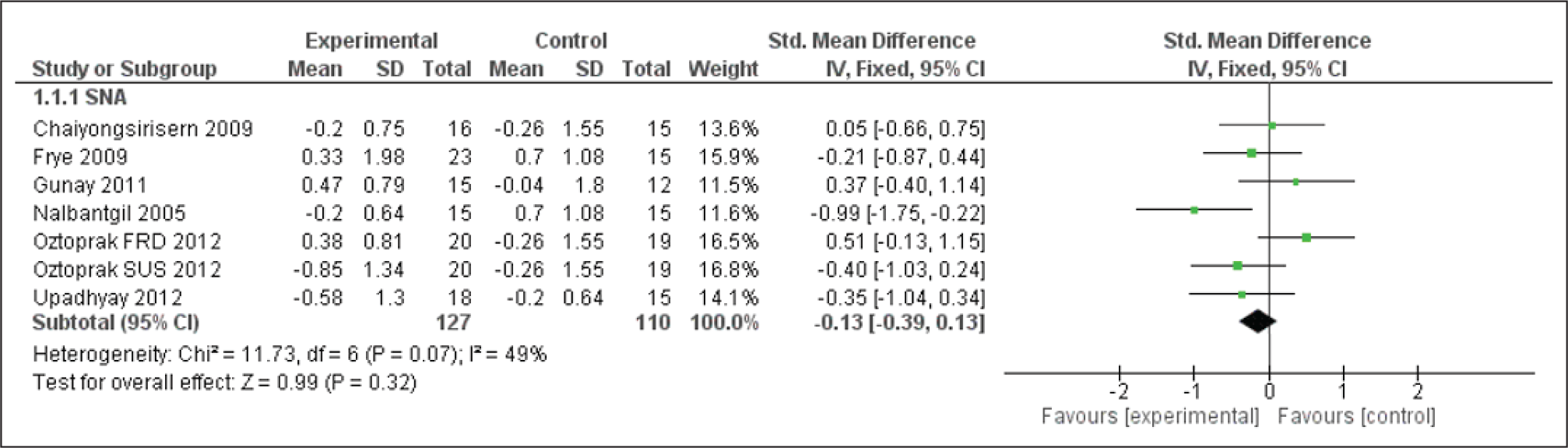
Forest Plot for the SNA Angle
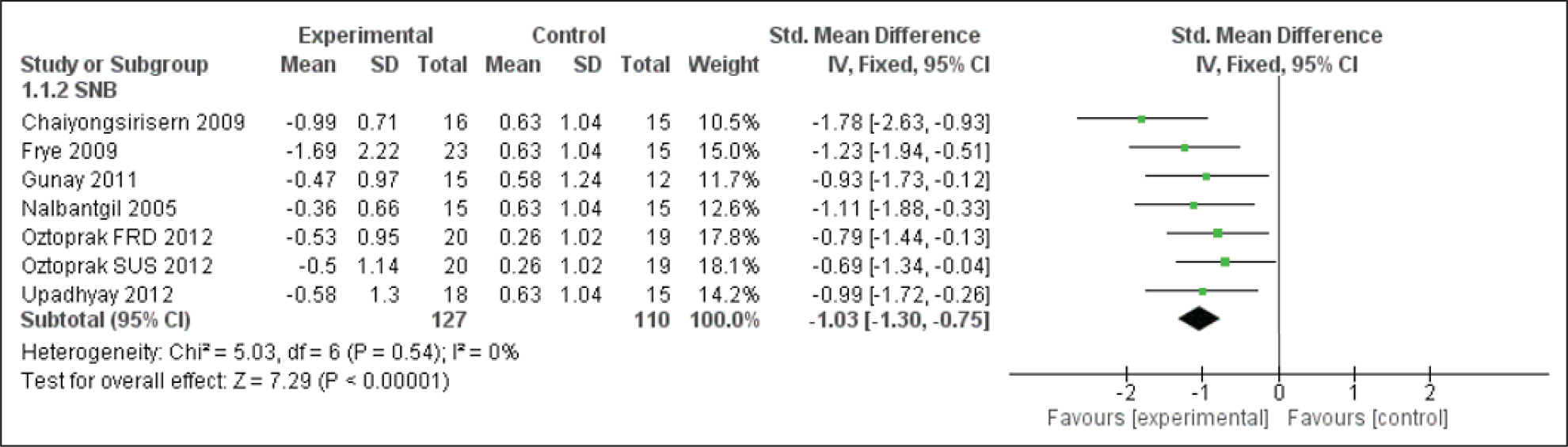
Forest Plot for the SNB Angle
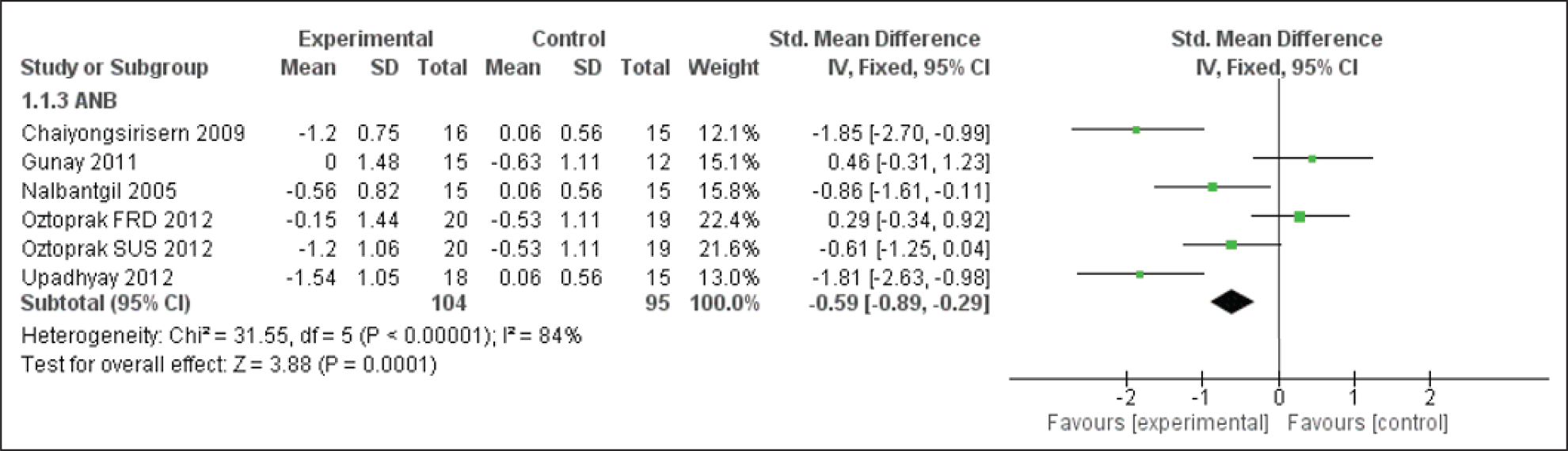
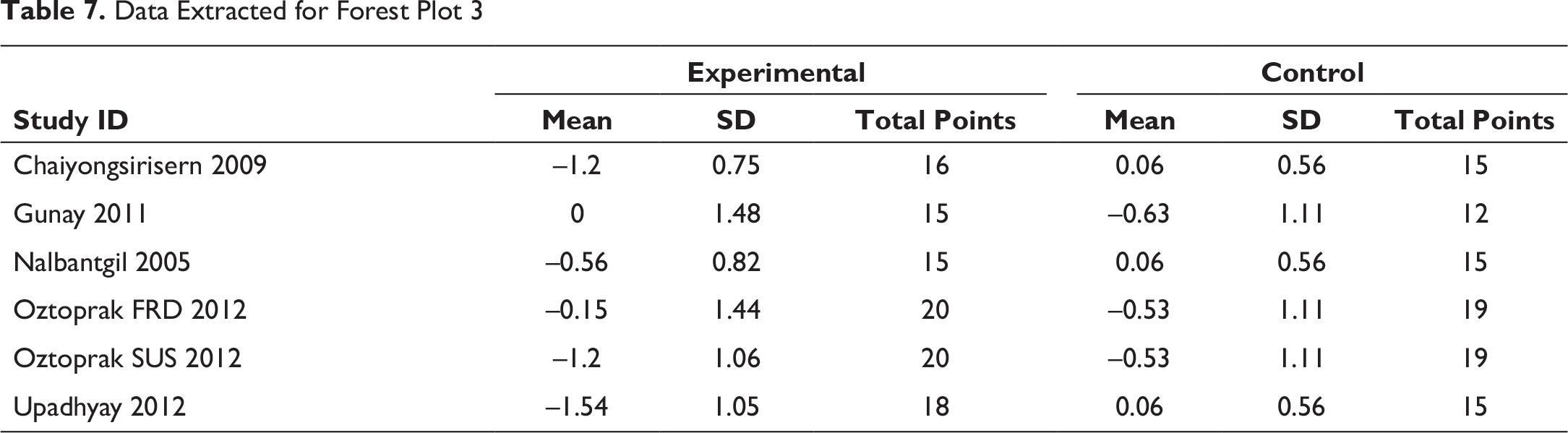
Forest Plot for the ANB Angle
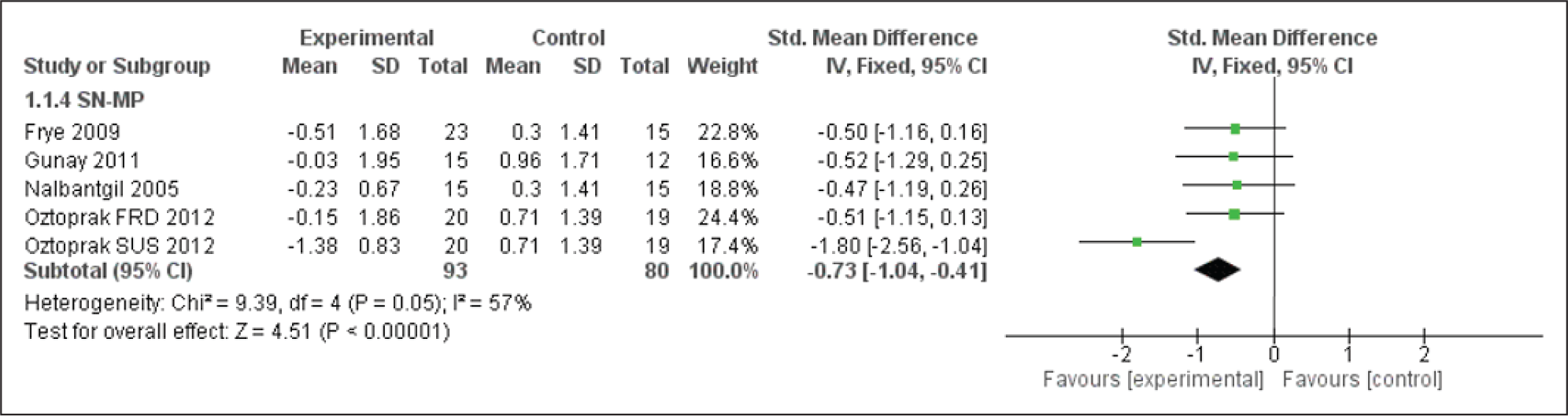
Forest Plot for the SN-MP Angle
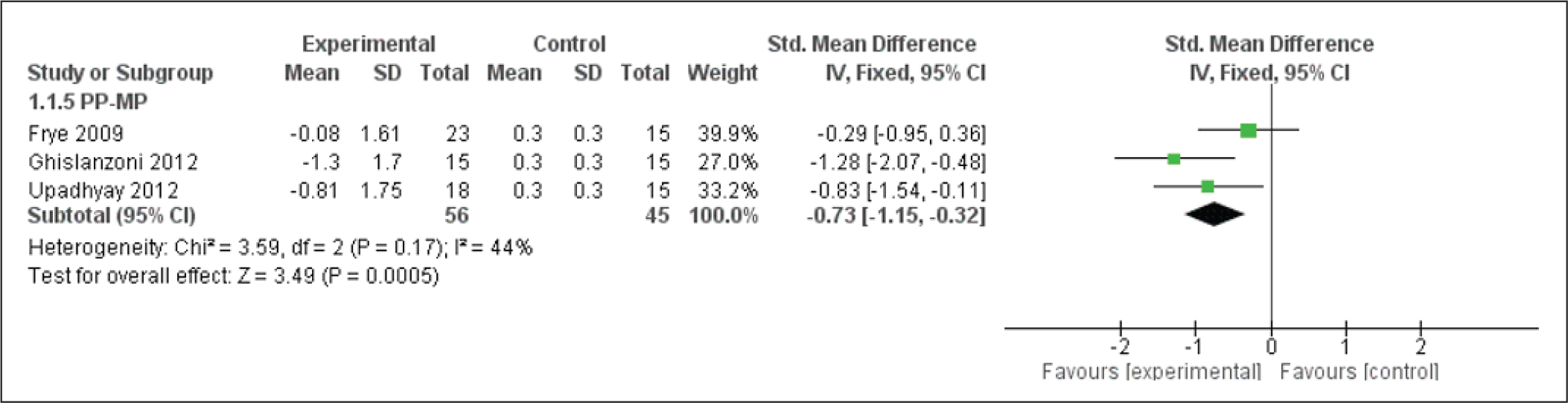
Forest Plot for the PP-MP Angle
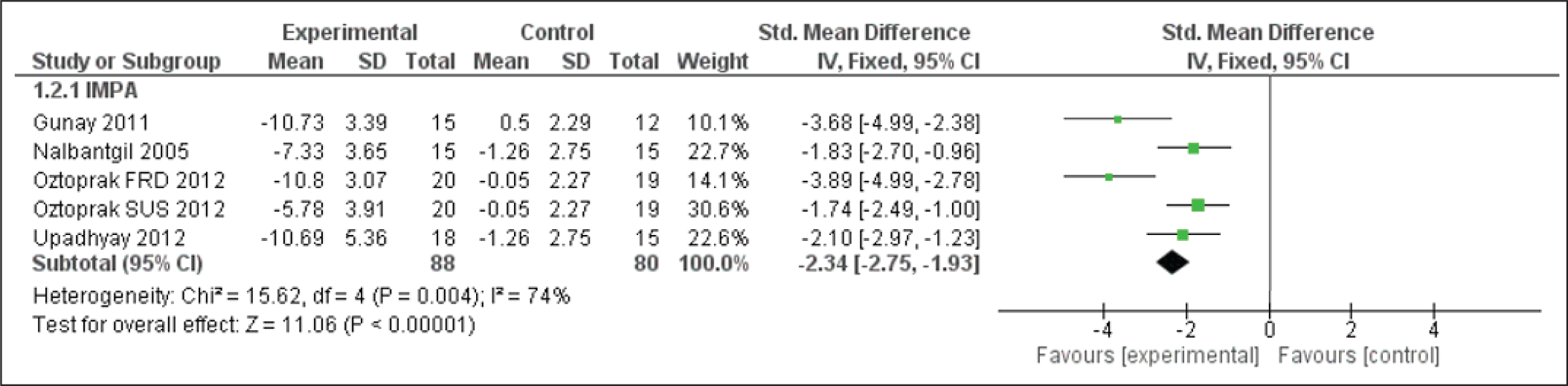
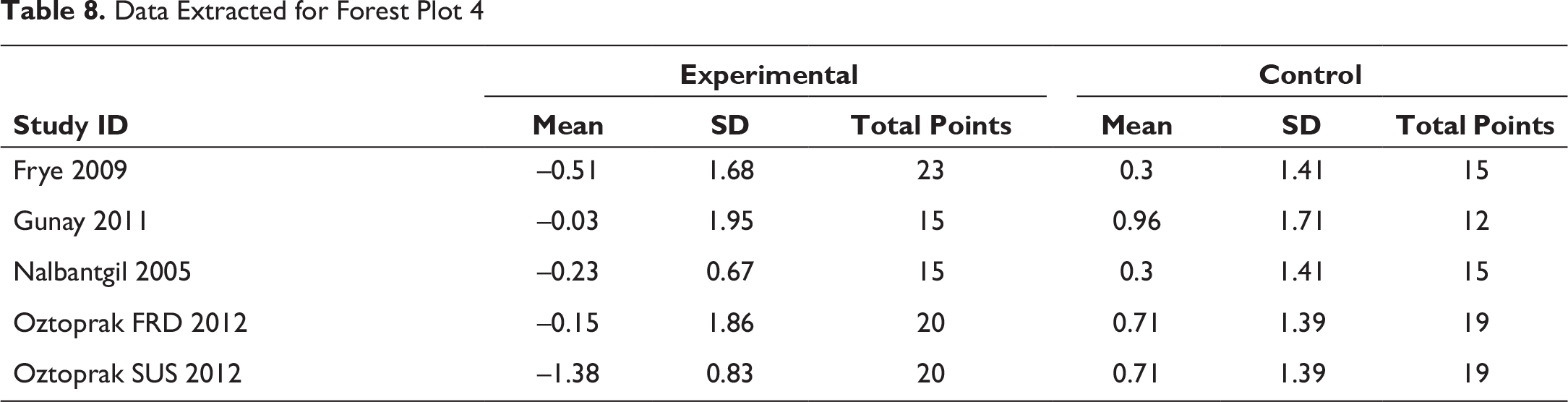
Forest Plot for the IMPA Angle
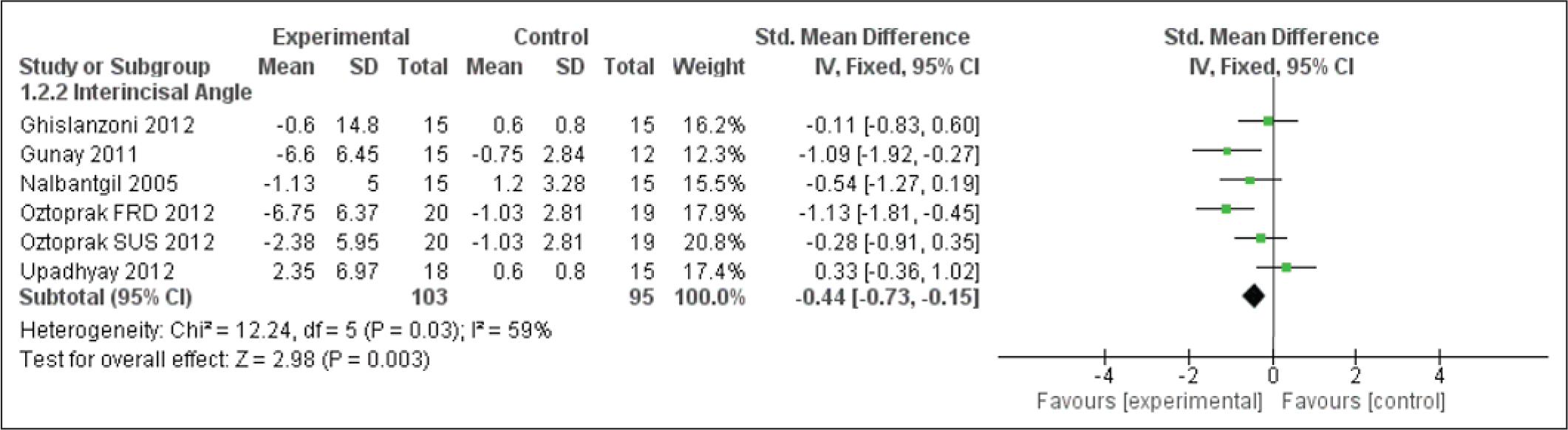
Forest Plot for the Interincisal Angle
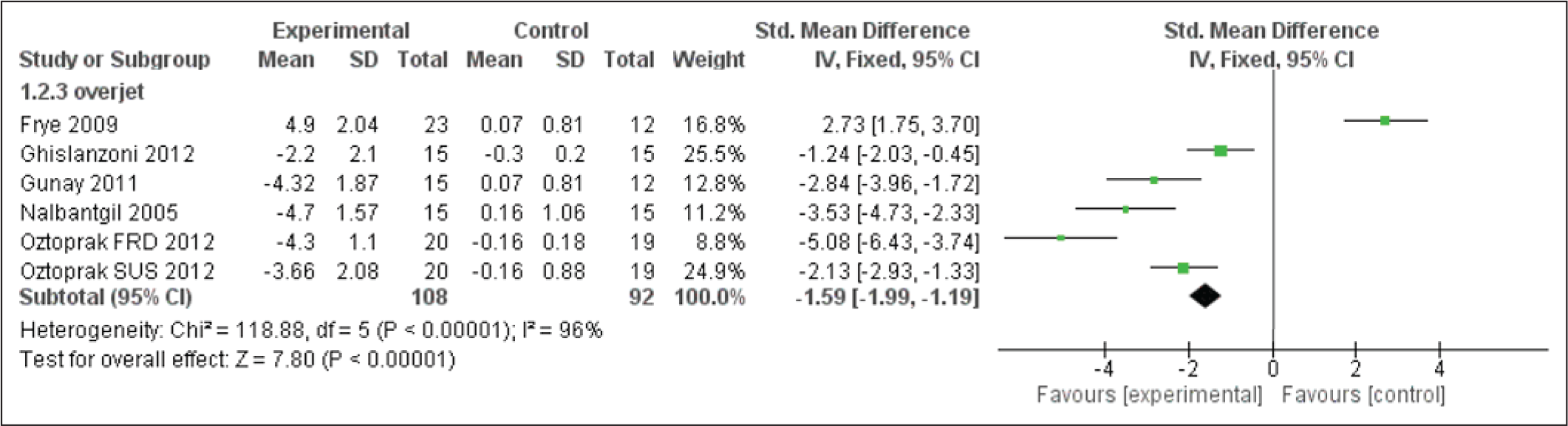
Forest Plot for Overjet
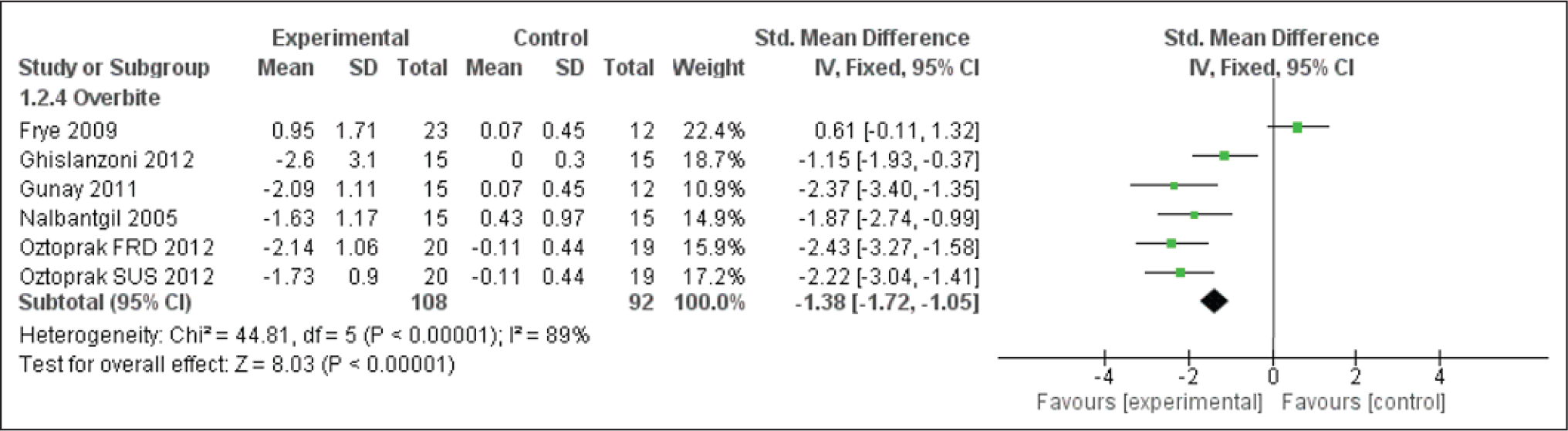
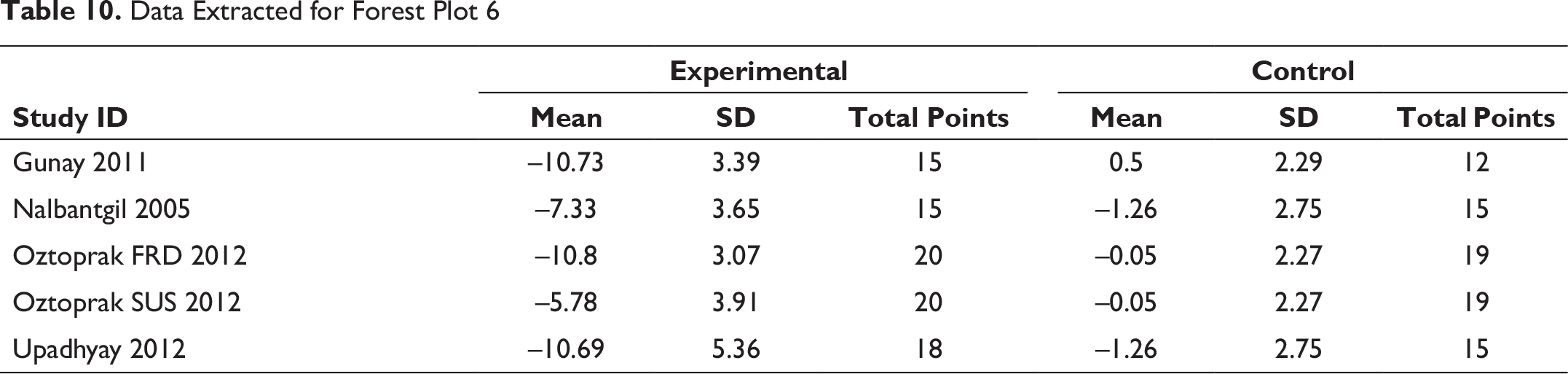
Forest Plot for Overbite
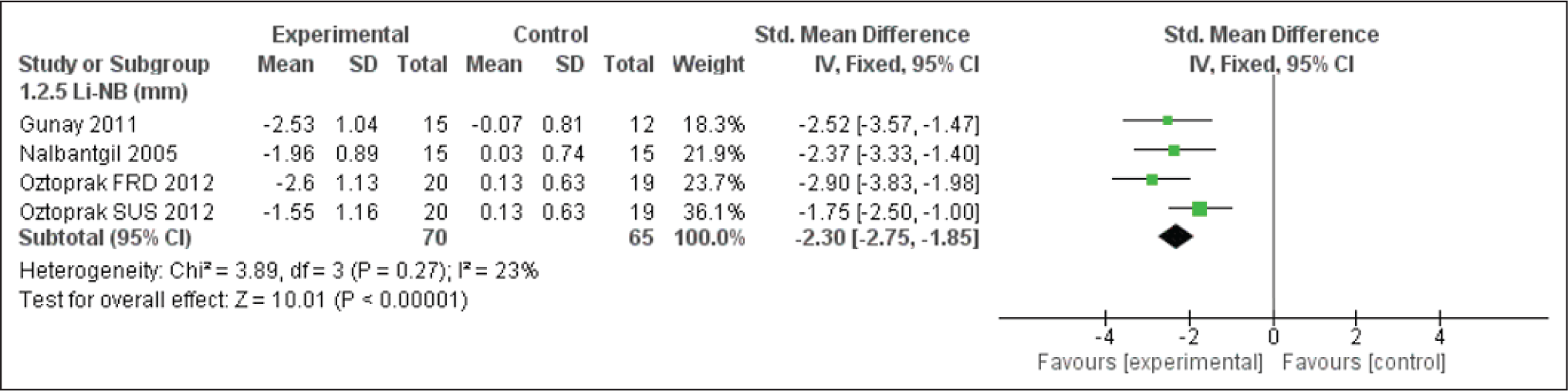
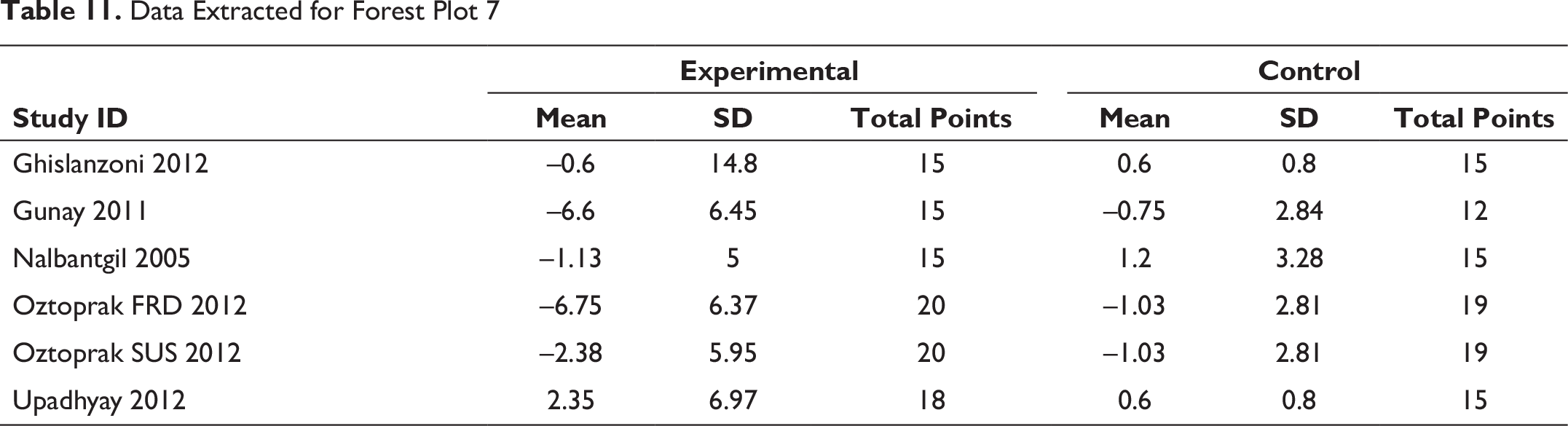
Forest Plot for Li-NB
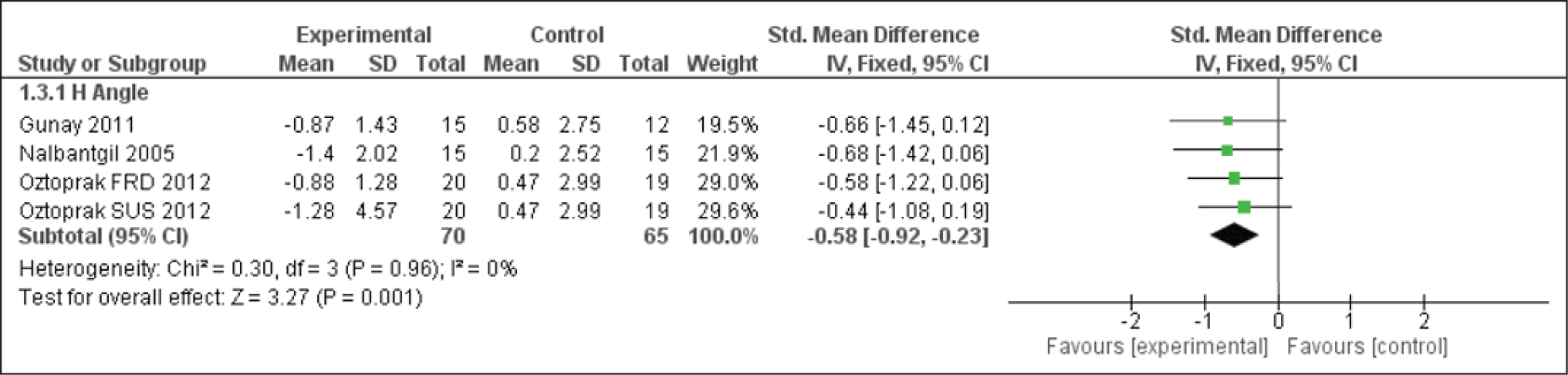
Forest Plot for the H Angle
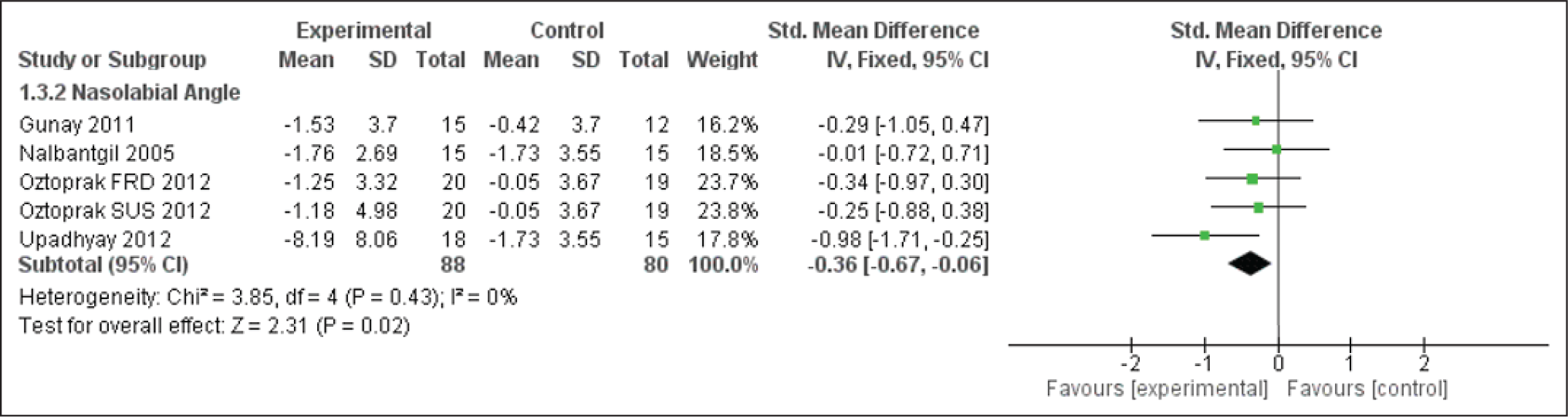
Forest Plot for the Nasolabial Angle
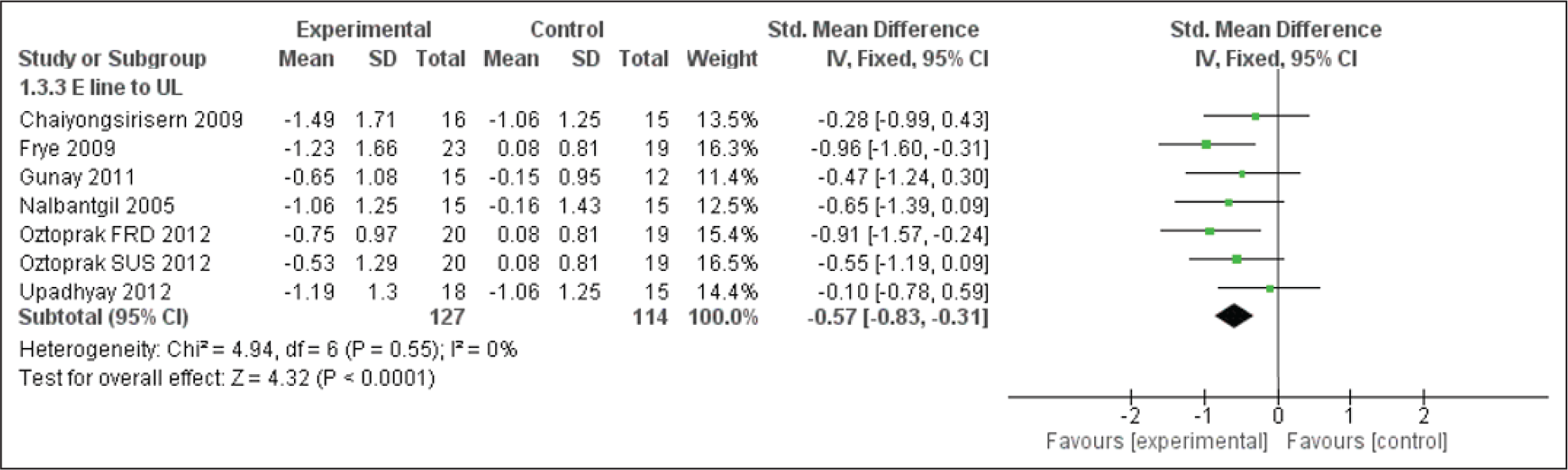
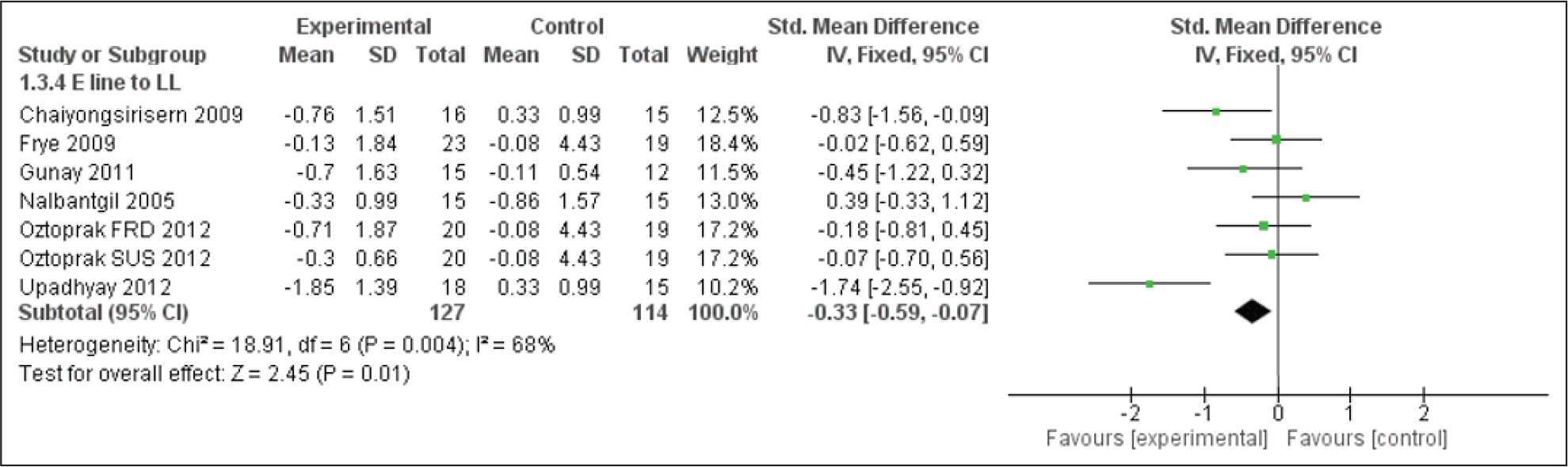
Forest Plot for the E Line to the Upper Lip
Forest Plot for the E Line to the Lower Lip
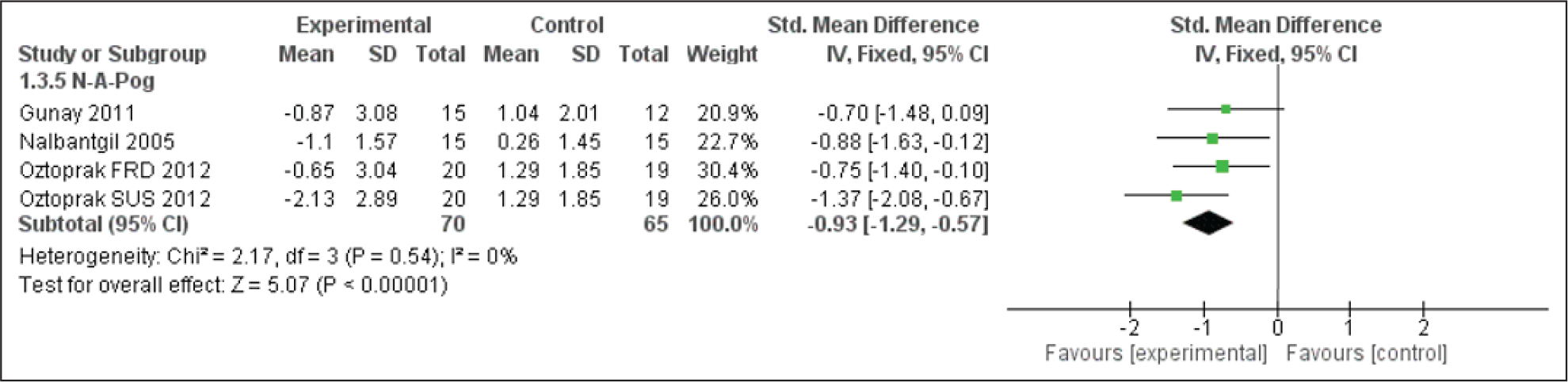
Forest Plot for N-A-Pog Angle
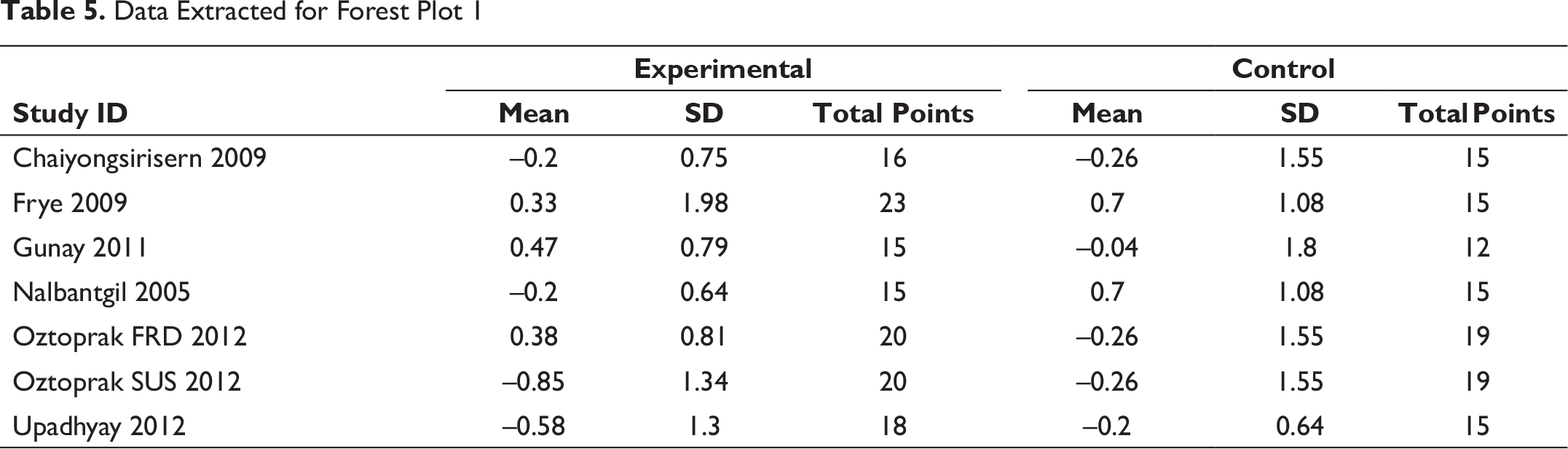
Data Extracted for Forest Plot 1
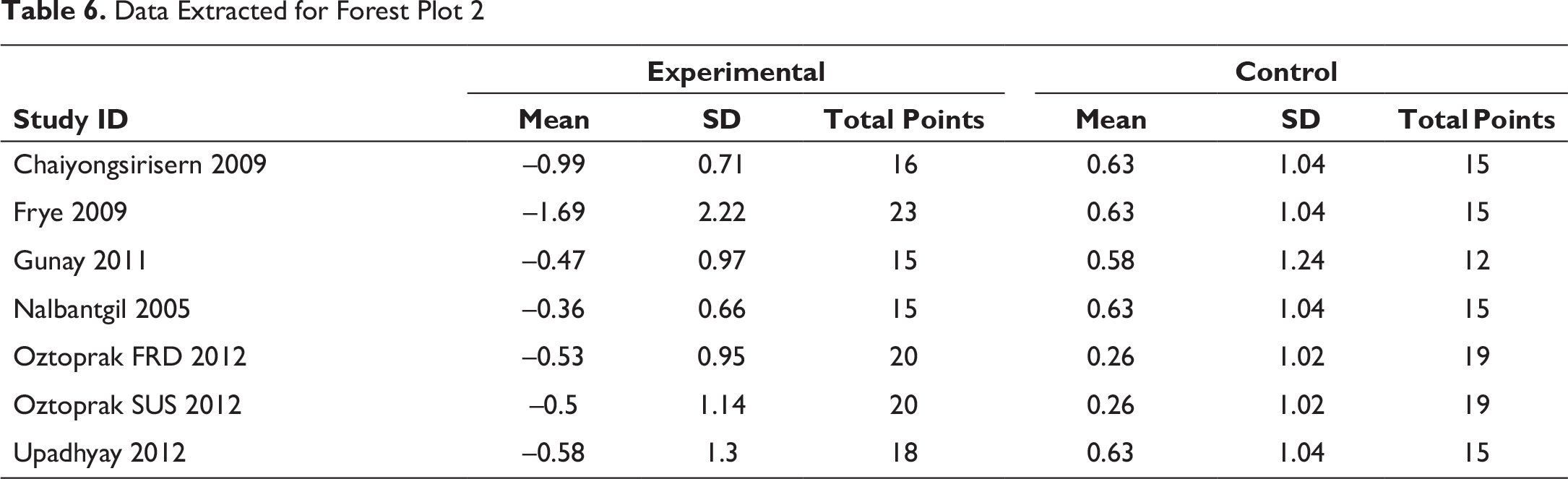
Data Extracted for Forest Plot 2
Data Extracted for Forest Plot 3
Data Extracted for Forest Plot 4
Data Extracted for Forest Plot 5

Data Extracted for Forest Plot 6
Data Extracted for Forest Plot 7
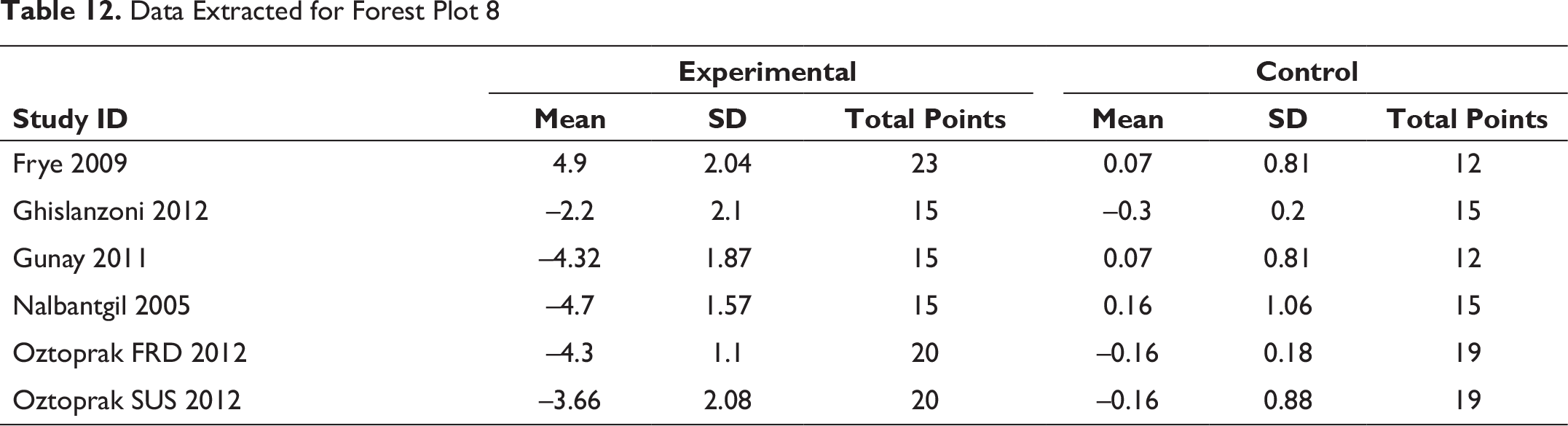
Data Extracted for Forest Plot 8
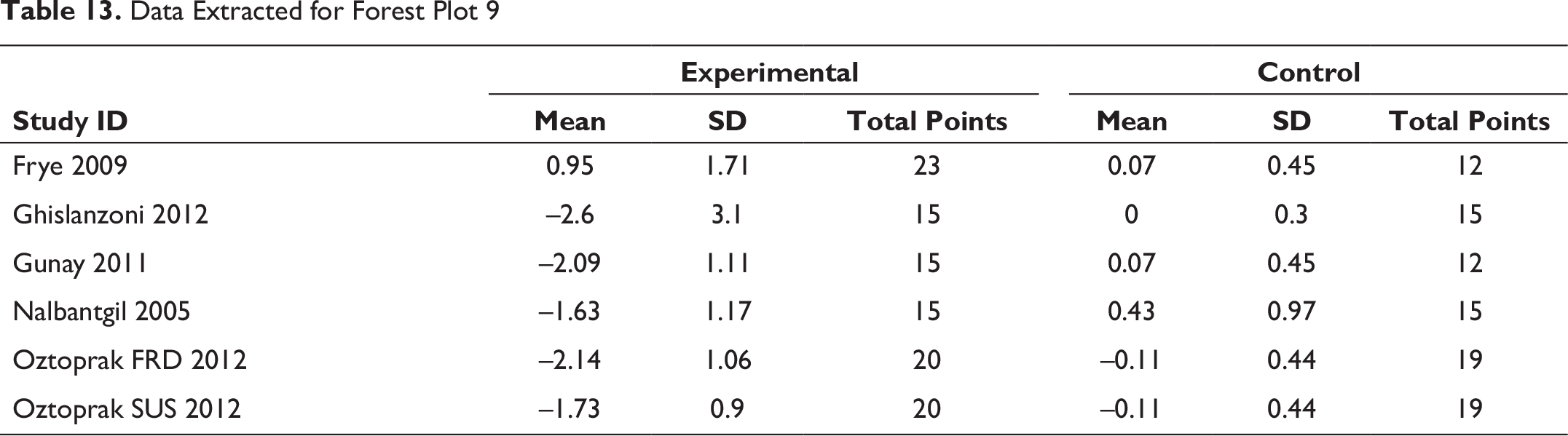
Data Extracted for Forest Plot 9
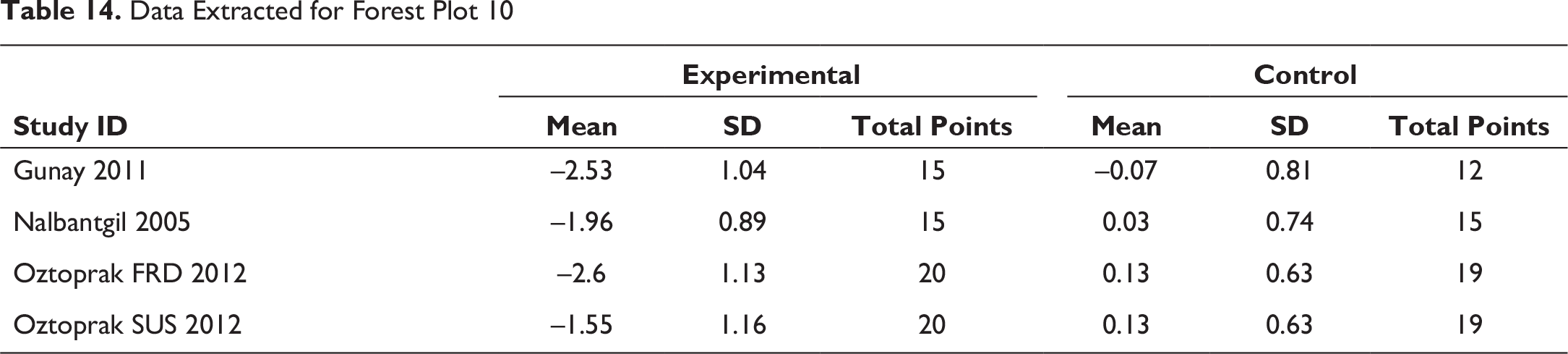
Data Extracted for Forest Plot 10
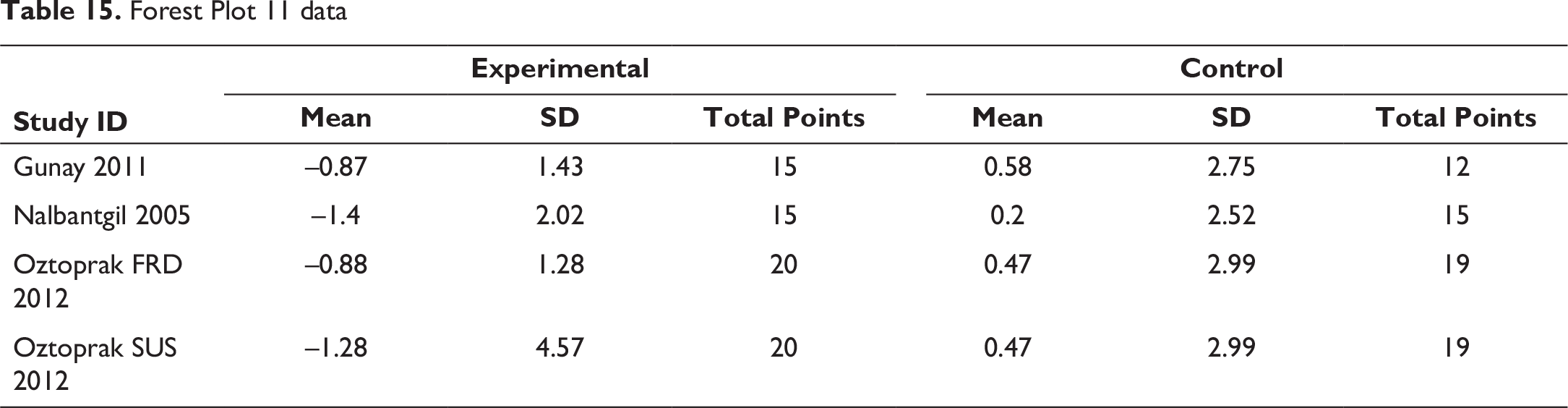
Forest Plot 11 data
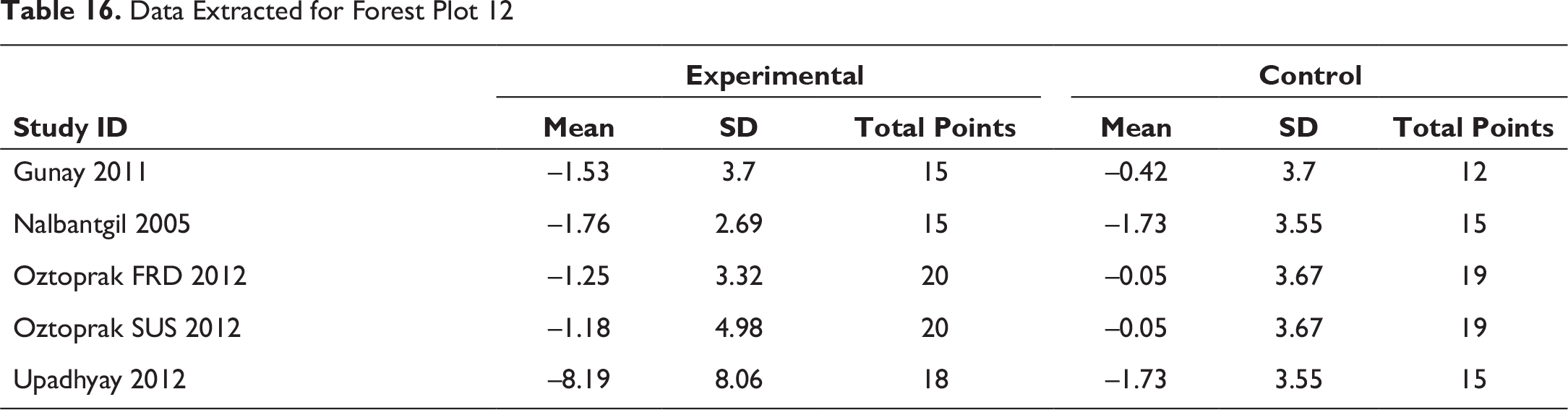
Data Extracted for Forest Plot 12
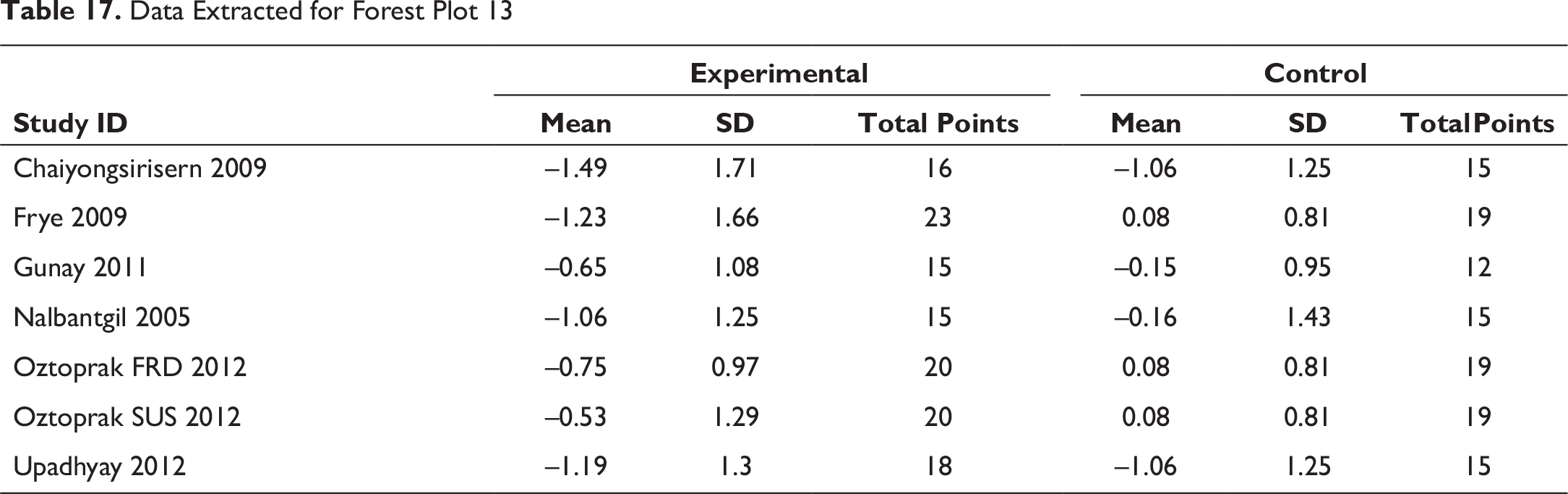
Data Extracted for Forest Plot 13
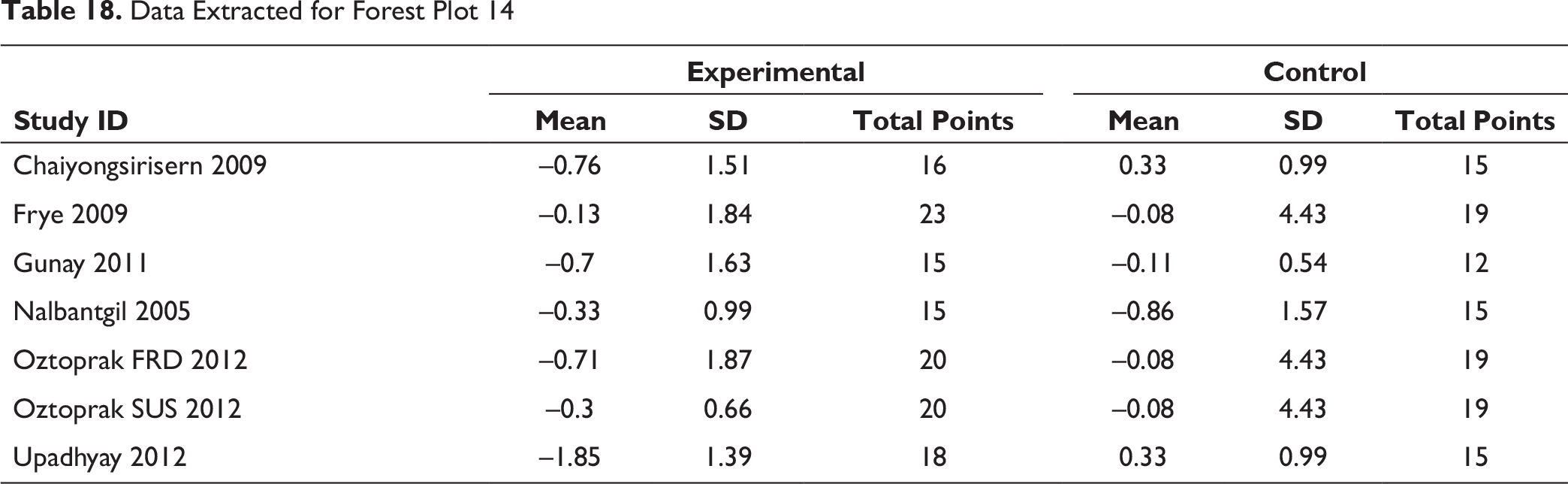
Data Extracted for Forest Plot 14
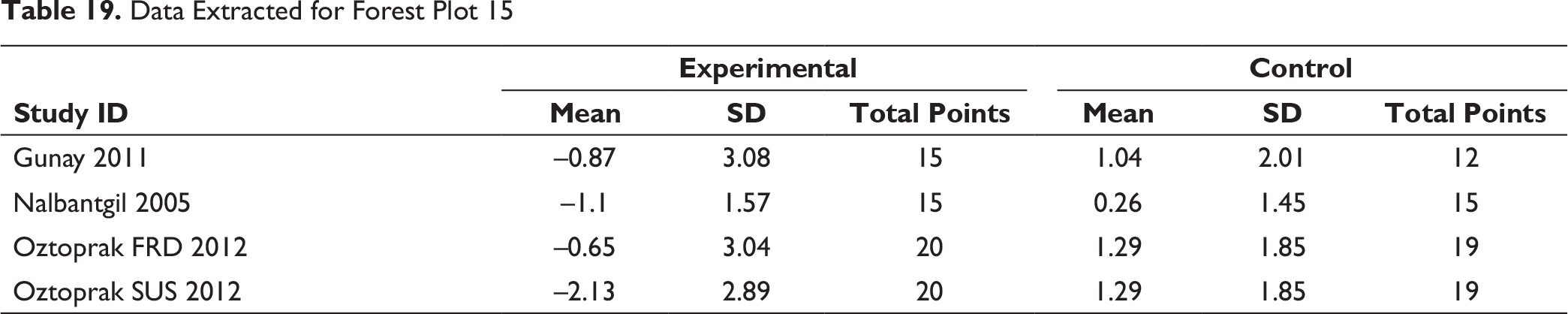
Data Extracted for Forest Plot 15
Risk of Bias Across Studies
Amid the various cephalometric parameters that were included in the analysis, only the SNA, SNB, SN-MP, PP-MP, interincisal angle, E line to upper lip, Li-NB, nasolabial angle, H angle, N-A-Pog, changes attained the acceptable level of heterogeneity (with i2 indexes 50% being medium and lower being low risk), whereas all of the other parameters yielded significant heterogeneity (i2 indexes generally above 60%). Therefore, meta-analysis was limited to the lower i2 index parameters.
Discussion
A major reason for the development of functional appliances was recognition that function had an effect on the ultimate morphologic structure of dentofacial complex. In order to deal with the noncompliance related to removable appliances, fixed functional therapy holds an upper hand and therefore has gained a lot of popularity. These appliances aim to bring the mandible forward into an anteriorly forced position so as to initiate or cause increased condylar cartilage growth as well as bring harmony to the skeletal defects.
Unfortunately, there have not been many studies on the effectiveness and efficiency of these appliances on treating adult or postpubertal patients, though it is a well-known fact that these have the ability to take advantage of the on-going growth during the prepubertal phase to correct the Class II skeletal base. Moreover, the existing studies provide with mixed conclusions; hence, this meta-analysis aims to provide with a single trustworthy conclusion.
The studies that were included were strictly seen to have performed treatment on bilateral Class II occlusion. Even though the strict inclusion and exclusion criteria were followed, large variations were still found in the hard- and soft-tissue measurements.
This meta-analysis has been conducted considering specific parameters to evaluate the changes brought about in the following 3 categories: skeletal, dental, and soft tissue. The studies were comprised of postpubertal or adult patients. This meta-analysis included data from 271 subjects (142 Class II patients and 129 untreated individuals/controls) from 8 RCTs, which assessed linear as well as angular cephalometric changes induced by Class II treatment with FFAs.
SNA Evaluation
The forest plot of SNA (Figure 4) depicted its pooled result, that is, the diamond in the control side, hence stating the intervention does not support the FFA therapy. Indicating there is not much changes caused to the position of maxilla because of FFA. 12
A study performed by Nalbantgil et al 11 analyzed the changes brought about by Jasper Jumper (American Orthodontics, Sheboygan, WI, USA) among patients of the mean age of 16.5 years, which reported to limited maxillary effect. Furthermore, negligible changes were seen starting from start to finish of the treatment. Still the authors11, 13 concluded that it may have the potential to restrict maxillary growth, though our meta-analysis confirms no such maxillary growth changes.
SNB and ANB Evaluation
In relation to the SNB and ANB angles, the conclusion made from fixed-effects meta-analyses indicates that FFAs have a statistically noteworthy involvement in the positive changes in the skeletal Class II relationship (Figures 5 and 6). The reason for the changes is that the functional appliance causes an increased contractile activity of the lateral pterygoid muscle. This in turn causes the intensification of the retrodiscal pad by repetitive activity (in the bilaminar zone). An increase in growth stimulating factors is also seen, that is,
Enhancement of local mediators Enhancement of local regulating factors.
This causes condylar cartilage to grow additionally along with subperiosteal ossification of posterior border of ramus. 13
Many studies have proved that FFAs move the entire mandible anteroinferiorly, with major parasymphyseal and midsymphyseal region displacement was appreciated. The mandibular dentition was displaced anteroinferiorly and especially in the incisor region; on the contrary, a posterosuperior displacement was seen in regard of the upper jaw. This displacement was seen to be more of dentoalveolar than skeletal. All dentoalveolar structures experience tensile stresses, except for the anterior nasal spine and the maxillary posterior teeth. Moreover, maximum tensile stress and von Mises stresses occurred in the condylar neck and head.13-17 Hence, the evident changes in the mandible positioning.
SN-MP and PP-MP Evaluation
There were significant changes seen with respect to SN-MP and PP-MP (Figures 7 and 8). The studies included showed an increase in this angle along with some mandibular advancement, which in turn resulted in reduced skeletal as well as soft-tissue convexity, though the convexity was noted to have increased with time in control.
IMPA Evaluation
Forest plot (Figure 9) shows a significant increase in the IMPA as the appliance tends to cause flaring of the lower incisor while pushing the mandible forward. This flaring should cause the inter incisal angle to close, that is, reduce, but posttreatment retroclined upper incisor causes the overall interincisal angle to increase. Hence, providing a more favorable interincisor angulation.
Interincisal Angle Evaluation
This angle shows evident changes, especially in cases of retroclined upper incisors and significantly proclined lower incisors, and therefore shows an increased angle. Hence, showing a forest plot of the intervention showing significant changes on the experimental side (Figure 10).
Overbite, Overjet, and Li-NB Evaluation
The appliances cause a reduction in overbite and the overjet encourages incisor inclination discrepancies. These overjet and overbite corrections are due to both forward positioning of mandible and inclination of upper and lower incisors (Figures 11 and 12). These also cause evident changes in the Li-NB values as shown in Figure 13. The study by Nalbantgil et al 11 found mesial tipping was seen in relation to lower molars, whereas upper molar displayed distal tipping and intrusion. A clockwise rotation seemed to be produced in both the jaws caused due to the dentialveolar effect.
Nasolabial Evaluation
A tremendous amount of soft-tissue improvement was seen to favor the profile. A statistically significant increase in the nasolabial angle was observed. Such changes overall helped in the reduction of facial convexity (Figure 15).
H Angle and E Line Evaluation
In response to the dentoalveolar changes produced by the FFAs, a decrease is observed in the E line and Holdaway angle (Figures 14, 16 & 17). The upper lip followed the upper incisors with a backward position. The lower lip was not any longer trapped behind upper incisors due to the proclined lower incisor and retruded upper incisors. Hence, a reduction in the E line to labialis inferior distance is observed.
N-A-Pog Evaluation
The N-A-Pog angle was observed to have improved reflecting a less convex profile (Figure 18). A study by Flores-Mir et al, 18 observed that soft-tissue changes were similar between growing as well as adult patients in nature as well as direction. Also, the facial profile enhancement was linked with upper lip retrusion but not as such with the forward lower lip.16, 18
Hence, significant soft-tissue changes were noted, reflecting the dentoalveolar changes that took place during fixed functional therapy.
Conclusion
The FFA provided adequate skeletal, dental, and soft-tissue changes for the Class II malocclusion.
The skeletal parameters such as SNB, ANB, SN-MP, and PP-MP supported the experiment over the controls, proving that FFAs do bring about skeletal changes even in postpubertal cases, though not much change was seen with respect to SNA.
There were significant dental changes that were concluded from changes in the IMPA, interincisal angle, overjet, overbite, and Li-NB on the completion of the fixed functional therapy.
There were substantial changes in the soft-tissue profile of the patient, that is, in the H angle, E line to upper and lower lips, nasolabial angle, and N-A-Pog.
According to stated evidence, the conclusions that can be drawn are as follows:
The treatment effects of FFAs on the skeletal tissues in patients with Class II malocclusion even after no potential growth was available were still significant to bring about angular as well as linear changes. FFAs allowed a small stimulation of mandibular growth, slight maxillary growth inhibition, but distinct dentoalveolar and soft tissue changes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.