
Abstract
This report describes periarticular plasma cell tumors with abundant amyloid in 11 cats. The tarsus was the most commonly affected joint (10/11), and the masses were often circumferential around the tarsal joint, involving the dermis and subcutis. The 2 cases in which synovium was examined had neoplastic cells expanding the synovium. Three of the 5 cases staged radiographically had bony lysis of the affected joint. Cutaneous biopsy specimens often consisted of more amyloid than plasma cells, making the diagnosis difficult on small samples. Follow-up information was available in 7 cases; in those cases, the median survival was 194 days (range 53–671 days). Four cases had confirmed metastases, most often to regional lymph nodes, liver, and spleen. Although canine cutaneous plasma cell tumors are typically benign, those with abundant amyloid surrounding the joints of cats may involve deeper tissues and have a more aggressive behavior. These tumors can be difficult to diagnose due to low cellularity and abundant amyloid.
Myeloma-related disorders in cats include 8 categories: multiple myeloma, cutaneous extramedullary plasmacytoma, noncutaneous extramedullary plasmacytoma, solitary plasmacytoma of bone, IgM macroglobulinemia, immunoglobulin-secreting lymphoma, immunoglobulin-secreting leukemia, and plasma cell leukemia. 8 Cutaneous extramedullary plasmacytomas in dogs are usually benign, but some are thought to be manifestations of multiple myeloma. 15 Multiple myeloma originates in the bone marrow and has a monoclonal gammopathy and multiple osteolytic bone lesions. 11,15 The purpose of this report is to describe a unique form of plasma cell tumor in cats with a periarticular location, abundant amyloid, and a poor prognosis, so that diagnostic pathologists can recognize the lesion and provide prognostic information.
The anatomic pathology databases at the University of Tennessee and University of Georgia Colleges of Veterinary Medicine were searched from January 1, 2002, to December 30, 2019, for feline species combined with the words amyloid and plasmacytoma or plasma cell. All reports identified in the search were reviewed, and cases of cutaneous plasma cell tumors with amyloid were selected. The 11 cases selected were routinely processed biopsy submissions with hematoxylin and eosin–stained slides. All cases had MUM1 immunohistochemistry performed to confirm the neoplastic cells as plasma cells; the protocol used a Dako Target Retrieval solution (pH 9.0) and a Dako monoclonal antibody. Submitting veterinarians were contacted to obtain treatment and survival information.
The site, age, sex, mitotic count, survival, and information regarding metastasis for each case are given in Table 1. The average age of the affected cases was 12 years (range 8–18 years). Seven cases were neutered males, and 4 were spayed females. A male predominance in myeloma-related disorders has been previously reported in cats 7 and humans. 11 Nine cases were domestic shorthair; 1 was a Siamese mix and 1 was a domestic longhair. Nine cases were presented for a mass found by the owner; 2 cases were identified during routine physical exam by their veterinarian. Ten cases had masses surrounding the tarsal joint; 1 mass surrounded the elbow. In 6 cases, the left limb was affected and in 5 the right. Four cases were lame at the time of presentation. The duration of clinical signs prior to diagnosis was 2 weeks to 2 months in the 9 cases presented for a mass. The swellings were soft to firm, multinodular, sometimes alopecic, and occasionally ulcerated. Clinically, the masses began on the medial or lateral side of the joint and eventually became circumferential. Marked edema of the affected hind limb occurred in 2 cases; in one case the proximal limb was affected and in the other it was the distal limb. Two cases (cases 4 and 7) were initially suspected to be abscesses and were lanced; in one, “thick clotted” material was extruded from the mass.
Clinical findings, mitotic count, and outcomes in 11 cats with periarticular plasma cell tumors.
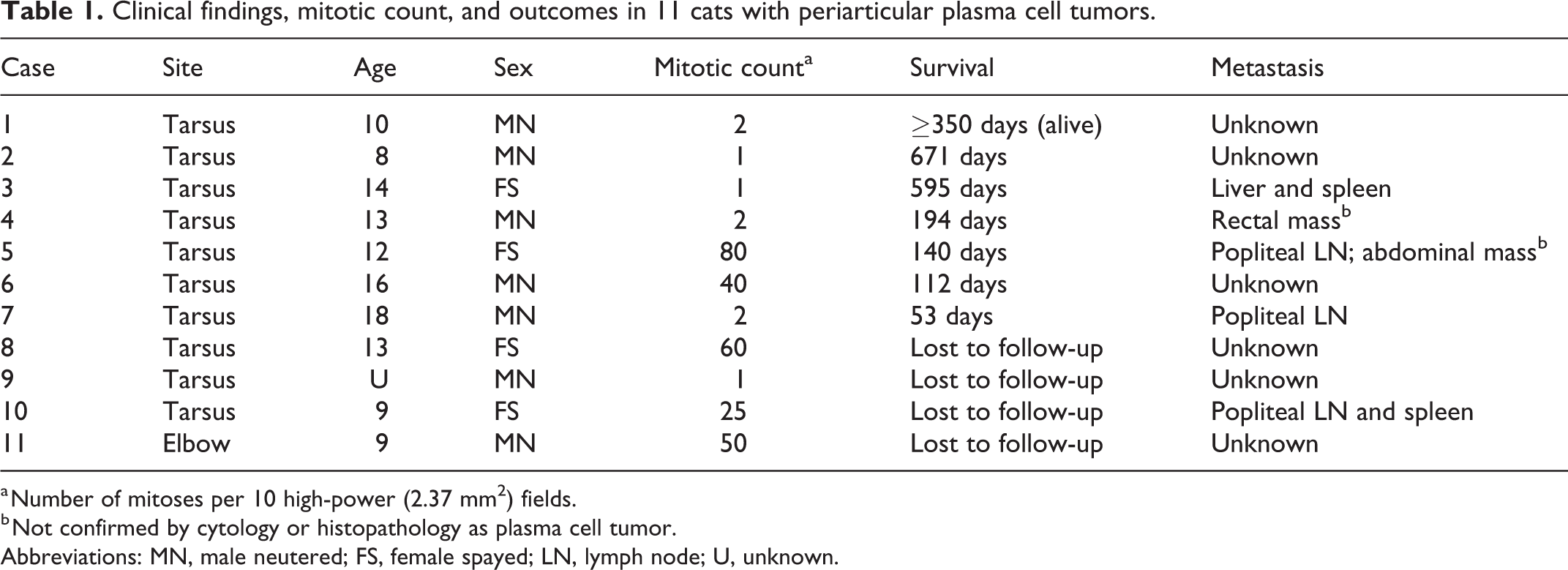
a Number of mitoses per 10 high-power (2.37 mm2) fields.
b Not confirmed by cytology or histopathology as plasma cell tumor.
Abbreviations: MN, male neutered; FS, female spayed; LN, lymph node; U, unknown.
Treatment included amputation alone in 4 cases (cases 2, 4, 5, 8), amputation, melphalan and prednisolone in 2 cases (cases 3 and 10), palliative therapy (buprenorphine, gabapentin, and antibiotics) in 2 cases (cases 1 and 7), and radiation in 1 case (case 6). Eight cases had bloodwork performed. All 8 were mildly anemic. Four had lymphopenia; 2 were hyperglobulinemic, and 1 was hypercalcemic. Protein electrophoresis was performed on 2 cases and were slightly abnormal (wide β2 peak in one, and a polyclonal gammopathy in the other); both were thought to be insignificant or consistent with chronic inflammation.
Cytology was performed on the tarsal mass in 6 cases: 3 were diagnosed as possible sarcoma (cases 3, 7, and 10), 2 as round cell tumor (cases 5 and 6), and 1 did not report the results (case 2). Cytology was performed for staging on 4 cases: 2 had neoplastic plasma cells in the ipsilateral popliteal lymph node (cases 7 and 10), 2 had neoplastic plasma cells in the spleen (cases 3 and 10), 1 of which also had neoplastic plasma cells in the liver (case 3). Neoplastic plasma cells were identified cytologically by their blue cytoplasm, eccentric nuclei, clumped chromatin, pink fringe at cytoplasmic margin, moderate anisocytosis and anisokaryosis, binucleation, and mitotic figures. Case 5 had normal cytology results from the lymph node, liver, and spleen.
Histopathology of the 11 cases was remarkably similar. All tumors were multinodular and contained abundant amyloid. Less than 50% of each mass consisted of neoplastic plasma cells, which were often at the periphery of the nodules (Fig. 1). The cells had typical features of neoplastic plasma cells, including hyperchromatic nuclei, coarsely clumped chromatin, anisokaryosis, binucleation, and occasionally multilobular nuclei or ≥3 nuclei (Fig. 2). The nuclei were labeled with antibodies to MUM1 in all cases. The amyloid was variably congophilic (Fig. 3), birefringent (Fig. 4), and variably resistant to potassium permanganate. The amyloid formed poorly demarcated nodules, reticular trabeculae, and surrounded blood vessels (Fig. 3). The amyloid was often surrounded by epithelioid macrophages and multinucleated giant cells, some of which contained intracytoplasmic pieces of amyloid. The multinucleated giant cell nuclei were negative for MUM1. One case had chondroid and osseous metaplasia within the amyloid. Lymphocytes and fibroblasts were also scattered throughout the affected tissue, which is the likely explanation for the 2 cases that were diagnosed as possible sarcoma on cytology. The mitotic count varied from 1 to 80 per 10 high-power fields (2.37 mm2, 10 based on the cellular areas of the tumors, not areas consisting only of amyloid; Table 1). Case 3 had so few plasma cells on the initial biopsy that it was diagnosed as cutaneous amyloidosis with granulomatous panniculitis. The amyloid in that case was not resistant to potassium permanganate pretreatment, so it was thought to be AA amyloid. A recent publication on the diagnosis of light-chain amyloidosis found that not all cases are congophilic or resistant to potassium permanganate pretreatment. 5
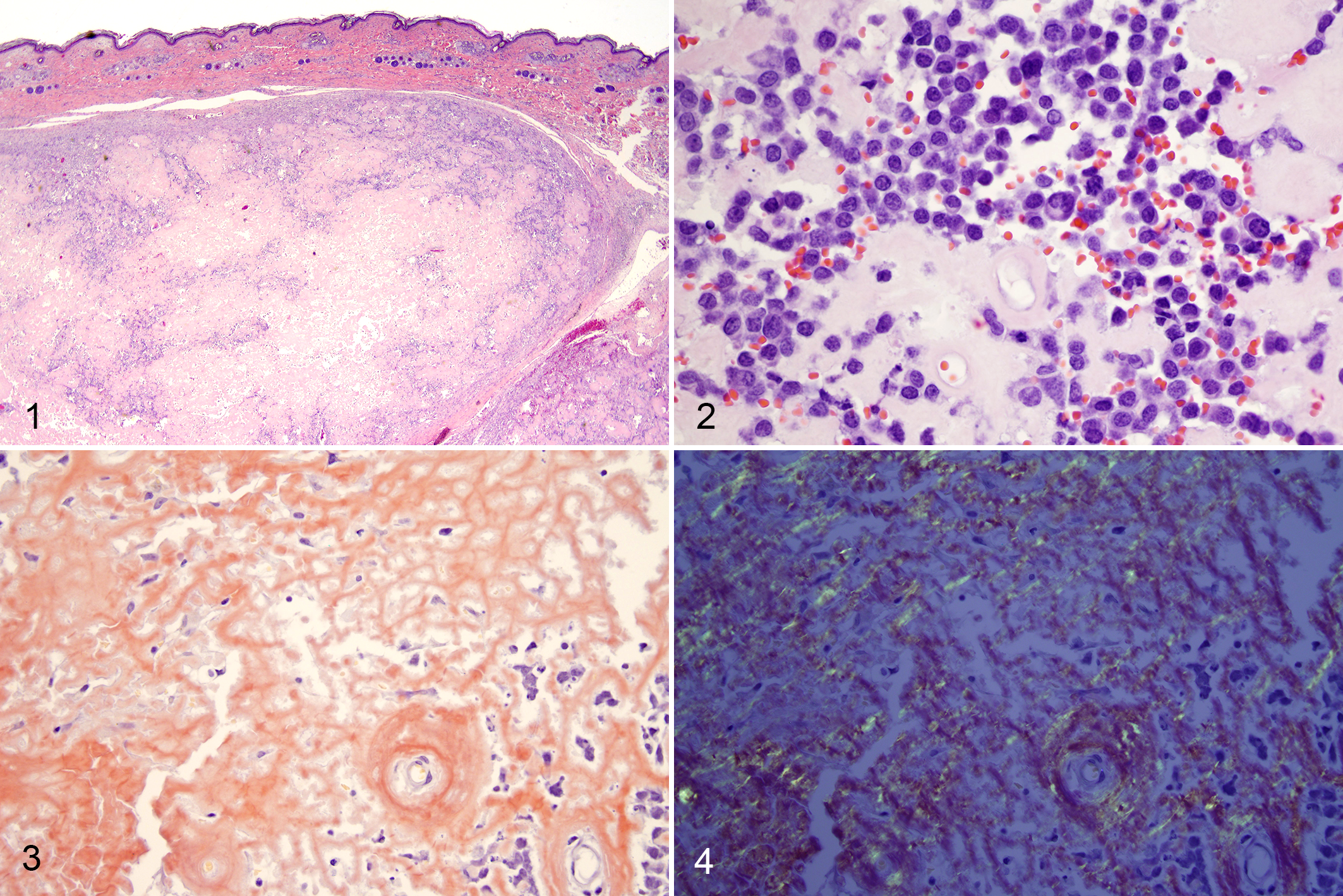
Plasma cell tumors with abundant amyloid, tarsal masses, cat.
Three cases (cases 4, 7, and 11) had radiographically visible lysis in multiple bones of the affected joint (Fig. 5). The lytic lesions crossed the joint and were indistinct (not punctate), and no other bones were affected in the 5 cases staged radiographically. One of the cases with radiographically visible lysis was confirmed to have replacement and expansion of the marrow space by neoplastic plasma cells and abundant amyloid (Fig. 6). That same case had neoplastic plasma cells and amyloid expanding the synovium (Fig. 7). One additional cat (case 1) had involvement of the joint capsule and synovium in the incisional biopsy sample. One cat (case 10) had diffuse osteopenia diagnosed by a radiologist at the referral hospital on staging thoracic radiographs. One cat (case 6) had a “periosteal reaction to the soft tissue mass” around the joint and degenerative joint disease of the affected tarsus. These findings are not typical of multiple myeloma, which causes punctate lysis without bone production and does not form amyloid in the marrow. 14
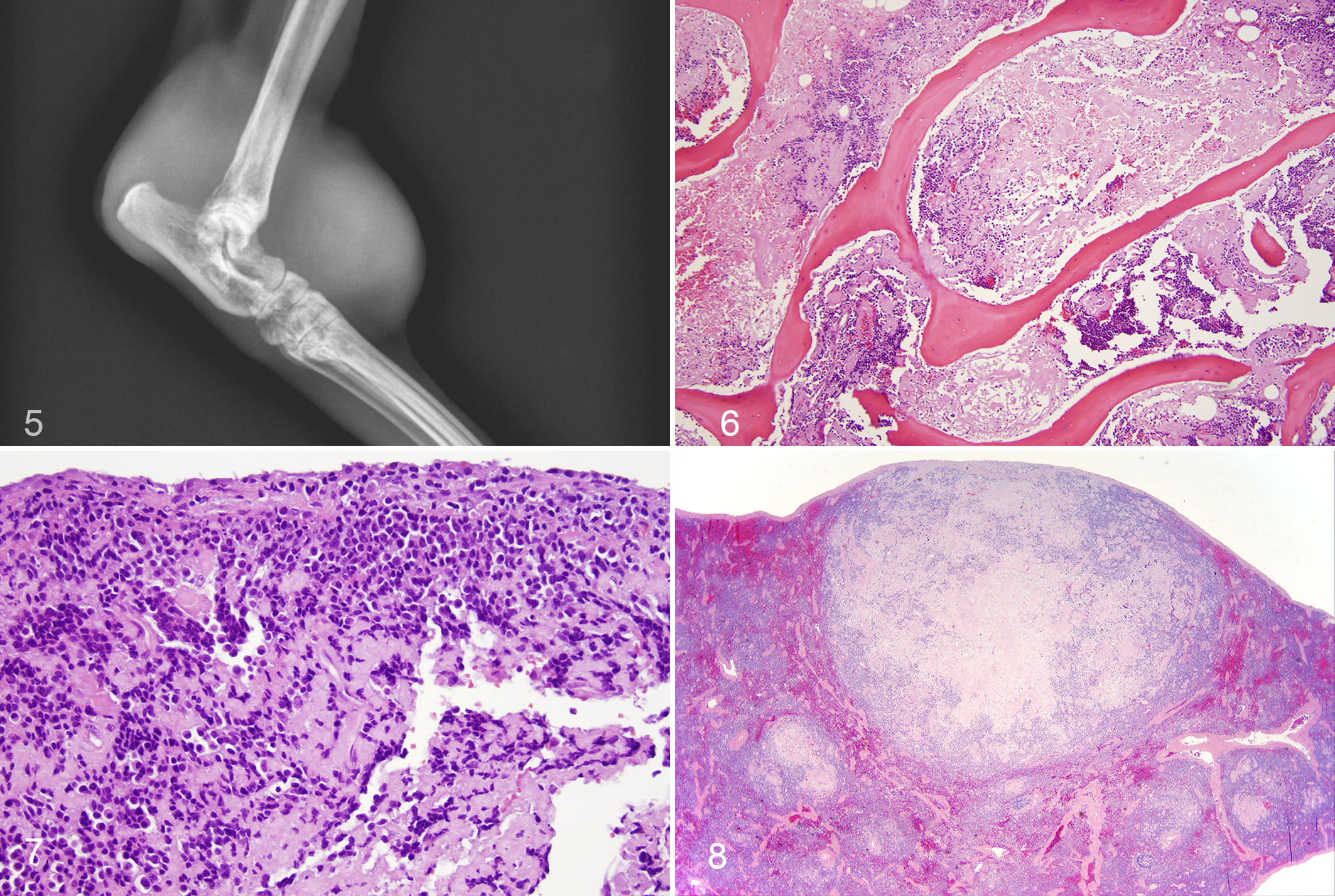
Plasma cell tumors, cat.
Survival information was available for 7 of the 11 cases. One died at home, 5 were euthanized, and 1 was alive 350 days after diagnosis. Overall median survival time was 194 days, and the 1-year survival rate was 33% (2/6). Four cases (cases 3, 5, 7, and 10) had metastasis to the ipsilateral popliteal lymph node; 3 confirmed by cytology and 1 by histopathology, where the metastatic nodule consisted of neoplastic plasma cells without amyloid. Two cases had metastasis to the spleen, confirmed by cytology (cases 3 and 10) and histopathology (case 3), where the masses resembled those in the skin, with abundant central amyloid and peripheral neoplastic plasma cells (Fig. 8). Case 3 also had metastasis to the liver, where the sinusoids were expanded by neoplastic plasma cells and amyloid. Two cases (cases 4 and 5) had palpable abdominal masses at the time of euthanasia that were not confirmed by cytology or histopathology as metastases. Death (case 7) or euthanasia (5 other cases with follow-up) was thought to be due to the plasmacytoma or a combination of the plasmacytoma and comorbidities such as renal failure or heart failure in all 6 cases.
Two retrospective studies of feline myeloma-related disorders found that cats are more likely to have extramedullary involvement and less likely to have bone lesions, compared with humans. 8,9 In those studies, most of the cats with cutaneous lesions were not systemically ill or hyperglobulinemic. Amyloid was “uncommonly observed.” A retrospective study of 9 extramedullary plasmacytomas in cats found 3 to have amyloid, which was identified by immunohistochemistry as lambda light chain in all 3 cases. 7 The metatarsus was 1 of 7 locations listed in that study. Plasma cell tumors composed mostly of amyloid are termed “amyloidomas” in humans, where they have an excellent prognosis. 1,16 The amyloid aggregates are proposed to be toxic to the neoplastic plasma cells, resulting in a mass composed of mostly amyloid. 16
It is unclear if these tumors arose in the skin, bone marrow, or other tissue in this area. It is tempting to speculate that the tumors originated in the synovium, given the periarticular location and involvement of bone as well as overlying subcutis and skin in some cases, but only 2 cases (cases 1 and 4) had synovium available for examination (Fig. 7). The synovium is a rare location for extramedullary myeloma in humans, but the knee joint was the first site of extramedullary multiple myeloma in one human case, in which multiple myeloma bone lesions were not present at the time of diagnosis, but developed later. 6 Solitary plasmacytoma of bone in humans rarely affects the ankle and most progress to multiple myeloma. 4
In 1996, the recommended site of feline vaccines was moved to distal limbs, and vaccine-associated sarcomas now occur there. 13 The possibility that the plasma cell tumors in this report could be related to vaccination was considered, but information about vaccines and their locations was not available for the cases in this report. However, one of the two previously reported cases of tarsal plasma cell tumors in cats was in 1989, 3 prior to the recommendation to vaccinate on the limbs. The tumor in that case was composed mostly of amyloid, and the cat died 6 weeks after amputation. The other tarsal plasmacytoma case report was in 2004; that neoplasm progressed to multiple myeloma and the cat was euthanized 5 months after diagnosis. 12 Cutaneous lymphoma of the tarsus has been reported in 23 cats. 2 Three of those were stained with Congo red and 2 were positive. Only 2 cats in that study had lameness, but it is unclear if the lame cats and those with amyloid were the same.
In summary, malignant plasma cell tumors with abundant amyloid occur in the tissues surrounding the tarsal joint in cats. The abundant amyloid makes these tumors difficult to diagnose with small biopsy samples. Lysis of the bones of the tarsus was present in some cases, but typical punctate widespread bony lesions were not. In this study, cats with periarticular plasma cell tumors with abundant amyloid did not progress to typical multiple myeloma, but did develop lymph node, splenic, and hepatic metastasis. Median survival was 194 days in the 7 cases with follow-up information.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.