
Abstract
Hypophysectomy specimens from 16 dogs with pituitary adenoma were evaluated with periodic acid-Schiff (PAS), reticulin, and immunohistochemistry for adrenocorticotrophic hormone (ACTH), melanocyte stimulating hormone (MSH), growth hormone (GH), and Ki-67. The reticulin network was obliterated in all adenomas. One adenoma expressed ACTH and GH. Eight corticotroph adenomas were basophilic to chromophobic, and PAS- and ACTH-positive. Seven melanotroph adenomas were distinguished from corticotroph adenomas by expression of MSH. Pituitary-dependent hypercortisolism was diagnosed in 5 of 8 dogs with corticotroph and 4 of 7 with melanotroph adenoma. Pituitary height/brain area (P/B) ratio was elevated in all dogs. Previous canine hypophysectomy studies suggested that melanotroph adenomas were larger and carried a worse prognosis than corticotroph adenomas; however, in this study, corticotroph adenomas in comparison to melanotroph adenomas were larger (median P/B ratio: 1.06 versus 0.76), more proliferative (median Ki-67 index: 9.47% versus 1.99%), and associated with shorter survival (median: 300 versus 793 days). Recommended immunohistochemistry for PAS-positive pituitary adenomas includes ACTH and MSH to distinguish corticotrophs from melanotrophs and Ki-67 for proliferation index.
Keywords
Although proposed as a treatment for canine pituitary-dependent hypercortisolism (PDH) as early as 1968, 17 until the 1990s, canine hypophysectomy was mainly an experimental method to investigate pituitary function. 9 With improved diagnostic imaging, microsurgical techniques, and postoperative care, transsphenoidal hypophysectomy is increasingly used to treat canine PDH and other sellar diseases. 11,14 The purpose of this study was to characterize the histochemical and immunohistochemical features of canine pituitary adenoma in transsphenoidal hypophysectomy specimens. All 16 cases submitted to the Indiana Animal Disease Diagnostic Laboratory from 2011 to 2016 were included. These were a subset of 44 transsphenoidal hypophysectomies by author T.J.O.; 10 of the 16 cases were also part of another study. 16
The criteria for inclusion were the presence of a sellar mass on magnetic resonance (MR) imaging, endocrine testing, knowledge of PDH diagnosis (yes/no), transsphenoidal hypophysectomy, histologic diagnosis of pituitary adenoma, and long-term follow-up. Each case was evaluated with hematoxylin and eosin (HE), periodic acid-Schiff (PAS), Gordon and Sweet’s reticulin histochemistry, and immunohistochemistry (IHC) 16 for adrenocorticotrophic hormone (ACTH), growth hormone (GH), melanocyte stimulating hormone (MSH), and Ki-67 (see online version for Supplemental Table S1). Adenomas that expressed only ACTH were classified as corticotroph adenomas; those that expressed ACTH and MSH, as melanotroph adenomas; and those that expressed ACTH and GH, as plurihormonal. 7 The proliferation index was calculated as the percentage of neoplastic cells with Ki-67–immunoreactive nuclei. At least 500 cells were counted (Count Tool in Adobe Photoshop CC 2015) in photographs taken at 400× magnification. See the previous study 16 for details of the statistical analysis.
The biopsy specimens were fragments of neoplastic and nonneoplastic adenohypophyseal tissue, which, along with involvement of both pars intermedia and pars distalis, obscured the precise histologic location of the adenomas. Eight tumors were classified as corticotroph adenoma, 7 as melanotroph adenoma, and 1 as a plurihormonal adenoma that expressed ACTH and GH. Corticotroph adenomas were composed of cells with sparsely (Fig. 1) to densely (Fig. 2) granulated cytoplasm. Cytoplasmic granules were basophilic to chromophobic, PAS-positive, and immunoreactive for ACTH. Melanotroph adenomas were also composed of sparsely to densely granulated, basophilic to chromophobic cells with similar PAS reaction and ACTH immunoreactivity but co-expressed MSH (Fig. 3). The mitotic index was >1/10 high-power fields (hpf) in only 2 adenomas, both of which were corticotroph adenomas.
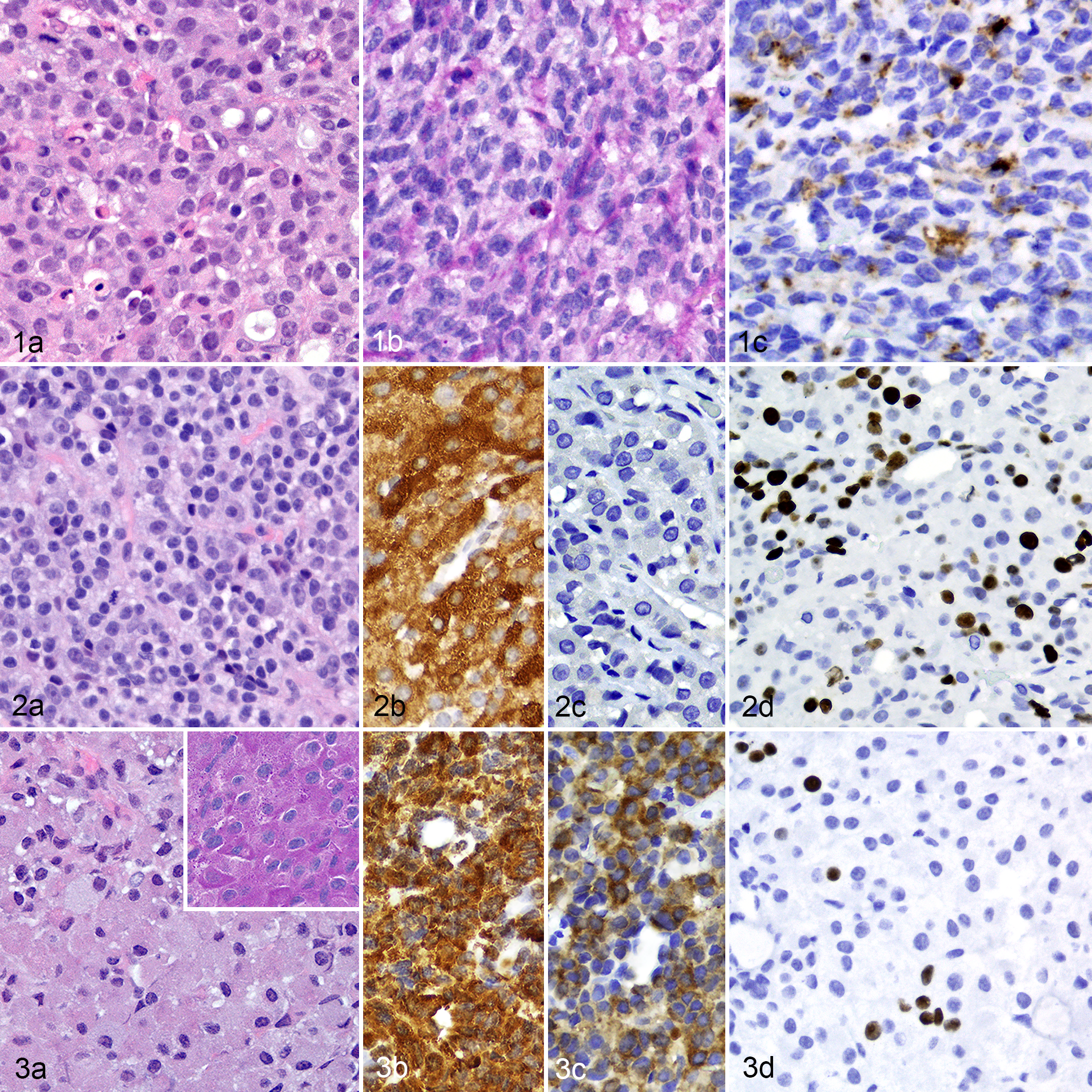
Corticotroph adenoma, pituitary gland, dog 4. (a) The neoplastic cells are sparsely granulated and chromophobic. HE. (b) The sparse cytoplasmic granules are PAS-positive. (c) The cytoplasmic granules are positive for ACTH by IHC.
Signalment, clinical, and histopathologic features are listed in Table 1. The dogs’ ages ranged from 4 to 13 years (median, 9.8 years). All 5 brachycephalic dogs had corticotroph adenomas, whereas none of the melanotroph adenomas were in a brachycephalic breed (Fisher exact test, P = .026). All 4 female dogs were spayed; all but 2 of 12 male dogs were castrated.
Clinical and Histologic Features of 16 Canine Pituitary Adenomas Treated by Transsphenoidal Hypophysectomy
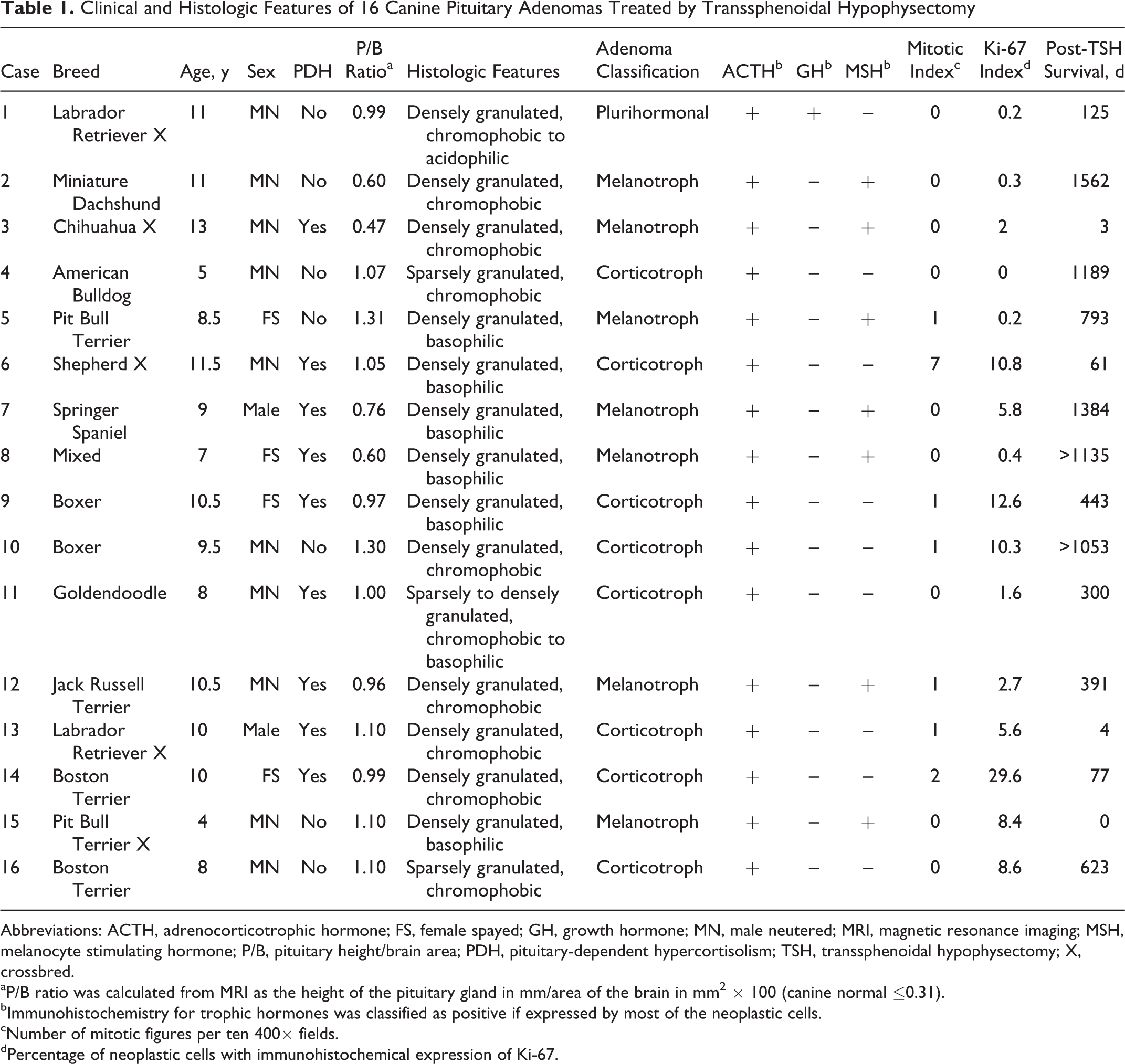
Abbreviations: ACTH, adrenocorticotrophic hormone; FS, female spayed; GH, growth hormone; MN, male neutered; MRI, magnetic resonance imaging; MSH, melanocyte stimulating hormone; P/B, pituitary height/brain area; PDH, pituitary-dependent hypercortisolism; TSH, transsphenoidal hypophysectomy; X, crossbred.
aP/B ratio was calculated from MRI as the height of the pituitary gland in mm/area of the brain in mm2 × 100 (canine normal ≤0.31).
bImmunohistochemistry for trophic hormones was classified as positive if expressed by most of the neoplastic cells.
cNumber of mitotic figures per ten 400× fields.
dPercentage of neoplastic cells with immunohistochemical expression of Ki-67.
All dogs had undergone a physical examination with hematology, serum biochemistry, and urinalysis. The criteria for diagnosis of hypercortisolism were failure to suppress cortisol concentration to <1.4 mg/dL at 8 hours on the low-dose dexamethasone suppression (LDDS), urinary cortisol to creatinine ratio >13, or post-ACTH serum cortisol >22 mg/dL. The criteria for diagnosis of PDH were hypercortisolism plus endogenous ACTH concentration >40 pg/ml and/or >50% suppression of serum cortisol concentration during the LDDS or high-dose dexamethasone suppression test. Nine dogs (5 of the 8 with corticotroph adenoma; 4 of the 7 with melanotroph adenoma) were diagnosed with PDH. The dog with a plurihormonal adenoma had no evidence of hyperadrenocorticism or hypersomatotropism. Pituitary adenomas in dogs without PDH or other pituitary-dependent condition were considered nonfunctional or clinically silent. 12
The pituitary height/brain area (P/B) ratio was calculated from MR images as pituitary height in mm/brain area in mm2 × 100 (canine normal, ≤0.31). 8 All pituitary glands were enlarged, with P/B ratio ranging from 0.47 to 1.31 (median, 1.00). Although the median P/B ratio (1.06) was larger in dogs with corticotroph adenoma than in dogs with melanotroph adenoma (0.76), the overall difference (Fig. 4) was not significant (Mann-Whitney U-test, P = .121).
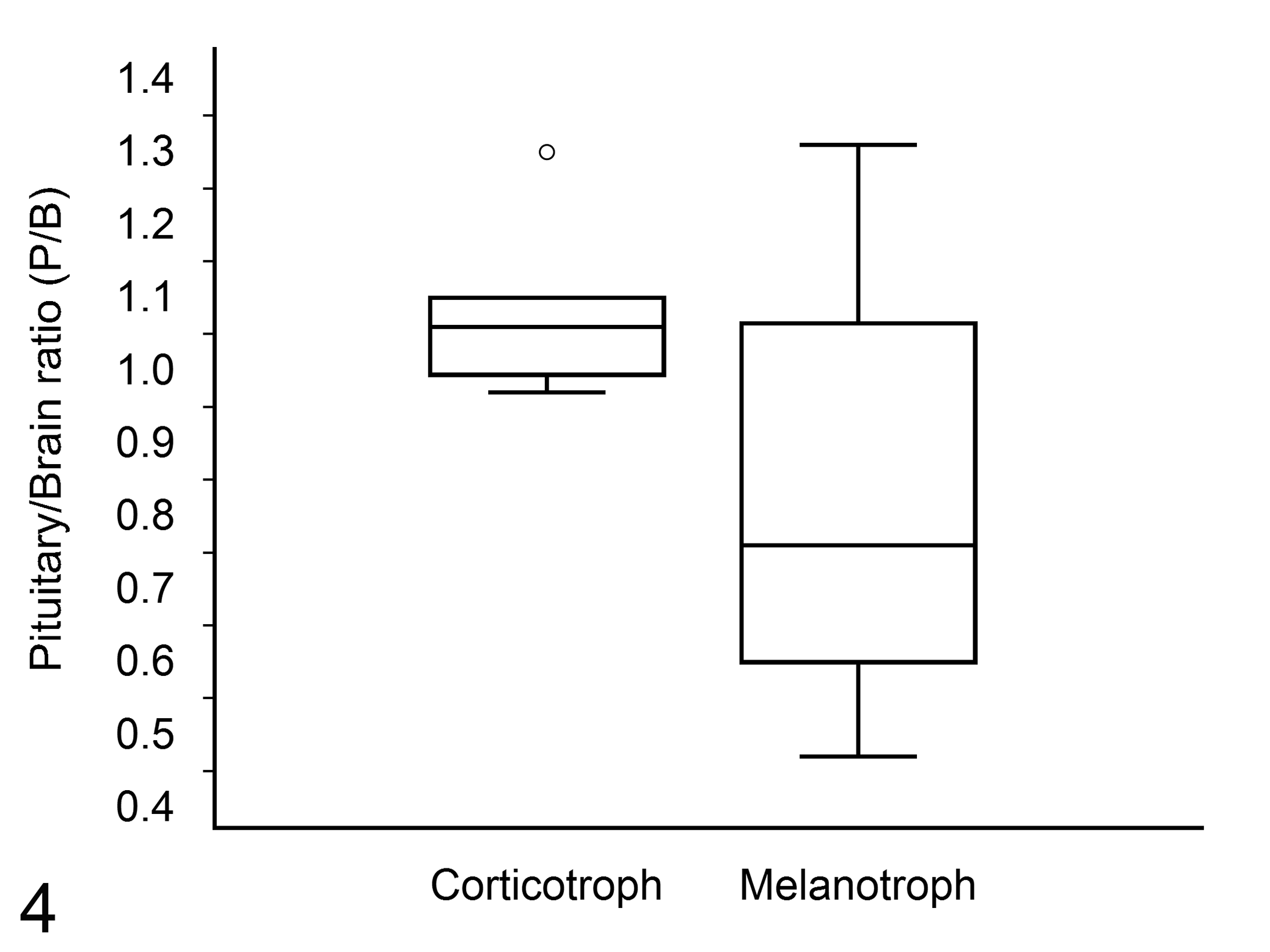
Pituitary height/brain area (P/B) ratio in dogs with corticotroph adenoma (n = 8) versus those with melanotroph adenoma (n = 7). Box and whisker plot depicting the data distribution. The difference was not significant (P = .121, Mann-Whitney U-test). The upper and lower edges of the box represent the interquartile range (IQR), the whiskers are 1.5
The Ki-67 proliferation index ranged from 0% to 29.6% (median, 3%). Corticotroph adenomas had a higher median Ki-67 proliferation index (9.47%) than melanotroph adenomas (1.99%), but the overall difference (Fig. 5) was not significant (Mann-Whitney U-test, P = .094). The correlation between Ki-67 index and P/B ratio was weak (Spearman’s ρ = 0.1, P = .711).
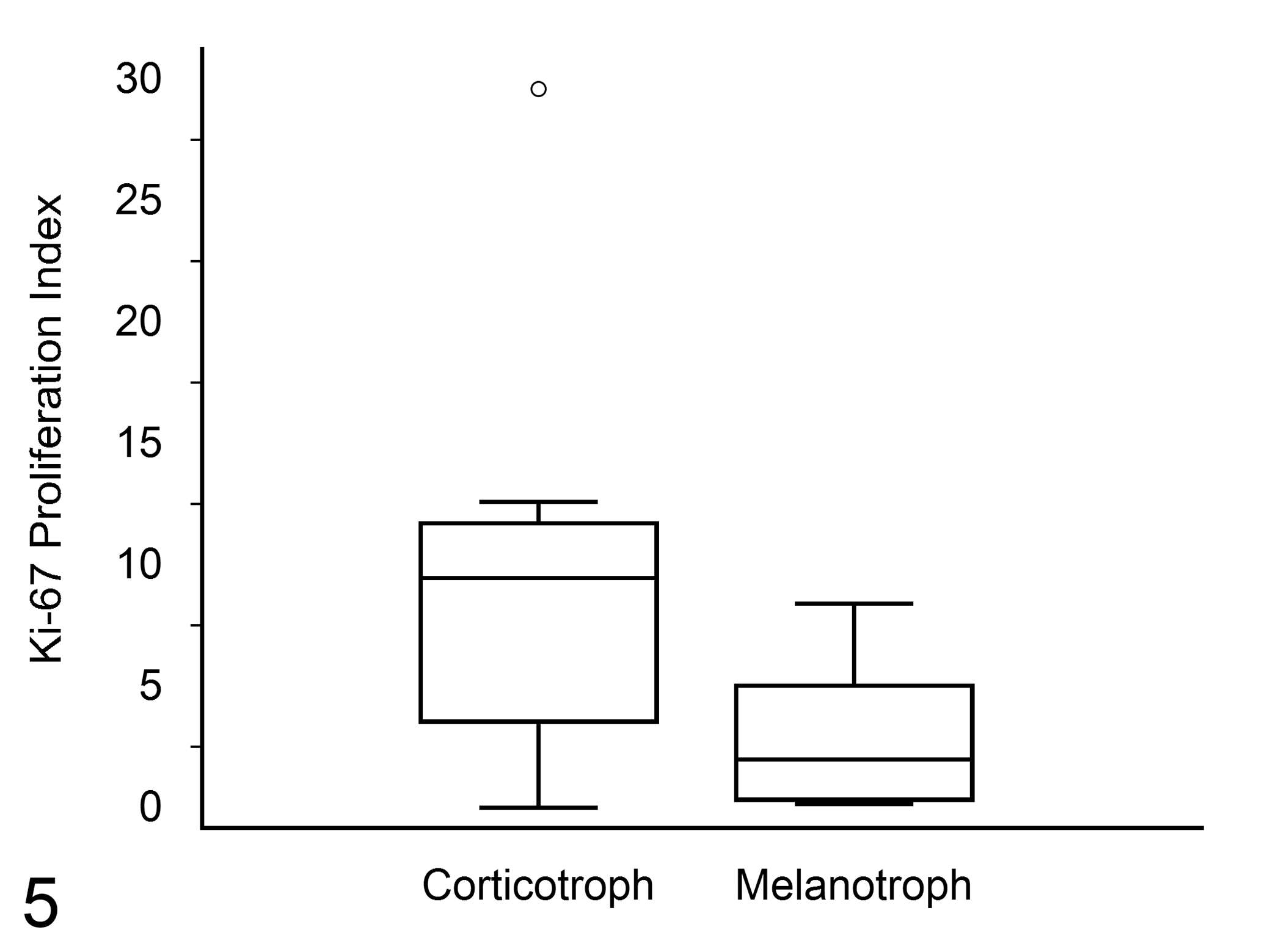
Ki-67 proliferation index in dogs with corticotroph adenoma (n = 8) versus those with melanotroph adenoma (n = 7). Box and whisker plot depicting the data distribution. The difference was not significant (P = .094, Mann-Whitney U-test). See Figure 4 for key.
Postsurgical survival, determined by review of the medical record or by contact with referring veterinarian (7 dogs) or owner (9 dogs), ranged from 0 to 1562 days (Kaplan-Meier estimated median, 391 days), and for the 13 dogs that survived the first 4 postoperative weeks, survival ranged from 61 to 1562 days (Kaplan-Meier estimated median, 623 days). Two dogs remained alive at the end of the study (both survived >1000 days; Table 1). The median survival time (and 95% confidence interval [CI]) for dogs with PDH (functional adenomas) was 300 days (61–443 days) versus 793 days (125–1562 days) for dogs without PDH (nonfunctional adenomas). The difference in overall survival between groups (PDH versus non-PDH) was not significant (log rank test, P = .256). The median survival time (and 95% CI) for dogs with corticotroph adenomas was 300 days (61–1189 days) versus 793 days (3–1562 days) for dogs with melanotroph adenomas. The difference in overall survival between groups (corticotroph versus melanotroph adenoma; Fig. 6) was not significant (log rank test, P = .323). The median survival (and 95% CI) for pituitary adenomas with a Ki-67 proliferation index >3% was 77 days (4–1384 days) versus 391 days (125–1189 days) for adenomas with Ki-67 index ≤3. The difference in overall survival between groups (Ki-67 >3% versus Ki-67 ≤3%; Fig. 7) was not significant (log rank test, P = .446). The median survival (95% CI) for pituitary adenomas with a P/B ratio ≥1.0 was 300 days (4–1189 days) versus 391 days (77–1384 days) for adenomas with a P/B ratio <1.0. The difference in overall survival between groups (P/B ratio ≥1.0 versus P/B ratio <1.0; Fig. 8) was not significant (log rank test, P = .432).
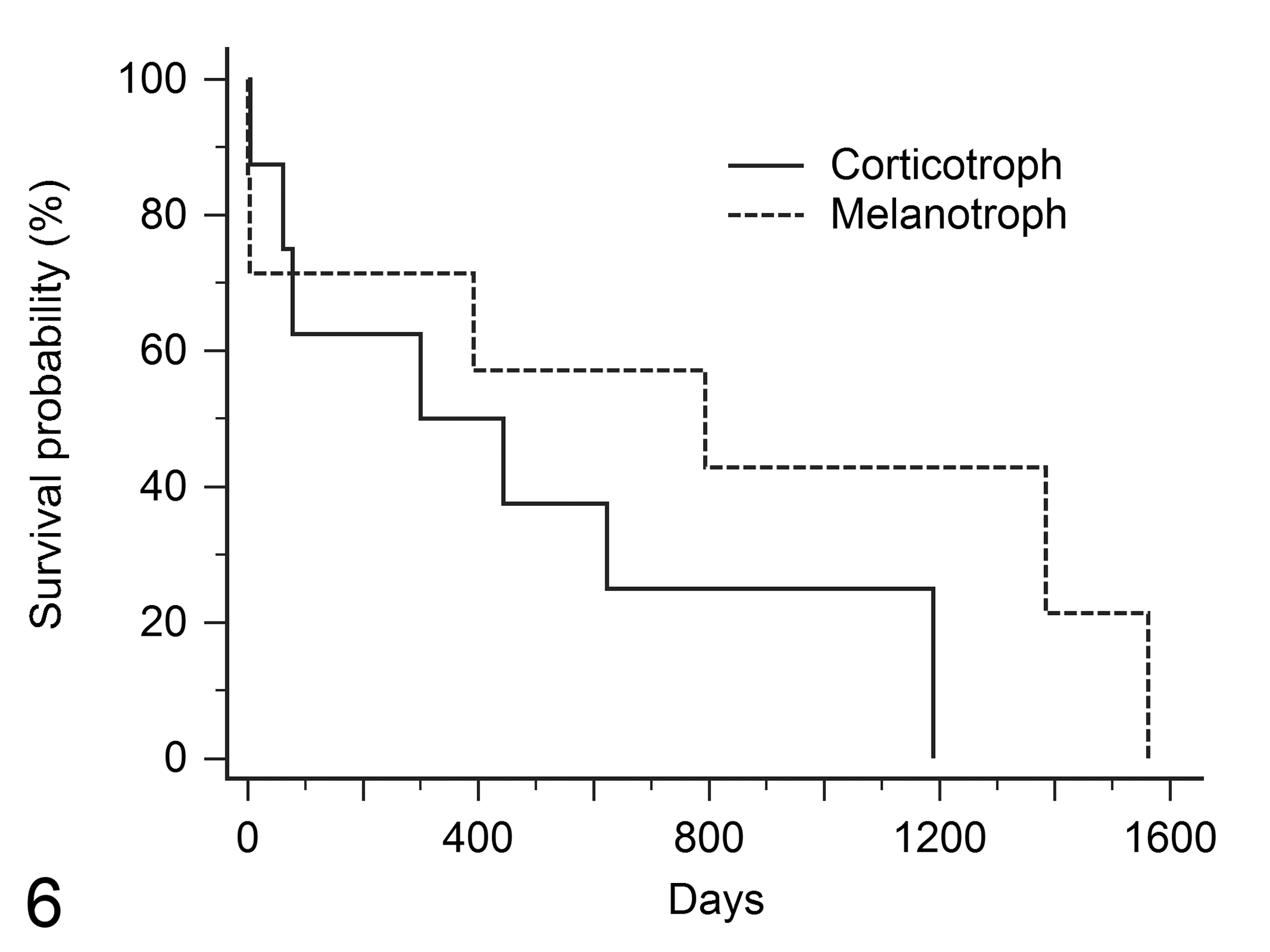
Posthypophysectomy survival (Kaplan-Meier survival curves) in dogs with corticotroph adenoma (n = 8) compared with melanotroph adenoma (n = 7). The median survival time (and 95% CI) was 300 days (61–1189 days) in dogs with corticotroph adenoma compared with 793 days (3–1562 days) in dogs with melanotroph adenoma. The overall survival patterns were not significantly different (P = .323, log-rank test).
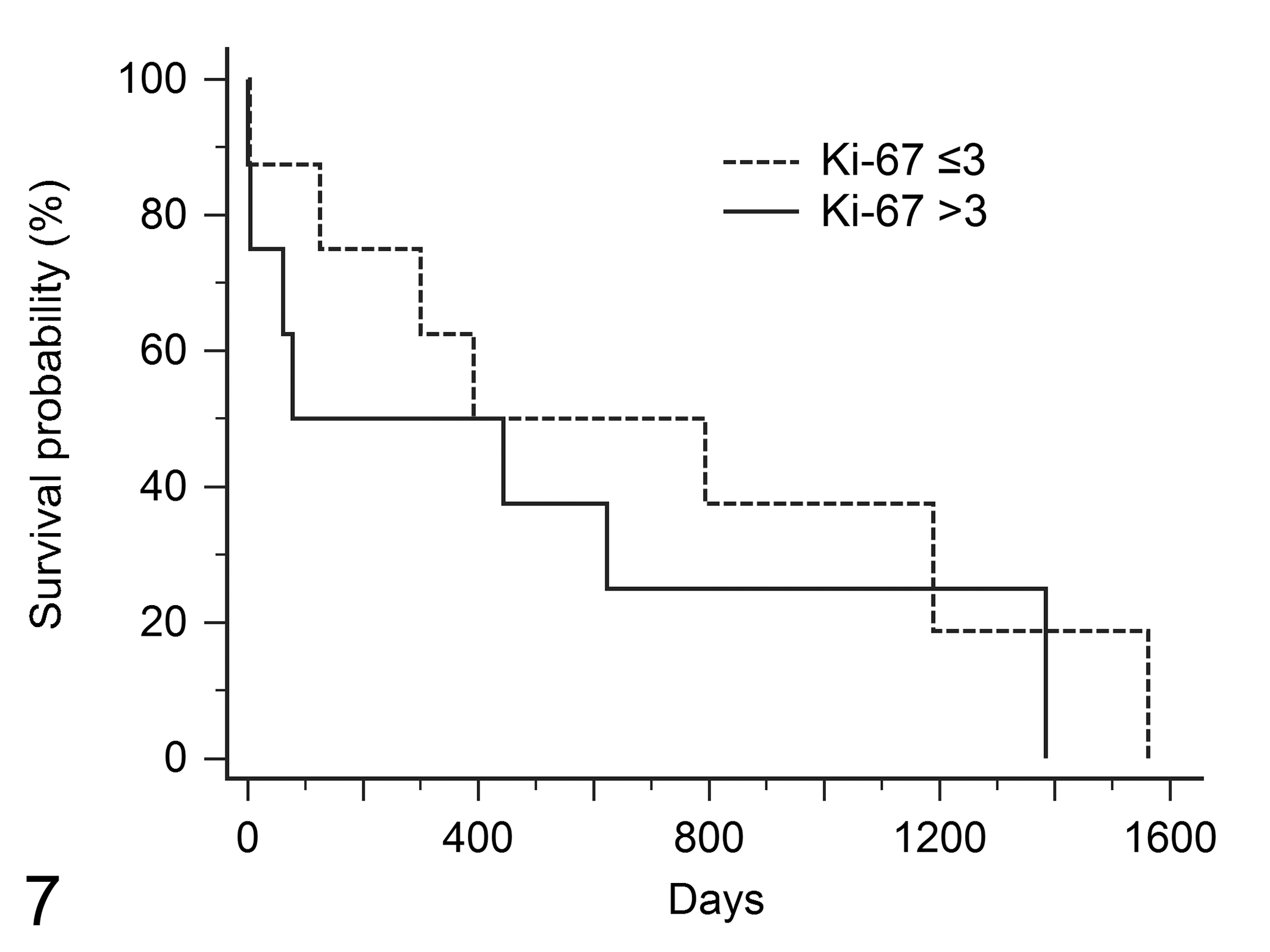
Posthypophysectomy survival (Kaplan-Meier survival curves) in dogs with pituitary adenoma with differing Ki-67 proliferation indices. The median survival time (and 95% CI) was 77 days (4–1384 days) in dogs with Ki-67 index >3 (n = 8) compared with 391 days (125–1189 days) in dogs with Ki-67 ≤3 (n = 8). The overall survival patterns were not significantly different (P = .446, log-rank test).
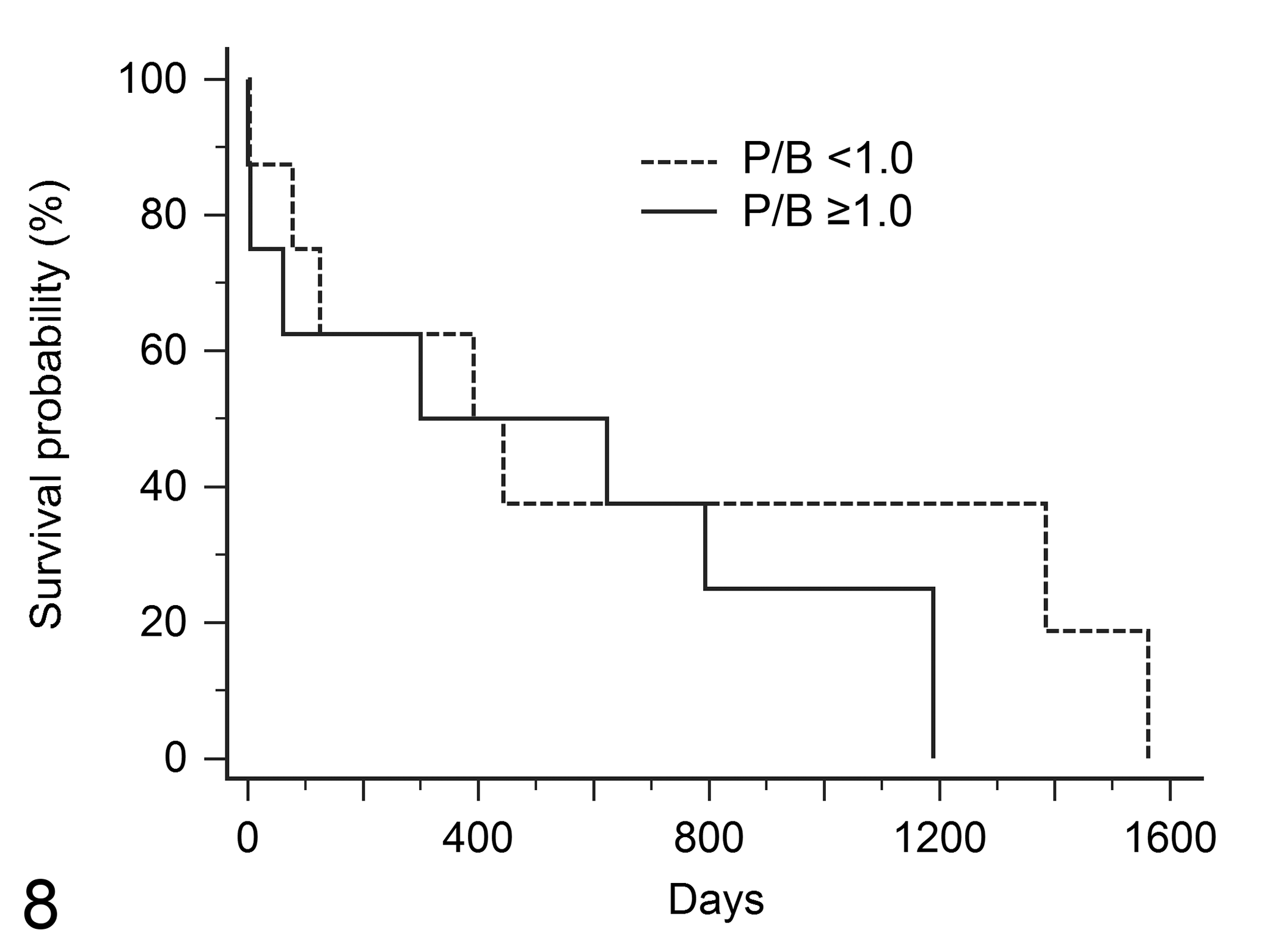
Posthypophysectomy survival (Kaplan-Meier survival curves) in dogs with pituitary adenoma with differing pituitary height/brain area (P/B) ratios. The median survival time (and 95% CI) was 300 days (4–1189 days) in dogs with P/B ratio
Pituitary size (P/B ratio) has been proposed as a prognostic indicator because dogs with an enlarged pituitary gland were more likely to have recurrence of PDH and had shorter survival and shorter disease-free interval. 4,5,20 However, in the current study, all 16 pituitary glands were enlarged, and an association between P/B ratio and survival was not apparent. In a hypophysectomy study of 15 dogs in Japan, 6 adenomas in enlarged pituitary glands had a higher Ki-67 index than those in nonenlarged glands. However, of 17 canine ACTH/MSH-positive pituitary adenomas in another study, neither Ki-67 nor proliferating cell nuclear antigen indices correlated with pituitary size. 21
Corticotroph adenoma and melanotroph adenoma were the most common adenohypophyseal tumors in this study. Most dogs with either type of adenoma developed PDH. The adenomas were composed of basophilic to chromophobic cells with PAS-positive granules, consistent with production of proopiomelanocortin (POMC), the precursor to ACTH and MSH. 7,19 Reticulin histochemistry facilitated the distinction of adenoma from hyperplasia in fragmented specimens. Plurihormonal adenomas are seldom reported in dogs, 7 and only 1 was diagnosed in this series. However, other types of plurihormonal adenoma would not have been detected without broader testing for trophic hormone expression.
In 46 pituitary adenomas evaluated in hypophysectomy specimens, 14 the neoplastic cells expressed ACTH and MSH but were immunohistochemically negative for GH. In another canine hypophysectomy series from the Netherlands, 15 pituitary adenomas 21 also expressed both ACTH and MSH but not GH. These IHC results prompt speculation that melanotroph adenomas may be more common than corticotroph adenomas in European dogs but could also reflect differences in immunohistochemical techniques.
Results of the current study suggest that corticotroph adenomas are more common in brachycephalic than in other breeds; however, the study sample was small. In a postmortem study, 2 Boxers and Boston Terriers were overrepresented for pars distalis adenomas (presumably corticotroph adenomas) but not for pars intermedia adenomas (presumably derived from melanotrophs). In contrast, Dachshunds, Miniature Poodles, Maltese, and Yorkshire Terriers were the most common purebred dogs and together composed 25% of 181 dogs with pituitary adenoma treated by hypophysectomy in the Netherlands. 4 This apparent difference in breed distribution could reflect differences in canine populations. The male:female ratio in the current case series was 3:1, but no reference population was available to determine whether this reflected a sex predilection for pituitary adenoma, which was not apparent in our retrospective study 16 and not reported in other studies.
The most common surgical pathology finding in human Cushing’s disease is a centrally located, basophilic, noninvasive corticotroph microadenoma. 1,18,19 In contrast, macroadenoma is the most common diagnosis in canine hypophysectomy specimens. The increasing size of canine pituitary adenomas at hypophysectomy over the past 20 years has been attributed to trilostane therapy or to the possibility that dogs with larger pituitary glands were more likely to be referred for surgery. 11,20 The treatment for corticotroph adenoma in humans is a selective adenectomy 3 ; however, incomplete removal of the canine pituitary gland leaves functional corticotrophs that can lead to recurrence, so in dogs, the complete pituitary gland is typically removed. 5,11,13,14
Although histologic grade does not always predict the behavior of human corticotroph adenomas, 10,19 criteria for classification of adenomas as aggressive-invasive include >2 mitotic figures per 10 hpf, a Ki-67 proliferation index >1% to 3%, and >10 nuclei/hpf with strong p53 expression. 15,18 Sparsely granulated corticotroph adenomas are considered more aggressive than densely granulated tumors. 15 In the current canine study, correlation between granularity of neoplastic cells and posthypophysectomy survival was not apparent, but corticotroph adenomas had a shorter median survival than that for melanotroph adenomas. The median survival was also shorter in dogs with a Ki-67 index greater than 3% (found in most corticotroph adenomas but in the minority of melanotroph adenomas). The mitotic index was of less value than the Ki-67 index because it was >2 in only 1 case, a corticotroph adenoma.
Although the differences were not significant, corticotroph adenomas in the current study tended to be larger, more proliferative, and associated with a shorter postsurgical survival than melanotroph adenomas. In a postmortem study, 2 canine pituitary glands with pars distalis (presumably corticotroph) adenomas were larger than those with pars intermedia (presumably melanotroph) adenomas. However, in a hypophysectomy study, 4 pars intermedia adenomas were reportedly larger and thought to have a worse prognosis than pars distalis adenomas. In addition, dogs with high presurgical plasma α-MSH concentration had an increased risk of posthypophysectomy recurrence of PDH. 4
Based on this study, the following protocol is recommended for histologic evaluation of canine transsphenoidal hypophysectomy specimens. The initial diagnosis is made from HE-stained sections, using reticulin histochemistry to distinguish pituitary adenoma from hyperplasia, and PAS to highlight the granules of POMC-producing corticotrophs or melanotrophs. If the proliferative cells are basophilic to chromophobic and PAS-positive, IHC for trophic hormones could be limited to ACTH and MSH to distinguish corticotrophs from melanotrophs, using IHC for other trophic hormones to detect the rare plurihormonal adenoma. A Ki-67 proliferation index greater than 3% may predict shorter posthypophysectomy survival.
Supplemental Material
Supplemental Material, DS1_VET_10.1177_0300985818784160 - Immunohistochemical Evaluation of Canine Pituitary Adenomas Obtained by Transsphenoidal Hypophysectomy
Supplemental Material, DS1_VET_10.1177_0300985818784160 for Immunohistochemical Evaluation of Canine Pituitary Adenomas Obtained by Transsphenoidal Hypophysectomy by Margaret A. Miller, Tina Jo Owen, David S. Bruyette, J. Catharine Scott-Moncrieff, José A. Ramos-Vara, Hsin-Yi Weng, Annie V. Chen, Linda G. Martin, and Deidre M. DuSold in Veterinary Pathology
Footnotes
Acknowledgements
We thank the histology technicians, pathologists, and pathology residents at the Indiana Animal Disease Diagnostic Laboratory and the Washington Animal Disease Diagnostic Laboratory; Connie Fraser, Washington State University; and Jan Shivers, University of Minnesota.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.