
Abstract
A 12-year-old male Yorkshire Terrier was presented because of decreased appetite. Physical examination revealed mammary gland swelling and galactorrhea. Contrast-enhanced computed tomographic scanning of the skull indicated an enlarged pituitary gland, compatible with a pituitary tumor. The serum prolactin concentration was markedly elevated. One week after the start of treatment with the dopamine agonist cabergoline, the serum prolactin concentration normalized and the galactorrhea resolved. Cabergoline was administered for approximately 4 months and then discontinued. Subsequently, serum prolactin concentration increased again, and mammary gland swelling and galactorrhea reappeared. The dog was euthanized 10 months after the first detection of the galactorrhea because of problems not directly related to pituitary disease. Postmortem examination revealed an infiltrative adenoma of the pituitary gland with immunolabeling for prolactin. The clinical and histopathologic findings indicated the diagnosis of a functional prolactinoma in a male dog.
Keywords
In humans, the most common functional pituitary adenomas are prolactinomas, while adenomas secreting growth hormone (GH), adrenocorticotrophic hormone (ACTH), and thyrotropin (TSH) as well as clinically nonfunctional adenomas are much less represented. 6 The incidence of functional pituitary adenomas is markedly different in the dog, in which ACTH-secreting adenomas causing hypercortisolism (ie, Cushing’s syndrome) are the most commonly diagnosed pituitary neoplasm. GH-producing pituitary tumors are considered rare, 4 and prolactin-, gonadotrophin- and TSH-producing pituitary adenomas have not been characterized in dogs to our knowledge.
Hyperprolactinemia due to prolactinoma may result in abnormal sexual and/or reproductive function or galactorrhea in humans. 12 Although prolactinomas are unknown in dogs, hyperprolactinemia and galactorrhea are conditions frequently described in bitches with pseudopregnancy. Pseudopregnancy can be associated with a high circulating prolactin concentration, mammary development, galactorrhea, and behavioral changes, and these findings are barely distinguishable from those of late pregnancy or lactation. Other conditions in dogs that have been reported to be associated with hypersecretion of prolactin are hypothyroidism, pituitary-dependent hypercortisolism, and mammary tumors. 3,8,10
A 12-year-old intact male Yorkshire Terrier (body weight 9 kg) was referred for intermittent anorexia. There was no history of polyuria or polydipsia, and the dog was not receiving any medication. On physical examination, mammary gland swelling and significant galactorrhea of the right caudal abdominal mammary gland were present. On subsequent visits in the following 2 months, mammary secretions were also observed from the left and right mammary glands, but the right caudal abdominal mammary gland remained the most swollen gland. The complete blood count was unremarkable, and serum biochemistry and urinalysis revealed no significant abnormalities.
Serum concentrations of total thyroxine (total T4), TSH, and urinary cortisol concentrations were measured using a homologous solid-phase, chemiluminescent enzyme immunoassay (Immulite canine total T4, canine TSH, cortisol; Diagnostic Products Corporation, Los Angeles, California) in accordance with the manufacturer’s instructions. Serum prolactin concentrations were measured using a homologous end point enzyme immunometric assay (Demeditec Diagnostics, Kiel, Germany). The intra-and interassay coefficients of variation of the kit were 5.3% and 8.7%, respectively. The lowest limit of detection (sensitivity) was 0.4 ng/mL.
The cortisol/creatinine ratio in a urine sample collected by spontaneous urination at home was normal (28.4 × 10–6; reference range, <33.0 × 10–6), as were serum total T4 concentration (25 nmol/L; reference range, 13–51 nmol/L) and serum TSH concentration (0.08 ng/mL; reference range, 0.03–0.38 ng/mL). However, serum prolactin concentration was markedly elevated (21.8 ng/mL; reference range, <6 ng/mL). Radiographs of the thorax revealed no significant abnormalities. Abdominal ultrasonography indicated that the prostate gland was hypoechoic, with pinpoint spots of mineralization, and it showed an irregular profile. The volume of the testicles was reduced.
Cytologic examination of fine-needle aspiration biopsies of the prostate revealed prostate carcinoma. Cytologic examination of fine-needle aspiration biopsies of the right abdominal mammary gland revealed well-differentiated mammary epithelium without indications for malignancy or inflammation, consistent with mammary hyperplasia or adenoma.
A single-slice computed tomographic scan (Pronto-XE; Hitachi, Tokyo, Japan) revealed an enlarged pituitary gland (Figure 1) (height 6.1 mm; reference range, <5.4 mm) and a pituitary height/brain area ratio of 0.48 (reference range, <0.31 5 ). Administration of intravenous contrast medium (3 mL/kg bolus Iomeron 300 mg/mL [iomeprolo], containing 300 mg iodine/mL; Bracco Imaging, Milan, Italy) produced a normal enhancement pattern (precontrast density 61.8 ± 10.3 Hounsfield units, postcontrast density 107 ± 19.1 Hounsfield units). The dog was discharged with a presumptive diagnosis of a prolactinoma (ie, a prolactin-secreting pituitary tumor) and prostatic neoplasia.
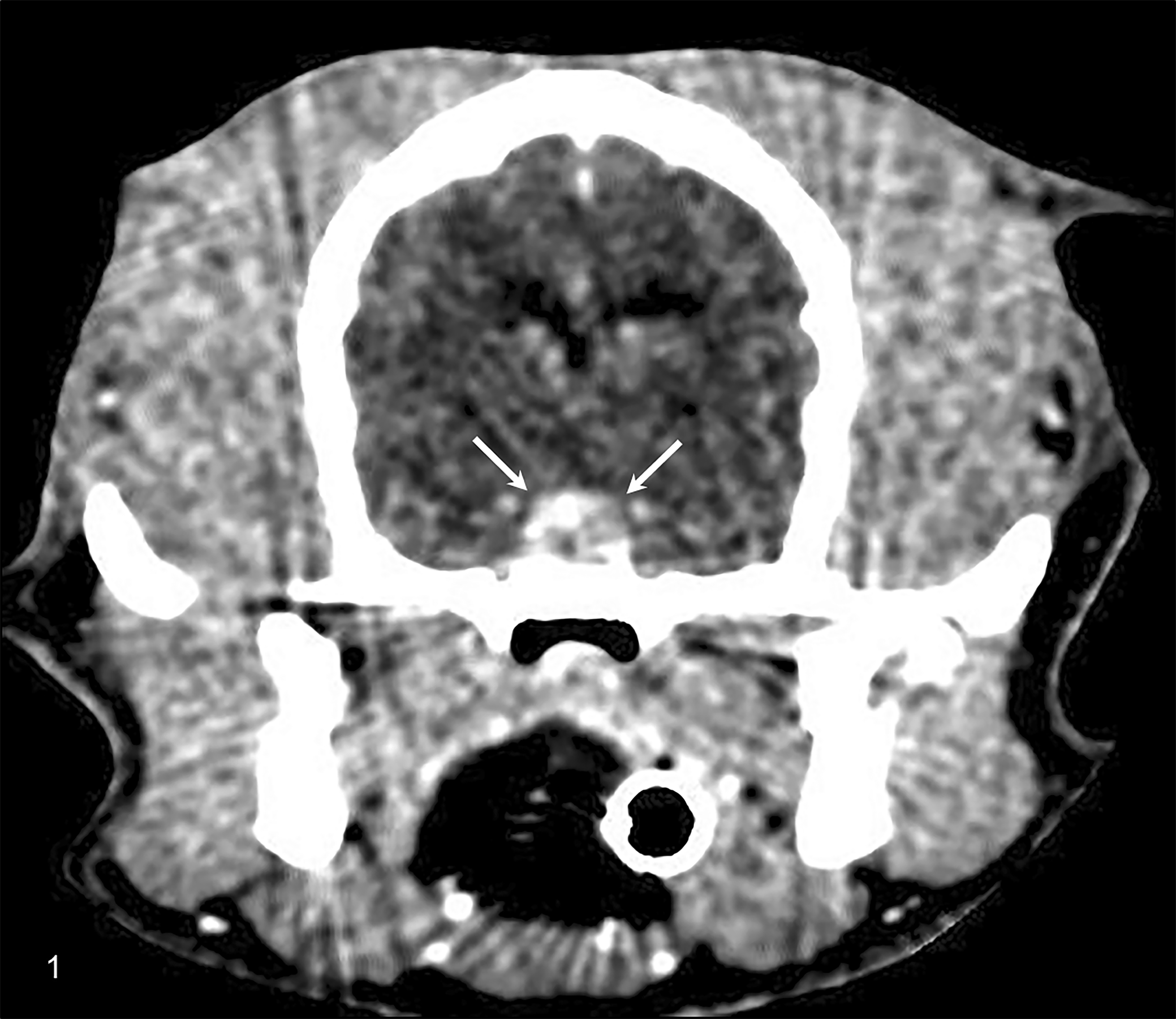
Prolactinoma, pituitary gland, dog. A mass is present in the area of the pituitary gland (arrows). Postcontrast computed tomography.
Galactorrhea reached its peak 1 month after the mammary swelling had been detected, but subsequently the secretion gradually declined in all mammary glands and became more serous. Three weeks later, galactorrhea of the abdominal mammary glands relapsed. At that time serum prolactin concentration was 9.2 ng/mL (reference range, <6 ng/mL), and treatment with the dopamine agonist cabergoline (Galastop; Ceva Animal Health, Amersham, UK) was initiated at 5 μg/kg orally once daily, 4 times per week. After 1 week of treatment, the galactorrhea had completely resolved, and after 4 weeks of treatment, the serum prolactin concentration had decreased to 0.42 ng/mL (Figure 2). Cabergoline treatment was discontinued after about 4 months; subsequently, the serum prolactin concentration increased to 17.9 ng/mL (Figure 2), and galactorrhea reappeared 26 days after the suspension of the treatment.
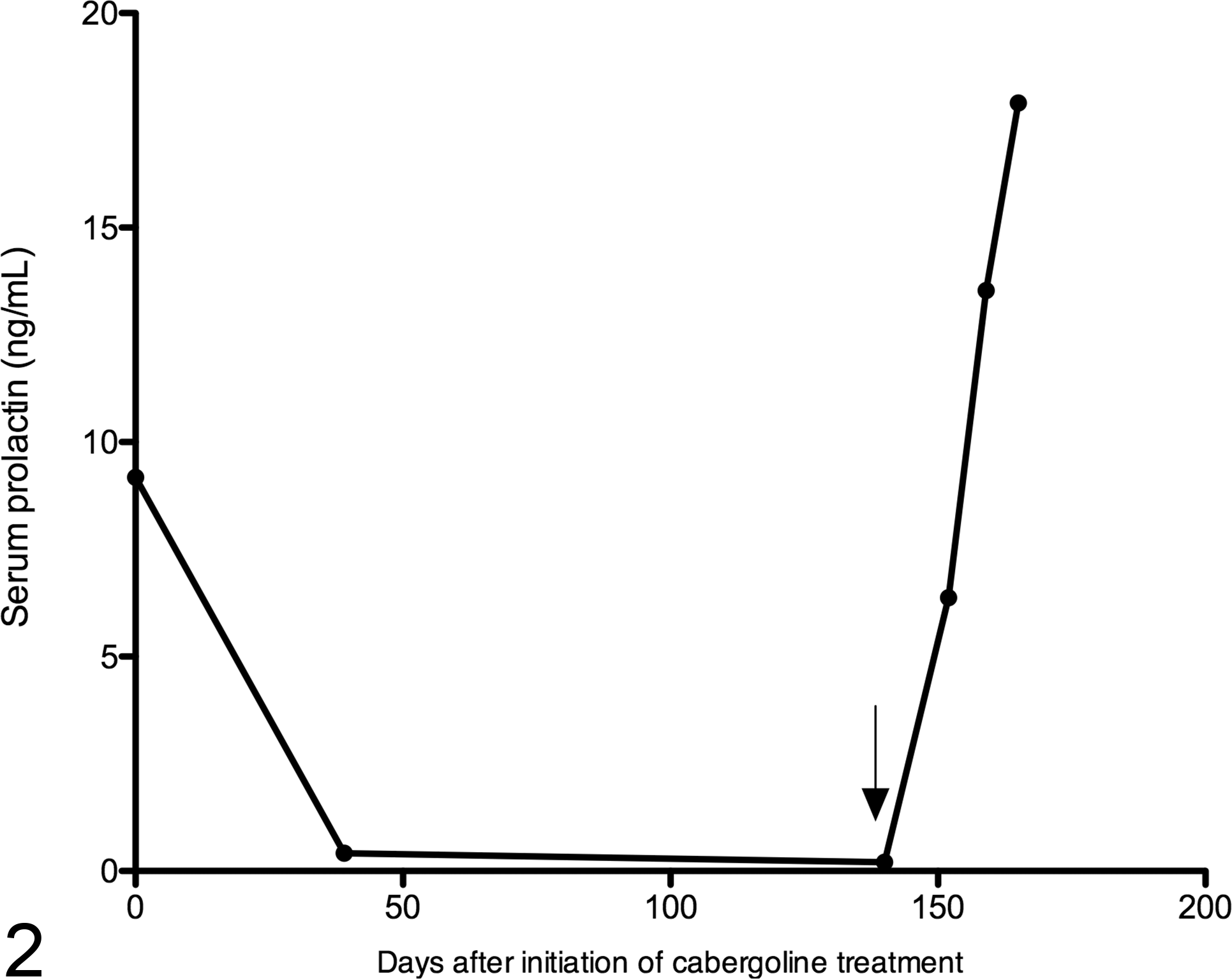
Serum prolactin concentrations in a dog with a prolactinoma before, during, and after treatment with the dopamine agonist cabergoline. The arrow indicates when cabergoline treatment was discontinued.
About 6 months after hyperprolactinemia had been diagnosed, the dog developed uveitis and retinal detachment, uncontrollable diarrhea, and anorexia and was euthanatized at the owner’s request. These clinical signs were not considered to have resulted from the pituitary disease.
A postmortem examination was conducted. Pituitary and prostate tissues were fixed in 10% neutral buffered formalin, and 4-μm-thick histologic sections were routinely prepared and stained with hematoxylin and eosin. Immunohistochemical staining for ACTH, α-melanocyte-stimulating hormone, GH, the proliferation marker Ki67, and prolactin (using a noncommercial polyclonal antibody against prolactin raised in a rabbit; courtesy of Dr B. P. Meij, Utrecht, the Netherlands) were performed on pituitary tissue sections following previously published protocols using 3-amino-9-ethylcarbazole as the chromogen. 9,11
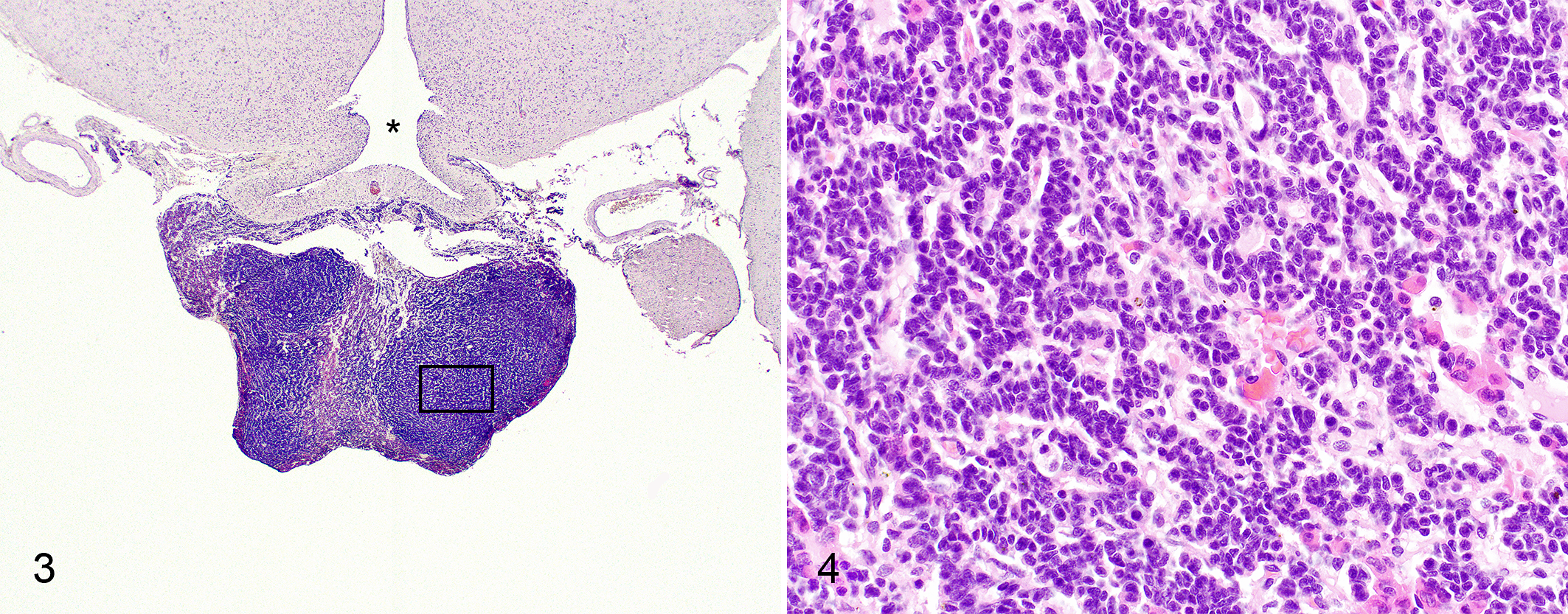
Autopsy revealed the presence of a pituitary neoplasm (Figures 3 and 4) that was histologically characterized by cords and trabecula of neoplastic cells with moderately sized oval nuclei with generally inconspicuous nucleoli, a low mitotic index (<1 positive nucleus per 100 cells in the Ki67 stain), indistinct cell borders, and a small amount of pale or sometimes faintly eosinophilic cytoplasm. In several areas within the neoplasm, palisading of the nuclei was visible with scattered rosettes and pseudorosettes, and the neoplasm infiltrated the non-neoplastic pituitary tissue. In addition, histologic examination revealed an adenocarcinoma of the prostate gland. Immunohistochemistry of the pituitary neoplasm was positive for prolactin (Figure 5), and negative for ACTH, α-melanocyte-stimulating hormone, and GH, consistent with a prolactinoma.
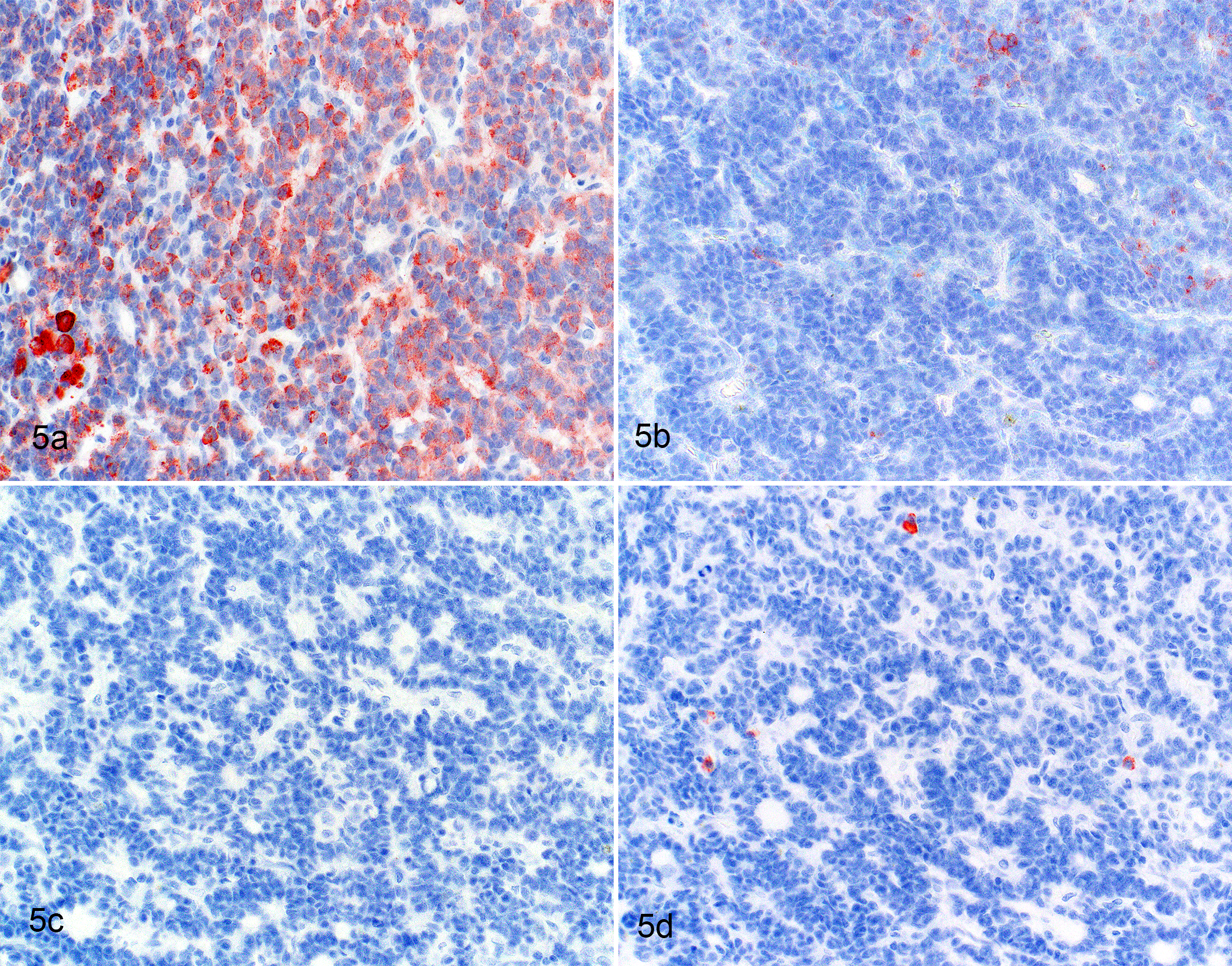
Prolactinoma, pituitary gland, dog. Immunohistochemistry of a representative area of the neoplasm as indicated in Figure 3, stained for prolactin (a), adrenocorticotrophic hormone (b), alpha-melanocyte stimulating hormone (c) and growth hormone (d). Immunohistochemistry using 3-amino-9-ethylcarbazole as chromogen.
The most relevant clinical signs of this dog were mammary swelling and persistent galactorrhea associated with hyperprolactinemia. The causes of hyperprolactinemia in humans include prolactinoma, the intake of various drugs (eg, antipsychotic drugs), compression of the pituitary stalk, hypothyroidism, moderate to severe renal failure, intercostal nerve stimulation by trauma or surgery, and chronic liver diseases. 12 Idiopathic hyperprolactinemia is diagnosed when all these causes are ruled out and pituitary imaging does not reveal a pituitary mass. 12
Hyperprolactinemia and galactorrhea in bitches are usually associated with a decline in circulating progesterone concentration in the second half of the luteal phase. Obviously, this cause of hyperprolactinemia does not occur in male dogs. To our knowledge, the only cases of pathologic hyperprolactinemia reported in dogs were associated with hypothyroidism, 3 pituitary-dependent hypercortisolism, 10 and mammary tumors. 8 The male dog in the present case was not affected by hypothyroidism or hypercortisolism, and there was no evidence of a mammary tumor. Moreover, there was no history of chest wall injury, and the dog had never been treated with antipsychotic drugs. There was also no evidence of significant kidney or liver abnormalities. Considering this, the only 2 options according to the differential diagnosis for hyperprolactinemia in humans were the presence of a prolactin-secreting pituitary tumor and idiopathic hyperprolactinemia. Pituitary imaging indeed revealed a pituitary mass, and its histopathologic evaluation was consistent with an infiltrative adenoma, of which the neoplastic cells showed immunoreactivity against prolactin.
About 1 month after the mammary swelling had been detected, the galactorrhea spontaneously became more mild. A possible explanation could be an inconstant secretion of prolactin by the pituitary tumor.
The dog in the present report had concurrent prolactinoma and prostatic carcinoma. Although experimental data indicate that prolactin stimulates proliferation of prostatic epithelium and regulates prostate growth, 2 prolactinomas in humans have not been shown to induce changes in the prostatic structure. 2 Moreover, hyperprolactinemia seems to reduce the risk for prostatic cancer. 1 To our knowledge, there are no data regarding a possible association between hyperprolactinemia and carcinomas in the prostate in veterinary medicine, and it is possible that the concurrent prostatic tumor was unrelated to the prolactinoma.
Medical therapy with cabergoline was prescribed because the initial treatment for human prolactinoma is dopamine receptor agonists (bromocriptine or cabergoline). 7 Cabergoline was effective in reducing the serum prolactin concentration and clinical signs in this dog. Furthermore, hyperprolactinemia and clinical signs reappeared when cabergoline treatment was discontinued. These observations suggest that cabergoline decreases the secretion of prolactin by the prolactinoma in this dog, comparable to what has been described in humans. 7
To our knowledge, this is the first case of hyperprolactinemia due to a prolactinoma in a dog. The definitive diagnosis was based on histopathology and immunohistochemistry of the pituitary neoplasm. Although prolactinomas (lactotroph adenomas) in other species usually consist of acidophilic cells, the neoplastic cells in the present canine case were not convincingly eosinophilic. Because GH-producing somatotroph adenomas are also composed of acidophilic cells, immunohistochemistry is a more reliable technique than histomorphology to evaluate such neoplasms. Cabergoline was effective in the medical management resulting in a reduction of clinical signs and resolution of hyperprolactinemia, and there was a relapse after cessation of the treatment. On the basis of this case report, a prolactinoma should considered as a cause of hyperprolactinemia or persistent galactorrhea in dogs.
Footnotes
Acknowledgements
We thank Dr Emilio Smadelli from Clinica Veterinaria S. Antonio Salò for the pro bono computed tomographic scan, Dr Corrado Dimauro for his help with diagnostic imaging, Dr Lucia Ramera for her insight. and Dr Paola Prati from IZSLER Pavia for performing the autopsy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.