
Abstract
Four captive, lesser hedgehog tenrecs (Echinops telfairi) were euthanized for soft bones that prevented normal mastication and/or ambulation. Antemortem radiographs (available in 2 cases) revealed osteopenia. Antemortem bloodwork (available in 2 cases) revealed hypophosphatemia. Dietary history (available in 2 cases) indicated the animals were eating only insects. Histologically, all examined bones had wide osteoid seams that caused expansion of the cortices. Osteoid deposition was exuberant and it partially filled marrow cavities (hyperostosis). Nondecalcified sections of bone (available in 2 cases) revealed that osteoid was poorly mineralized, consistent with osteomalacia. Insects are poor dietary sources of vitamin D, and dietary vitamin D deficiency is considered the most likely cause for metabolic bone disease in these animals.
Lesser hedgehog tenrecs (Echinops telfairi) are small (approximately 100 g) placental mammals from the family Tenrecidae and are native to Madagascar. Genetically, tenrecs are part of the Afrotheria assemblage, indicating their genetic relatedness to elephants, hyraxes, dugongs, and manatees. Tenrecs were historically called insectivores, but are actually faunivores and eat a wide variety of animals, many of which are terrestrial insects. 5
The most commonly reported cause of death in captive lesser hedgehog tenrecs is neoplasia, with hepatic lipidosis, bacterial infection, cardiomyopathy, and renal disease also commonly reported. Approximately 50% of deaths in lesser hedgehog tenrecs are of unknown cause, and many of those occur in the neonatal period. 4 The aim of this study is to describe a disease in lesser hedgehog tenrecs that was previously unpublished and was the cause for death or euthanasia in this case series.
Four cases (cases 1–4) of osteomalacia were diagnosed histologically in captive tenrecs. Clinical information was requested from clinicians, including clinical history, animal origin, radiographs, blood work, urinalysis, and diet. Information was collated when available. For each case, a complete necropsy was performed, and tissues were collected in 10% neutral buffered formalin. Representative tissue sections were processed, embedded in paraffin blocks, and 5 µm sections were stained with hematoxylin and eosin (HE). Spinal column, skull, and long bones from cases 1, 3, and 4 and mandible from case 2 were decalcified for several days using BBC Rapidcal (Fischer Scientific) in cases 1 and 2, 15% formic acid in case 3, and 5% trichloroacetic acid in case 4. Additional sections of rib and long bone were also processed without decalcification in cases 2 and 4, respectively. Control tissues included long and skull bones from a 2.5-year-old male tenrec that died from anaphylactic shock and long bones from an 11-year-old male that died from bacterial infection.
Cases 1 and 2 were a 5-year-old male and female, respectively, from the same litter, born in captivity at a zoo in Illinois. At 6 months of age, the animals were acquired by a second zoo in Florida. Case 1 had hemiparesis (forelimb). Case 2 had a soft lower jaw that prevented him from chewing. Additional clinical history, diagnostics, and necropsy findings were not available for either case.
Case 3 was a 4-year-old male born in captivity at a zoo in Virginia and later acquired by a zoo in northern California. The animal was offered a balanced diet including Mazuri Insectivore chow diet, mixed vegetables, mealworms, and waxworms. The animal selectively ate only mealworms and waxworms, which were not supplemented with vitamins. Radiographs revealed loss of bone density (osteopenia), particularly of the long bones, approximately 6 months prior to the onset of clinical signs (12 months prior to death; Fig. 1). The animal had progressive tetraparesis for 6 to 8 months prior to death. One to 9 months prior to death, serial bloodwork revealed serum phosphorus ranging from 1.7 to 2.5 mg/dL (reference 4.7–6.5 mg/dL) and serum calcium ranging from 10.8 to 12.8 mg/dL (reference 9.5–10.9 mg/dL). 6 The animal was given empirical calcium therapy 2 months prior to death, which did not dramatically improve clinical signs or serum chemistry abnormalities, and was euthanized for presumed metabolic bone disease.
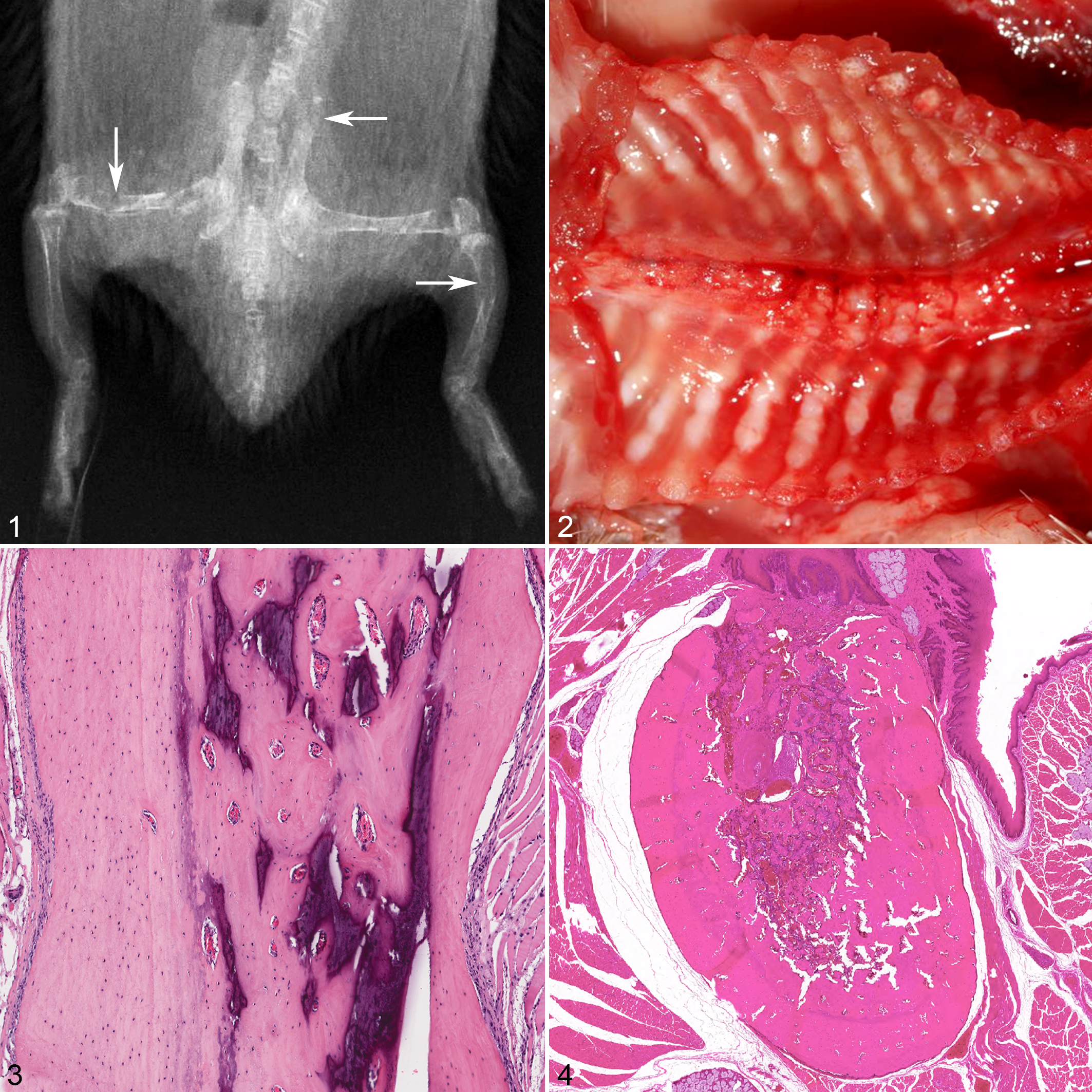
Osteomalacia, lesser hedgehog tenrecs.
Case 4 was a 2-year-old female born in captivity at a wildlife park in Texas, later acquired by a zoo in southern California, and subsequently transferred to a zoo in Washington, DC. The animal was offered a balanced diet including Mazuri Insectivore chow, Mazuri Insectivore ground diet, and mealworms. The tenrec selectively ate only the mealworms, which were not supplemented with vitamins. Mealworms were dusted with Mazuri Insectivore ground diet, but it was not readily retained on the worms. The animal had progressive lameness of unspecified duration. Radiographs revealed severe loss of bone density (osteopenia), particularly of the long bones, and the tenrec was euthanized for presumed metabolic bone disease. Bloodwork 6 months prior to death revealed hypophosphatemia of 1.5 mg/dL (reference 4.7–6.5 mg/dL) and serum calcium level of 11.4 mg/dL (reference 9.5–10.9 mg/dL). 6
Gross necropsy information was available for cases 3 and 4, which had similar findings. Case 3 weighed 99 g and case 4 weighed 100 g at the time of death. Long bones of the forelimbs, hind limbs, and ribs had multifocal, irregular thickening and multifocal curvatures (Fig. 2). Multiple long bones were soft and pliable. Both animals had scoliosis. Adipose stores were adequate in both animals.
Microscopically, in cases 2 and 4, sections of bone that were not decalcified prior to processing had only minimal multifocal mineralization of less than 10% of the bone (Fig. 3). In all animals, the cortices were multifocally expanded by well-organized, predominantly central lamellar and peripheral woven bone that bulged from the periosteal surfaces and obscured the preexisting cortical margins (wide osteoid seams; Fig. 4). Occasionally, the cambium layer of the periosteum was thickened (hyperplastic) over regions of superficial woven bone. Medullary trabeculae were markedly thickened by woven bone and crowded out marrow elements. Cartilage of the physes in all examined long bones and vertebrae was retained and bordered by a horizontal plate of metaphyseal bone (ie, there was no evidence of active endochondral ossification). In the bone, there was no evidence of increased numbers of osteoclasts. In cases 3 and 4, thyroid tissue had collapsed follicles with moderately reduced colloid. Thyroid tissue was not available for histologic examination for cases 1 and 2. Parathyroid gland tissue was not identified in any case.
Case 1 had no additional microscopic findings. Case 2 had abundant, intracytoplasmic, yellow, granular material in hepatocytes and to a lesser extent in renal tubular epithelial cells. Additional microscopic diagnoses in case 3 included moderate microvesicular hepatic lipidosis, moderate hyperkeratotic dermatitis, and splenic extramedullary hematopoiesis. Case 4 had keratin and bacteria in the vaginal lumen. All animals had adequate adipose stores grossly and histologically. The control animals had retained physeal cartilage of the long bones without active endochondral ossification, similar to that seen in cases 1 to 4.
In skeletally mature vertebrates, deposition of abundant unmineralized osteoid, combined with radiologic evidence of osteopenia and clinical evidence of soft bones, is consistent with the diagnosis of osteomalacia. The most common cause of osteomalacia in animals is inadequate vitamin D and/or phosphorus. 2 Phosphorus deficiency is usually the result of inadequate dietary phosphorus. Inadequate vitamin D has many causes, including genetic predisposition, dietary deficiency, ingestion of vitamin D antagonists, and inadequate exposure to ultraviolet light. The 2 animals for which detailed clinical history was available both selectively ate only mealworms and waxworms and did not eat the supplemented, formulated food. Mealworms and waxworms contain adequate, bioavailable phosphorus for mammals, but inadequate vitamin D. 3 Commercially bred insects are known to have major deficits in multiple vitamins, including vitamin D, which frequently requires supplementing (or “gut loading”) insects with vitamins prior to feeding captive insectivores. Commercially bred waxworms and mealworms had undetectable levels of vitamin D in one study. 3 Vitamin D binds to receptors on renal tubular and intestinal epithelial cells, resulting in increased absorption of phosphorus. 2 It is likely that inadequate dietary vitamin D prevented these animals from absorbing adequate phosphorus from their diet, leading to hypophosphatemia and osteomalacia. The animals for which blood work was available had low serum phosphorus, further supporting the proposed pathogenesis. Serum levels of vitamin D were not available, which limits the ability to further confirm vitamin D deficiency as the cause for these lesions.
The 2 animals that did not have detailed clinical history were siblings. Genetic causes for osteomalacia, such as predisposition to vitamin D deficiency or hypophosphatemic rickets (which is caused by genetic mutations in phosphorus metabolism), could not be completely excluded. However, if these animals had a lifelong genetic defect in vitamin D or phosphorus metabolism, physeal lesions of rickets (which affects growing animals with active endochondral ossification) would have been expected. Additionally, the lack of physeal lesions suggests that dietary deficiencies were not present early in life, during active endochondral ossification. All animals in these series were transferred to a different institution after at least 6 months of age. Dietary histories from the native institution were not available in any case. It is suspected that dietary deficiencies occurred only later in life, after completion of endochondral ossification.
Osteomalacia results in deposition of unmineralized osteoid at foci where mechanical stimuli are the greatest (eg, tendon insertions). In these tenrecs, osteoid deposition was not only observed in regions of mechanical tension but also throughout all regions of the bone (including in the marrow cavities), which is consistent with hyperostosis. The cause for hyperostosis in these tenrecs may have been an exuberant compensatory response to bone softening, or vitamin and/or mineral imbalances. 2
On initial examination, retention of physeal cartilage was suspected to be a pathologic finding. Review of control long bones from 2.5-year-old and 11-year-old tenrecs revealed similar retention of cartilage in the physeal plate, suggesting that this is a normal feature of tenrec skeletal development.
A limitation of this study was the inability to examine parathyroid gland in any of the lesser hedgehog tenrecs. The anatomic location and number of parathyroid glands in lesser hedgehog tenrecs is unknown, but they may be located within and/or adjacent to the thyroid gland. Thyroid gland was collected in the 2 cases for which anatomic pathologists performed the necropsy, and no masses were identified in the region of the thyroid glands. Thyroid gland was not collected in the remaining 2 cases, likely due to difficulty in grossly identifying thyroid tissue in these small animals. It is unlikely that metabolic bone disease in these cases was caused by hyperparathyroidism, which typically results in compensatory deposition of fibrous tissue coupled with osteoclast-mediated decreased osseous matrix (ie, fibrous osteodystrophy), which was not observed in these cases. 2 If these animals had vitamin D deficiency and no histologic evidence of hyperparathyroidism, it is unclear how they maintained adequate serum calcium. Vitamin D deficiency typically impairs calcium resorption and absorption from the kidney, intestines, and bone, resulting in hypocalcemia. This is typically compensated for by parathyroid hormone-induced bony resorption (ie, hyperparathyroidism), leading to normalization of serum calcium and histologic lesions of fibrous osteodystrophy, the latter of which was not observed. 2 However, some studies have shown that the major mode of calcium absorption may be from vitamin D–independent passive diffusion in the intestines. 1 If the tenrecs in this study had adequate dietary calcium, it is possible they were able to maintain normocalcemia in the face of inadequate dietary vitamin D. Further research on calcium and vitamin D metabolism in tenrecs is needed.
Osteomalacia has not been previously reported in this species. In a review of the husbandry and mortality in lesser hedgehog tenrecs, a wide range of diets were reported, including cat food, dog food, insects, fruit, and vegetables. In that review, none of the animals had lesions of osteomalacia despite the wide variety of diets and options provided. 4 Whether or not the animals in the current series were genetically predisposed to osteomalacia remains unknown. According to the referenced study, the median age of death in captive lesser tenrecs is 8 years old. 4 Compared to this value, all animals with metabolic bone disease in this study were relatively young (2–5 years old).
Footnotes
Author’s Note
The views expressed in this article are those of the authors and do not reflect official policy of the Department of Army/Navy/Air Force, Department of Defense, or the US government.
Acknowledgements
The authors thank John Trupkiewicz for initial review of one of the cases. We also thank clinicians and veterinary care staff for providing antemortem data, including Jenessa Gjeltema and Ray Wack of Sacramento Zoo, Victoria Hample of Palm Beach Zoo, Meredith Clancy and Katie Kerr of San Diego Zoo Global, and Kenton Kerns of Smithsonian National Zoo. The authors also thank Cathy Minogue of Northwest ZooPath for collating case materials, Gaius Nti of Joint Pathology Center (JPC) for scanning slides, Mark Murphey of JPC for reviewing radiographs, Alejandro Luina-Contreras of JPC for reviewing bone slides, and Caitlin Burrell of Zoo Pathology Program for initial consultation on study design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.