
Abstract

Keywords
On January 2, 2023, an American professional football player experienced a collision to the chest and seconds later he collapsed to the ground. Cardiopulmonary resuscitation and cardiac defibrillation were administered in a timely fashion which contributed to his survival and continued recovery. The news media interviewed several medical experts, not affiliated with the case, who suggested commotio cordis was the likely diagnosis. The breadth of media coverage raised significant awareness and curiosity of this rare human condition (https://www.npr.org/2023/01/03/1146744819, assessed 01/18/2023).10,21,23
Commotio cordis is caused by a low-energy, blunt-force trauma to the chest that initiates cardiac arrest, and affected individuals may not survive without timely cardiopulmonary resuscitation and defibrillation. Commotio cordis is likely under-reported with ~20 to 30 cases a year, but the incidence started to increase in the late 1990s due to awareness from high profile review articles.3,16,23 Increased awareness and increased availability of automated external defibrillators (AEDs) have significantly raised the survival rate from about 10% to 15% in the 1990s to nearly 60% in the early 2000s. 11 Commotio cordis is most commonly seen in young athletes and is the second leading cause of sudden death for this population. 3 Baseball is the principal sport where cases originate, but several other sports have representation, especially those with exposure to chest trauma from hard projectiles (e.g., balls and pucks) or direct physical contact from participants.22,23 Commotio cordis can be induced in several nonsport situations too including assaults/fights, traffic accidents, work-associated injuries, accidental falls, and even playful fights.11,18,21,24 Blunt-force impact to the chest is a necessary precursor for commotio cordis diagnosis but is not sufficient on its own for definitive diagnosis.3,18 Fatal impacts to the chest require pathologist examination for cardiac and extracardiac lesions.3,25 If cardiac involvement is suspected, the autopsy can determine if the heart has pre-existing or trauma-associated structural lesions (contusio cordis). 3 Commotio cordis is a diagnosis by exclusion of structural lesions to the heart, so if autopsy examination is not available in a sudden death, then it is recommended to qualify the diagnosis of commotio cordis as “possible.” 18 Studies of commotio cordis cases in humans have identified these clinical commonalities, including precordial chest trauma, lack of structural lesions in heart, and ventricular fibrillation (VF) when electrocardiogram reads of cardiac arrests were available.3,22,23
Commotio cordis was recognized as early as the mid-19th century, and anecdotal case reports consistent with the condition were reported more than a century earlier.7,24,29 Interestingly, the ancient Chinese martial art known as Dim-Mak (touch of death) taught that a strike to the precordium could be a fatal blow to an opponent.6,21 In the 1930s, Schlomka led multiple studies of rabbit, cat, and dog models.24,27 Cumulatively, these studies suggested that the type of impact, force of impact and precordial location were relevant factors in commotio cordis pathogenesis, and these studies also excluded aberrant autonomic reflexes as a relevant factor. Rat, rabbit, and canine models have contributed to the knowledge base of commotio cordis,2,4,32 but the significant differences in body size, projectile force and projectile dimensions in these studies have limited direct translational applications. Given the rarity and lethality of commotio cordis in humans,1,23 detailed understanding of risk factors, mechanisms, or preventive interventions were considered by some to be nearly impossible without development of new models.
In 1998, a novel swine model of commotio cordis was reported that produced VF following a low-energy, chest impact. 16 This model has been remarkably insightful for clarifying commotio cordis mechanisms, testing of therapies, and driving the development and validation of protective gear/equipment for prevention (Table 1). Low-energy, blunt-force impacts to the precordium caused intracardiac pressures that stretched the myocardium sufficiently to activate K+ATP channels (a process known as mechanotransduction) producing VF (ie, cardiac arrest). For regulation-sized baseballs, the baseline threshold for VF induction in the model was 20 to 25 miles-per-hour (mph) that peaked at ~40 mph and then regressed at higher velocities in a Gaussian-like curve. It is interesting to note that for youth baseball, the common velocity for thrown balls is estimated between 30 and 50 mph, very similar to the window of VF induction (~25-40+ mph). 28 Contusio cordis was also detected in the model as papillary muscle rupture or myocardial wall tears/perforation. It was initially evident near ~40 to 50 mph, and its incidence elevated rapidly with increased velocity. From the swine model, informative concepts of cardiac trauma emerged. Velocity of precordial chest trauma directly correlated with left ventricular pressures, but the induction of VF (commotio cordis) and structural lesions (contusio cordis) were dramatically different in onset and distribution (Fig. 1). 15
Key clinical features of commotio cordis that were illuminated by swine models.
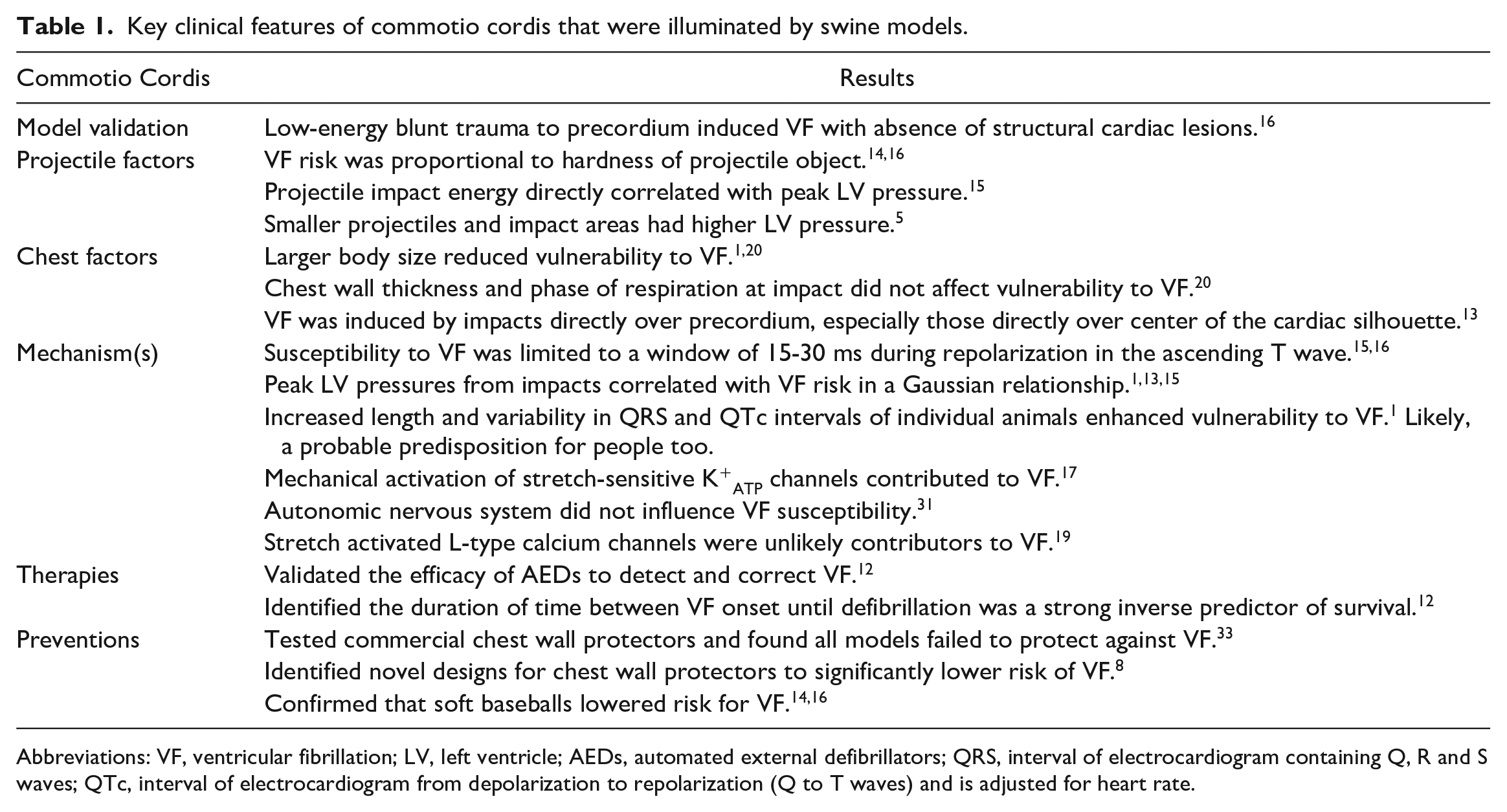
Abbreviations: VF, ventricular fibrillation; LV, left ventricle; AEDs, automated external defibrillators; QRS, interval of electrocardiogram containing Q, R and S waves; QTc, interval of electrocardiogram from depolarization to repolarization (Q to T waves) and is adjusted for heart rate.
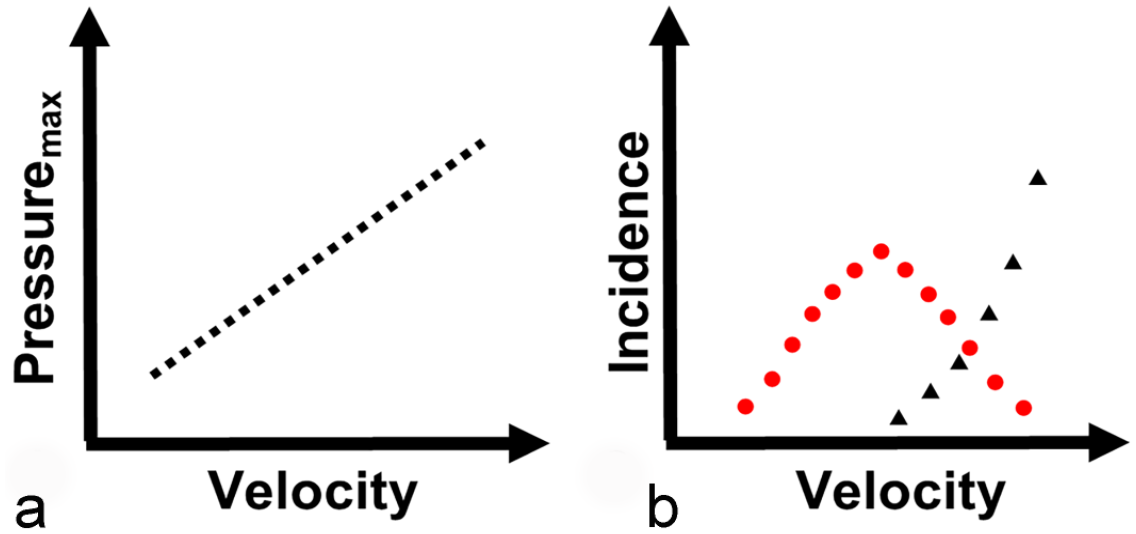
Concepts derived from the swine model of commotio cordis. (a) Schematic figure showing a linear relationship between projectile velocity and peak left ventricular pressure (Pressuremax). (b) Schematic figure showing the relationship between projective velocity to the relative incidence of commotio cordis (red circles) and contusio cordis (black triangles).
Commotio cordis is in many ways an example of one medicine in action. The swine model provided mechanistic insights of the condition, tested therapies and guided development of novel protective gear to mitigate risks for many people. Interestingly, commotio cordis is recognized as a possible differential diagnosis in veterinary medicine, 25 but Pubmed and Google searches for “commotio cordis” AND “veterinary” (assessed 01/18/2023) yielded no obvious case reports. Given that animal models are susceptible2,4,9,16,27,32 and the fact that chest traumas are not uncommon in veterinary medicine,25,26,30 it would seem that increased awareness in the veterinary community might, like in humans, further illuminate this condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.