
Abstract
Abstract
This case was submitted to the board under category IV for the Indian Board of Orthodontics examination, November 2013. The summary of the treatment, records, and treatment progress are reprinted with minimal editing and reformatting so that the manuscript resembles the actual documents submitted to the board.
Keywords
Introduction
PL, an 18-year-old male, presented with class II div 2 incisor relationships with high and buccally placed upper canines and end-on molar on a class II skeletal base. He had severe deep bite and reduced overjet with severe crowding in upper and lower arches. Lips were incompetent with gumminess on smiling.
Treatment involved extraction of upper first premolars and nonextraction in lower arch with interproximal reduction in the incisor region. Appliance used is preadjusted edgewise with 18 × 25 slot and MBT prescription.
Section 1. Pretreatment Assessment
Initials: P. L.
Sex: Male
Date of birth: November 3, 1991
Age at start of treatment: 18 years 5 months
Patients complaints: Irregularly placed front teeth
Relevant medical history: Nil relevant
Clinical examination: Extraoral Features (Figure 1)
Average toward horizontal mandibular plane angle
Skeletal class II pattern with convex profile and prominent chin
Acceptable facial symmetry and balance on frontal examination
Upper dental midline shifted toward left by a 1 mm in relation to facial midline.
Incompetent lips
Normal nasolabial angle
High lip line
No sign and symptoms of temporomandibular disorder
Pretreatment Photographs (Extraoral)

Pretreatment Photographs: Intraoral

Clinical Examination: Intra-Oral Features (Figure 2)
Soft tissues: Moderate gingivitis
Oral hygiene: Poor oral hygiene
Erupted teeth present: Central incisor to second molars in all quadrants
General dental condition: Attrition of Incisal edges of LR1 and LL1
Crowding/Spacing
Maxillary Arch:
Contracted arch form Severe labial segment crowding Deep palate High placed upper canines UR1, UL1, UL2: Retroclined, UR2: Proclined
Mandibular Arch:
Tapered arch form Severe labial segment crowding
Occlusal Features:
Incisor relationship: Class II div 2
Overjet (mm): 0 mm
Overbite: Complete coverage of lower incisors (90%)
Centrelines: Upper and lower coincident and toward left by 1 mm in relation to facial midline
Left buccal segment relationship: Molars: class II, Canines: class II
Right buccal segment relationship: Molars: class II (End-on), Canines: class II
Crossbites: None, Displacements: None
Other occlusal features: Deep curve of spee
General radiographic examination (Figure 3)
Pretreatment radiographs taken: Orthopantomogram (17/4/10)
Lateral Cephalogram (17/4/10)
Unerupted teeth: 8 8
Other relevant radiographic findings:
Space for erupting third molar seems to be deficient Roots of upper and lower incisors mesially angulated indicating lack of space for proper Alignment Diffuse calcification present between roots of lower right first and second premolars.
Pretreatment Radiographs

Other Special Tests/Analyses
Bolton’s Analysis:
The mesiodistal widths of the maxillary and mandibular teeth were ascertained using spring dividers. The mesiodistal widths of the maxillary and mandibular teeth are as under:
Sum of maxillary 12 teeth (6-6) = 101 Sum of mandibular 12 teeth (6-6) = 94.5 Sum of maxillary 6 teeth (3-3) = 50 Sum of mandibular 6 teeth (3-3) = 41 Overall Bolton Ratio = 94.5/101 × 100 = 93.56 % (Mean 91.3, SD 1.91) (> 91.3%).
This value reveals that there is an overall mandibular excess, calculated in mm as follows:
Overall Mandibular excess (in mm) = Sum of mandibular 12 – Sum of maxillary 12/100 × 91.3
= 94.5 – 101/100 × 91.3
= 2.287 mm
Anterior Bolton ratio = 41/50 × 100 = 82% (Mean 77.2, SD 1.65)
(> 77.2%) This value reveals that there is an anterior mandibular excess, calculated in mm as follows:
Anterior mandibular excess (in mm) = Sum of mandibular 6 – Sum of maxillary 6/100 × 77.2
= 41 – 50/100 × 77.2
= 2.4 mm
The ratio was outside one standard deviation of the mean overall and anterior ratio suggesting a tooth size discrepancy. In this instance the discrepancy was considered to be largely due to overall mandibular dental excess.
Radiographic Interpretation
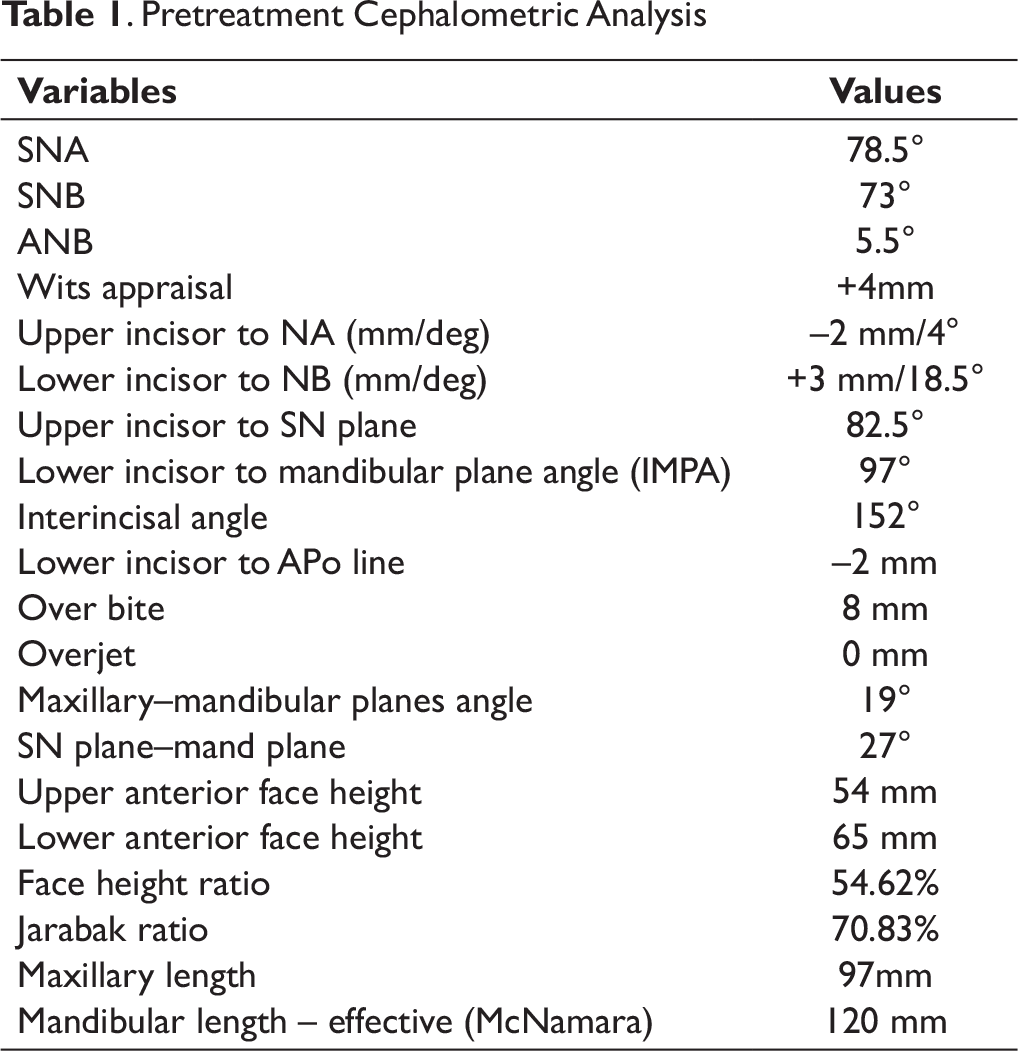
Following are the radiographic interpretation (refer to Table 1):
Vertical proportions indicate to a horizontal growth pattern as suggested by GoGn to SN, MM angle and Jarabak ratio.
Pretreatment Cephalometric Analysis
Diagnostic Summary
PL an 18-year-old male presented with a class II div 2 incisors and angles class II molar relationship on a class II skeletal base with normal or mildly reduced vertical height. There was a severe crowding in upper and lower arches with increased overbite and decreased overjet. Canines were high and buccally placed. Lips are incompetent and upper midline is shifted toward left by 1 mm.
Problem List
Class II skeletal jaw relationship
Deep bite
Severe crowding in upper and lower arches
High placed canines
Deep curve of spee in lower arch
Reverse curve of spee in upper arch
Incompetent lips
Gummy smile
Centerline discrepancy
Aims and Objectives of Treatment
To achieve functionally optimum and aesthetically acceptable occlusion
Accept the skeletal class II pattern
Relief of crowding
Correction of deep bite and reduced overjet
Level, align, and coordinate the dental arches
Correction of gummy smile
Correction of centerline discrepancy
Competency of lips
Achieving class II molar, class I canine, and incisor relationship
Retain corrected results
Evaluate for third molar extraction
Treatment Plan
The treatment was aimed mainly at dental correction of skeletal problem. Space needed to relieve crowding in the upper arch is resolved by extraction of first premolars. Extraction/Nonextraction in the lower arch is to be planned after alignment of upper arch, correction of deep bite, and overjet. In case of nonextraction, interproximal reduction is to be planned for space requirement in lower arch during the course of treatment. Bolton’s tooth size analysis shows mandibular anterior excess by 2.4 mm.
Extractions: upper first premolars
Appliances: PEA with MBT prescription 018 × 025 slot
Special anchorage requirements: None
Minor adjunctive surgery: None
Major adjunctive surgery: None
Additional dental treatment: None
Proposed Retention Strategy
Lingual bonded retainer in upper and lower arches to be given. Hawleys retainer to be worn full time along with fixed retainer for a period of 6 months followed by night wear for next 6 months.
Prognosis for Stability
Provided the lower incisors were not proclined excessively from the original position, good archform maintained, and good occlusal interdigitation was achieved the long-term stability of treatment changes was considered good.
Being a dental camouflage of a skeletal problem, the lower incisors will get proclined to correct overjet. To maintain their position, permanent retention is desirable. Maintenance of corrected deep bite will need mild anterior bite plane in upper Hawley’s for long-term stability of results.
Section 2. Treatment
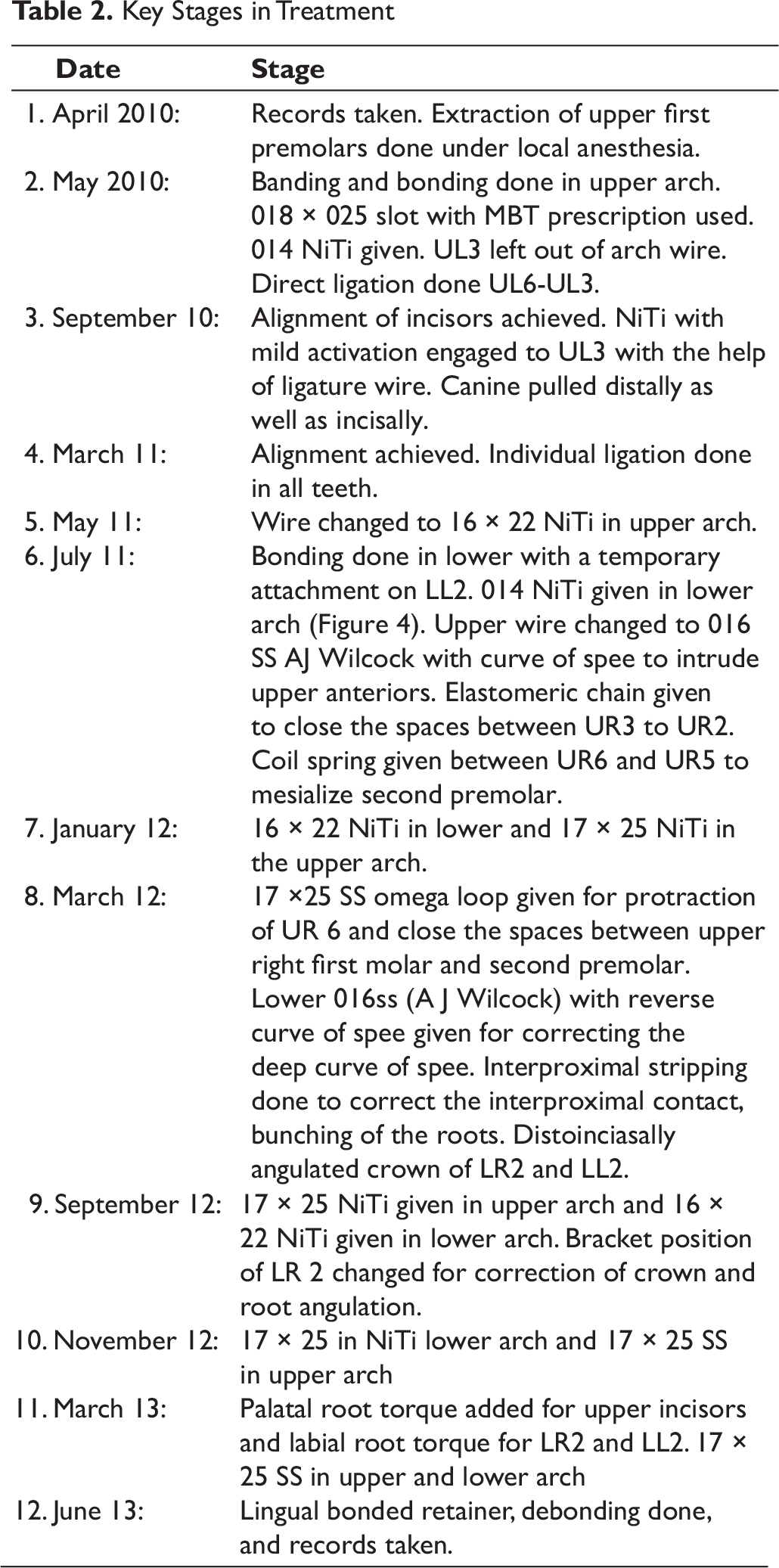
Treatment progress (Table 2)
Start of active treatment: 17 April 2010
Age at start of active treatment: 18 years 5 months
End of active treatment: 15 June 2013
Active treatment time: 3 years 2 months
Midtreatment Photographs
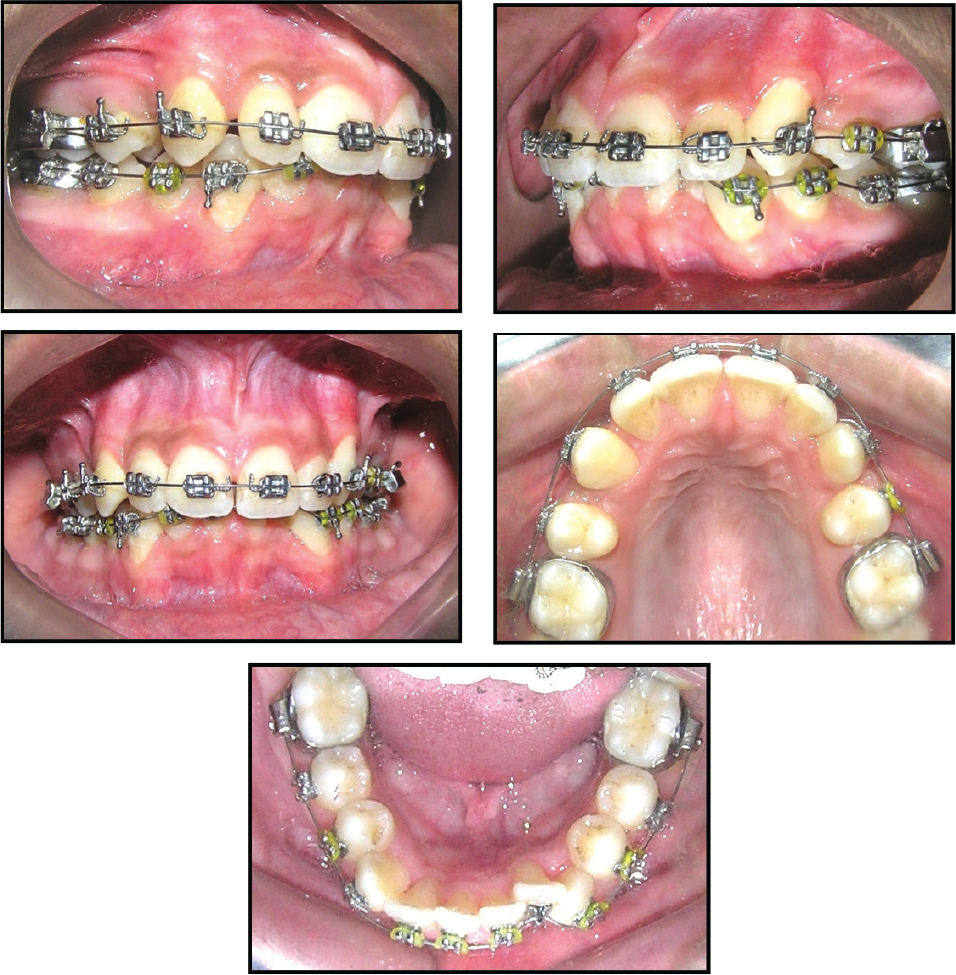
Key Stages in Treatment
Section 3. Post treatment Assessment
Occlusal features (Figures 5 and 6)
Incisor relationship: Class I
Overjet (mm): 2 mm
Overbite: 2 mm
Centerlines: Coinciding with each other and with facial midline
Left buccal segment relationship: Molar, class II
Canine: Class I
Right buccal segment relationship: Molar, class II
Canine: Class I
Crossbites: None
Displacements: None
Functional occlusal features: Mutually protected occlusion with canine guidance on excursive movements
Posttreatment Photographs: Extraoral

Complications Encountered During Treatment
The patient had difficulty in maintaining a good standard of oral hygiene. Poor oral hygiene led to black triangles at interdental pappilae in the lower incisor region. Had to reduce interproximally to establish good contact and correct black triangle. Treatment of lower arch without extraction made alignment little difficult. Torqueing and up righting of LL 2 and LR 2 roots took a lot of time.
Posttreatment Photographs: Intraoral

Posttreatment Radiographs

Radiographs Taken Toward/at the End of Treatment
Radiographs taken: Lateral Cephalogram & OPG (Figure 7)
Relevant Findings
No pathology seen.
No change in root length of incisors.
Good parallelism of roots achieved.
Lack of space for eruption of lower third molars.
UR3 and UR5 roots are closer to each other and UR3 more distally inclined.
Super Imposition of Pre- and Postlateral Cephalograms (A) Maxillary Changes and Mandibular Changes. (B) Overall Skeletal and Dental Changes.
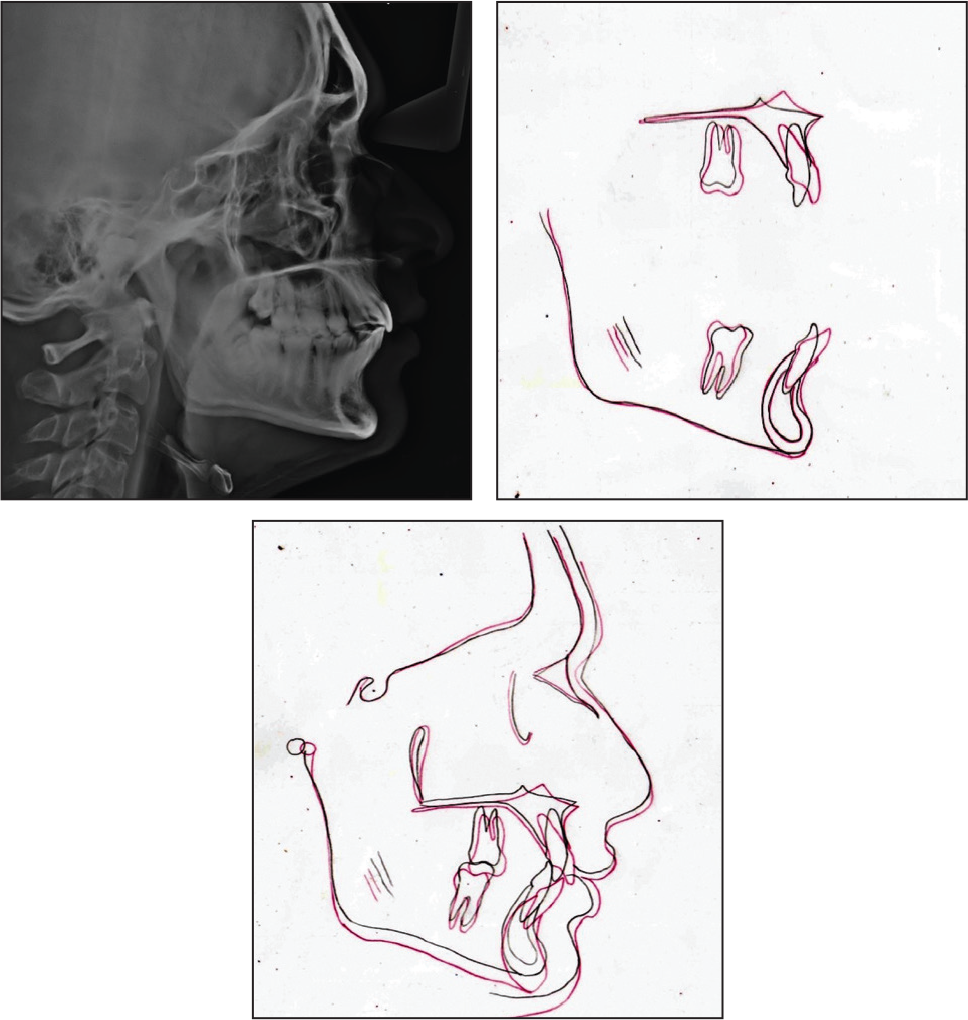
Interpretation of Cephalometric Changes (Figure 8)
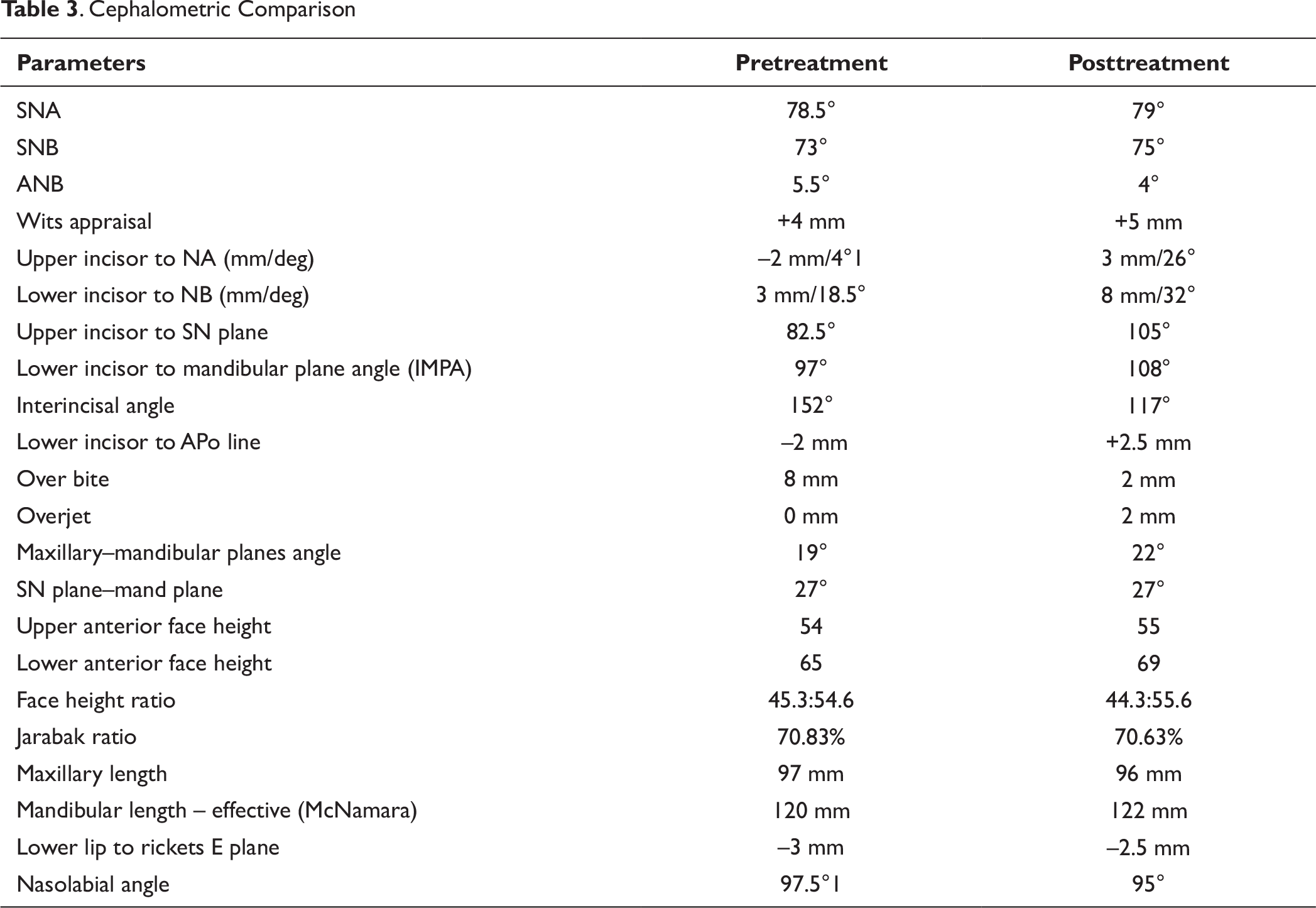
Skeletal: There is a mild change in ANB value. It has reduced by 1° from 5° to 4°. May be attributed to dentoalveolar changes that taken place. SNA has increased by 1° to 79° and SNB has increased by 2° to 75°. The M-M angle has opened up by 3 from 19 to 22. Other skeletal values have remained more or less close to normal.
Dental: Significant changes in upper incisor angulation have taken place. The upper incisor has Proclined to close to normal value from an upright position. upper incisor in relation to NA has changed from 4° and –2 mm to 26° and 3 mm. in relation to SN plane it has changed from 82.5 to 105.5 but the lower incisor has proclined significantly in relation to NB from 18.5 and +3 mm to 32 and 8 mm. IMPA has increased from 97 to 108. In relation to A-Pog plane it has changed from –2 mm to +2.5 mm.
Soft tissue: Competence of lips achieved. Nasolabial angle has decreased by 2.5 from 97.5 to 95 attributed to change in position of upper incisor position. Lower lip in relation to rickets E plane is placed –2.5 mm, indicating a normal positioning.
. Cephalometric Comparison
Section 4. Critical Appraisal
PL was successfully treated by orthodontic camouflage over a period of 38 months. The original treatment aims were accomplished and the patient’s chief complaint addressed. PL was notably pleased with the treatment outcome. A good occlusal and aesthetic result was achieved.
Skeletal: The anteroposterior skeletal pattern improved during treatment from moderate to mild class II relationship. This may be due to dentoalveolar remodeling. The vertical proportions have been maintained. Dental: The severe crowding in the upper and lower arches is successfully relieved. The incisor angulations corrected to allow good aesthetics and proper function. Significant amount of bite opening has been achieved with a combination of anterior intrusion and little posterior extrusion. Good overjet and overbite have been achieved. High placed canines have been brought nicely into the occlusion without loss of gingival attachment. Well-settled class II molar and class I canine relationship has been achieved. Midlines are coincident. Interproximal stripping done in lower incisors will bring more anteroposterior stability in lower labial segment as lower incisors have been proclined significantly. Canine root torque in upper arch is different on the right and left sides. More palatal root torque was needed in UL3. Tip on the UL3 is also more compared to the right side. UL6 is relatively more mesiopalatally rotated in comparison to UR6. Lower incisors are significantly proclined. Increased labial root torque in LR2 and LL2 was needed. Soft tissue: A notable change in the lip line was achieved with normal show of incisors at rest. While smiling there is less show of gingiva with improvement in gumminess. Lip competency has been achieved.
Iatrogenic
Poor oral hygiene has led to loss of gingival height interdentally leading to black triangles in lower anteriors. No change in root length was observed in upper and lower incisors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.