
Abstract
Since its discovery, the immunogenicity of the Dal blood type has not been further investigated. The aim of this study was to better characterize anti-Dal alloantibodies produced following sensitization of Dal-negative dogs, notably their rate of appearance, the agglutination titer over time, and their immunoglobulin class. A secondary objective was to obtain polyclonal anti-Dal alloantibodies to increase the availability of Dal blood typing. Of 100 healthy laboratory Beagles tested, 2 Dal-negative dogs were identified as recipients. Ten healthy Dal-positive dogs were investigated as potential blood donors. All dogs were extensively blood typed for DEA 1, 3, 4, 5, and 7, as well as for Dal. Then, the recipients were transfused uneventfully with 10 ml/kg of Dal-positive but otherwise compatible packed red blood cells. Posttransfusion blood samples were collected routinely over a minimum of 1 year. Using a gel column technology, anti-Dal alloantibodies were detected as early as 4 days posttransfusion and remained detectable 2 years posttransfusion, with maximum agglutination titers reached at 1 and 2 months posttransfusion. The immunoglobulin class was IgG. The immunogenicity and clinical significance of the Dal blood type were confirmed. The results support the recommendations that previously transfused dogs be crossmatched starting 4 days posttransfusion and for the animal’s lifetime. The polyclonal anti-Dal antibodies produced will allow blood typing of a significant number of dogs, especially transfused dogs facing blood incompatibilities and canine blood donors.
Canine blood types were first identified due to the investigation of alloantibodies produced following experimental blood transfusions in dogs. 7,31 Dogs do not possess naturally occurring red blood cell (RBC) antibodies of clinical importance. 18,31,32 However, a blood transfusion containing RBC antigens lacking in the recipient may lead to sensitization, that is, the production of alloantibodies directed against such antigens. 3,7,37 Advancements in veterinary medicine have resulted in more frequent multiple blood transfusions in canine patients, increasing the risk of transfusion reactions including hemolytic immune-mediated reactions.
Current transfusion recommendations are to blood type canine recipients for DEA 1 prior to transfusion and to provide DEA 1 type-specific blood. When typing is not available, use of DEA 1-negative blood is recommended because of its well-documented immunogenicity and its prevalence in the canine population. Several commercial in-house typing kits are available (DEA 1 Alvedia QuickTest, Alvedia, Lyon, France; DiaMed-Vet ID Card DEA 1.1, DiaMed (no longer available in North America), Cressier-sur-Morat, Switzerland; RapidVet-H Canine, DMS Laboratories, Flemington, NJ, USA; QuickVet DEA 1.1 blood typing cartridge/analyzer, Scandinavian Micro Biodevices ApS, Farum, Denmark). 14,30 Following a first blood transfusion, most authors recommend to crossmatch the recipient to possible blood donors starting 4 days posttransfusion and before every blood transfusion thereafter for the animal’s lifetime. 4,13,14,17 Most experimental studies involving incompatible blood transfusions in dogs were published before 1970. 8,27,32,37 –39 Although several recent case reports have documented acute immune-mediated hemolytic transfusion reactions in dogs, notably to DEA 1, DEA 4, and a common antigen not further characterized, 6,14,24 little is known about the production of alloantibodies following sensitization, including the rate of appearance of alloantibodies and their persistence over time.
The Dal blood group is an immunogenic red cell antigen associated with the production of anti-Dal alloantibodies following a first incompatible Dal-positive (Dal+) transfusion. The Dal antigen was identified a decade ago following a blood incompatibility in a Dal-negative (Dal–) Dalmatian. 3 Dal– dogs are rare and, to date, they have been identified in Dalmatians and in Doberman Pinschers, 15 but little is known about the clinical importance of anti-Dal alloantibodies.
Except for DEA 1, canine blood typing relies on the availability of polyclonal reagents produced following the sensitization of negative dogs. 19 Such availability may become problematic when dealing with a high-frequency antigen. Currently, there is limited accessibility to DEA 3, 5, and Dal reagents and a complete lack of accessibility to DEA 6 and 8 reagents, threatening the sustainability of canine blood typing. 18 The last studies using DEA 6 and 8 reagents were published in 1986 and 1976, respectively. 10,34
We aimed to produce anti-Dal alloantibodies following sensitization of Dal– dogs to better characterize anti-Dal alloantibodies, notably the rate of appearance, the agglutination titer over time, and the immunoglobulin class, and assess the stability of stored frozen aliquots of polyclonal anti-Dal alloantibodies to increase the availability of Dal blood typing.
Materials and Methods
Animals
To identify Dal– recipients and Dal+ donors, 100 healthy research/teaching Beagles located on the campus of the Faculté de Médecine Vétérinaire of the University of Montreal were investigated from January 2010 to July 2014. Ten blood donors (> 25 kg, 2 to 8 years old) already enrolled in the canine blood donor program of the University of Montreal were also blood typed extensively in November 2013. For antibody detection, the plasma of interest was tested against a panel of fresh RBC (Ethylenediaminetetraacetic acid [EDTA]-anticoagulated samples ≤ 72 hours after collection) from known Dal+ and Dal– dogs. More precisely, the RBC used on the panel were collected from known Dal+ blood donors of the canine blood donor program of the University of Montreal, which had already been blood typed as part of a prevalence study. 15 In addition, leftover EDTA-anticoagulated canine blood samples from the laboratory were used as needed for additional Dal+ control. Finally, 2 previously identified Dal– dogs were used as negative controls. The study was approved by the Institutional Animal Care and Use Committee of the University of Montreal.
Presensitization Steps
To identify Dal– recipients and their respective Dal+ donor, all dogs were typed for Dal. Briefly, following centrifugation of the EDTA blood, 5 μl of RBC concentrate were added to 0.5 ml of an antibody enhancement solution (low ionic strength saline; Ortho-Clinical Diagnostics, Raritan, NJ, USA) to obtain a 0.8% RBC suspension. Fifty μl of the RBC suspension and 25 μl of the anti-Dal polyclonal antiserum (serum from a sensitized Dal– Doberman Pinscher, Tufts University, 2007) were placed on top of a gel column on a buffered saline ID card (ID-MTS Micro Typing system; Ortho-Clinical Diagnostics, Pompano Beach, FL, USA). The card was incubated at 37°C for 15 minutes (ID incubator 37 S I, DiaMed Microtyping System, Switzerland) and then centrifuged for 10 minutes (ID centrifuge 12 S II, DiaMed Microtyping System). Results were interpreted according to a standardized classification and graded from 1+ to 4+. 3,16 Dal+ agglutination reactions are usually strong, that is, 3 to 4+. 3,19 Only 2+ or greater agglutination reactions were considered positive.
To assure sensitization specifically for Dal, the identified Dal– recipients and 10 healthy blood donors were extensively blood typed for DEA 1, 2 using the Alvedia DEA 1 lab test and DEA 1.1 and 1.X reagents (ABRI, Stockbridge, MI, USA), as well as for DEA 3, 4, 5, and 7 (ABRI; DEA 3 polyclonal antibodies available for research purposes only), using tube and gel column techniques in parallel, 19 according to the manufacturer’s instructions. Both recipients were blood typed as DEA 1+ and 4+ (Dal–). The blood donor selected had to be incompatible only for Dal, that is, Dal+, but compatible for all other blood types tested. As several blood donors respected these criteria, final selection was based on donor availability and the strength of the agglutination reaction for Dal; that is, dogs with the maximal agglutination reactions (4+) were selected, which most likely correlates with a higher erythrocyte antigen expression. 2 Consequently, the 2 healthy blood donors selected for the study were blood typed DEA 1–, DEA 4+, and Dal+ (4+ agglutination reaction).
Sensitization of Dal– Dogs
The day before sensitization, blood was collected from the selected blood donor using the standardized procedure of the Centre Hospitalier Universitaire Vétérinaire (CHUV) canine blood donor program and following owners’ consent. A total of 450 ml ± 15 ml of whole blood was collected from the jugular vein with a sterile vacuum system using appropriate collection bags (Teruflex blood bag system anticoagulant citrate phosphate dextrose and Optisol [AS-5] red cell preservative; Terumo Corporation, Tokyo, Japan). The blood collected was centrifuged, and the plasma was separated and frozen for clinical purposes. Packed RBC were stored at 4°C until transfusion the day after.
To avoid fluid overload, 15 ml/kg of blood was collected prior to transfusion from each recipient following mild sedation with butorphanol (Torbugesic-SA; Zoetis/Fort Dodge Animal Health, Overland Park, KS, USA) (0.2 mg/kg IV) on day 0, that is, November 2013 for dog No. 1 and January 2015 for dog No. 2. To mimic the exposure to red cell antigens from a standard blood transfusion, a total of 10 ml/kg of Dal+ packed RBC from the selected donor was transfused over a maximum of 4 hours.
During the transfusion and every 4 hours for the following 24 hours, the dogs were closely monitored including rectal temperature, pulse, respiratory rate, mucous membranes, and urine color (eg, hematuria or hemoglobinuria). Packed cell volume, total solids, and serum color were evaluated 2 hours posttransfusion for dog No. 1 and 1, 2, and 4 hours posttransfusion for dog No. 2. Hematology and biochemistry profiles, in addition to Coombs tests, were performed pretransfusion and, on several occasions, posttransfusion (see Supplemental Table 1 for laboratory testing after transfusion of Dal+ erythrocytes in dog No. 1 and dog No. 2). More specific, all Coombs tests were performed using antiserum to canine IgG, IgM, and C3 (VMRD, Pullman, WA, USA) and occasionally performed in parallel with the immunochromatography-based canine direct antiglobulin test (QuickTest DAT; Alvedia, Lyon, France), according to the manufacturers’ instructions.
Concordance of Dal Typing Using Different Reagent Sera.a
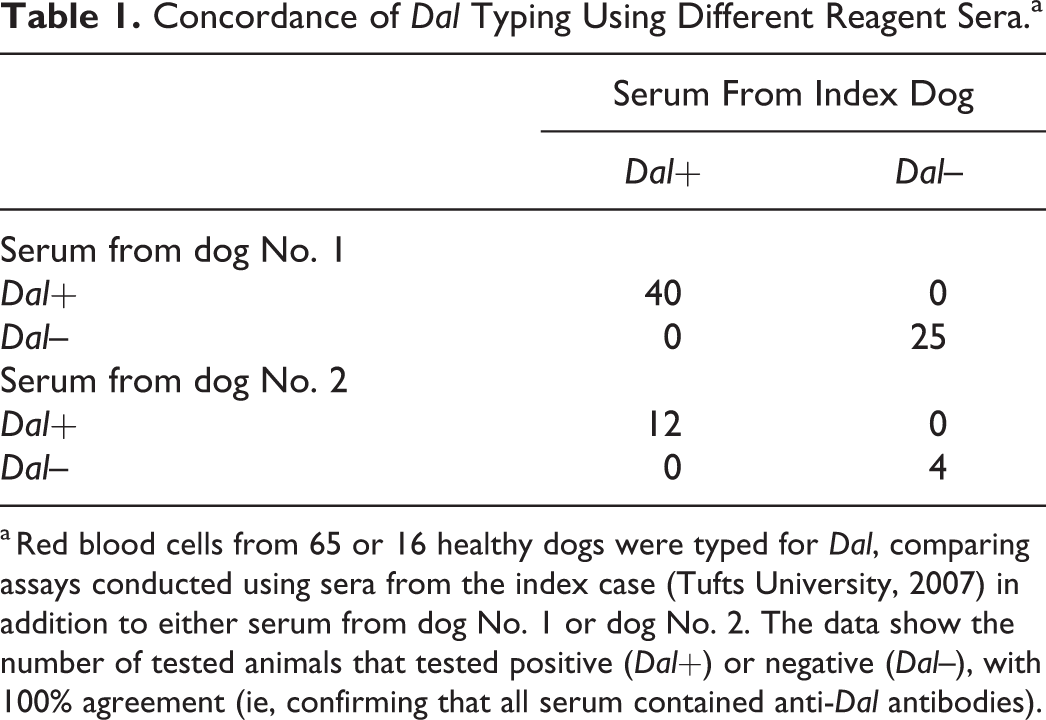
a Red blood cells from 65 or 16 healthy dogs were typed for Dal, comparing assays conducted using sera from the index case (Tufts University, 2007) in addition to either serum from dog No. 1 or dog No. 2. The data show the number of tested animals that tested positive (Dal+) or negative (Dal–), with 100% agreement (ie, confirming that all serum contained anti-Dal antibodies).
Rate of Appearance of Alloantibodies and Agglutination Titers
To detect Dal alloantibodies in the serum or the plasma of the recipients, gel column technology was used. The testing was performed daily for the first week and once a week for the first month until alloantibodies were detected. Briefly, serum or plasma was separated by centrifugation and then 25 μl were added to the incubation chamber in addition to 50 μl of a 0.8% specific RBC suspension. For the auto-control, RBC from the sensitized dog itself were used. For antibody detection, a panel of known Dal+ RBC from 2 to 3 dogs was used. Known Dal– RBC from 1 to 2 dogs was used as a negative control. The gel column card was incubated at 37°C for 15 minutes and then centrifuged for 10 minutes. Results were interpreted as follows: anti-Dal alloantibodies were considered present when the RBC were trapped on top of or within the gel column containing Dal+ RBC (graded 1+ to 4+). If the RBC were able to pass through the gel column forming a pellet at the bottom, the reaction was considered negative.
The agglutination titer was defined as the highest serum dilution where a positive agglutination reaction was observed and was expressed as the whole number corresponding to the serum dilution. Once anti-Dal alloantibodies were detected, agglutination titers were assessed daily for the first week, once a week for the first month, and then once a month for 1 year. In addition, the agglutination titers of dog No. 1 were reassessed at 1.4 and 2 years posttransfusion. The agglutination titers were determined using a 2-fold dilution of the recipients’ serum or plasma in phosphate-buffered saline (PBS), against known Dal+ RBC, similarly to the antibody detection steps described above. This step was repeated in duplicate or triplicate to assure repeatability of the results (Fig. 1).
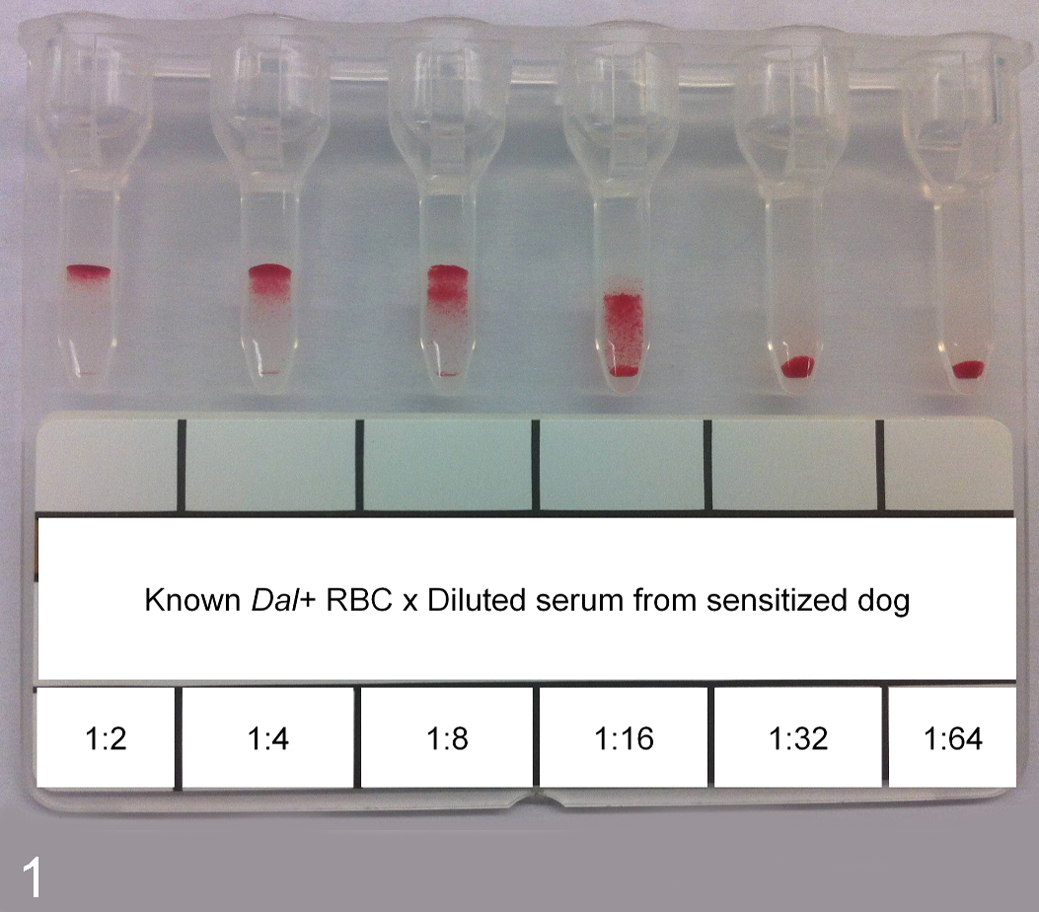
An agglutination titer of 16 with a 2-fold serum dilution and known Dal+ red blood cells (RBC). The results shown correspond to the fresh serum of dog No. 1, 5 months after transfusion of Dal+ RBC.
Persistence of Transfused RBC
For dog No. 2, for each blood sample collected posttransfusion, the RBC were incubated with anti-Dal polyclonal reagent using the gel column technology to detect the Dal+ transfused RBC. This step was performed in duplicate using 2 undiluted anti-Dal polyclonal reagents (1-serum from a sensitized Dal– Doberman Pinscher dog, agglutination titer of 8, Tufts University; 2-serum from previously sensitized dog No. 1, agglutination titer of 32) until Dal+ RBC could no longer be detected.
Immunoglobulin Class
To determine the immunoglobulin class, agglutination titer was determined following treatments with sulfhydryl reagents (dithiothreitol [DTT] and 2-mercaptoethanol [2-ME]), which break the disulfide bonds of IgM and abolish their agglutinating and complement-binding activities. For dog No. 1, a frozen serum aliquot collected 12 weeks posttransfusion was tested 8 weeks later. For dog No. 2, as soon as antibodies were detected, that is, day 21 posttransfusion and up to 8 weeks posttransfusion, fresh serum was tested. Serum was incubated in a 1:1 ratio with either PBS, DTT 0.01 M, or 2-ME 0.1 M. 11,14 The suspensions were incubated at 37°C for 60 minutes and then the agglutination titer was determined as described above.
Concordance of Dal Blood Typing
To confirm that the antibody produced by the recipient was specific for Dal, the sera of both recipients were compared to the anti-Dal polyclonal serum from the index dog identified at Tufts University in 2007. In other words, Dal typing of 65 and 16 dogs was performed in duplicate using the index anti-Dal polyclonal serum as well as the frozen serum from dog Nos. 1 and 2, respectively.
Stability Through Freezing
At each time point when blood was collected, serum aliquots were frozen at –20°C. Agglutination titers were performed in triplicate on frozen serum aliquots 6 months posttransfusion to evaluate the stability of the polyclonal anti-Dal antibodies through freezing.
Results
Presensitization Steps
Of 100 Beagles, only 2 Dal– Beagles were identified (ie, 98/100 Beagles were Dal+) and they were selected as recipients. Dog No. 1, a 2-year-old female spayed Beagle, was identified from the CEGEP of Saint-Hyacinthe teaching colony in June 2013. Dog No. 2, a 3-year-old female intact Beagle from the University of Montreal teaching and research colony, was identified in July 2014. Both dogs were originally acquired from Marshall BioResources (North Rose, NY, USA); their closest shared ancestor was a great, great grandsire. Both recipients were healthy based on physical examination, hematology, and biochemistry profiles.
Sensitization of Dal– Dogs
Transfusions from the Dal+ donors to Dal– recipients were uneventful with no clinical signs of acute or delayed transfusion reaction observed. Overall, packed cell volume (PCV) and total solids remained stable over time. No evidence of intravascular hemolysis was noted on serum or urine evaluation. Laboratory results were all within normal range including bilirubin, and all Coombs tests remained negative.
Rate of Appearance of Alloantibodies and Agglutination Titers
A positive anti-Dal agglutination reaction was first observed on day 4 for dog No. 1 (titer of 1; 2+ agglutination reaction using undiluted serum) and on day 21 for dog No. 2 (titer of 64; 4+ agglutination reaction using undiluted serum). For dog No. 1, the agglutination titer reached a maximum of 64 at 8 weeks posttransfusion and decreased to 8 one year later and to 2 two years later. For dog No. 2, the agglutination titer reached a maximum of 1024 at 4 weeks posttransfusion and decreased to 32 one year later (Fig. 2). Once the maximal agglutination titer was reached, all agglutination reactions using undiluted serum/plasma of the recipients yielded 4+ reactions.
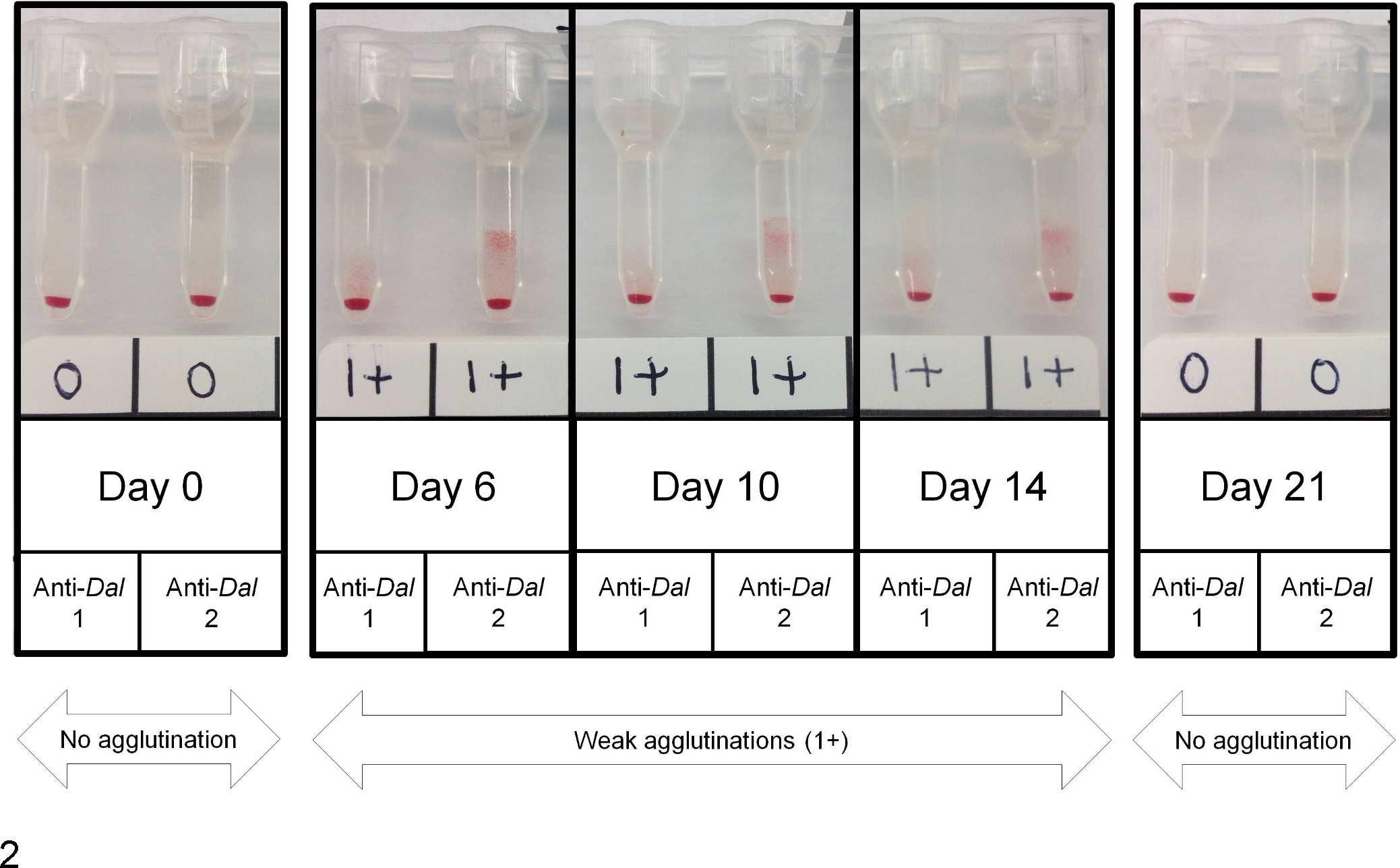
Persistence of transfused red blood cells (RBC) in dog No. 2 assessed by gel column technology with 2 different anti-Dal reagents on several occasions posttransfusion. No agglutination reaction was detected pretransfusion (day 0). A weak agglutination reaction (1+) was detected on days 1 to 10 and day 14. The agglutination reaction was no longer detected on day 21, most likely indicating that no transfused RBC remained in circulation.
Persistence of Transfused RBC
During the 2 weeks following sensitization (samples collected on days 1–10, and on day 14), Dal+ transfused RBC were detected in the blood sample of dog No. 2. The agglutination reaction was weak (1+) but detected on days 5, 6, 9, 10, and 14 with anti-Dal reagent 1 and detected consistently on days 1 through 10 and 14 with anti-Dal reagent 2. However, the agglutination reaction was no longer detected using either reagents on day 21, most likely indicating that no transfused RBC remained in circulation (Fig. 3).
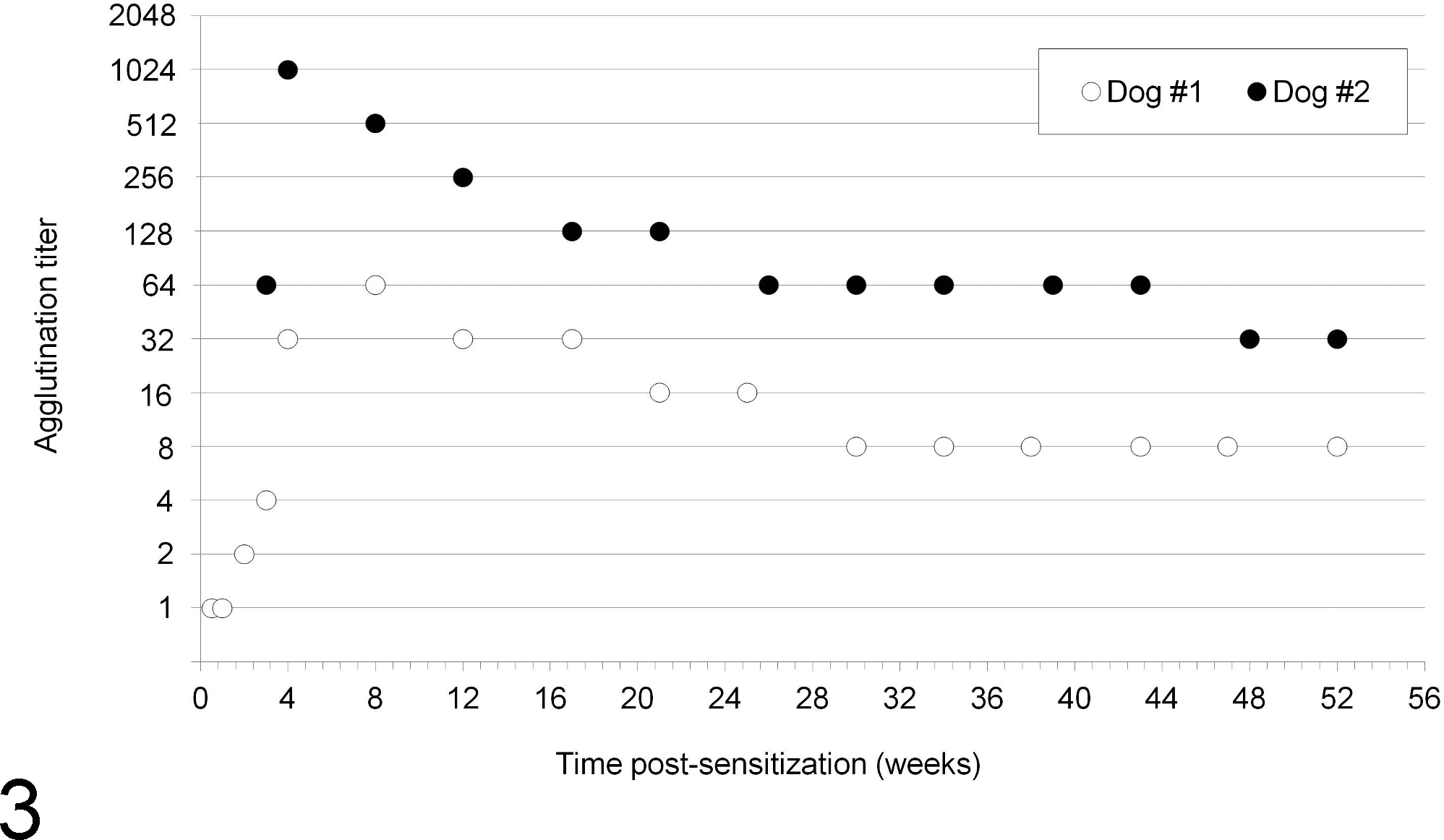
Anti-Dal agglutination titers after sensitization in dog Nos. 1 and 2 over a 1-year period (52 weeks). For dog No. 1, a positive anti-Dal agglutination reaction was first observed on day 4 with a maximum agglutination titer of 64 reached at 8 weeks posttransfusion. For dog No. 2, the anti-Dal alloantibodies were first detected on day 21 with a maximum agglutination titer of 1024 reached at 4 weeks posttransfusion.
Immunoglobulin Class
All agglutination titers remained unchanged following treatment with either DTT or 2-ME, which implies that the causative immunoglobulins were not destroyed by the sulfhydryl reagents, that is, that anti-Dal alloantibodies were IgG.
Concordance of Dal Blood Typing
All dogs typed in duplicate with either serum from dog No. 1 or dog No. 2 had concordant results (Dal+ or Dal–) (Table 1) and similar strength of agglutination reactions when positive (ie, only 3+ or 4+ reactions were observed), which confirmed that at 100%, all serum contained anti-Dal antibodies.
Stability Through Freezing
For dog No. 1, anti-Dal alloantibodies produced between days 4 and 21 (titer between 1 and 4; agglutination reactions graded 2+ to 3+ with undiluted serum) were no longer detected when tested 6 months posttransfusion. However, freezing did not cause any decrease in agglutination titer of anti-Dal antibodies collected on day 28 and thereafter. For dog No. 2, freezing did not cause any change in the agglutination titer for any aliquots tested. In all cases, once the agglutination titer reached a 4+ reaction, aliquots were stable over a 6-month freezing period.
Discussion
Our study highlights the immunogenicity of the Dal blood type with the production of anti-Dal alloantibodies detectable as soon as 4 days posttransfusion and the capacity to shorten the lifetime of transfused RBC. Anti-Dal alloantibodies remained detectable as long as 2 years posttransfusion, supporting that they are long lasting. These results are in agreement with the standard of care in the current literature, which recommends that, to ensure blood compatibility, crossmatching should be performed as early as 4 days following a first blood transfusion and prior to any blood transfusion thereafter for the animal’s life. 4,13,14,17
Acute immune-mediated hemolytic reactions are characterized by clinical signs that usually develop within minutes to hours after a transfusion is started and generally resolve within 24 hours. These clinical signs vary and may include fever, incontinence of urine and feces, vomiting, salivation, lethargy, icterus, tachypnea, hemoglobinemia, bilirubinemia, pigmenturia, hives, and tremors but are rarely fatal. 6,14,24,37 As dogs do not possess clinically important naturally occurring alloantibodies 18,31,32 and as the recipients had never been previously transfused, it is not surprising that both first transfusions of unmatched packed RBC in our study were well tolerated and that no clinical signs of acute hemolysis were detected. For ethical reasons, a second Dal-incompatible transfusion was not administered, limiting some pertinent clinical data. In the literature, all dogs described with an acute immune-mediated hemolytic transfusion reaction had already been sensitized by a first incompatible blood transfusion. However, acute hemolytic transfusion reactions following a first blood transfusion have been reported and are most likely attributable to improper storage or handling of the units or sepsis. 5,29
During and following the Dal-mismatched blood transfusions, no signs of delayed transfusion reactions were observed despite close monitoring and laboratory tests. The definition of a delayed hemolytic transfusion reaction tends to vary between authors. Overall, 2 criteria need to be respected: (1) the reaction/adverse event should occur more than 24 hours posttransfusion, and (2) an increase in the speed of RBC destruction should be detected by either a rapid drop of PCV or clinical/laboratory signs of intravascular or extravascular hemolysis. 1,9,12 –14,22,33 Despite the detection of alloantibodies as early as day 4 in dog No. 1, we were not able to document a delayed hemolytic transfusion reaction using typical clinical and laboratory data. In fact, the destruction of Dal+ RBC could not be indirectly assessed despite repeated PCV and bilirubin measurements over time. Similarly, all Coombs tests remained negative even once anti-Dal alloantibodies were detected. Using the gel column technology, we were able to document in dog No. 2 the presence of Dal+ RBC in circulation until day 14. However, Dal+ RBC could no longer be detected on day 21 posttransfusion, suggesting that Dal+ RBC had been cleared from the recipient’s bloodstream or at least had fallen below the level of detection. It is interesting that this coincided with the first detection of anti-Dal alloantibodies in this recipient.
Using an in vitro biotinylation technique followed by autologous transfusions, the mean ± standard deviation RBC lifespan in Beagles (n = 3) was determined to be 104.3 ± 2.2 days. 26 Comparably, the half-life of compatible transfused RBC is 21 to 43 days, and therefore, a transfusion is expected to last 4 to 6 weeks. 1,23 Similarly, during the course of several experiments focused on the lifespan of donor RBC in previously untransfused recipients, Swisher and Young reported in 1961 evidence of an abrupt increase in the rate of RBC destruction between days 14 and 21 posttransfusion. 31 However, the method used to monitor RBC destruction was not mentioned.
In addition to the presence/production of alloantibodies leading to an immune-mediated hemolysis of transfused RBC, many factors can be responsible for a shortened RBC lifespan posttransfusion, notably inappropriate pretransfusion blood storage conditions and transfusion techniques. 23,29,37 In our study, storage conditions and transfusion techniques followed strict standardized protocols and the transfused packed RBC were collected the day before the transfusion. As the loss of detection of Dal+ transfused RBC after day 21 coincided with the initial detection of anti-Dal alloantibodies, immune-mediated destruction of the Dal+ RBC is quite plausible. That said, the use of more sensitive techniques to assess RBC survival time posttransfusion, for example, chromium-51- or biotin-labeled RBC, would have been ideal, 20,21,25,28,35 but they were not available for this study. In that regard, the gel column technology proved to be a straightforward, inexpensive, and repeatable alternative.
The transfusion of Dal+ packed RBC in Dal– recipients induced marked antibody production with a maximum agglutination titer as high as 1024, which confirms the vigorous immunogenicity of the Dal antigen. The highest reported agglutination titer was also 1024 but was obtained in an experiment study where most DEA 1-negative dogs were immunized repeatedly using multiple 5-ml DEA 1-incompatible transfusions. 7 To our knowledge, the highest documented agglutination titer responsible for an acute hemolytic transfusion reaction in a clinical context was 16, using the tube technique in a dog receiving immunosuppressive drugs. 6,14,24 Similarly, the original Dal study reported an agglutination titer between 8 and 16 in an anemic Dalmatian suffering from chronic kidney disease. 3 It should be noted that the gel column technology used in this study has been shown to be a more sensitive technique than the tube assay used in previous studies. 36 In the present study, the anti-Dal immunoglobulins produced were of the IgG class, which is in agreement with the original publication on Dal and with other known blood group-related alloantibodies described in dogs, although IgM have been described in other species. 3,14
The immunogenicity of blood group antigens is quite variable. In experimental studies, some antigens, like DEA 1, are known to produce strong agglutination titers that can clearly result in acute hemolytic transfusion reactions. Other antigens, like DEA 3 and 5, have been reported to produce weak agglutination titers mostly associated with shortened RBC survival in previously sensitized dogs. 7,32 In general, the higher the titer, the more severe the hemolytic transfusion reaction. 1 That said, the immunogenicity of the Dal was expressed with significant variation between the 2 recipients, notably in the rate of appearance of antibodies (dog No. 1: day 4; dog No. 2: day 21), but mostly with the maximum agglutination titer observed (64 and 1024 for dog Nos. 1 and 2, respectively) and the moment when it was reached (8 and 4 weeks posttransfusion for dog Nos. 1 and 2, respectively). The variable degree of sensitization of the recipients may be explained by numerous factors related to the recipient, including their age, immune system, and hormonal status (intact vs spayed) as well as environmental and genetic factors. In addition, 2 different blood donors were used and their level of erythrocytic antigen expression may have differed. For instance, it has been documented that dogs may express different levels of DEA 1 antigens. 2 However, methods to evaluate the level of antigen expression, for example, flow cytometry, were not available for the present study. To limit the variation of antigen expression, both blood donors were chosen based on the strongest agglutination reaction, that is, 4+. In addition, both recipients received the same quantity of packed RBC within the same timeframe (10 ml/kg within 4 hours to mimic a real blood transfusion). This highlights an obvious limitation of our study. In a clinical context, patients receiving blood transfusions are often in critical condition, requiring multiple treatments including immunosuppressive drugs. Thus, the immunogenicity of the Dal observed in the present study is specific to a particular research context and the data cannot be extrapolated to other blood groups and to sick animals, notably if immunosuppressed. For instance, using healthy dogs may overestimate the immunogenicity of the Dal compared with a clinical setting.
The alloantibodies produced at 21 days postsensitization and thereafter remained stable following a 6-month freezing period, allowing banking of anti-Dal sera for future Dal blood typing. It is unclear why the same freezing period caused the antibodies produced before 21 days in dog No. 1 to be no longer detectable despite the fact that they had been originally detected in duplicate. Their agglutination titer was certainly lower and therefore their clinical significance may have been less.
The lack of access to DEA 6 and 8 could have limited the specificity of the sensitization for Dal. Despite their unavailability, both polyclonal alloantibodies produced showed 100% concordance with the original serum from the index dog and easily interpretable Dal typing results, that is, clear negative (0) or strong positive (3 to 4+) agglutination reactions. Nevertheless, the lack of typing reagents, even for research purposes, highlights an existing problem in veterinary transfusion medicine: by relying solely on polyclonal alloantibodies, the sustainability of blood typing is in peril and comparison studies between already-reported blood groups and newly described ones are already impossible. It is fortunate that this study led to the production and banking of a considerable amount of anti-Dal sera, even though it did not generate a long-term solution.
To date, Dal– dogs have been identified in only Dalmatians and Doberman Pinschers with a prevalence in recent studies of 19% (n = 26) and 37% (n = 310), respectively. 3,15 It is surprising that our study identified Dal– dogs in an additional breed, that is, Beagle. In contrast, all dogs of other breeds tested were Dal+, which means that the vast majority of blood donors are Dal+. 15 Thus, Dal– individuals face a high risk of transfusion incompatibility when in need of blood, and when requiring further blood transfusion, compatible Dal– blood may be almost impossible to find. The polyclonal anti-Dal antibodies produced in this study will permit Dal– blood typing for a significant number of dogs, including canine blood donors and previously transfused dogs with incompatible crossmatches prior to subsequent blood transfusion.
As mentioned, the availability of Dal blood typing remains limited by the use of polyclonal reagents produced following sensitization of a rare Dal– dog. When using gel column technology, the results are easily interpretable (Dal+ agglutination reactions are usually strong, that is, 3 to 4+), but the equipment is usually limited to veterinary teaching hospitals, commercial blood banks, and laboratories. The production of a monoclonal antibody would ensure anti-Dal reagent sustainability and could lead to more user-friendly typing kits, allowing for better description of the Dal prevalence in the general canine population and for characterization of the Dal red cell antigens on a molecular level.
Following sensitization of 2 Dal– dogs, the strong immunogenicity of Dal was documented with anti-Dal alloantibodies detected as early as 4 days posttransfusion, maximum titers reached at 1 and 2 months posttransfusion, and anti-Dal alloantibodies still observable up to 2 years posttransfusion. Our results support that to ensure blood compatibility, crossmatching should be performed as early as 4 days following a first blood transfusion and thereafter prior to any blood transfusion during the animal’s life. Although a hemolytic transfusion reaction was not clinically appreciated, the transfusion of Dal-incompatible packed RBC resulted in a shortened RBC lifespan. Given the very high titers of anti-Dal alloantibodies produced by the Dal– recipients, an acute hemolytic transfusion reaction is considered likely if subsequent incompatible blood transfusions are administered. This poses a considerable challenge for the rare Dal– dogs that will almost certainly be sensitized via a first blood transfusion and for which Dal-compatible blood may be very difficult to find thereafter. A considerable amount of anti-Dal polyclonal reagents stable through freezing was banked for further clinical use and will allow for more readily identifying such patients and compatible canine blood donors.
Footnotes
Acknowledgement
We thank the employees of the Division Ferme et Animaleries of the Université de Montréal located on the Faculté de Médecine Vétérinaire campus for their assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Association des Médecins Vétérinaires du Québec.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.