
Abstract
Abstract
Objective: Fixed orthodontic appliances may influence the oral environment through accumulation of plaque, decreased plaque pH, and increased gingival inflammation. These changes in the oral cavity can potentially lead to periodontal disease, demineralization, and other infectious diseases.
Materials and Methods: To investigate the changes in biofilm throughout the initial 2 weeks, we placed a stainless steel bracket on the upper second premolar and collected plaque samples on the bracket and on the tooth surface at different time points (0, 24, 48 h and 1 and 2 weeks) and plated on tryptic soy agar blood agar plate, and kept at 37°C in an anaerobic chamber for 5 days to determine the CFUs of bacteria. At the end of 2 weeks, we removed the bracket and elastomeric module, and we isolated genomic DNA from the bacterial biofilm for identification of bacteria by 16S rRNA PCR analysis. We also analyzed the morphology of biofilm on the bracket by scanning electron microscope.
Results: Our results show that the bacterial biofilm was significantly increased on the bracket in all the subjects, whereas on the tooth surface, the CFUs were not significantly increased. PCR assay showed that biofilm on orthodontic brackets from all subjects showed colonization by Streptococcus gordonii, Porphyromonas gingivalis and Streptococcus mutans were observed on some of the subjects after 48 h, whereas Aggregatibacter actinomycetemcomitans biofilm was observed in all the time points except 24 h.
Conclusion: This study demonstrated that both periodontal and cariogenic bacterial biofilms were formed on the bracket as early as 24 h.
Introduction
Fixed orthodontic appliances may influence the oral environment through accumulation of plaque, decreased plaque pH, and increased gingival inflammation.1-3 These changes in the oral microflora can potentially lead to periodontal disease and demineralization of teeth, which can result in caries or white spot lesions that pose a significant esthetic problem posttreatment. 4 This becomes a challenge to both clinicians and patients as it is important to maintain the health of teeth and supporting periodontium during prolonged orthodontic treatment. 3 Several studies demonstrated that the introduction of orthodontic appliances in a patient’s mouth alters the composition of plaque and increases the prevalence of bacterial species that are known periodontal and cariogenic pathogens.1, 5, 6 The initial biofilm formation can be influenced by multiple factors including surface free energy, affecting wettability and surface tension, surface roughness, and salivary protein adhesion.7, 8 It is known that the initial attachment of bacteria to a surface is mostly as a result of hydrophobic and electrostatic interactions, and different bracket materials may lead to differences in bacterial attachment due to their surface properties.
Little information is present on the profile of early colonizers of biofilm on orthodontic brackets, and there is a lack of true in vivo studies to demonstrate the process of initial biofilm development on fixed orthodontic appliances. Several studies8, 10-12 have confirmed the capacity of orthodontic brackets regardless of bracket material and design to provide a platform for biofilm formation as early as 60 minutes in laboratory settings. 8 A few in vivo studies7, 13 on early biofilm formation on orthodontic brackets noted the comparison of different bracket materials and designs on quantity of biofilm formed during the initial days, but they did not delve into the exact composition of the microbial communities formed on the bracket surfaces.
Our study is a preliminary prospective clinical study that aimed to investigate the dynamic process of early biofilm formation when a metal bracket is placed on a tooth. This study aims to examine the rate at which biofilm forms on a bracket surface and the tooth surface adjacent to the bracket during the first 14 days after bracket placement.
Materials and Methods
Experimental Design and Sample Size Calculation
On the basis of previous studies, power was calculated using the G*Power software. We set the effect size of 1.0, a power of 0.9, and a significance level of .05, which calculated our sample size to be 5. 14 Five healthy participants were recruited for the study. Inclusion criteria were as follows: (1) Subject population should consist of 3 women and 2 men with an average age of 26.5 (±2.20) years; (2) population should have both genders; (3) all ethnicities should be included; (4) complement of all permanent teeth from second molar to second molar; (5) no crowns, labial bondings, or laminates on designated teeth; and (6) good alignment of teeth. Exclusion criteria were as follows: (1) subjects with poor systemic health, (2) history of antibiotic use in the past month, (3) tobacco use, (4) professional cleaning or scaling in the past 2 weeks, (5) poor oral hygiene (gingival index of ≥1 and plaque index of >1), and (6) active caries or periodontal disease. All subjects who agreed to participate in the study signed consent forms approved (#Pro20150001973) by Rutgers-NJMS Institutional Review Board.
All subjects were instructed to use standard toothpaste (Crest Cavity protection toothpaste, 0.243% Sodium Fluoride) 1 week prior to the beginning of the study. They were given standard oral hygiene instructions including brushing at least twice a day and flossing once a day but were instructed not to use any additional oral hygiene products including mouthwash and xylitol gum. The subjects were also instructed not to brush or floss in the morning and not eat or drink anything other than water for 4 hours prior to sample collection.
Sample Collection
On each of the subjects, a stainless steel bracket (0.022 × 0.028 Victory series, 3M Unitek, Monrovia, CA, USA was bonded on the upper right second premolar using 37% phosphoric acid gel, Transbond XT adhesive primer, and adhesive. An elastomeric module was placed on the bracket for the subject’s comfort. Baseline sample collection was performed prior to bracket placement. At each time point (0, 24, and 48 h and 1 and 2 wk), plaque samples were collected on supragingival tooth surface adjacent to the bracket, on the buccal surface of the bracket, and on the contralateral upper second premolar under cotton roll isolation using a microbrush (Microbrush International). The sample containing plaque was plated on tryptic soy agar (TSA) plate containing 5% sheep blood. We also added the samples to a 12-well cell culture plate, incubated for 5 days at 37°C in an anaerobic chamber (miniMACS anaerobic work station, Microbiology Inc., USA), and then washed the biofilm with phosphate-buffered saline (PBS). We then incubated the biofilm with 0.1% crystal violet for 10 minutes and then washed again with PBS, air dried, and photographed.
Determine the Multispecies CFUs on the Bracket and Elastomer
To determine colony-forming units (CFUs) of multispecies biofilm on the bracket and elastomers after 2 weeks, they were removed from the subject and washed with PBS and vortexed to remove the biofilm, serially diluted, and plated on TSA plate containing 5% sheep blood and kept at 37°C in anaerobic chamber for 5 days. The colonies were counted using plate counter (Color Qcount, Advanced Instruments, Inc., USA).
Bacterial Growth Medium
Porphyromonas gingivalis was grown in brain heart infusion (BHI) broth containing hemin and vitamin K at 37°C in an anaerobic chamber. 14 Aggregatibacter actinomycetemcomitans was grown in trypticase soy broth supplemented with yeast extract and glucose. The plates were inoculated at 37°C in 10% CO2 for 48 hours. Streptococcus gordonii and Streptococcus mutans were grown on mitis salivarius agar plates or BHI broth in anaerobic chamber with 5% CO2.
Scanning Electron Microscopy
Scanning electron microscopy (SEM) analysis was performed to examine biofilms on brackets and elastomers. After being washed with PBS as mentioned above, bracket and elastomer were then incubated at 37°C in an anaerobic chamber for 5 days in BHI media. After 5 days, the bracket and elastomer were washed with PBS fixed with 2% glutaraldehyde for 2 hours, dehydrated, and processed for SEM (Hitachi SEM S2500; Hitachi High Technologies America, Inc.). 15
Polymerase Chain Reaction-based Identification of Multispecies Bacteria on Brackets
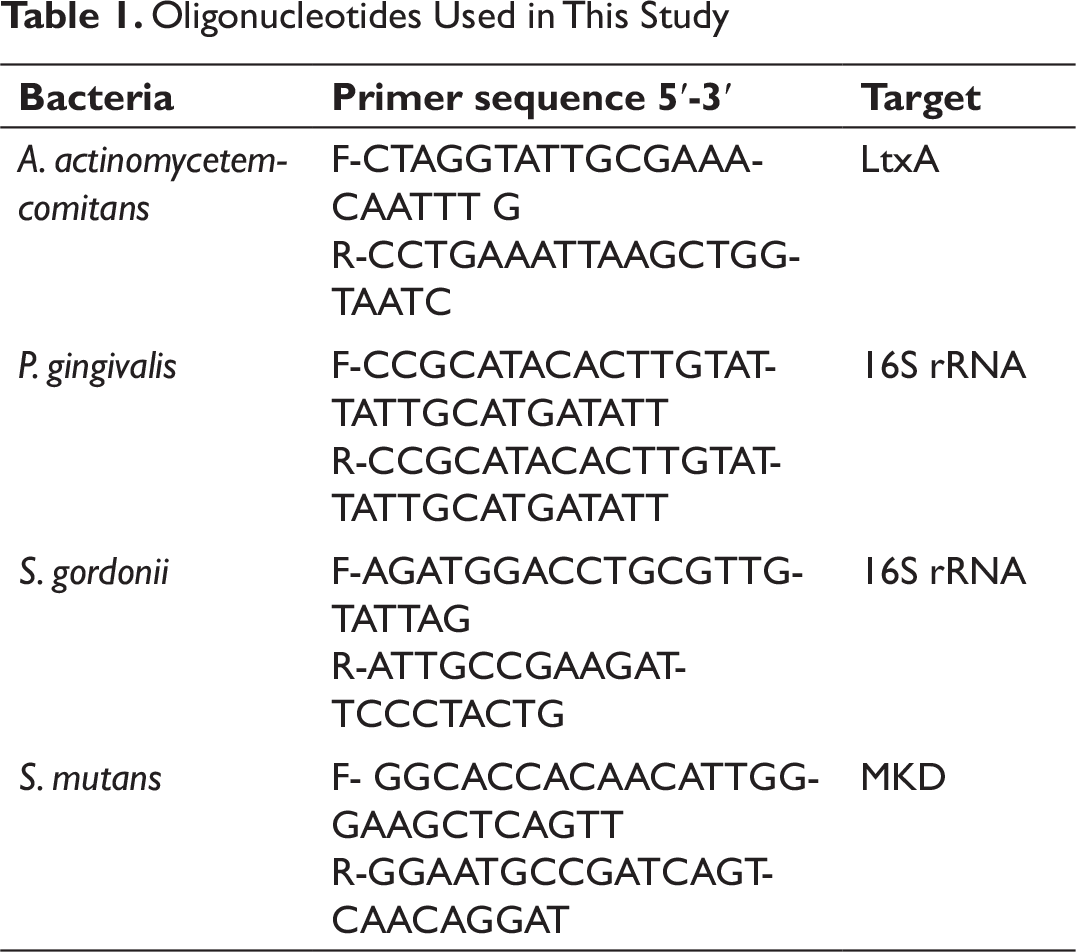
DNA from different orthodontic patient samples was extracted using a kit as described by the manufacturer (Qiagen, Inc., USA). The presence of A. actinomycetemcomitans, P. gingivalis, S. gordonii, and S. mutans DNA on the brackets was analyzed using polymerase chain reaction (PCR) (Table 1). The PCR products were electrophoresed in 1.5% agarose gel, stained with SYBR Green, and photographed (Gel Doc XR with Image Lab Software, Bio-Rad, Inc., USA).
Statistical Analysis
Oligonucleotides Used in This Study
Results
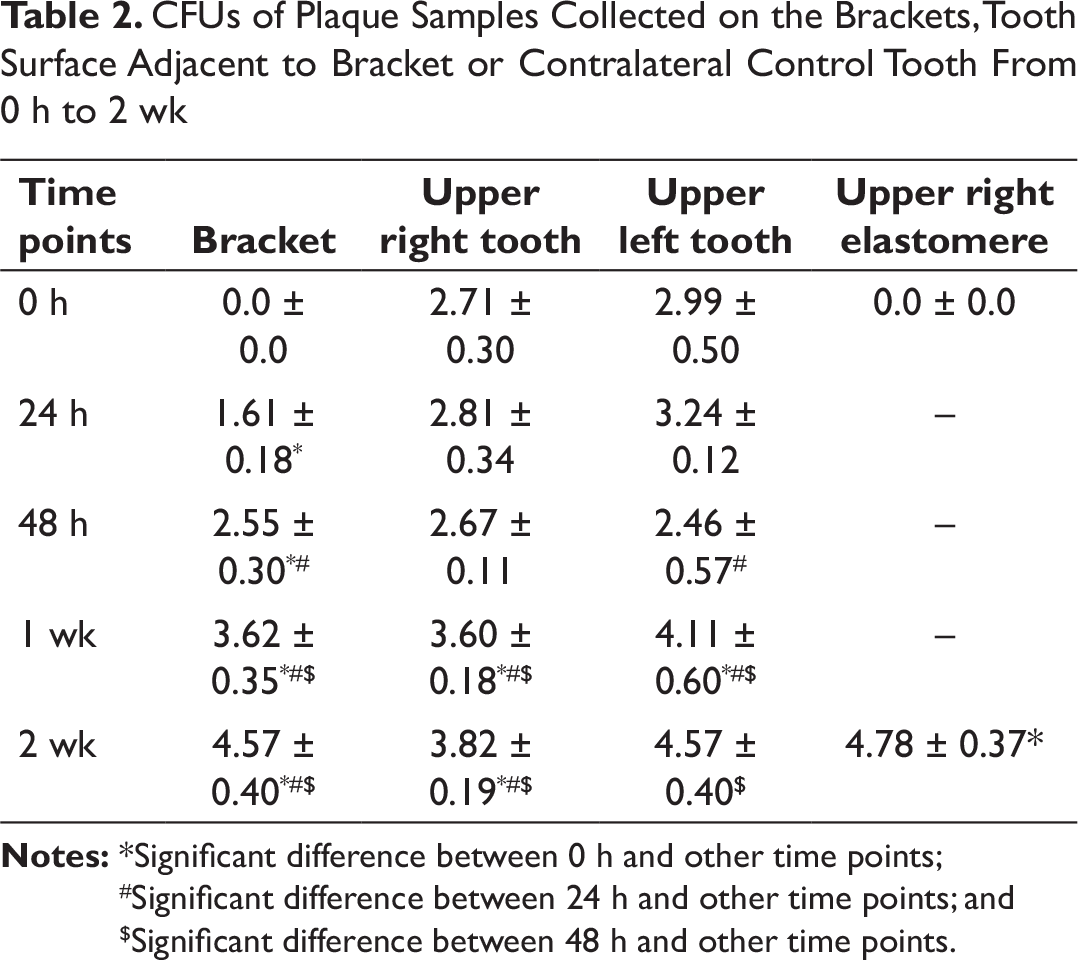
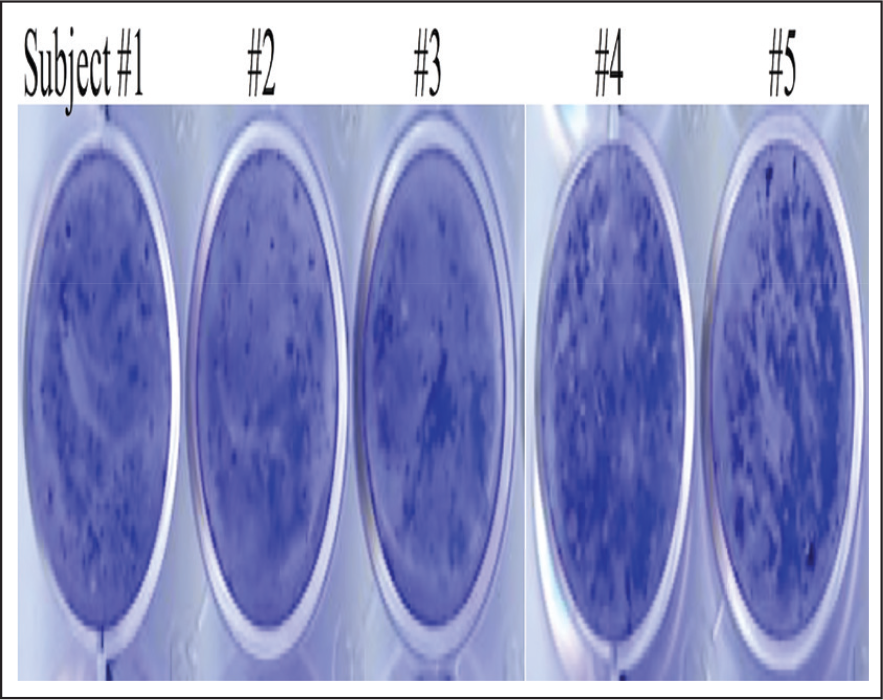
The multispecies bacterial CFUs for plaque samples on the orthodontic bracket from different time intervals show a clear upward trend from 0 hours to 2 weeks. Mean CFUs from each time interval show significant differences compared with all the other time intervals (P < 0.01). Similar results were observed when the elastomer surface was scrapped for bacterial biofilm. The results revealed that after 2 weeks, significant differences in CFUs were observed (4.78 ± 0.37) when compared with the initial time point. Multispecies bacteria within the plaque samples demonstrated that the plaque samples from tooth surface adjacent to the bracket showed a gradual increase in CFUs from weeks 1 and 2 when compared with the other time points. We also analyzed the plaque collected from the contralateral control tooth; it showed no consistent pattern of differences in bacterial colony counts between various time points (Table 2). Crystal violet assay of bracket plaque samples from 2-week time point confirmed the capability of these multispecies bacteria found on orthodontic bracket to form biofilm (Figure 1).
Cfus of plaque samples collected on the brackets, tooth surface adjacent to bracket or contralateral control tooth from 0 h to 2 wk
Crystal violet assay performed on culture plates with bracket plaque samples from 2-week time point from all 5 subjects confirmed biofilm-forming capacity of multispecies bacteria present in the samples.
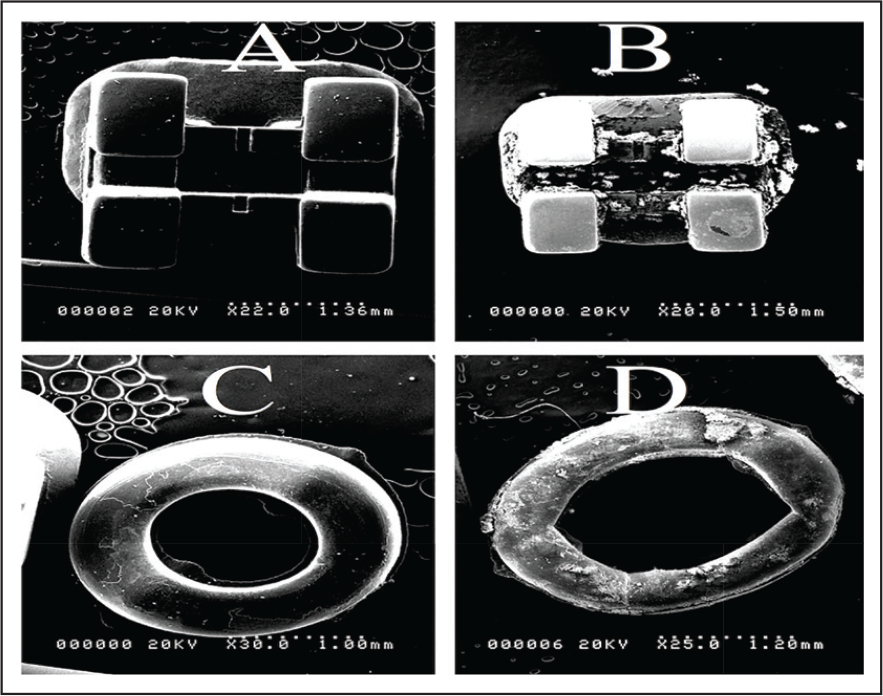
Scanning electron microscope images of bracket and elastomere after 2 weeks collected from healthy subjects. (a) control bracket, (b) bracket removed from subject’s tooth after 2 weeks, (c) control elastomeric module, and (d) elastomeric module removed from subject’s tooth after 2 weeks.
Identification of Bacterial Biofilm on Bracket by PCR
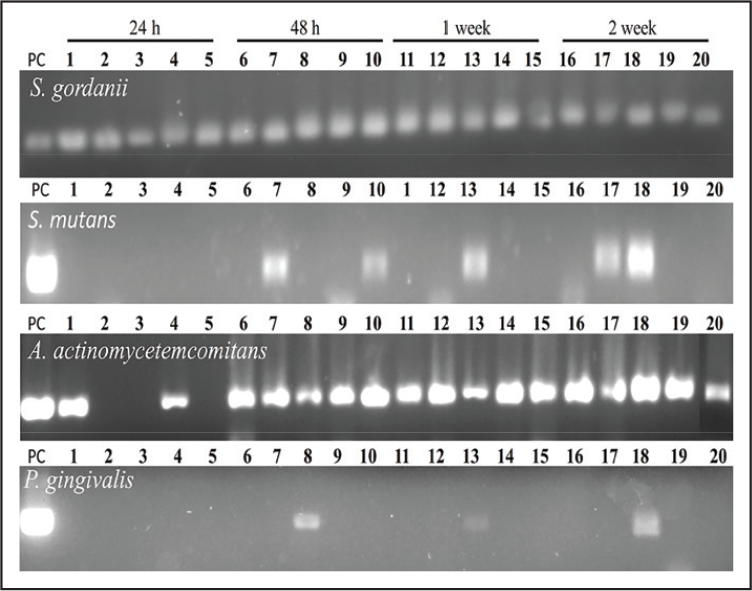
PCR gel electrophoresis results indicate that the biofilm on the brackets from all subjects showed positive for S. gordonii colonization at all time points. P. gingivalis biofilm was confirmed in 1 subject at all time points except 24 hours (Figure 3; lanes 8, 13, and 18). Interestingly, at 24 hours, only 2 subjects were positive for A. actinomycetemcomitans, whereas all subjects were positive from 48 hours to 2 weeks. We detected S. mutans DNA in 2 patients at 48 hours and 2 weeks and in 1 patient at 1 week (Figure 3).
Detection of adherent bacterial dna at the surface of brackets after 2 weeks. The brackets were removed and washed with pbs and then the biofilm was scraped and dna isolated; pcr was performed as described in the materials and methods. Pc: positive control; 1-5, subjects.
To Determine Whether Periodontal Pathogens Form Biofilm on the Bracket In Vitro
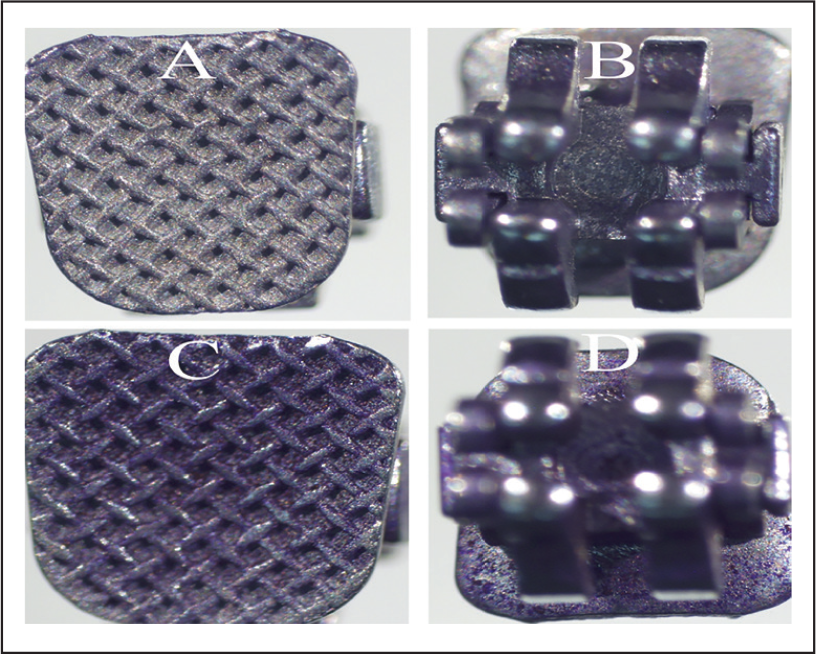
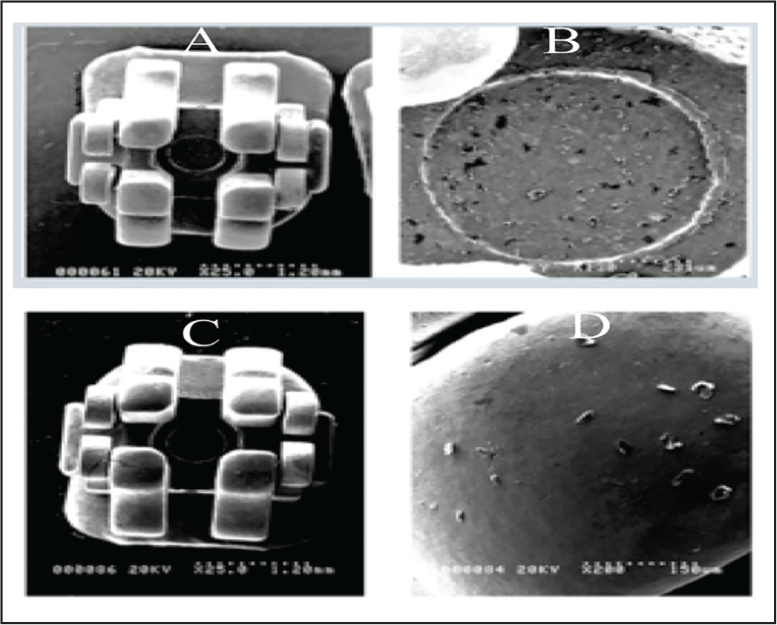
The brackets were incubated either with or without A. actinomycetemcomitans, were washed with PBS, stained with crystal violet (0.1%), and then photographed. The light micrograph showed that a dense biofilm of A. actinomycetemcomitans formed on both sides of the brackets, whereas brackets incubated without A. actinomycetemcomitans showed a clear bracket (Figure 4 A-D). SEM analysis of the bracket showed colonies of A. actinomycetemcomitans biofilm on the bracket surface (Figure 5A and B). A bracket incubated by a similar method with and without P. gingivalis also showed some biofilm, although to a lesser extent than that of A. actinomycetemcomitans (Figure 5C and D).
Light micrograph of crystal violet assay of a bracket after incubation with a. Actinomycetemcomitans for 48 h: (a and b) control bracket (c and d) bracket incubated with a. Actinomycetemcomitans.
Sem analysis detected a. Actinomycetemcomitans and p. Gingivalis biofilm on the bracket surface: (a and b) a. Actinomycetemcomitans and (c and d) p. Gingivalis.
Discussion
Plaque accumulation and oral hygiene issues pose a severe challenge for maintaining oral health of patients during prolonged orthodontic treatment. Fixed orthodontic appliances can act as a retentive site for plaque buildup 16 and are known to cause decreases in plaque pH and increase in salivary S. mutans and gingival inflammation. 17 Although studies have found that the periodontal changes brought on by orthodontic treatment are transient,18, 19 the effects of plaque accumulation due to orthodontic appliances can be more permanent and destructive as in the case of caries and white spot lesions. 17 The study of biofilm formation on orthodontic appliances and the surrounding hard and soft tissues will improve our understanding of the microflora changes that occur during orthodontic treatment and their potential role in causing disease process.
The decision to recruit dental students as opposed to patients was taken to ensure that the subjects will practice good oral hygiene throughout the study and that they will be compliant with coming to the frequent plaque sample collections. We restricted the age of subjects from 25 to 30 years to prevent any confounding factors from age-related oral microflora changes. 20 Our results demonstrate that within 2 weeks of introduction of an orthodontic bracket, a relatively mature biofilm can form on the buccal surface of the bracket in healthy subjects. On the basis of CFUs of bacteria from 0 hours to 2 weeks, the biofilm appeared to grow continuously throughout the 2-week interval. The CFU count increase for tooth surface adjacent to the bracket, however, was more gradual. The fluctuations of CFU on the contralateral control tooth could be due to expected changes and/or inconsistencies in the subjects’ daily diet or brushing habits 21 as these factors are known to cause changes in the plaque density or shifts in microbial community. On the contrary, we noted a clear upward trend on the CFUs on the bracket surface and a gradual but notable increase on the adjacent tooth surface could be attributed to the introduction of a bracket on the tooth.
By the end of 2 weeks, all 5 subjects’ brackets showed positive for S. gordonii, a known early colonizer in the oral cavity. 22 Brackets also showed positive for P. gingivalis and A. actinomycetemcomitans, which are known periodontal pathogens that generally appear as part of a more complex biofilm. 22 These findings are in line with the previous in vivo studies7, 13 that were able to confirm growth of biofilm on stainless steel orthodontic brackets as early as 48 hours after bracket introduction. 7 No in vivo studies have investigated the initial biofilm formation, and our findings offer new knowledge regarding the continuous pattern of biofilm growth throughout first 2 weeks. Previous in vitro studies confirmed that S. mutans and P. gingivalis can attach onto stainless steel orthodontic brackets within 90 minutes of laboratory incubation.11, 12 S. mutans and P. gingivalis showed differing reactions to salivary pellicle, demonstrating that in vivo colonization of bacterial strains may depend on host factors and are species-dependent. 12
Our in vitro study that tested the attachment of A. actinomycetemcomitans on orthodontic bracket when incubated in A. actinomycetemcomitans-treated PBS showed that in 48 hours, the bacteria formed a biofilm on the bracket surface. Additionally, our in vivo PCR results also indicate that by 2 weeks, A. actinomycetemcomitans had colonized the bracket surface in all the subjects. In a study by Nelson-Filho, 23 A. actinomycetemcomitans was detected on all of the metal brackets via checkerboard DNA-DNA hybridization technique from their 35 subjects after 30 days of in vivo bracket placement. Another study by Pejda 16 found that subjects with conventional metal brackets have higher A. actinomycetemcomitans counts subgingivally compared to self-ligating brackets in 18-week period.
The SEM images show the differences between smooth surface of a control bracket and elastomer to the clearly visible irregular surface of the experimental ones. Surface roughness appears to be concentrated in the archwire slot region. This confirms the findings from previous studies that noted the highest amount of biofilm in the slots, which can act as a heavy retentive site for plaque.24, 25 It is important to note that these studies were in vitro and the findings may have been different in vivo with an archwire actually engaged in the bracket slot.
Conclusion
This study demonstrated that both periodontal pathogen and cariogenic bacterial biofilms were formed on the bracket as early as 24 hours. The results of our study provide an insight into the initial biofilm formation on stainless steel brackets. The clinical implication of these findings is that more aggressive oral hygiene measures may be necessary from the beginning of the treatment to control further increase in colonization by periodontal pathogens, which could contribute to future periodontal issues.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors wish to thank the Department of Orthodontics for their generous funding for the project.