
Abstract
A new orthodontic index was proposed by the College of Diplomates to assess the degree of difficulty of cases submitted for the IBO Phase III clinical examinations. This article is the continuation of Parts I and II of the article, which gave a brief insight into the need and the methodology undertaken to formulate this index. A weightage score grading the degree of difficulty was formulated based on the Dental, Cephalometric, and Miscellaneous components. An Aesthetic component was also developed. Further statistical evaluation was done to formulate a cut-off score required for cases submitted for the Phase III examination. This index would help to categorize the malocclusion in a structured manner.
Introduction
A proposal to formulate an orthodontic index to determine the acceptability and degree of difficulty of cases submitted for the phase III examination was discussed at the College of Diplomates (CDIBO) meeting of the Indian Board of Orthodontics (IBO). This article is in continuation with Part I and II of the articles: Formulating a New Orthodontic Index: An Indian Board of Orthodontics Initiative. 1
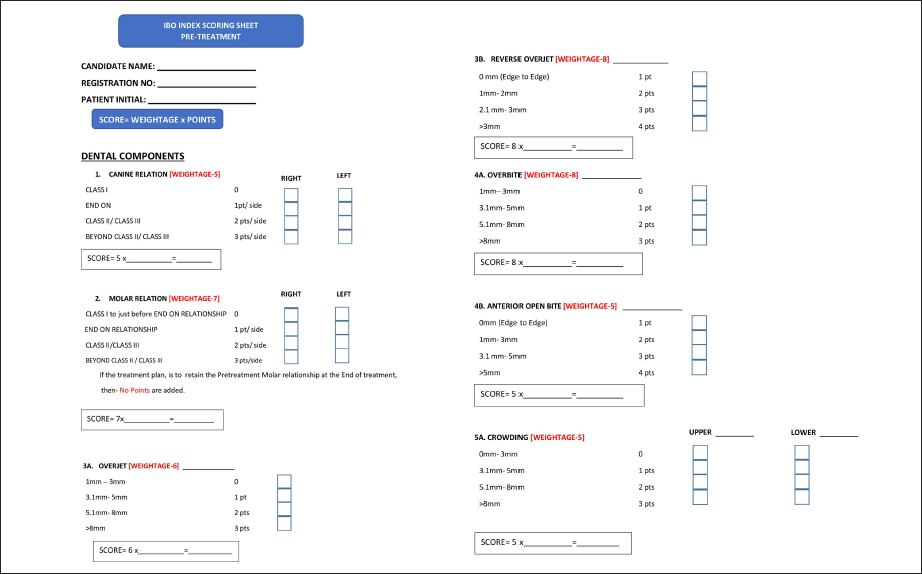
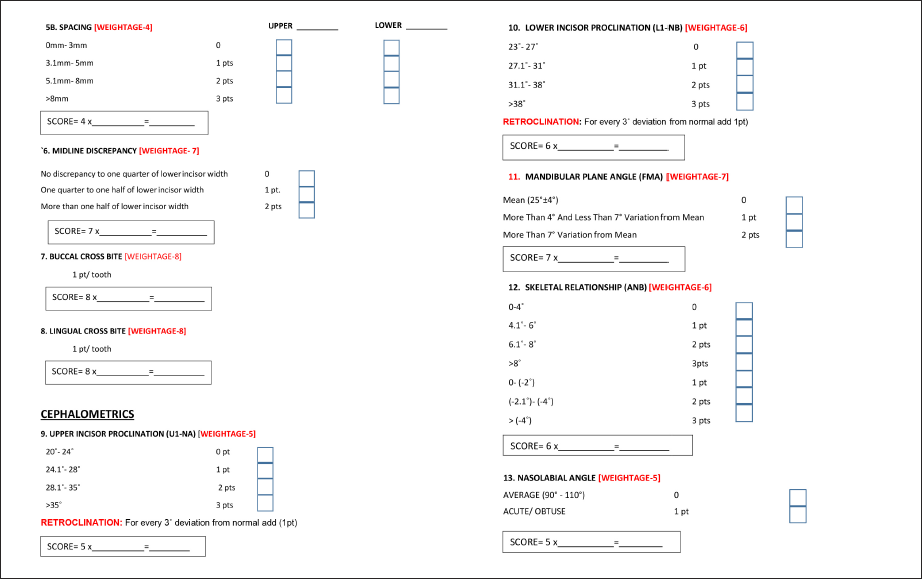
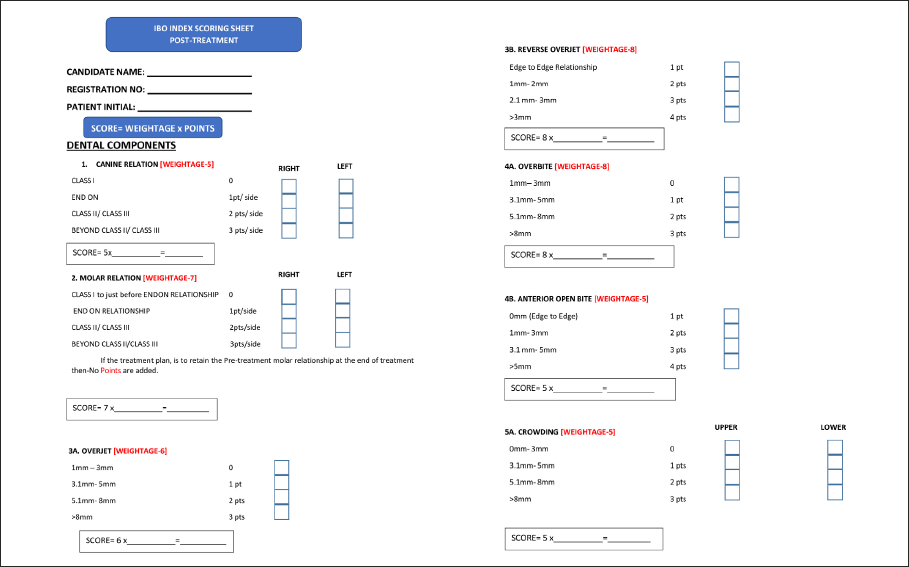
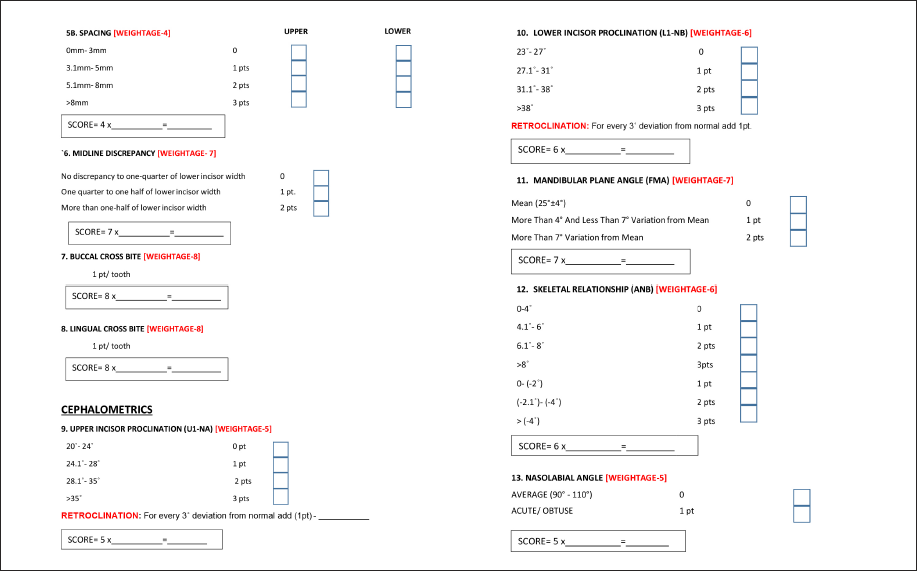
To develop the Discrepancy Index, 14 dental and cephalometric components of malocclusion were assessed. Frontal intraoral photographs were evaluated to assess the aesthetic component of the particular patient. After a survey among 109 IBO diplomates, a weightage score was assigned for each component of the malocclusion based on the degree of difficulty to manage the particular component of malocclusion. They were asked to rate each of the 14 components with a score ranging from 1 to 10, with the least difficult scored as 1 and the most difficult being placed with a score of 10. The value of a component multiplied by its weightage point provides the total score of the particular component. 2 This was similar to the earlier available indexes, such as the PAR and IOTN, but some changes have been made to overcome the limitations of the other available indices.3–5 The summation of the scores of all 14 components of the malocclusion gives us the overall score of the patient. The components were separated into Skeletal and Dental and are given below.
Materials and Methods
The 14 components assessed were as follows:
Canine Relationship
Molar Relationship
Overjet/Reverse Overjet
Over bite/Open bite
Crowding/Spacing
Midline Discrepancy
Buccal Posterior Crossbite
Lingual Posterior Crossbite
Upper Anterior Proclination (U1 to NA)
Lower Anterior Proclination (L1 to NB)
Mandibular Plane Angle (FMA)
Skeletal Relationship (ANB)
Nasolabial Angle
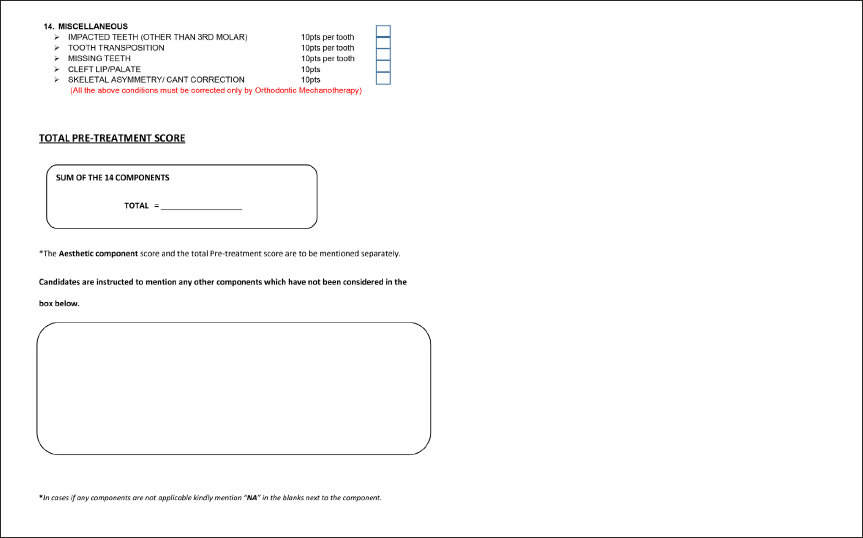
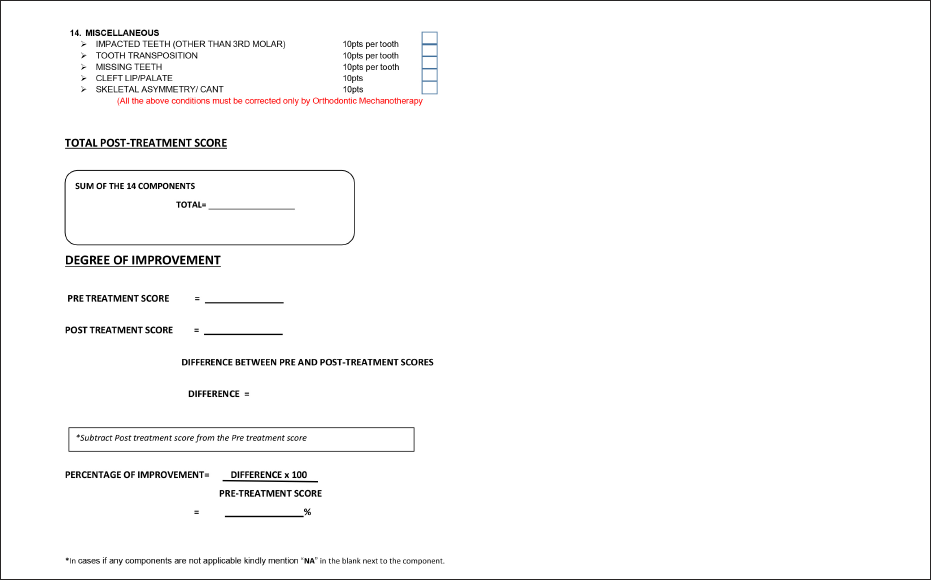
Miscellaneous
Impacted Teeth (Other than Third Molar)
Tooth Transposition
Missing Teeth (Other than Third Molar)
Cleft Lip/Palate
Skeletal Asymmetry (Nonsurgical Management)
After the compilation of the weightage score, the Board of Directors of IBO found a Discrepancy in the Weightage Score assigned for the Canine and the Molar relations. The Board then decided to re-evaluate the weightage score of the Canine and Molar relations with guidance from senior diplomates and the past chairmen of the IBO. The final weightage score for the Canine and Molar relationships was assigned as 5 and 7, respectively.
The total pre- and post-treatment scores can be calculated from the IBO index scoring sheets given at the end of this article. The difference between the pre-treatment and post-treatment scores can be used to assess the degree of improvement, from which the percentage of improvement could be calculated.
Formulating a Cut-off Score for IBO Examination
The next important aspect was to come to a consensus with regard to determining the minimum cut-off score required for a case to qualify for Category IV and V of the IBO Phase III examinations.
A total of 350 pre-treatment records were collected across India. The samples were collected across all parts of India to compensate for any confounding factors based on race and ethnicity. The records were divided into two groups. A separate category for bimaxillary protrusion cases, as it was predominately seen in the Indian population, and another group for non-bimaxillary cases was formed. Of the 350 cases selected, 30 were excluded because of insufficient records, and only the cases with sufficient records were included, as it will be essential for formulating the pre-treatment score.
Results
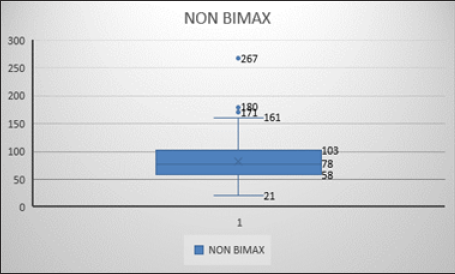
The values were tabulated, and statistics were carried out using SPSS software (IBM SPSS). The mean and standard deviation were derived for 43 bimaxillary cases and 277 non-bimaxillary cases. The descriptive statistics obtained from the study are shown in Table 1 and Figures 1 and 2. The mean score for the bimaxillary cases was 52.44 and the mean score for the non-bimaxillary cases was 83.22.
Descriptive Statistics of Bimaxillary and Non-bimaxillary Cases.

Chart Showing Statistics of Bimaxillary Cases.
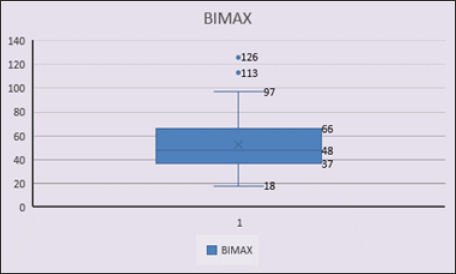
Chart Showing Statistics of Non-bimaxillary Cases.
Discussion
To compensate for the decreased cut-off score value, the board decided to give the bimaxillary cases an additional 30 points and round the minimum qualifying overall pre-treatment score to 80 for a case to be presented in Category IV and V of the IBO Phase III Clinical examinations.
Conclusion
The IBO Discrepancy and Aesthetic Index can be used as an indicator to determine case complexity, and the IBO is considering this option to measure the degree of difficulty of the cases submitted for the Phase III Clinical Examination. Due to its vast and reliable study methods, this Index can be used as a tool of assessment to categorize and classify any malocclusion and can also be used to study the percentage improvement of the case by using the pre-treatment score, post-treatment score, and the formula given in the post-treatment scoring sheet. The index will be continuously updated in the future, incorporating the valuable insights and recommendations from the board as we progress through our experiences.
Pre-Treatment Scoring Sheet
Post-Treatment Scoring Sheet
Footnotes
Acknowledgments
The Board would like to acknowledge the contributions of Dr Shobha Sundareswaran, Dr Nandini V. Kamat, Dr Elbee Peter and Dr Shakeel Ahmed V.K in formulating this index.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Not applicable.