
Abstract
Endolymphatic sac tumors (ELSTs) are rare neoplasms of the inner and middle ear described in humans. Diagnosis of such neoplasms is difficult and largely dependent on a combination of histologic, immunohistochemical, and clinical findings. Although the neoplastic cells lack cellular features of malignancy, these are clinically aggressive tumors that often invade the surrounding temporal bone. Here, we describe 2 dogs with middle ear masses that share morphologic, immunohistochemical, and clinical similarities with human ELSTs. Advanced imaging of the masses revealed evidence of aggressive behavior such as bony lysis of the temporal bone. Histologically, the neoplastic epithelial cells formed papillary structures, lacked mitotic figures, and had mild anisocytosis and anisokaryosis. The neoplastic cells were immunohistochemically positive for cytokeratin AE1/AE3 but were negative for chromogranin, synaptophysin, and thyroglobulin. Local invasion and bone destruction but no evidence of metastases suggest a clinical behavior similar to human ELSTs.
Low-grade adenocarcinomas of the endolymphatic sac, also known as ELSTs, are rare neoplasms of the inner and middle ear that have been described in humans as slow-growing papillary tumors with a benign histologic appearance and aggressive biological behavior. 3 Although such neoplasms rarely metastasize, they are locally invasive, causing lysis and destruction of surrounding temporal bone. Here, we describe neoplasms in 2 dogs (Fig. 1) that share morphologic, immunohistochemical, and clinical similarities with human ELSTs.
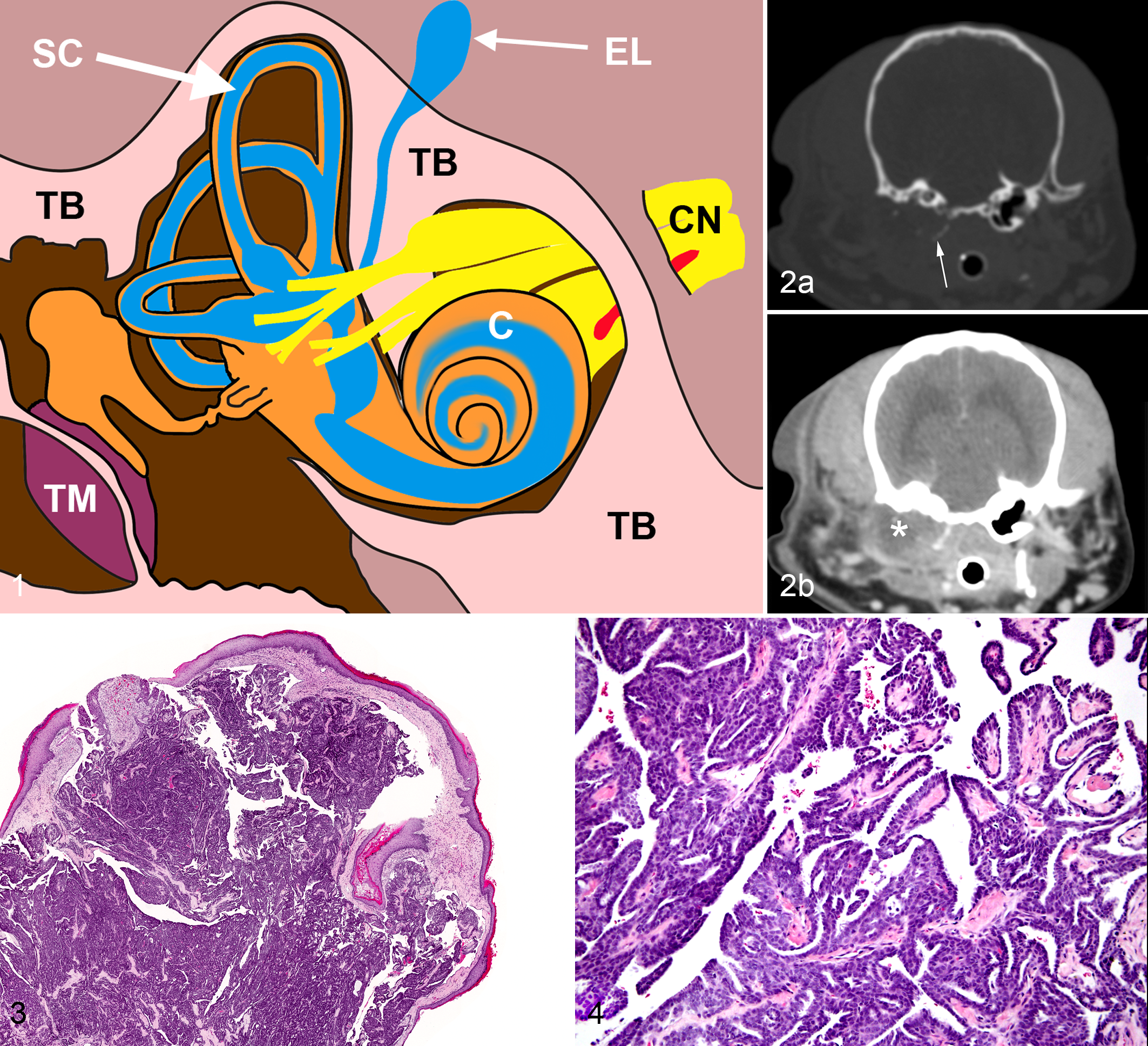
Dog No. 1 was a 9-year-old spayed female toy Poodle who presented with a 1.5-year history of chronic bacterial otitis externa of the right ear with intermittent bleeding and purulent discharge. Video otoscopy of the right ear canal revealed a ruptured tympanic membrane and a smooth to mildly irregular pale pink lobulated mass occupying the distal horizontal canal. Computed tomography examination exposed marked lysis of the right temporal bone (Fig. 2a) and a large (1.4 × 2.7 × 2.7 cm) soft-tissue-attenuating rim-enhancing mass that filled the bulla with extension into the nasopharynx (Fig. 2b). The right internal acoustic meatus was widened with an adjacent thin hypo-attenuating material within the calvarium. Dog No. 2 was a 9-year-old female spayed Airedale Terrier with a 10-month history of left-side otitis, previous rupture of the tympanic membrane, and bleeding from the left ear canal. Magnetic resonance imaging identified a soft-tissue-enhancing mass that extended from the left tympanic bulla into the horizontal canal, as well as an obvious expansion or breach of the ventromedial bulla wall.
Total ear canal ablation and bullae osteotomy was performed in both dogs, and formalin-fixed specimens from the distal external ear canal, tympanic membrane, and nasopharynx from dog No. 1 and tympanic bulla from dog No. 2 were submitted for routine histopathologic examination. Specimens were routinely processed and 5-µm sections stained with hematoxylin and eosin were examined.
Samples from both dogs consisted of epithelial neoplasms with a similar histomorphology. The neoplastic cells were arranged in anastomosing papillary projections supported by a thin fibrovascular stalk (Fig. 3). Papillary structures were lined by 1 to 2 layers of cuboidal to polygonal neoplastic cells, with variably distinct cell borders, moderate amounts of eosinophilic cytoplasm, ovoid nuclei with finely stippled chromatin, and unapparent nucleoli (Fig. 4). In dog No. 2, the neoplastic epithelial cells were also focally ciliated and rarely interspersed with goblet cells. Anisocytosis and anisokaryosis were mild, and mitotic figures were not detected. Inflammation was minimal within all specimens. Immunohistochemistry for chromogranin, synaptophysin, cytokeratin AE1/AE3, and thyroglobulin was performed on formalin-fixed, paraffin-embedded sections. The neoplastic cells expressed strong perimembrane labeling for cytokeratin AE1/AE3 but were negative for chromogranin, synaptophysin, and thyroglobulin. Based on the location, morphologic appearance, immunohistochemical labeling, histologic pattern, and aggressive clinical behavior, a diagnosis of endolymphatic sac tumor was made.
The endolymphatic sac is a normal part of the inner ear located along the posterior wall of the temporal bone (Fig. 1). 1 Neoplasms of the endolymphatic sac in humans have been reported as histologically bland papillary neoplasms that are variably ciliated and lack prominent pleomorphism and mitotic figures. 2,5,6 The exact site of origin of these tumors is controversial, partly due to the extent of tissue destruction found at the time of diagnosis, but ELST has become the accepted nomenclature for tumors with a combination of bland histologic features, local invasion into the temporal bone, and a certain immunohistochemical labeling pattern. 1 Human ELSTs are consistently positive for cytokeratin AE1/AE3 and negative for chromogranin and synaptophysin. 2,5 Based on the location, a neuroendocrine middle ear adenoma would be considered as a differential diagnosis, whereas the histomorphology of papillary projections could be suggestive of a metastatic papillary thyroid carcinoma or a choroid plexus papillary carcinoma, all uncommon neoplasms in dogs. Middle ear adenomas do not typically exhibit papillary projections, do not invade temporal bone, and do not have biologically aggressive behavior. 4,5 Immunohistochemically, middle ear neoplasms are positively labeled for chromogranin and synaptophysin, which were negative in this case. 5 In humans, ELSTs can have a cystic appearance similar to thyroid adenomas. 5 Although 1 of the neoplasms described here had rare focal goblet cell differentiation, a cystic pattern was not observed in either case. There was no clinical evidence of a functional thyroid neoplasm for either dog, and the neoplastic cells were negative for thyroglobulin, making a diagnosis of a thyroid neoplasm highly unlikely. The endolymphatic sac is considered neuroectodermal in origin; therefore, it is difficult histologically and immunohistochemically to differentiate between a choroid plexus papilloma and an ELST. 5,6 In this case, a choroid plexus tumor was considered less likely due to lack of neurologic signs and absence of a choroid plexus neoplasm. Endolymphatic sac tumors have not been previously reported in dogs but should be considered for inner and middle ear masses. The diagnosis in both of these dogs was based on a combination of location of the neoplasm, its morphologic appearance and immunohistochemical labeling pattern, and its aggressive clinical behavior.
Endolymphatic sac tumors in humans are slow growing, locally invasive, and rarely metastasize. 3 This is similar to what was observed in the 2 dogs described here, as there was no obvious tumor recurrence at 12-month (dog No. 1) and 9-month (dog No. 2) recheck examinations.
Footnotes
Acknowledgement
We thank Thomas Wood for technical assistance in immunohistochemistry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.