
Abstract
Abstract
A proposal to formulate an orthodontic index specific for the Indian Board of Orthodontics (IBO) to determine the acceptability and degree of difficulty of a cases submitted for the phase III examination was discussed at the College of Diplomates meet (CDIBO). To ascertain the degree of difficulty of a case is very subjective; therefore, the need to quantify the complexity of a case in a standard format is required. To develop a Discrepancy Index for the IBO, 20 Dental and Cephalometric components of a malocclusion and 20 intraoral frontal photographs would have to be evaluated and a weightage score for each component would be assigned. Components such as upper and lower anterior proclination, commonly seen in our Asian population which have been omitted in the commonly used indices such as PAR (Peer Assessment Review) IOTN (Index of Orthodontic Treatment Need) and the ICON (Index of Complexity,Outcome and Need) have been included. The proposed IBO Index would add uniformity and standardization in assessing the degree of difficulty and also the degree of improvement of a case, which would be a beneficial tool for a fair evaluation.
Introduction
In orthodontics, it is important to objectively assess whether a worthwhile improvement has been achieved. It is unrealistic to expect all malocclusions to be treated to an ideal occlusion. The outcome of treatment is often dependent on many factors, for example, complexity of the case and the expertise of the practitioner. Individual assessment of the degree of improvement is very subjective, and the need for a standard protocol with uniform interpretation needs to be used. An essential factor to precisely grade the quality of orthodontic treatment delivered requires a standard mode of evaluation. An index formulated to grade is the standard method for such situations.
Presently, the current Indices commonly used to evaluate the case submitted for the phase III examinations are the peer assessment review (PAR), index of orthodontic treatment need (IOTN) and the index of complexity, outcome and need (ICON)1–3 index which have its own share of limitations.
All the three indices do not take into account the proclination of the anterior teeth, which is a very common malocclusion in our population. In the ICON index the lower arch is completely not taken into account, the molar relation correction which is also another important factor has not been taken into account, and the Aesthetic component is based on the European population. In the Par Index the, Aesthetic component has been ignored.
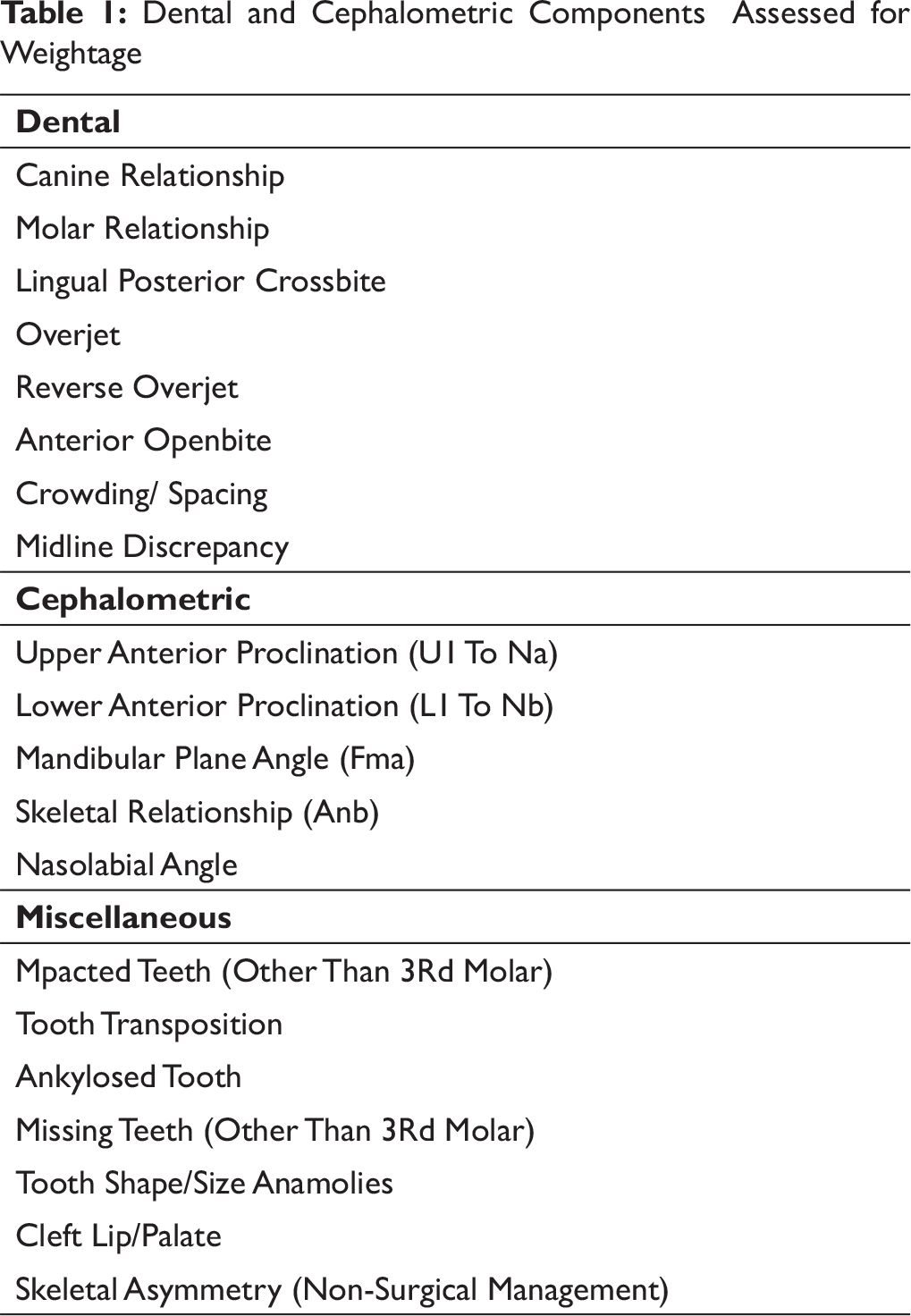
In our proposed index for IBO, to overcome these limitations, we give weightage to anterior teeth proclination and molar relation correction, as given in the table below (Table 1). Also, the need to formulate a new aesthetic index (AI), 20 frontal photographs of malocclusion commonly seen in our population was taken into our consideration (Figure 1).
Components in the Dental Index to be Assessed for Weightage
Dental and Cephalometric Components Assessed for Weightage
To give a weightage score separately for the dental and aesthetic components, a Google link was sent to each of the 109 Diplomates of the IBO. Each diplomate was to give a score of 1–10 for the degree of difficulty according to their own individual perception.
We then propose to do a statistical analysis and calculate an average score for each of the dental and aesthetic component to be evaluated. From the statistical analysis, we would also be able to assess the degree of improvement of a case.
Discussion
The need to formulate an individual index for the IBO was initiated because of the complexity in evaluating the degree of difficulty of cases in a standard format. Although categories 1, 11 and 111 have specified criteria for selection, in the categories 1V and V, the candidates are allowed to bring any case of their choice. It has been observed that some candidates bring very simple cases and get a good finish, whereas other candidates have cases with very high degree of difficulty and find it difficult to get a good finish, and this could bring about a bias in the evaluation.
The components for the dental index (DI) were selected because they represent most conditions that orthodontists treat. The 20 components were also chosen because all could be related to deviations from generally accepted norms and were also selected to match the malocclusions prevalent in our population. Another consideration was that the DI measurements could be done relatively quickly and simply.
Intraoral Frontal Photos Assessed to Determine the Aesthetic Component

Over the years, indices have been developed primarily to assess treatment need. Most of the indices record the treatment need, which is not the main objective of the IBO. The main need for the IBO was to develop a method to assist in selecting cases for the phase III examination that was related to the complexity of treatment and also to evaluate the degree of improvement.
Conclusion
The proposed IBO index would provide a single summary score for the dental and aesthetic components of a malocclusion. The score would provide an estimate of how far a case deviates from normal, and the difference in scores between pre and post treatment records reflects the degree of improvement and therefore the overall success of treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.