
Abstract
A new orthodontic index was proposed by the College of Diplomates to assess the degree of difficulty of cases submitted for the Indian Board of Orthodontics Phase III clinical examinations. This article is the continuation of the part 1 article which gave a brief insight into the need and the methodology undertaken to formulate this index. A weightage score grading the degree of severity of a case was obtained for dental, cephalometric, and miscellaneous components based on the results of a survey taken from the Diplomates of the Indian Board of Orthodontics. An aesthetic component was also developed using photographs and the relative aesthetic score for every photograph was graded. This index would help to categorize the malocclusion based on the severity, in a single, linear, and transparent manner.
Introduction
The Indian Board of Orthodontics had constituted the need to ascertain the degree of difficulty of a case submitted for the phase III clinical examination. The need to formulate an index catered to the malocclusions presenting predominately in our ethnic population was ascertained. In the part 1 publication, we had given a broad insight on the need for an orthodontic index and discussed the drawbacks of other commonly used indices which did not take into consideration the malocclusions predominantly seen in our population. 1 Two surveys were taken separately by the Diplomates of the Indian Board of Orthodontics to grade (a) dental component (DC) and (b) aesthetic component (AC).
Both the surveys had questions regarding the basic information about the author including the name, email id, and the current position of the diplomates. The designation of the participant was asked to determine if there is any gross deviation between the diplomates who are private practitioners and the diplomates who are working or affiliated with an institution.
To give a weightage score separately for the DC and AC, each diplomate was to give a score of 1 to 10 for the degree of severity according to their individual perception with score 1 denoting the least degree of severity and score 10 denoting the highest degree of severity of the malocclusion. Out of a total of 109 diplomates in the Indian Board, we had 97 diplomates who had graded all the components of the survey.
Dental and Skeletal Component
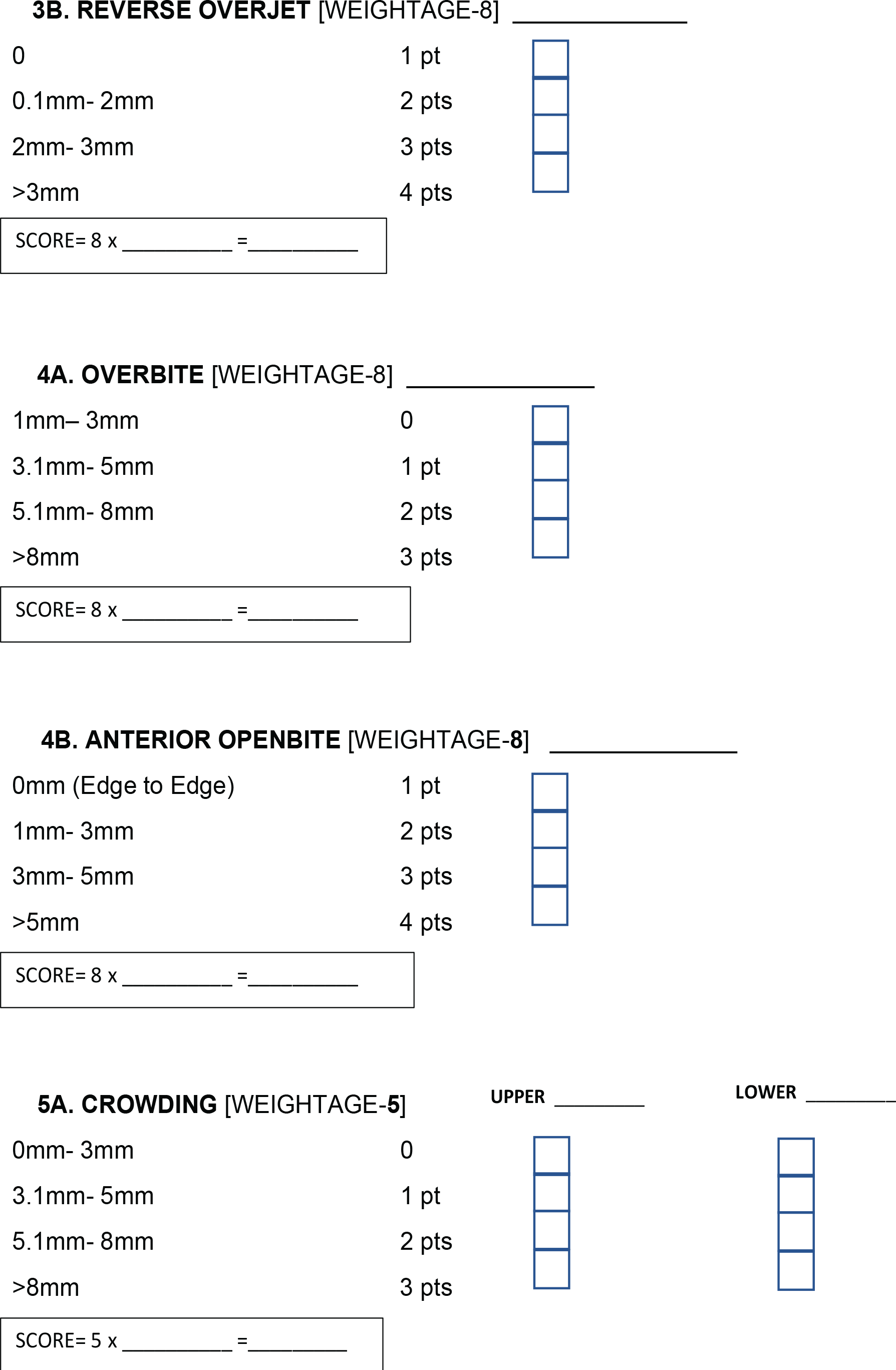
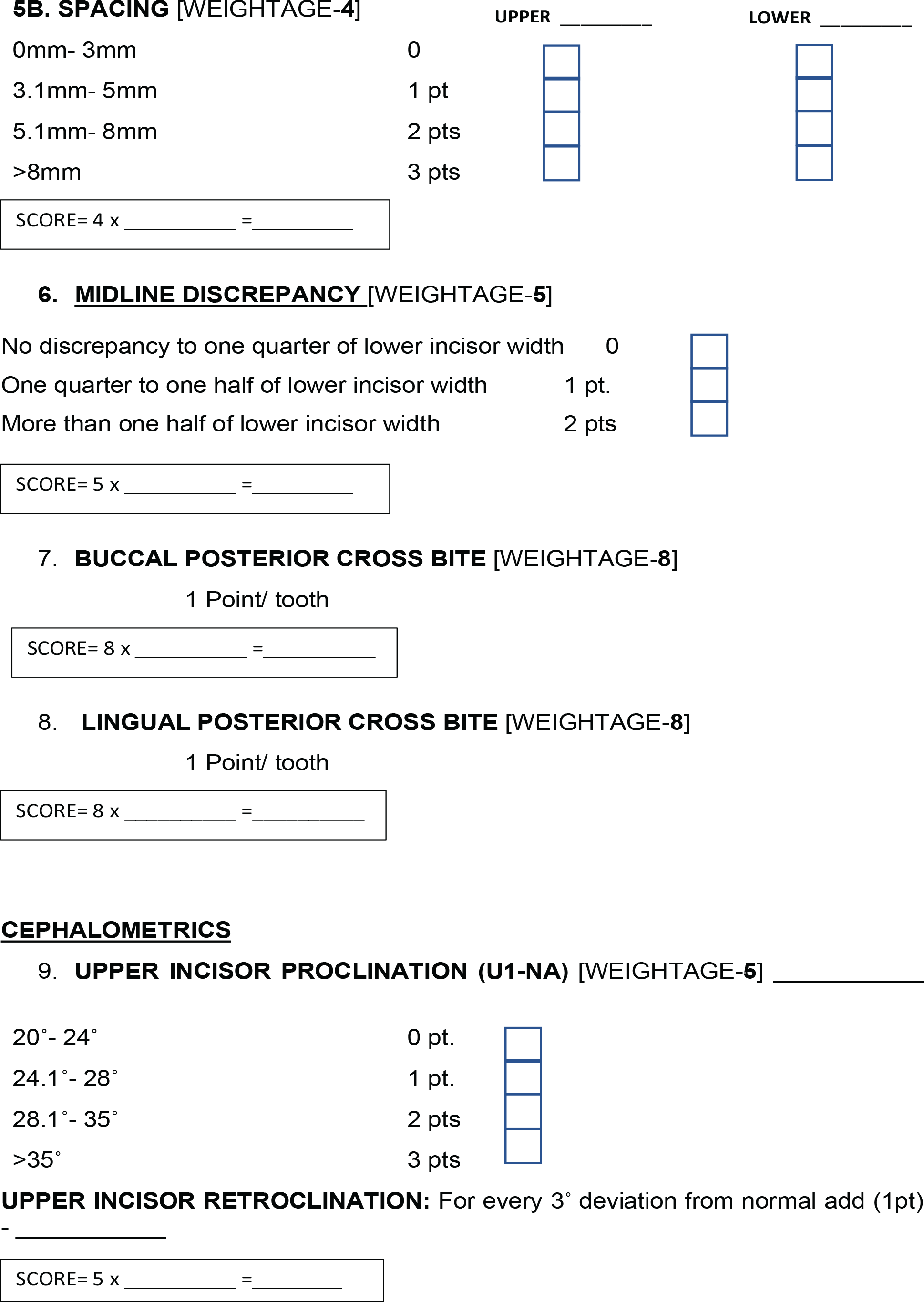
The dental, cephalometric, and miscellaneous components were scored in the survey. The participants were asked to score the components by determining the complexity of the malocclusion and how well these components influence the correction and stability of the malocclusion. The components that are included in the survey are given below.
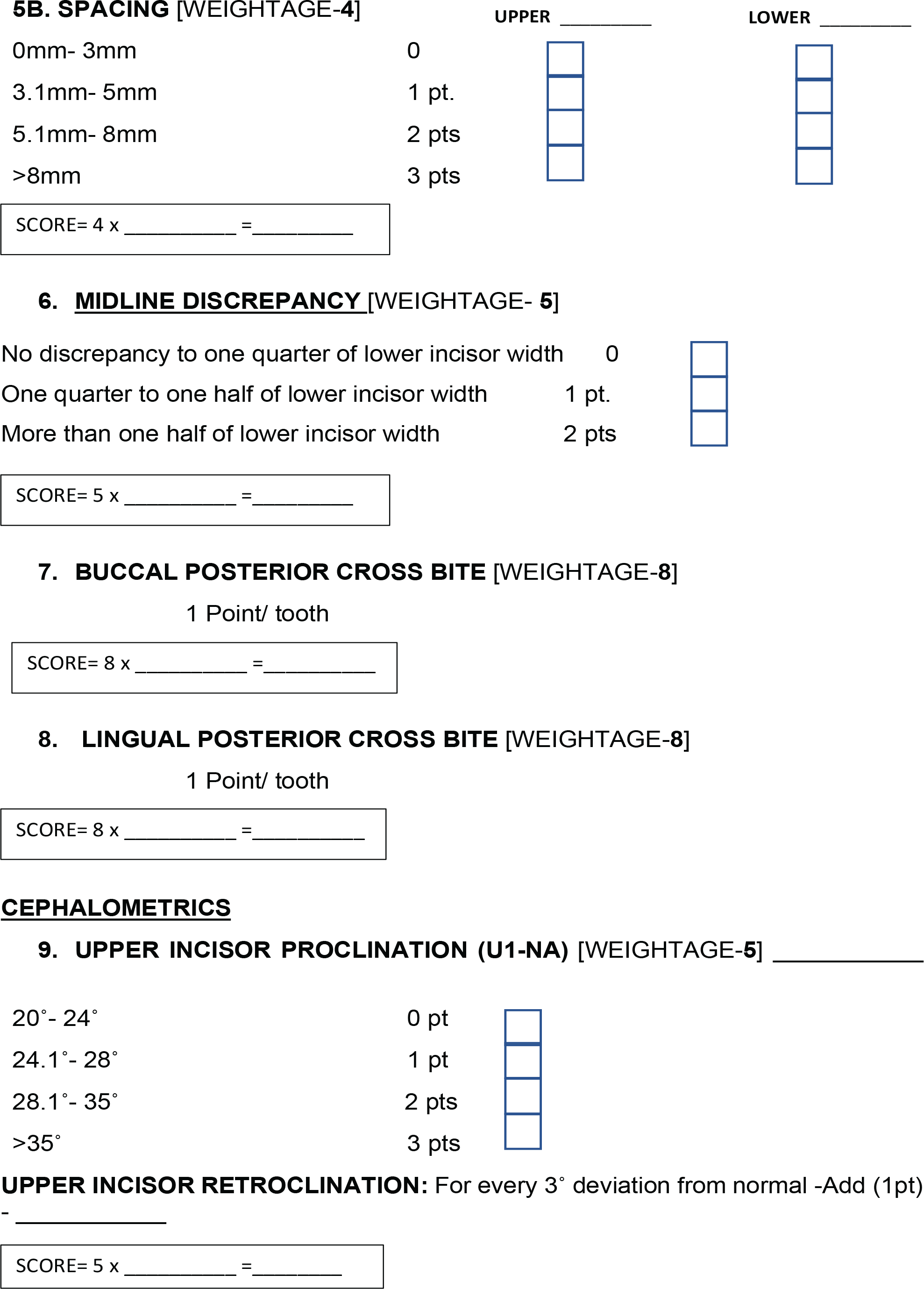
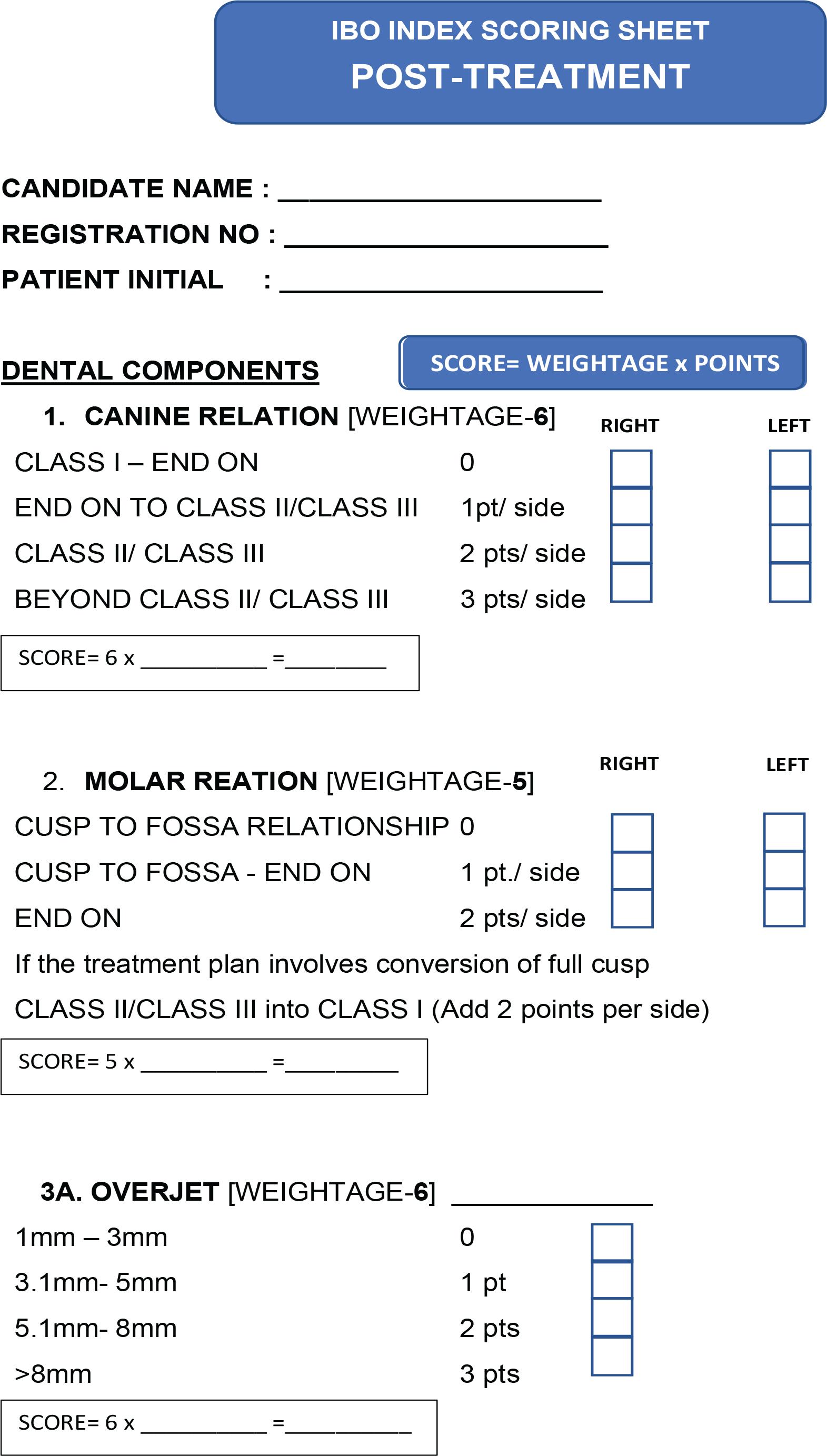
Canine Relationship Molar Relationship Overjet/Reverse Overjet Over bite/Openbite Crowding/Spacing Midline Discrepancy Buccal Posterior Crossbite Lingual Posterior Crossbite
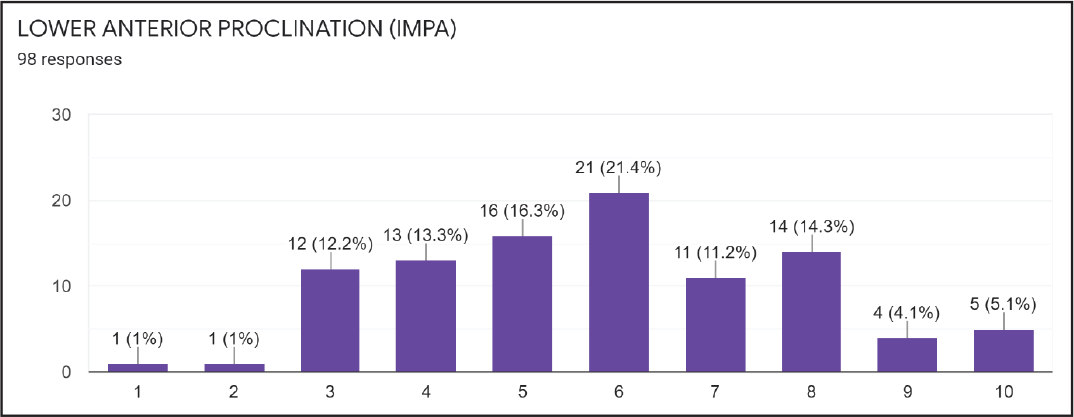
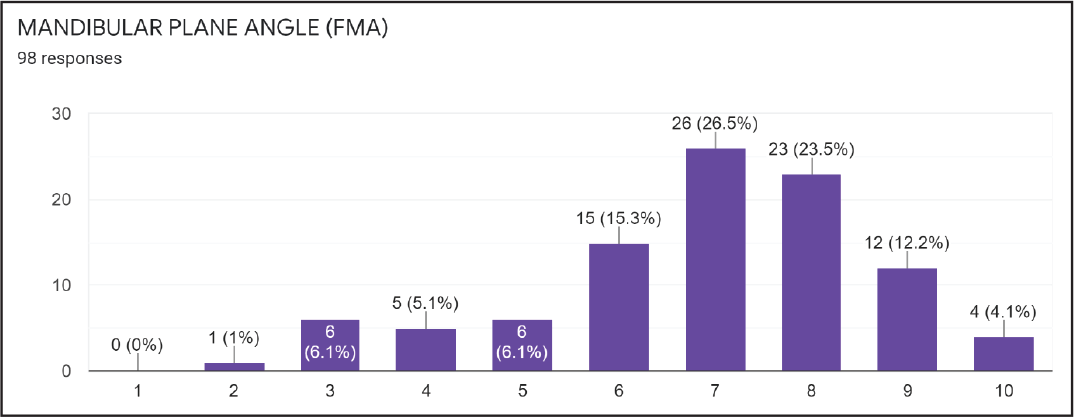
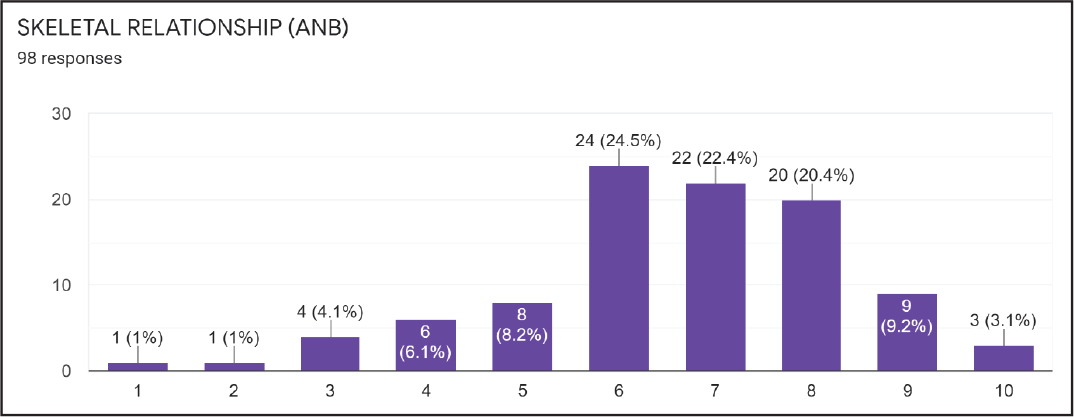
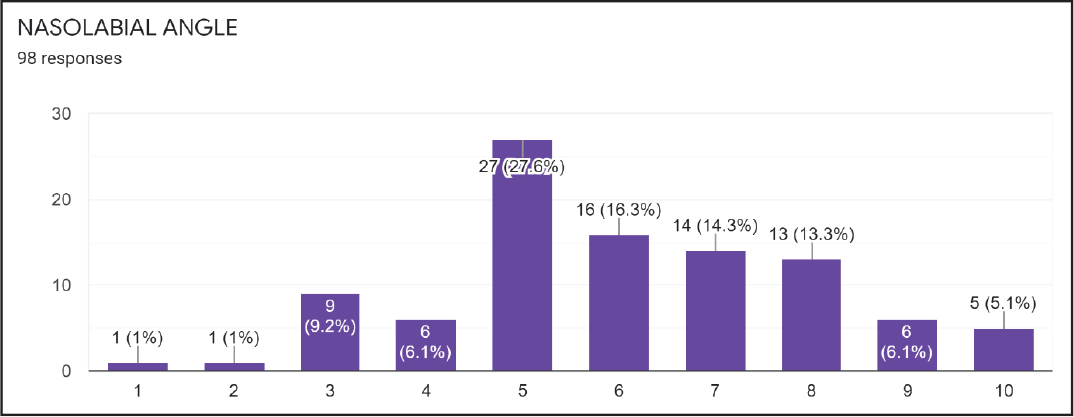
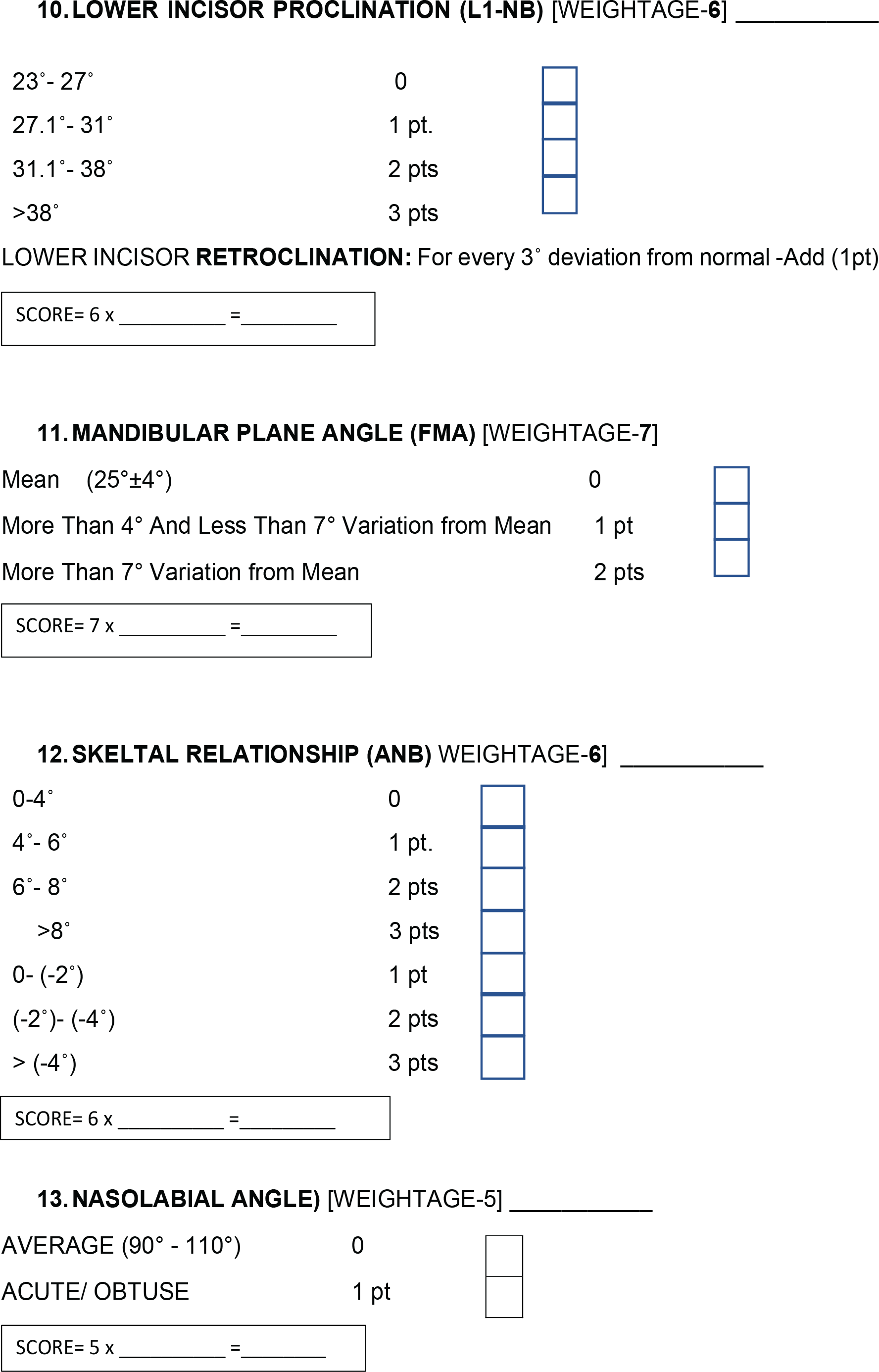
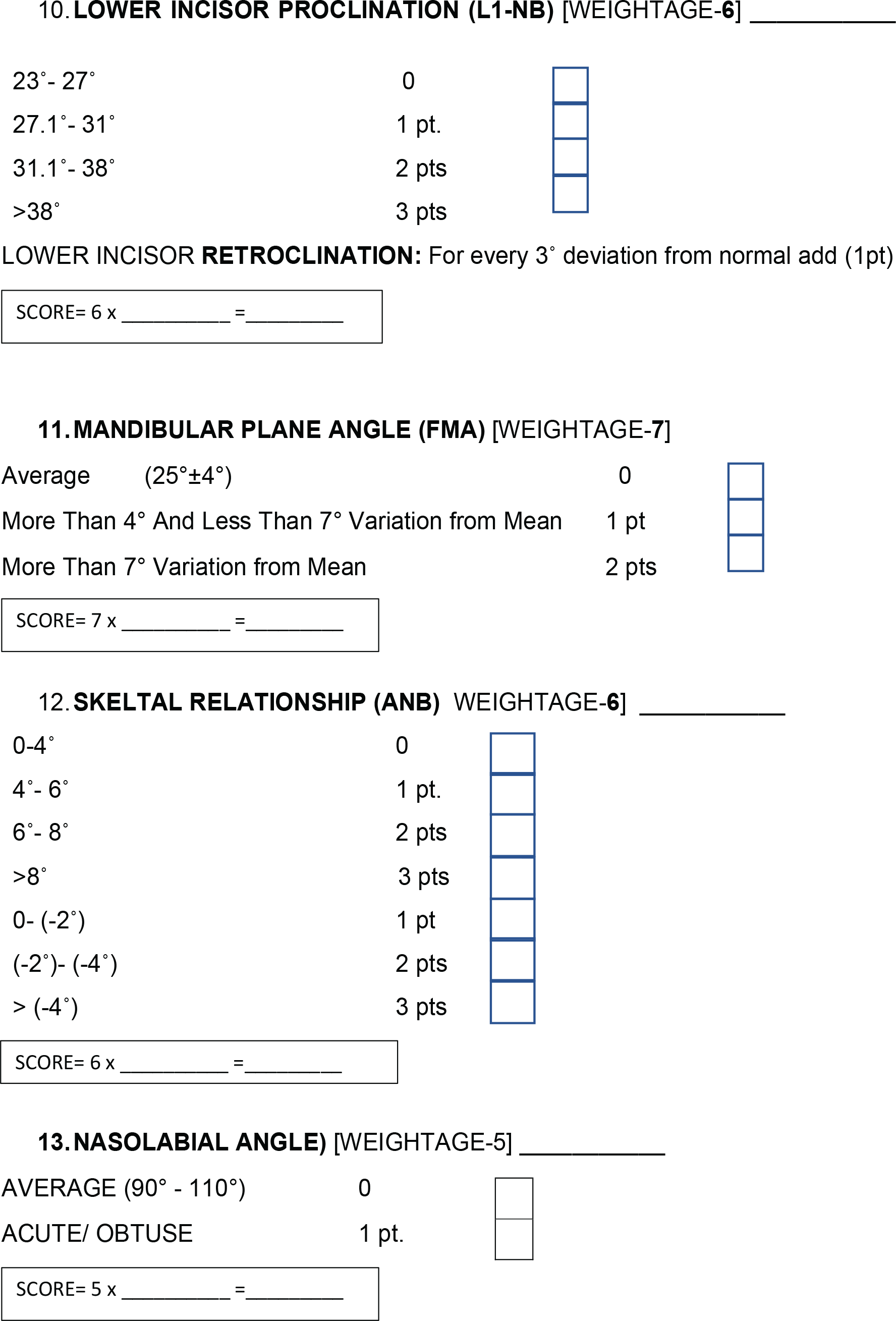
Upper Anterior Proclination (U1 to NA) Lower Anterior Proclination (L1 to NB) Mandibular Plane Angle (FMA) Skeletal Relationship (ANB) Nasolabial Angle
Impacted Teeth (Other than Third Molar) Tooth Transposition Missing Teeth (Other than Third Molar) Cleft Lip/Palate Skeletal Asymmetry (Nonsurgical Management)
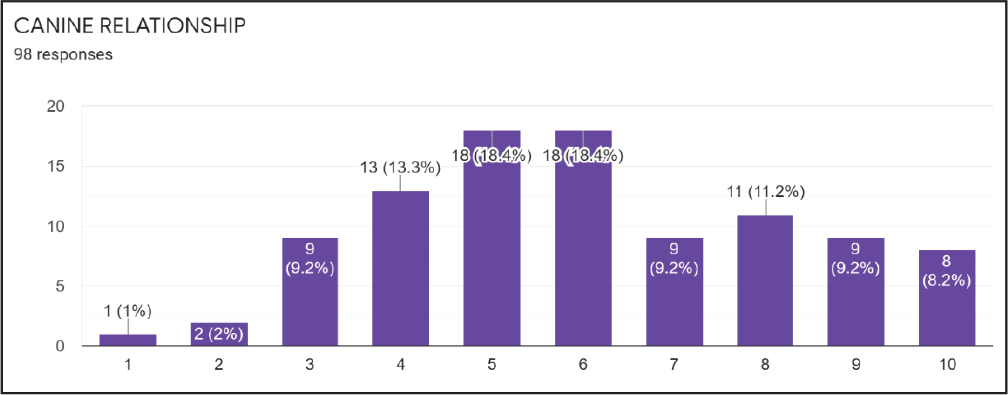
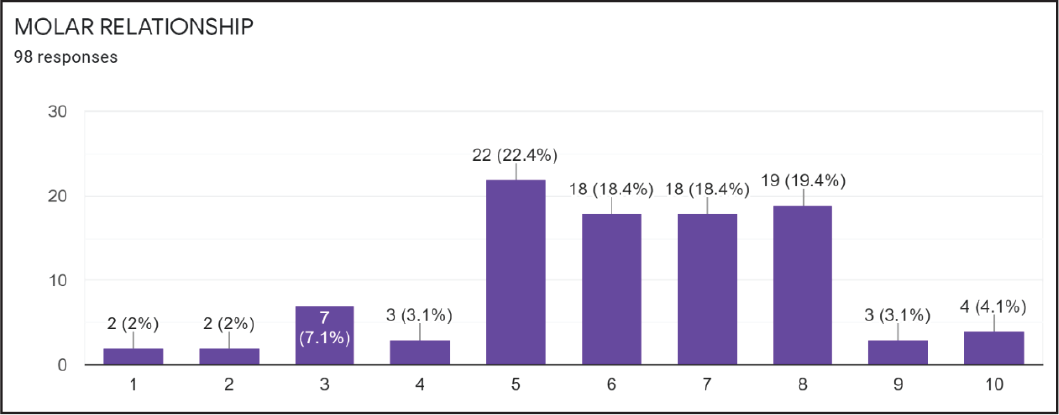
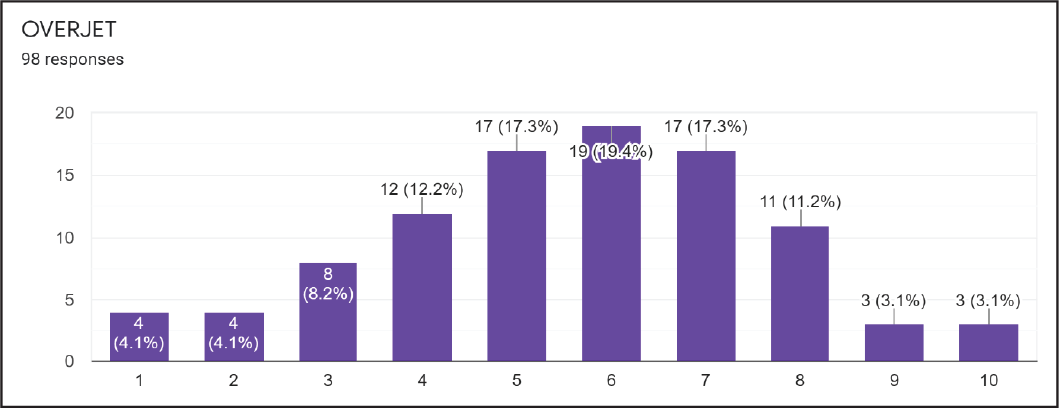
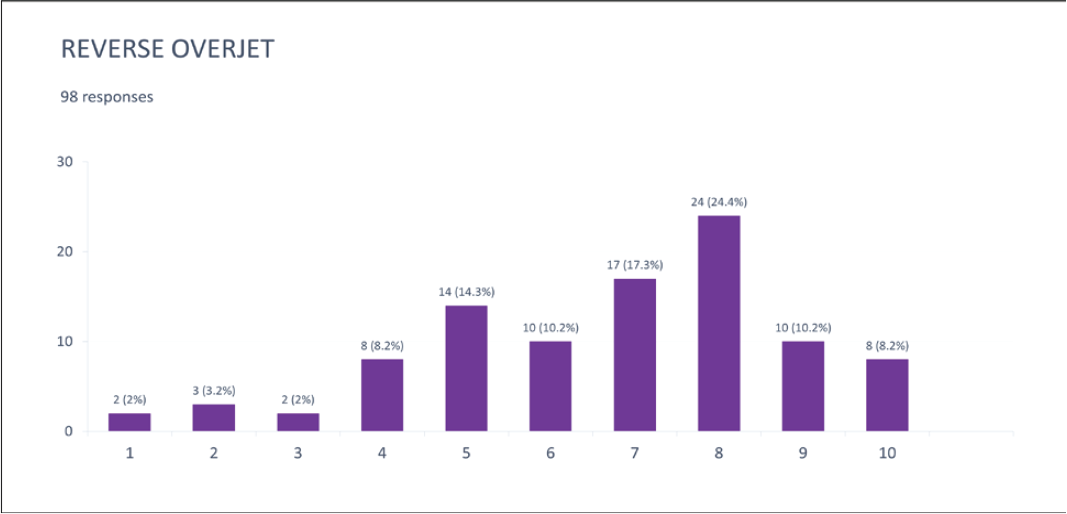
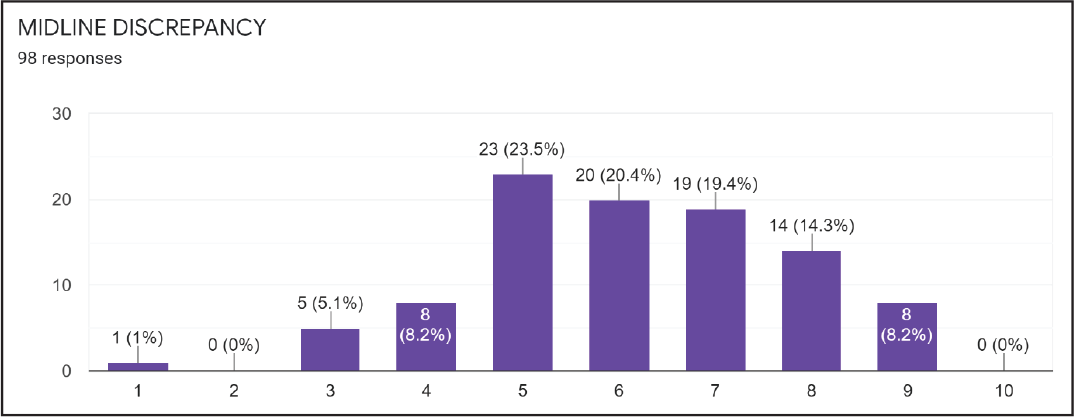
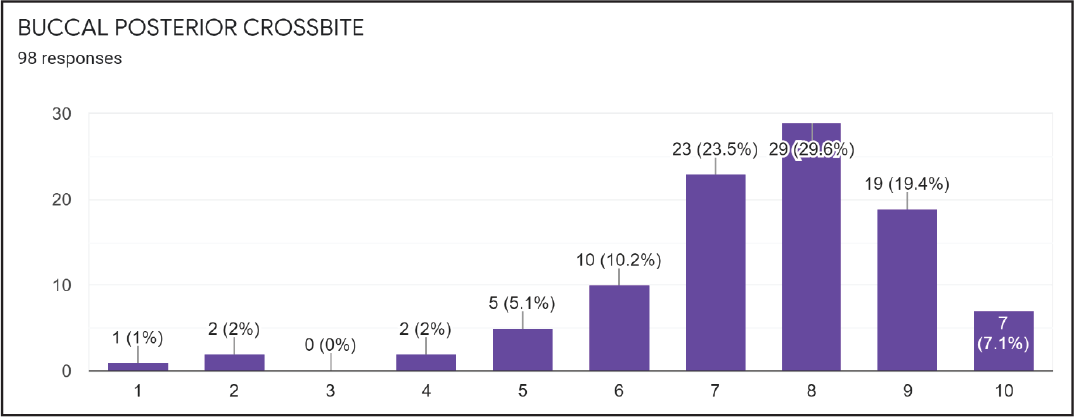
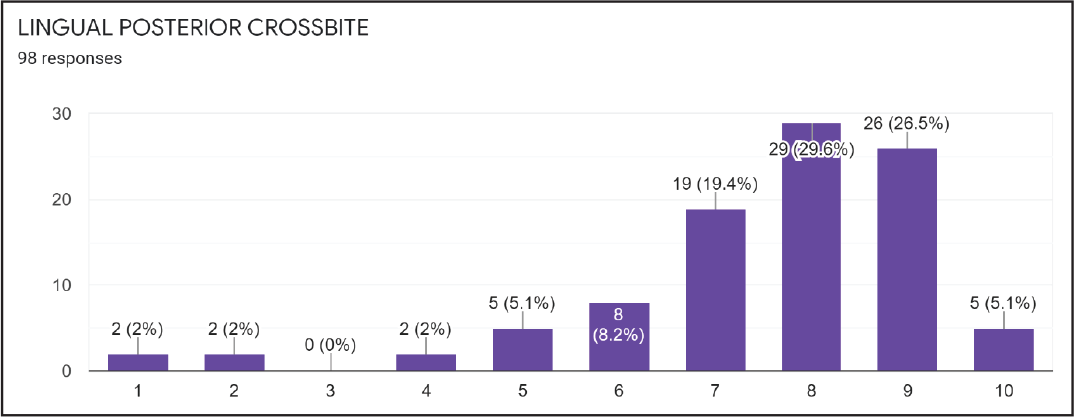
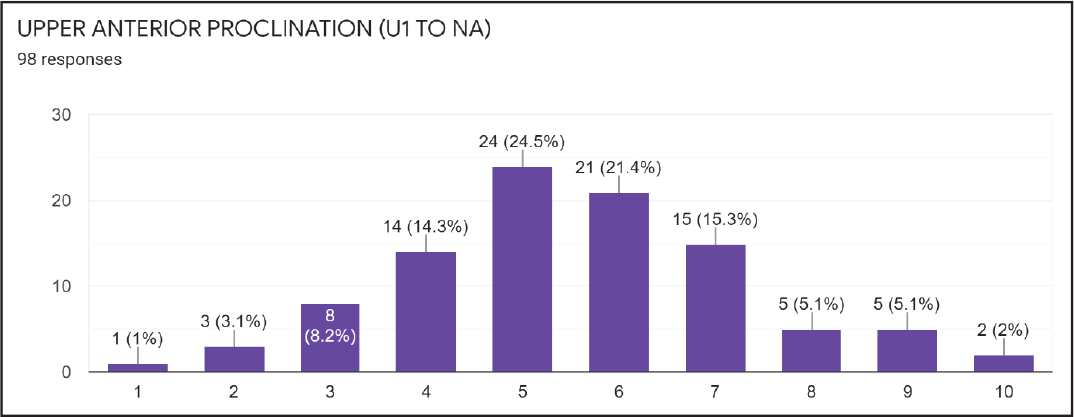
Statistical analysis was done using the SPSS software (SPSS Statistics V26) to determine the mean and standard deviation of the scores obtained and determined an average weightage for each of the dental and cephalometric components to be evaluated. The response obtained from every component in the survey is given in the form of bar charts below.
Dental Components
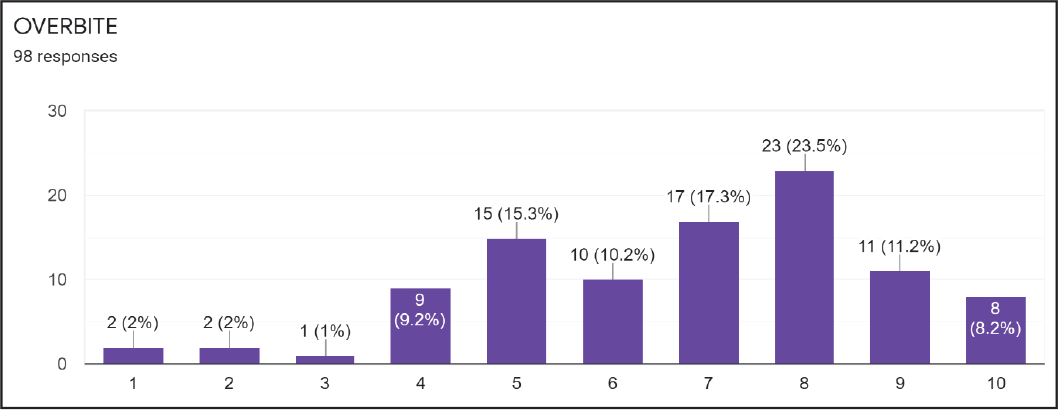
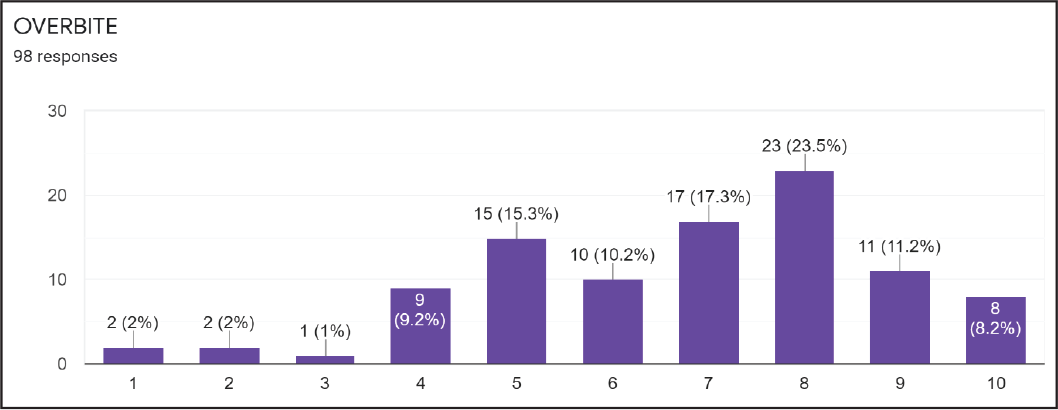
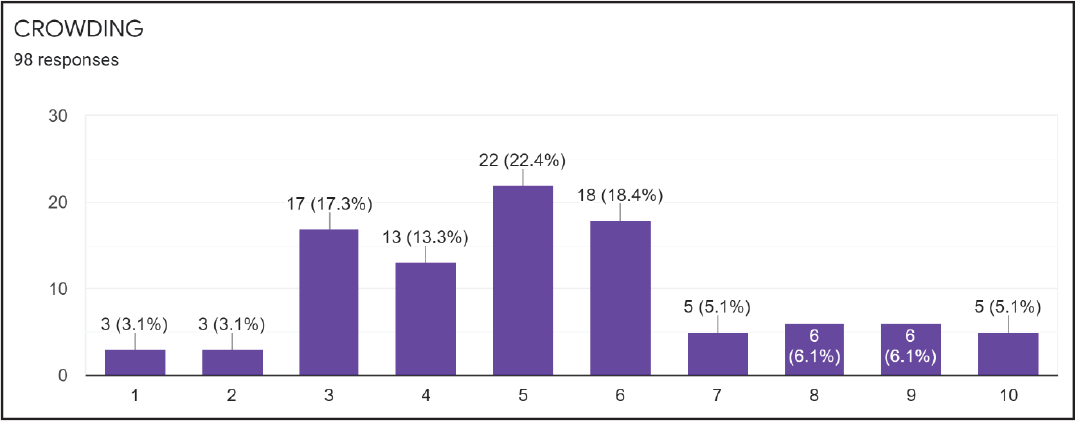
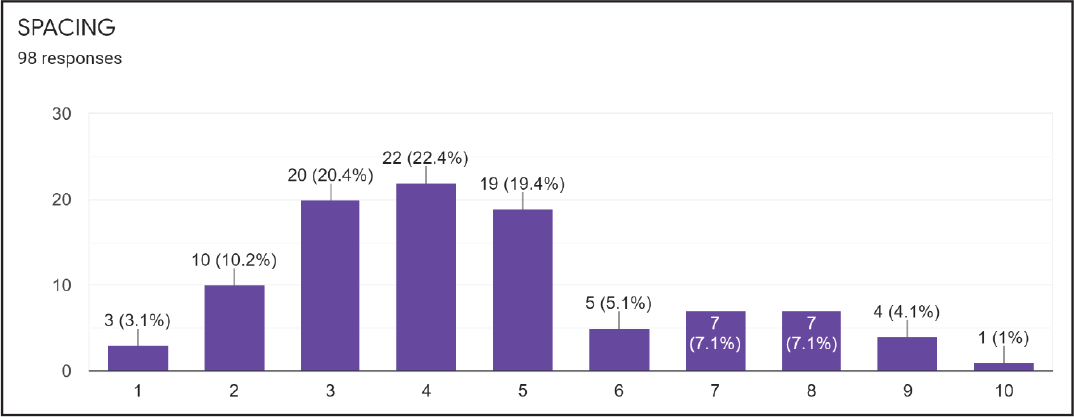
The X-axis in the chart represents the weightage score from 1 to 10 (where 1 is the least severe and 10 is the most severe malocclusion).
The Y-axis in the chart represents the number of participants who have graded for the particular weightage (The IBO diplomates grading each score). The percentage of the same is also mentioned in the Y-axis of the chart.
(B) Reverse Overjet
(A) Overbite
Cephalometric Components
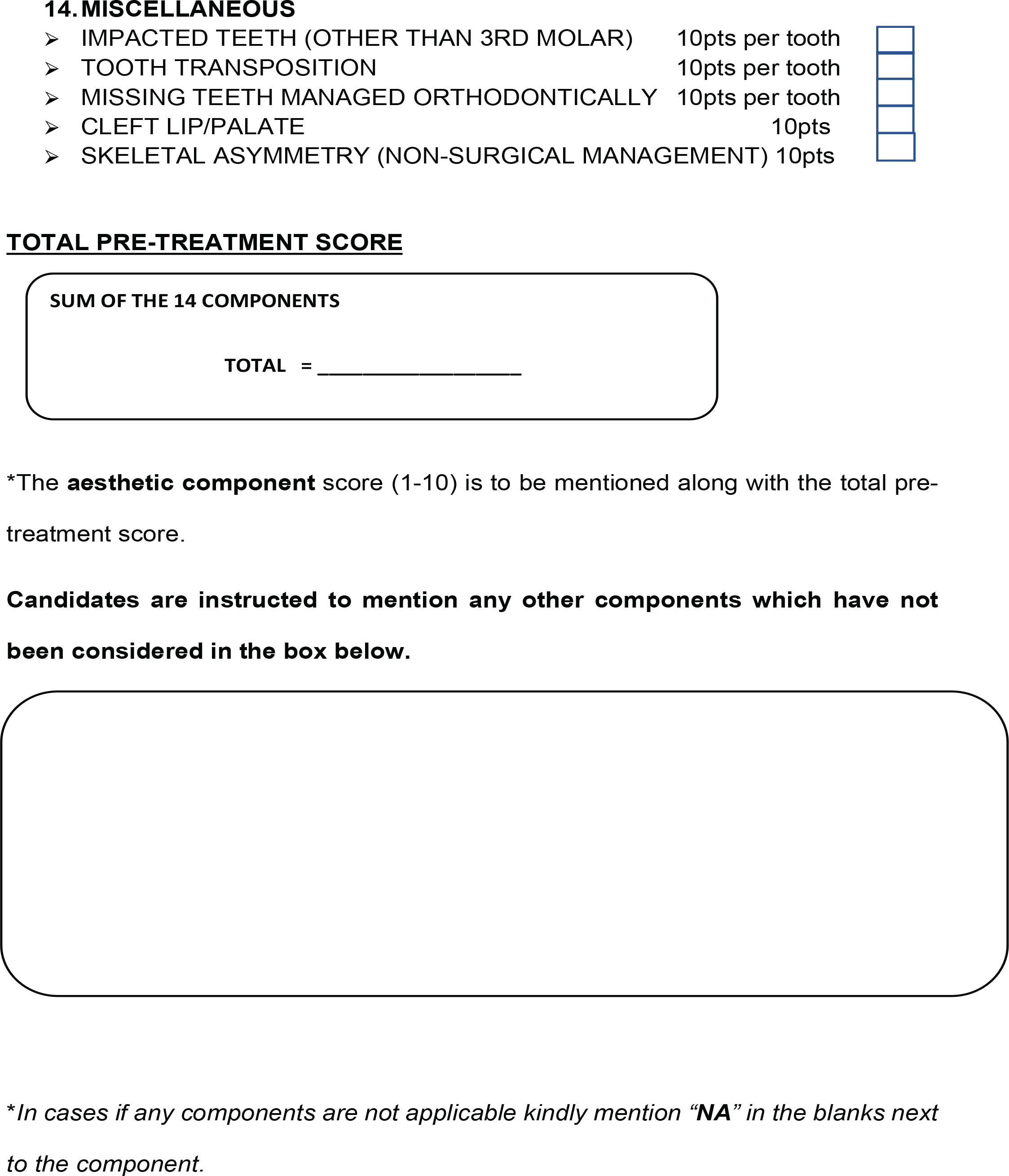
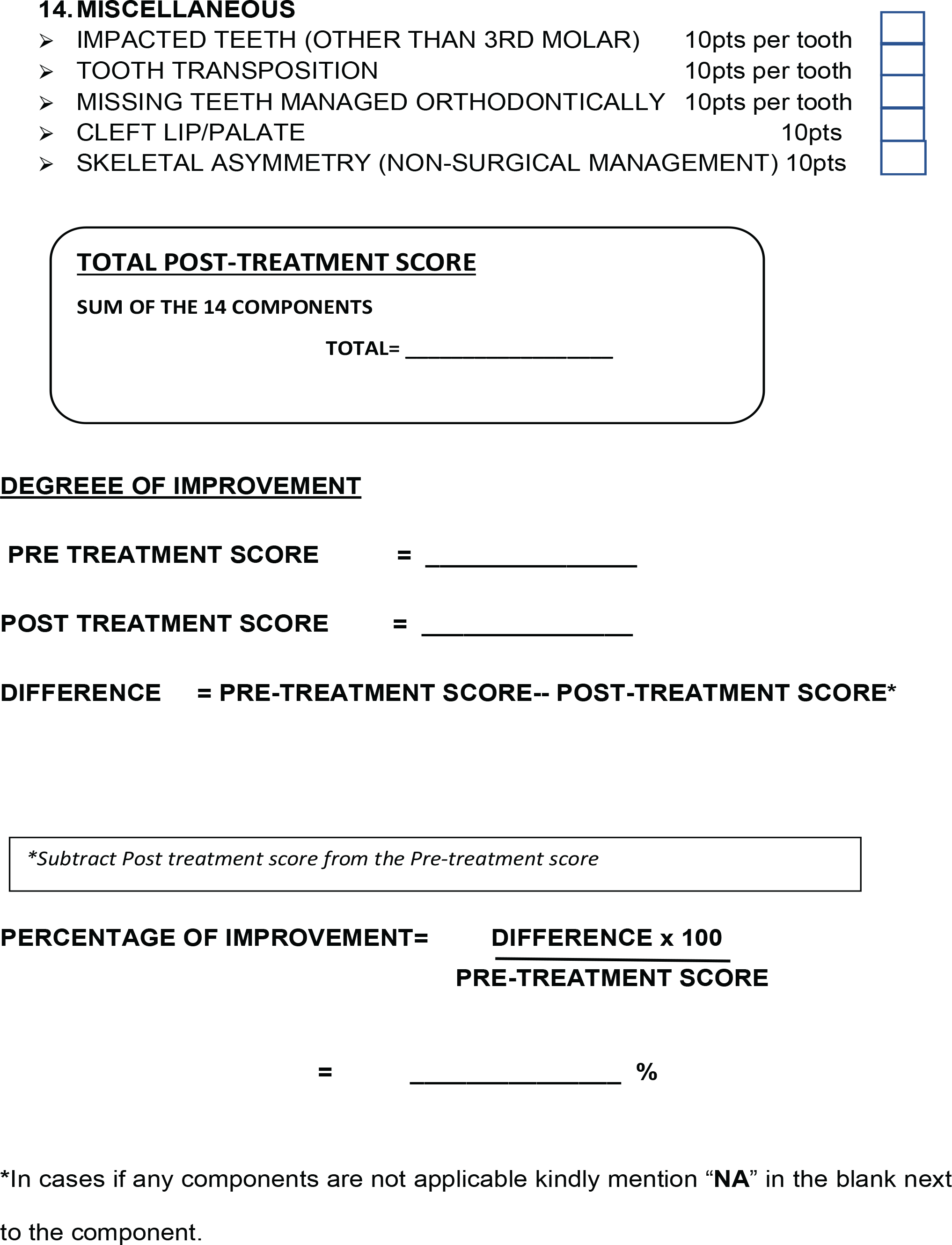
The Five miscellaneous components that were considered were given the highest weightage score of 10 points considering their degree of difficulty for correction. The miscellaneous components involved in the evaluation index are as follows.
Impacted Teeth (Other than Third Molar) Tooth Transposition Missing Teeth (Other than Third Molar) Cleft Lip/Palate Skeletal Asymmetry (Nonsurgical Management)
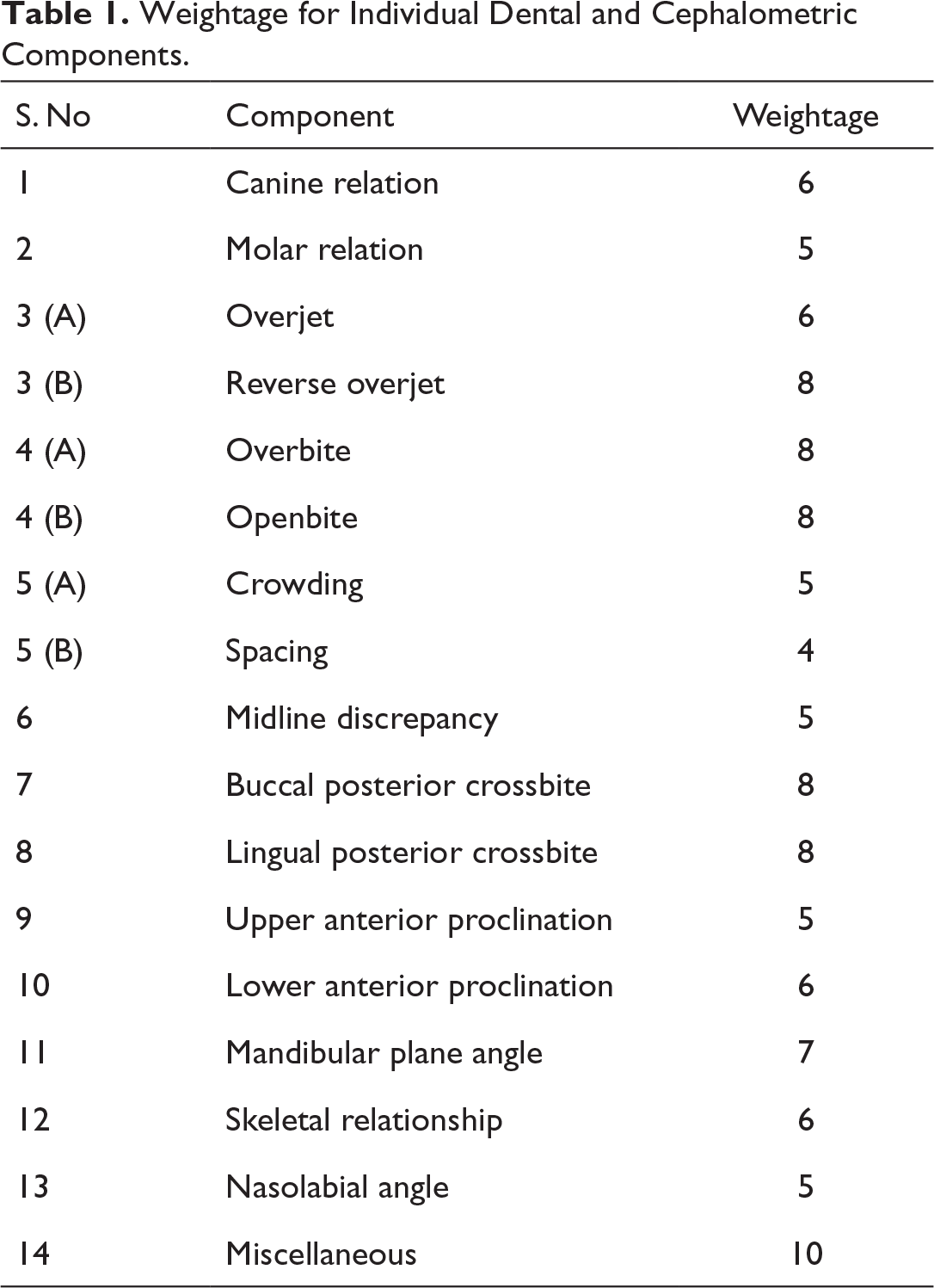
The score for the particular component is determined by the score that is chosen by most of the diplomates. There were high variations in the scoring when it came to the dental and skeletal components. The weightage score for a particular component was decided by the degree of severity of the malocclusion and the score selected by the highest number of participants. In cases where there was a similar number of responses for two scores (eg, canine classification), the director’s opinion was obtained to decide the weightage. The weightage of dental and cephalometric components obtained from the questionnaire is given in Table 1.
Weightage for Individual Dental and Cephalometric Components.
Aesthetic Component
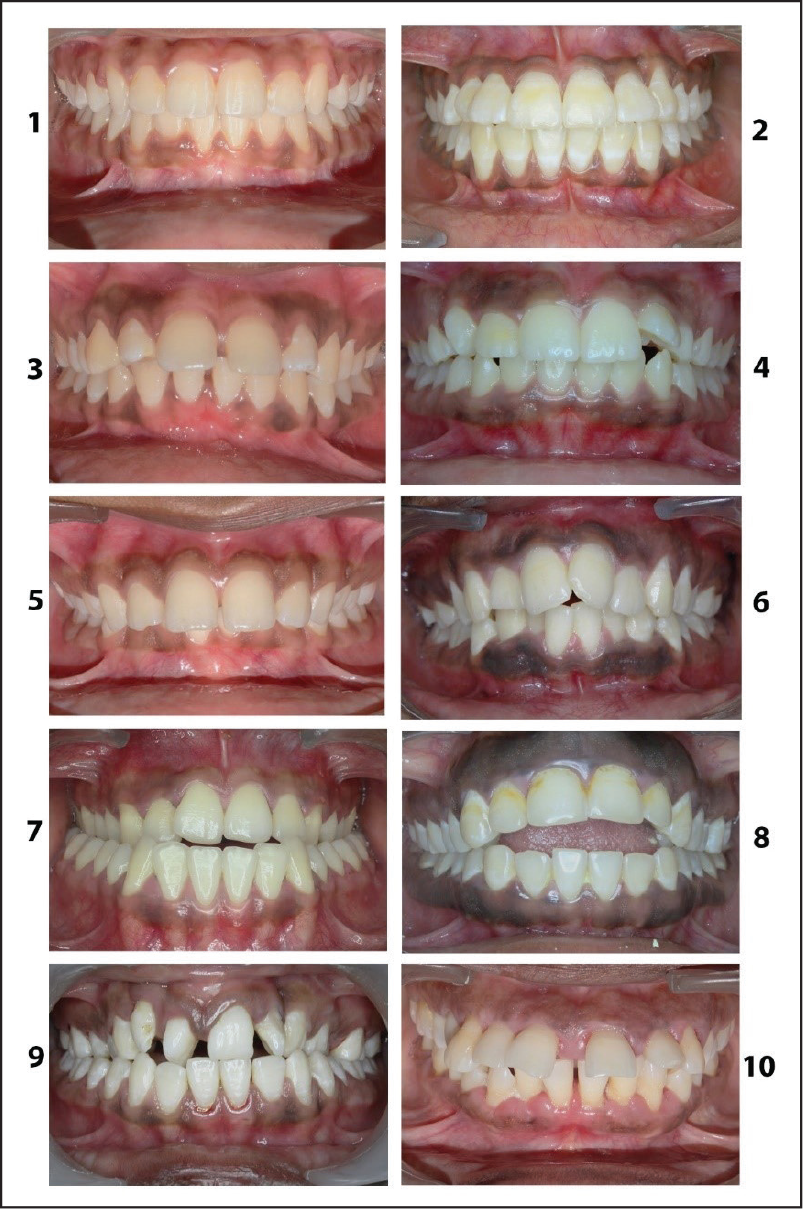
In the aesthetic component survey, the diplomates are asked to score the photographs in the malocclusion based on their aesthetic values. The photographs were chosen based on the most common malocclusions seen in the population. The aesthetic perception of the participants was determined using this survey.
The relative aesthetic score for every photograph was assessed and based on the survey and the values were obtained as follows with score 1 being the most aesthetic and score 10 being the least aesthetic (Figure 1).
Aesthetic Component Scoring Photograph.
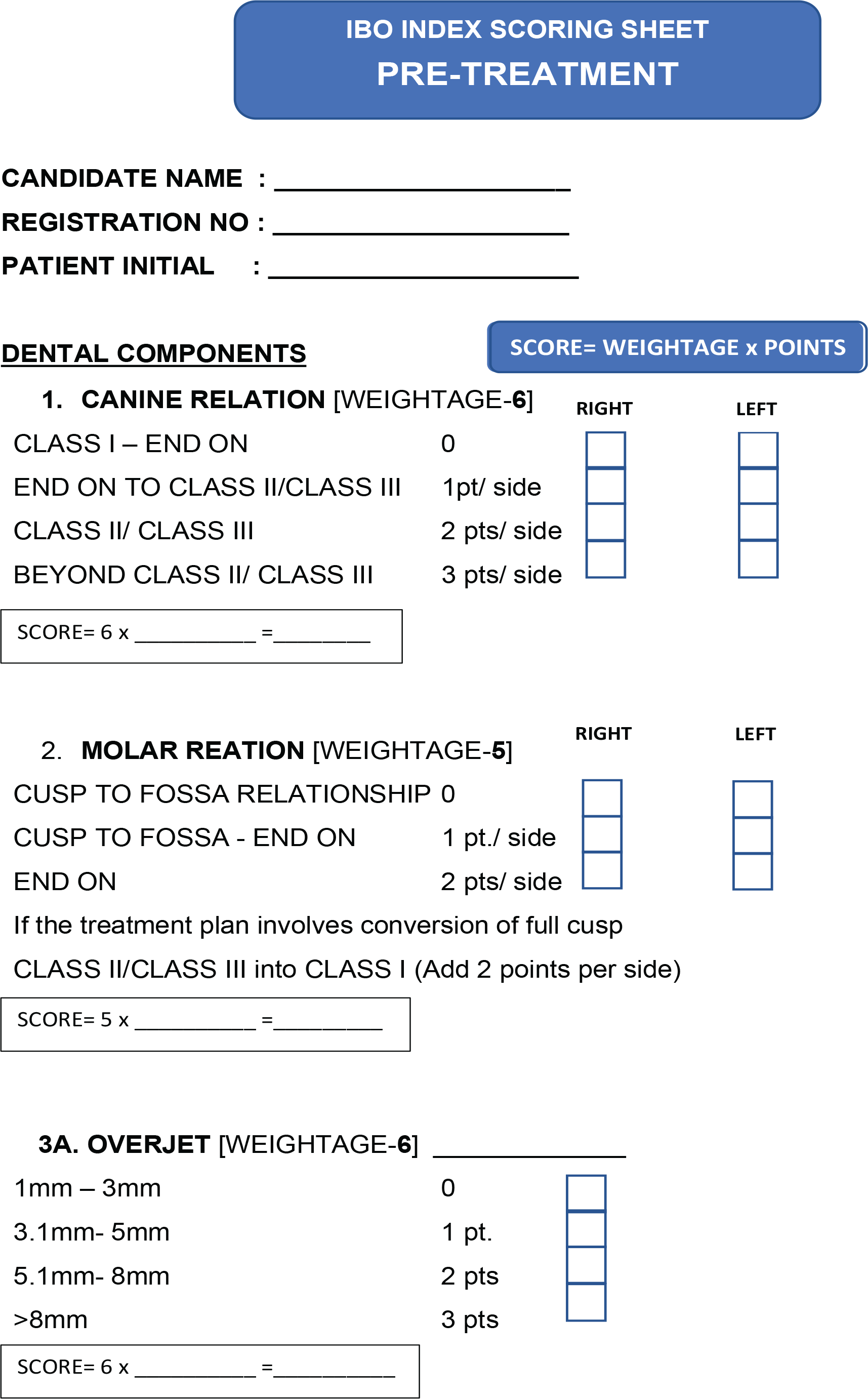
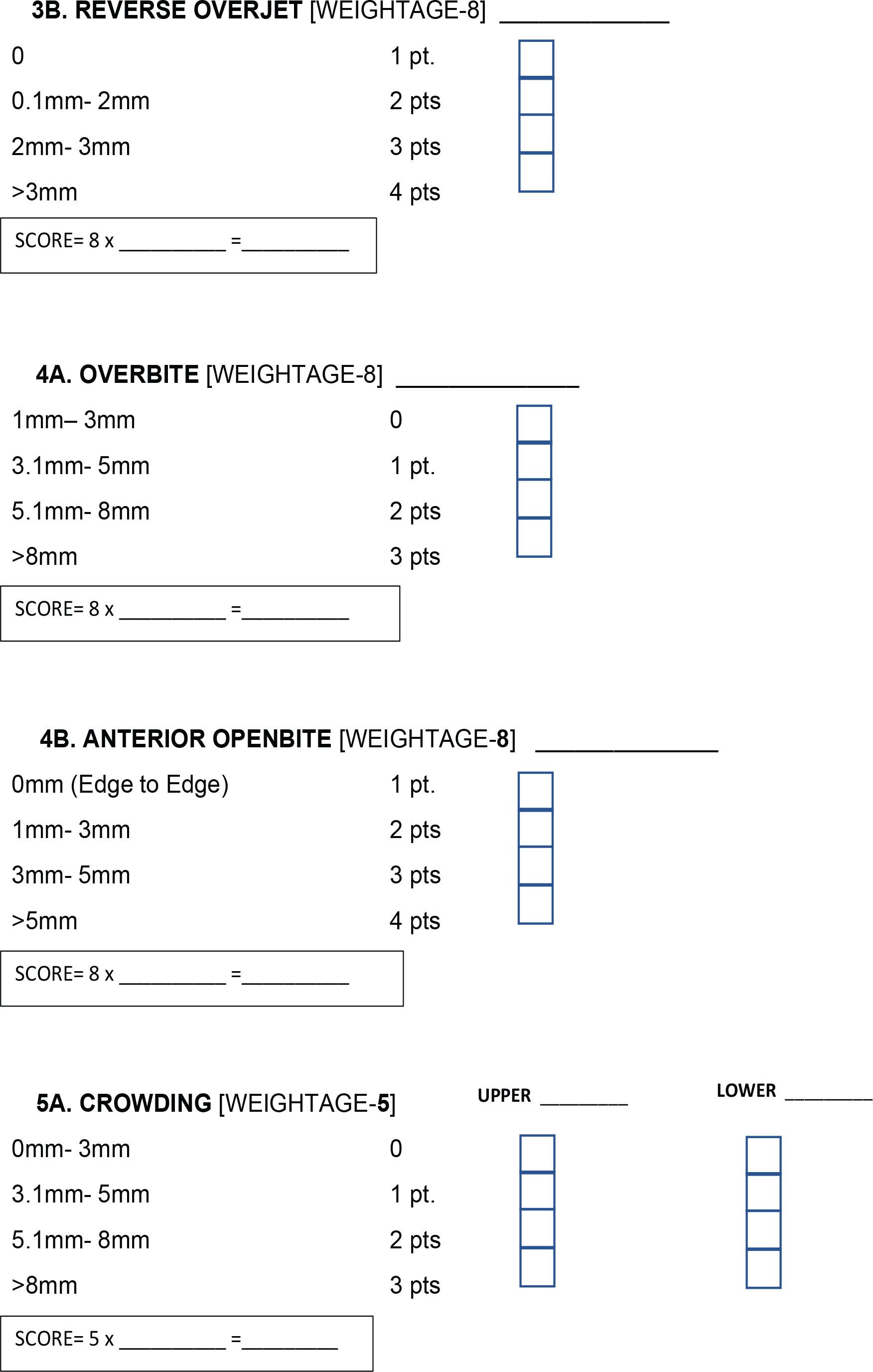
A scoring sheet was formulated to check the overall scores for assessing the degree of difficulty of the case selected based on the weightage of each component of the malocclusion.
Discussion
Various orthodontic indices were previously published on a particular population. The commonly used orthodontic indices in practice are IOTN, PAR, ICON, and so on.2–7 The validation of those indices was previously studied and published earlier.8–10 A grading system was also previously formulated by the American Board of Orthodontics for their dental casts and panoramic radiographs. 11
Most of the above indexes that have been previously developed were primarily meant to assess treatment needs for the patient, but this did not meet the purpose of an index to assess the degree of difficulty of a case. The need to assess the complexity of a case selected by the candidate presenting for the clinical phase III of IBO examinations is of prime importance especially for category IV and V where candidates are allowed to present any case of their choice with a high degree of difficulty. Therefore, a new index specifically addressing the need of our Board is being formulated.
The need to include various components of malocclusions predominantly seen in our ethnic population was the main criteria to formulate a discrepancy index specific for the IBO. This index also constituted an aesthetic component based on the malocclusions commonly seen in our population. This index has been formulated in a way that it included all the major ways to categorize any particular case skeletally, dentally, aesthetically, and the conditions pertaining mostly to the Indian population.
The index will be implemented in the IBO examinations after assessing its validity by comparing the same with earlier available and commonly used orthodontic indices. This index will help in streamlining the cases submitted for the phase III clinical examinations based on the degree of difficulty of treatment. The IBO would keep this index updated and would take all measures to help candidates to prepare and appear for the examination. Any updates on further validation of the index and its improvement will be updated periodically. This index developed would not only help candidates to assess the degree of difficulty of their cases submitted but it could also be used as a model of self-assessment to stimulate the spirit of self-improvement amongst teachers, practitioners, and students of the Indian Orthodontic Society.
Conclusion
This new IBO index formulated would serve as a guide for case selection to candidates appearing for the phase III clinical exams primarily to assess the complexity of the case. This index would include two charts to evaluate (a) pretreatment score and (b) posttreatment score and also would be able to determine the percentage of improvement between pre- and posttreatment. Although the posttreatment score may be brought down to a value of zero using this index, the finished case would still have to meet the other requirements of the Board concerning the final occlusion. The IBO is considering different options for applying this index for a comprehensive method to assess the degree of difficulty of cases submitted for the phase III clinical examination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.