
Abstract
Bone-sawing procedures are routinely performed during veterinary and human autopsies and represent an important source for infectious aerosols. Here we investigate the generation of aerosols during bone-sawing procedures using 5 different saws regularly used in veterinary and human pathology. In particular, the electrical bone band saw produced vast amounts of aerosolized particles less than 5 µm in diameter, which spread rapidly throughout the entire autopsy hall, leading to an exposure of all personnel. Other sawing devices tested were a diamond-coated cut grinder, an oscillating saw, a reciprocating saw, and a hand bone saw. Although these saws, especially the handsaw, generated fewer aerosolized particles than the band saw, the level of exposure of the saw operator would still be of concern in cases where infectious material would require sawing. Contamination of the entire autopsy area was successfully prevented by the construction of a separately ventilated sawing cabin inside the existing autopsy room. Saw operators in this cabin, however, were exposed to even higher aerosol concentrations. Protection of saw operators was achieved by using a powered air-purifying respirator. In conclusion, our results demonstrate that all bone-sawing procedures applied in veterinary and human pathology can generate aerosols that are of concern for the health of autopsy personnel. To reduce the risk of aerosol infections from bone-sawing procedures, efficient and properly designed ventilation systems to limit the spread of aerosols and appropriate personal protective equipment against aerosols for exposed personnel should be implemented.
Keywords
Autopsies in veterinary and human pathology are usually conducted to determine the cause of death or disease after the death of a patient. Clinical histories vary from detailed presumptive clinical diagnoses to no information on disease status or clinical signs of the patient. During autopsies, pathologists are thus often confronted with unexpected findings, 5,13,23,30 and oftentimes it is not clear at the beginning or even during autopsies whether pathologists are exposed to specific health risks, such as infectious diseases, derived from the autopsied body. Routine autopsy protocols therefore should take necessary work safety precautions into account. Cuts while using scalpels or knives are the most obvious sources of mechanical hazards 32 and are dealt with by a combination of appropriate training and personal protective equipment (PPE). In addition, chemical hazards also exist. 26,28 Furthermore, infectious agents represent a continuous health risk for pathologists. Particularly important for human pathologists are, among others, type A Streptococci, human immunodeficiency virus (HIV), hepatitis B and C, and Mycobacterium tuberculosis. 4,8,9 Veterinarians have a similar risk of infection with numerous zoonotic pathogens. Examples are rabies virus, avian and swine influenza virus, Brucella spp., Coxiella burnettii, Francisella tuarensis, and mycobacteria. 1,23,26,31 Transmission of infectious agents during autopsies can take place through different routes. Most likely routes of infection are via cut wounds or preexisting skin wounds, via smear infections onto skin or mucous membranes, via droplets reaching mucous membranes, and through inhalation of aerosols. 26 Direct contact and smear and droplet infections can be prevented by appropriate autopsy techniques combined with PPE and strict hygiene protocols. Protection against aerosols, however, requires, besides engineering controls, specialized and well-fitted PPE, such as filtering facepiece type 3 (FFP3) respirators or powered air-purifying respirators (PAPRs). 3,22 Such PPE, however, can impair the work of pathologists and should therefore be worn based on a thorough risk assessment. In case the source of the aerosol cannot be eliminated (eg, in routine work procedures), a knowledge of the routine autopsy procedures that generate aerosols and how these aerosols are distributed throughout the autopsy facility is essential to protect personnel by using appropriate PPE.
Aerosols are suspensions of solid or liquid particles in a gas (usually air). Infectious aerosols are frequently composed of airborne particles with a size of approximately 1 to 5 μm in diameter. They can remain suspended in the air for a long time and can reach the pulmonary alveoli upon inhalation. 4,7,19,26 Due to their size, 6,10,18,24,31 many pathogens of zoonotic concern can therefore be aerosolized and be transmitted through inhalation (Table 1). A thorough risk assessment must consider that the level of contamination of aerosols with infectious agents is unknown and can vary to a great extent. Furthermore, the steadiness and longevity of aerosols depend on many factors such as particle size, humidity, and air exchange. 15,20,27 In general, aerosolized particles can lead to a long-lasting contamination of the air 12,19 and thus represent a significant health risk in autopsy facilities. A main source of aerosols in autopsy facilities are bone-cutting procedures, 4,7,19 which are regularly applied during veterinary and human autopsies. Besides the danger of aerosolization of infectious agents from bone lesions, noninfectious bone dust itself might be of concern for autopsy workers as hypersensitivity reactions have been described after inhalation. 2,21 A large variety of instruments, ranging from manual saws to electrical high-power saws and diamond-coated cut grinders especially designed for autopsies, are available. Several studies in human pathology have described aerosols generated by sawing bones. 4,14,25,30 In veterinary medicine, only few reports exist that discuss health risks associated with aerosols generated during autopsies. 1,17,23 To date, no systematic studies about aerosol production during different routine bone-sawing procedures in veterinary pathology have been published.
Sizes and Minimal Infective Doses of Selected Zoonotic Pathogens.
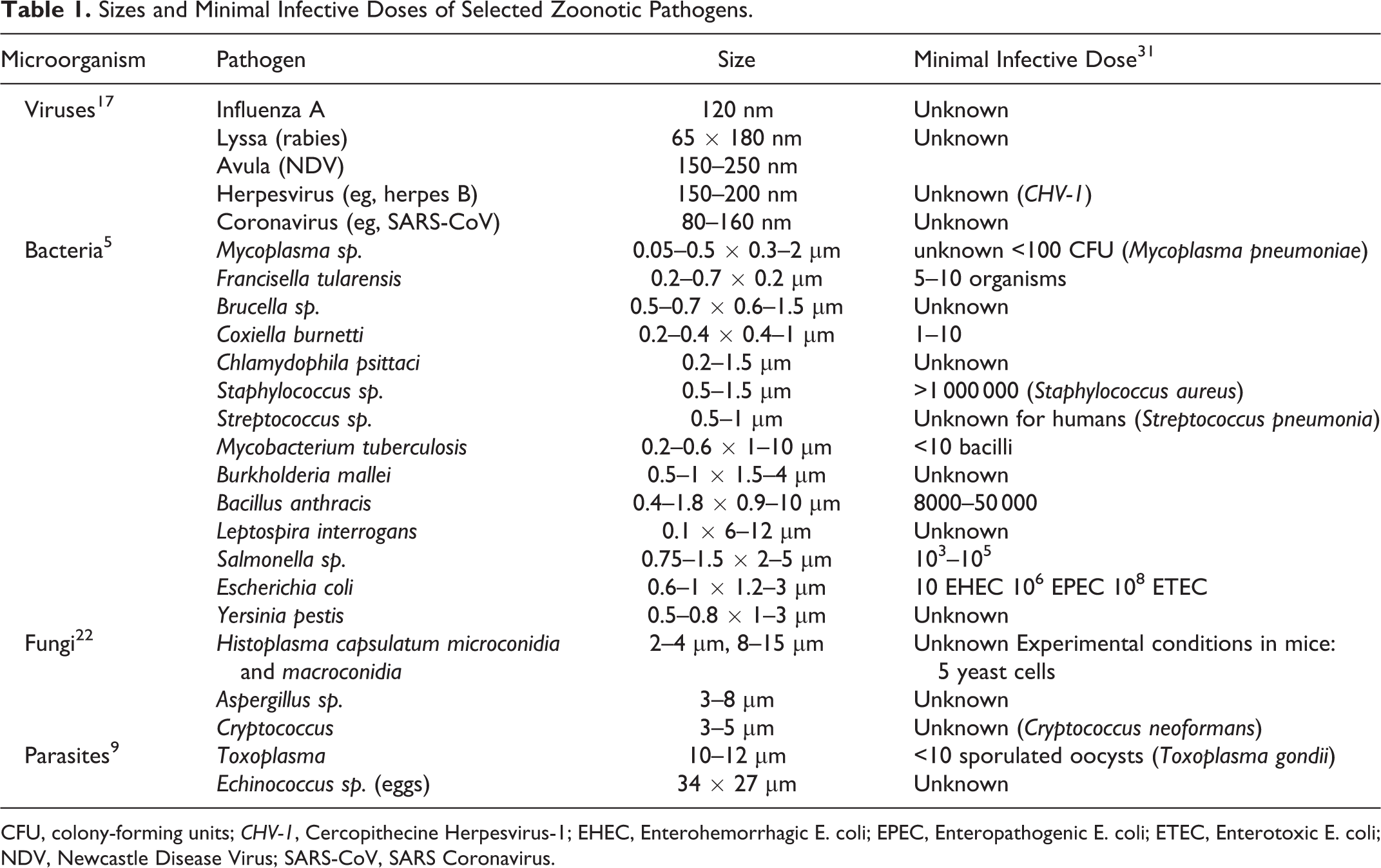
CFU, colony-forming units; CHV-1, Cercopithecine Herpesvirus-1; EHEC, Enterohemorrhagic E. coli; EPEC, Enteropathogenic E. coli; ETEC, Enterotoxic E. coli; NDV, Newcastle Disease Virus; SARS-CoV, SARS Coronavirus.
In this study, we analyzed the aerosol production in 5 bone-cutting procedures that are regularly applied in veterinary pathology. Measurements were taken under controlled conditions and resembled routine daily work, with the regular ventilation system of our autopsy room in operation. Besides aerosol production by different saws, we tested the distribution of aerosols in our autopsy room. Based on our initial findings, a partial reconstruction of the autopsy hall was initiated to limit the spread of infectious aerosols inside our facility. Therefore, we were able to compare aerosol distribution in our facility before and after the construction of a separately ventilated sawing cabin.
Material and Methods
Autopsy Facility
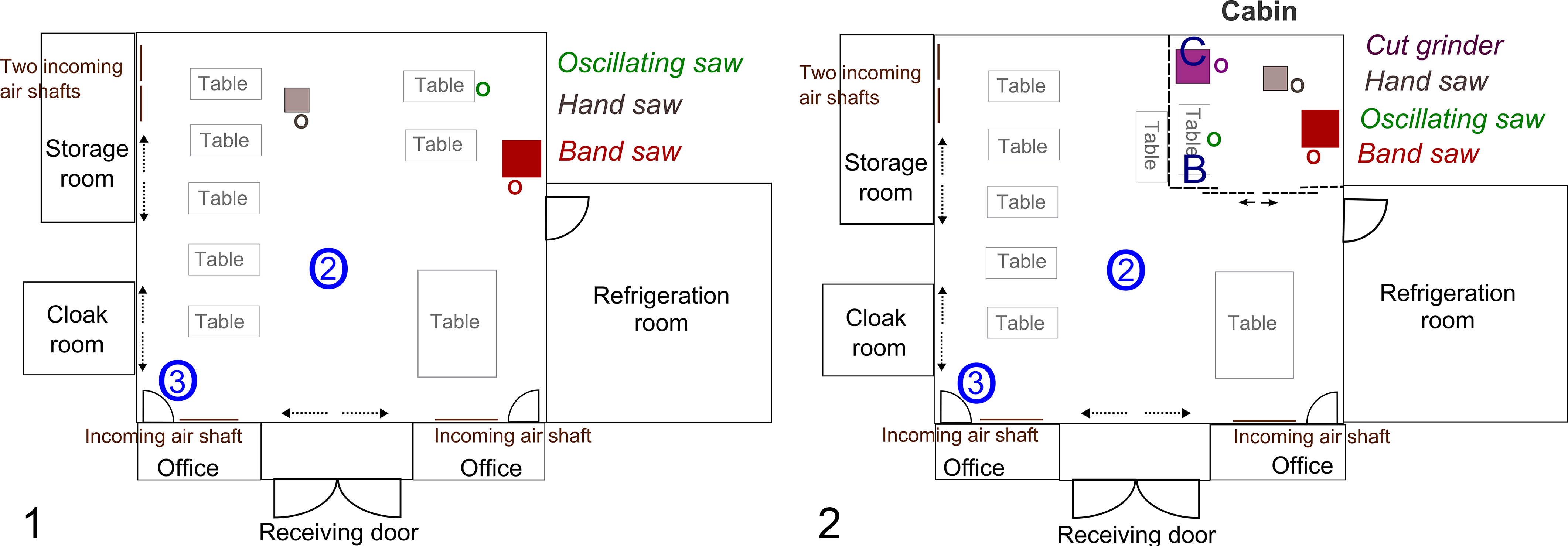
Measurements were carried out in the autopsy hall of the Institute of Animal Pathology, Vetsuisse Faculty, University of Bern. The hall, which was built in 1964, measures 10 × 12 × 4.88 m in size (approximately 485.6 m3). It is equipped with 7 dissecting tables for small animals and 1 table for large animals. Adjacent, but separated by a door from the autopsy hall, are 2 small offices, a storage room, the cloakroom, and a 4°C refrigeration room, which is used to store carcasses for disposal (Fig. 1). After renovation in 2015, the autopsy hall included a separately ventilated cabin (3.30 × 3.80 × 2.90 m), located in 1 corner of the autopsy hall and connected to it via 1 sliding door (Figs. 2–6).

Ventilation System
Before renovation, the ventilation system of the autopsy hall was composed of 4 inflowing air shafts, allocated on 2 sides of the hall, and 8 return air shafts on the ceiling (Frigo AG Bern, Bern, Switzerland). The ratio of exhausted air to the air inflow via the ventilation system was set that an inward airflow toward the autopsy hall was created. The delta between air exhaust and inflow was then replaced by air flowing in through doors and openings to adjacent rooms and the receiving door (Fig. 1). The air exchange rate of the autopsy hall was calculated to be approximately 10 times per hour. Because a separate inflowing airshaft to the sawing cabin was considered technically unfavorable for the existing building, the walls of the newly constructed sawing cabin were elevated 5 cm above the ground, and the cabin received its inflowing air from the main autopsy hall via this slit. Its air exhaust zone was located in the center of the cabin ceiling. This air was HEPA-filtered before being exhausted on the roof of the autopsy building. The output of the exhaust during use of the cabin was set to 1200 m3/h; thus, the air exchange rate in the cabin was set to approximately 30 times per hour.
Saws
The experiments were carried out with 5 different saws: a stationary butcher bone band saw (Suppl. Fig. S1; MKB-653, 5.7A, 400 V, 2.2 kW [MADO GmbH, Dornhan, Germany] with saw blades of 3160 mm length, 340 teeth [J-P. Fracheboud, Worb, Switzerland]), a diamond-coated pathology cut grinder (Suppl. Fig. S2; 50 Hz, 230/400 V, 2 kW, with diamond-coated blade D151, 0.3 mm; Walter Messner GmbH, Oststeinbek, Germany), an oscillating autopsy saw (Suppl. Fig. S4; HB-740, 50 Hz, 230 V, 125 W, 12 000–21 000 oscillation/min [KUGEL Medical GmbH, Regensburg, Germany] with 50-mm saw blades [BIO SYSTEMS AG, Muttenz, Switzerland]), a reciprocating butcher bone saw (Suppl. Fig. S5; EFA 63, 60 Hz, 230 V, 1020 W with 350-mm saw blades; EFA Schmid & Wezel GmbH, Maulbronn, Germany), and a butcher handsaw (Suppl. Fig. S3; INOX, with sawblade: 330 mm length, 100 teeth; F. Dick GmbH, Deizisau, Germany).
Before renovation, the bone band saw was located inside the autopsy hall, close to the refrigeration room door (Fig. 1). The handsaw and the oscillating autopsy saw were used either on a table or on the bench vice inside the autopsy hall (Fig. 1). After renovation, all saws were located inside the sawing cabin (Fig. 2).
Sawing Procedures
To generate aerosols, humeri or femurs of cattle, pig feet, pig spines, thorax of cattle, and pig skulls were sawed according to routine protocols performed during diagnostic autopsies. The samples were taken from regular diagnostic submission to the Institute of Animal Pathology. Skin and muscles were removed and bones were stored at 4°C for 1 to 4 days until use. To compare the aerosol production by different saws, the duration of sawing in each experiment was set at 2 minutes, a time that was considered representative for routine sawing procedures. An exception was the comparison between the diamond-coated cut grinder and the band saw, where not time but the completed procedure of cutting 1 swine foot into 4 pieces (2 cuts) was the limiting parameter. To test the bone band saw, humeri or femurs of cattle older than 1 year were cut twice (sagittally and longitudinally). The sharpness of the band saw blades was categorized into 3 different groups (sharp, medium, and dull). Sharp blades were new or freshly sharpened blades, which had been used only 1 to 3 times. Dull blades were those that caused difficulty for the operator to cut through bone. Medium was predefined as blades that were neither sharp nor caused difficulties to cut through the respective bone. A water supply to provide constant moistening of the band saw blade by tap water was also added to the band saw (Suppl. Fig. S1). To examine aerosol production by the diamond-coated cut grinder, 1 swine foot was sawed twice (sagittally and longitudinally). The oscillating autopsy saw was tested by opening spines of pigs ranging from 50 to 80 kg to the left and the right of the spinous processes until the spinal cord was freed. To demonstrate aerosol production by a reciprocating saw, we had to adapt the routine protocol because on-site measurement under conditions simulating our routine operating procedure were hampered by large fluctuations of base levels of aerosol particles during the routine procedure on our large animal autopsy table. We therefore prepared isolated thoracic cavities from cattle over 1 year (emptied thoracic cavity with intact ribcage) and placed them on a table inside the sawing cabin to be sawed using the reciprocating saw for 2 minutes. To test aerosol production by the handsaw, a rectangle was sawed into a pig skull (50 to 80 kg total body weight) with 1 transversal cut on the frontal bone, 2 cuts parallel to the crista sagitalis (left and right side of the occipital bone), and a fourth transverse cut through the parietal bone.
Particle Counting
Aerosolized particles were counted using the laser diode particle counter CI-7300 (Suppl. Fig. S12; 50 Hz, 230 V, 1.32 kW; CLIMET Instruments Company, Redlands, CA), in combination with the diluter DIL-554 (9 V, 30 kPa; Topas GmbH, Dresden, Germany) (Suppl. Fig. S6). Six different particle sizes were recorded as 0.3 to 0.5 μm, 0.5 to 0.7 μm, 0.7 to 1 μm, 1 to 5 μm, 5 to 10 μm, and >10 μm. The DIL-554 generated a constant and reproducible aerosol dilution of 1:100 at a total flow rate of 1 cubic feet per minute (1 cfm = 28.3 l/min). The particle counter was set to determine the average particle count of 3 measurements (20 seconds with a 5-second interval) for each indicated time point. Because personnel movements and opening of doors resulted in large disturbance of airflows in the autopsy hall and thus large fluctuations of base levels of particles in the air, all measurements were performed in the morning, during times when no regular autopsy work was performed. Before the start of the sawing procedures, ground measurements were obtained for all differently sized particles. The inlet of the particle counter was fixed at a height of 1.60 m (Suppl. Fig. S6), which was equivalent to the shoulder height of the operator. Three different positions of the particle counter were chosen inside the autopsy hall: the operator position (shoulder height of the operator, at a 50-cm distance from the saw blade), position 2 (in the middle of the autopsy hall, at a 7.50-m distance from the stationary band saw), and position 3 (in 1 corner of the autopsy hall, at a 15-m distance from the stationary band saw) (Fig. 1). After the renovation, positions 2 and 3 remained the same, while the operator position was now located inside the cabin (Fig. 2). Inside the sawing cabin, we also measured at position B (in the left front corner of the cabin, a 3.40-m distance from the band saw) and position C (in the left back corner of the cabin, a 2.90-m distance from the band saw).
PAPR
We tested a commercially available PAPR with a TH3 protection level (Suppl. Fig. S7; 3M Versaflo TR-300) in combination with a head cover with integrated head suspension (S-133L-5; 3M GmbH, Rueschlikon, Switzerland) for aerosol protection for our personnel.
The test was performed using the TSI Portacount Pro+ Respirator Fit Tester (Model 8030; TSI Incorporated, Shoreview, MN), as previously described. 22 Shortly, the device determined the performance factor (PF) of the PAPR as the ratio of particle concentrations outside to particle concentrations inside the head cover. The test included 7 measurements in 64-second intervals, each consisting of 24 seconds of cleaning the sensors and 40 seconds of measurement time, and was repeated 3 times. During the 40-second measurement period, calf femurs and humeri were cut once sagittally using the bone band saw. The TSI Portacount Pro+ Respirator Fit Tester determined the PF for each individual measurement and finally the overall performance factor using the Porta Count Pro Fit Tester (FitPro+ Fit Test Software) software following the Occupational Safety and Health Administration (OSHA) protocol as previously described. 22
Statistics
Statistical analyses were performed using SPSS (version 21.0; SPSS, Inc, an IBM Company, Chicago, IL). Normal distribution was analyzed by histograms and Kolmogorov-Smirnov tests. All data were transformed logarithmically, and significance was evaluated with the univariate analysis of variance (ANOVA) and t test. Due to the large number of tests carried out, the differences were considered significant when P < .005. This is 10 times lower than the common significance level of P < .05. The Scheffé test was used as post hoc analysis to evaluate variations in the number of particles produced between the saw blades with different sharpness.
Results
Band saw
The bone band saw produced vast amounts of respirable aerosolized particles of diameters between 0.3 and 5 μm (Fig. 7). At the position of the operator, a massive and rapid increase of aerosols was detected shortly after starting the sawing (Fig. 7 and Suppl. Figs S8 and S15-S18, Suppl. Movie). The peak concentration of particles from 0.3 to 0.5 μm in diameter was 7.1 × 106 particles/cfm (Fig. 7). With a time lapse of approximately 75 seconds after the start of the sawing procedure, an increase of particles was detected at position 2 (data not shown). Here, the maximum value of 1.8 × 106 particles/cfm (0.3–0.5 μm particles) was detected after 4 minutes. Importantly, also 15 m away from the saw (position 3), aerosol concentrations mounted considerably 2.5 minutes after the start of the sawing procedure (Fig. 7). The maximum concentration (approximately 9.8 × 105 particles/cfm, particle size 0.3–0.5 μm) was detected after 5 minutes and remained on this level for another 2.5 minutes, until values dropped slowly (Fig. 7). The concentrations of larger particles increased similarly, albeit to a lesser extent (Suppl. Fig. S9). Upon termination of the sawing procedure, the concentrations of differently sized particles decreased relatively quickly during the first 15 minutes at all positions, but base levels, especially of the smallest particles, were reached only after approximately 1 hour. Large particles between 5 and 10 μm reached a maximum of 2.2 × 103 particles/cfm at the operator position and 1 × 102 at position 3 (data not shown). Particles >10 μm in diameter reached a maximum of 1.7 × 103 particles/cfm at the operator position and 7 × 101 at position 3 (data not shown).
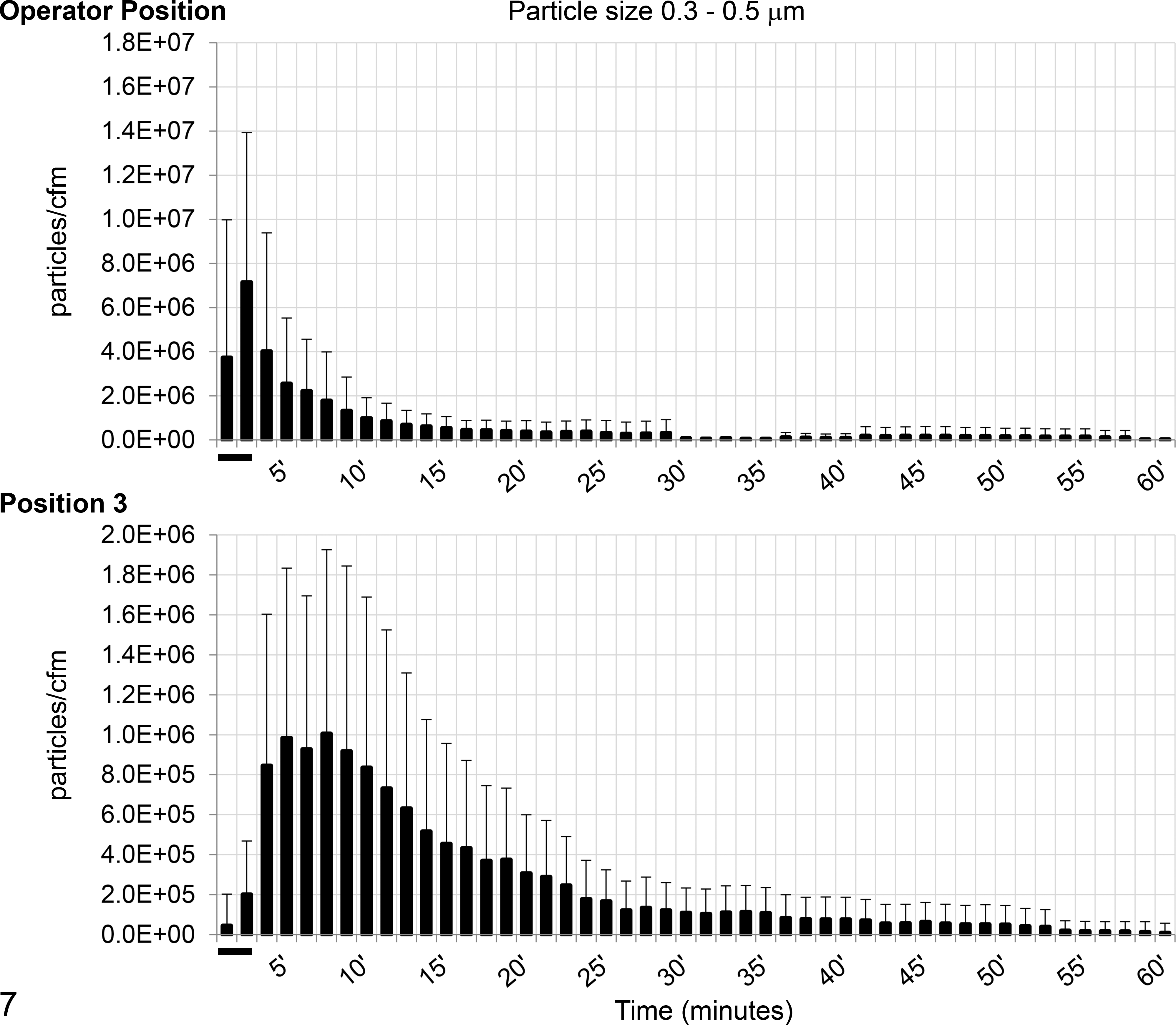
Particle concentrations at 2 different positions generated by the bone band saw inside the autopsy hall: operator position (refers to the person operating the band saw) and position 3, which was at a 15-m distance from the band saw. Mean values (bars) and the standard deviations of 20 experiments of particles 0.3 to 0.5 μm in diameter. Note differences in scales on y-axes. Bones used were bovine humeri or femurs. The saw was operated during the first 2 minutes (indicated by a black bar).
These results prompted us to construct a separately ventilated sawing cabin inside the existing autopsy hall as an engineering control to decrease the exposure of personnel to aerosols (Figs. 2, 4–6). After these renovations were completed, the same measurements were repeated with saws now located inside the sawing cabin.
Importantly, aerosol concentrations generated by the bone band saw inside the cabin were even higher than those detected when the saw was operated in the main autopsy hall (Fig. 8). After 2 minutes, the maximum value of 11.7 × 106 particles/cfm (0.3–0.5 μm) was detected at the operator position, and with a time lapse of 1 minute maximum, levels of 7.7 × 106 (position B) and 6.7 × 106 particles/cfm (position C, data not shown) were measured at distant spots in the cabin. The concentrations of larger particles again rose similarly but to lower levels (Suppl. Figs. S10, S11). Similar to the results in the autopsy hall, concentrations of particles larger than 5 μm hardly rose and reached maximum levels at the operator position of 8 × 103 particles/cfm (5–10 μm) and 6.6 × 103 particles/cfm (>10 μm) (data not shown). The decrease of the particle concentrations was faster compared with the situation inside the autopsy hall, and base levels for all particles were reached within 20 minutes (Fig. 8 and Suppl. Figs. S10, S11).
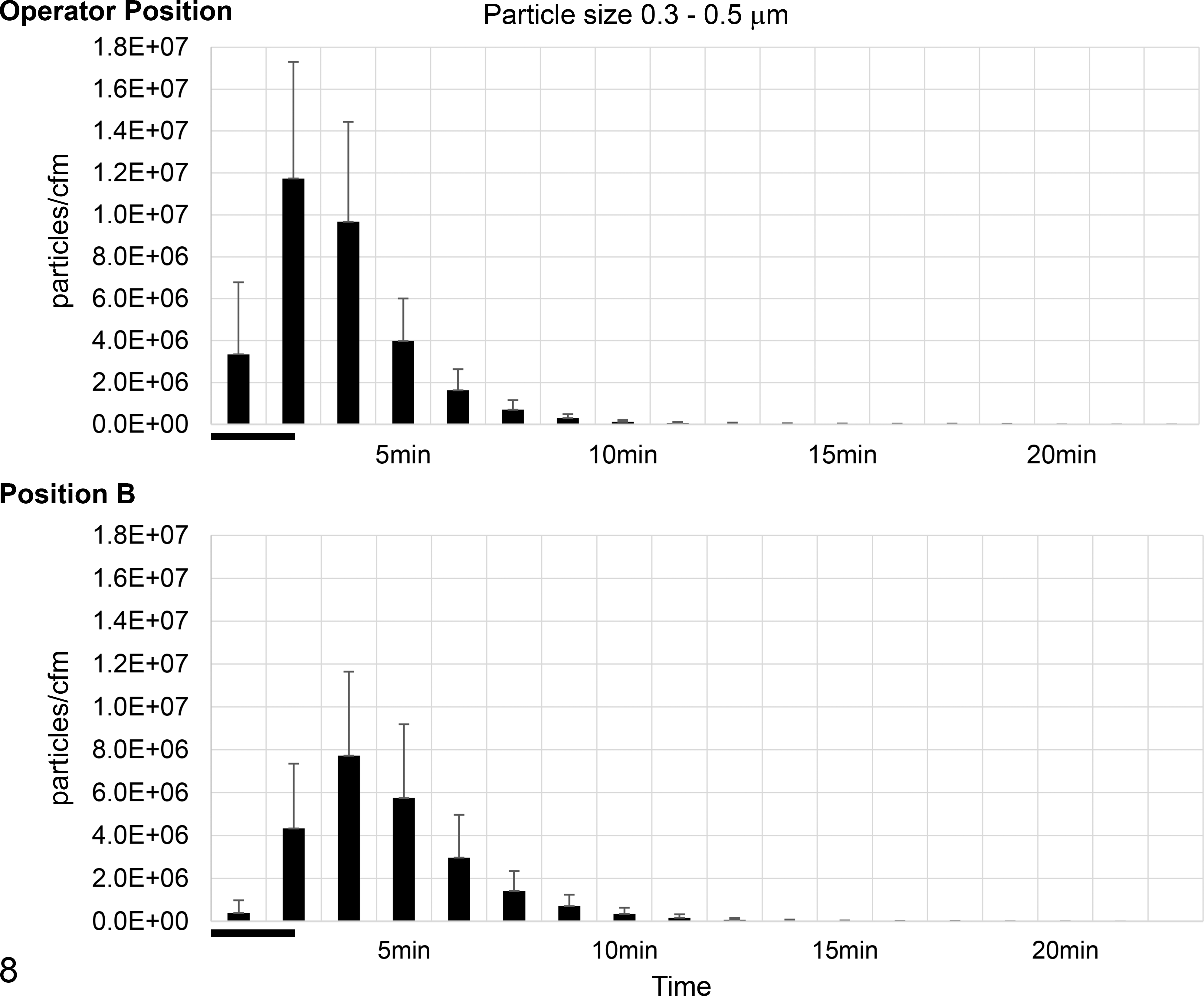
Particle concentrations at 2 different positions generated by the bone band saw inside the sawing cabin: operator position (refers to the person operating the band saw) and position B, which was at a 3.4-m distance from the band saw. Mean values (bars) and the standard deviations of 20 experiments of particles 0.3 to 0.5 μm in diameter. Bones used were bovine humeri or femurs. The saw was operated during the first 2 minutes (indicated by a black bar).
When the doors of the sawing cabin remained closed during the sawing procedure, no increase in particles was detected inside the autopsy hall (Fig. 9). However, when the door was left open, an increase of particles of sizes 0.3 to 0.5 μm was detectable outside the cabin shortly after starting the sawing procedure (Fig. 9). A small rise was also seen for particles with the sizes of 0.5 to 0.7 μm in diameter (data not shown). No increase was detected for particles larger than 0.7 μm.
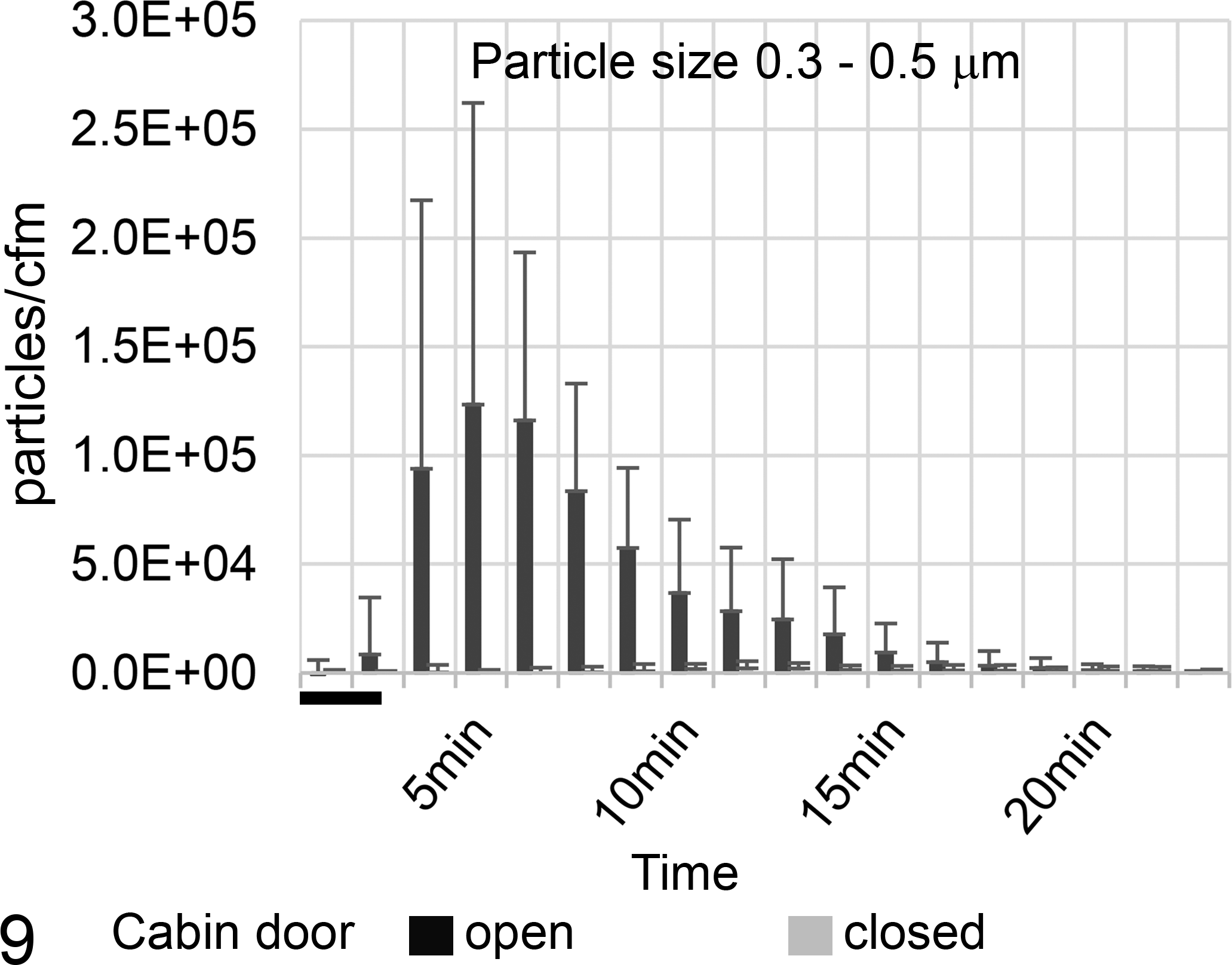
Concentration of 0.3- to 0.5-μm diameter particles in the middle of the autopsy hall (position 2, after renovation), during and after sawing with the bone band saw inside the sawing cabin with closed and open cabin door. Mean values (bars) and the standard deviations of 11 experiments. Particle concentrations under 2000 particles/cfm were considered normal fluctuations of the base value. Bones used were bovine humeri or femurs. The saw was operated during the first 2 minutes (indicated by a black bar).
Impact of the Sharpness of the Band Saw Blades
In addition, the impact of the sharpness of the band saw blades on aerosol production was tested. Medium and dull blades produced considerably more aerosolized particles than sharp blades (Fig. 10). The difference between the groups was significant (P < .003). Notably, there was a significant difference for particle sizes of 0.3 to 0.5 μm, 0.5 to 0.7 μm, 0.7 to 1 μm, and 1 to 5 μm between dull and sharp blades (P < .0000008), between dull and medium blades (P < .001), and between medium and sharp saw blades (P < .003). Significant differences in particle sizes of 5 to 10 μm (P = .003) and >10 μm (P = .005) were present between dull and sharp blades (data not shown).
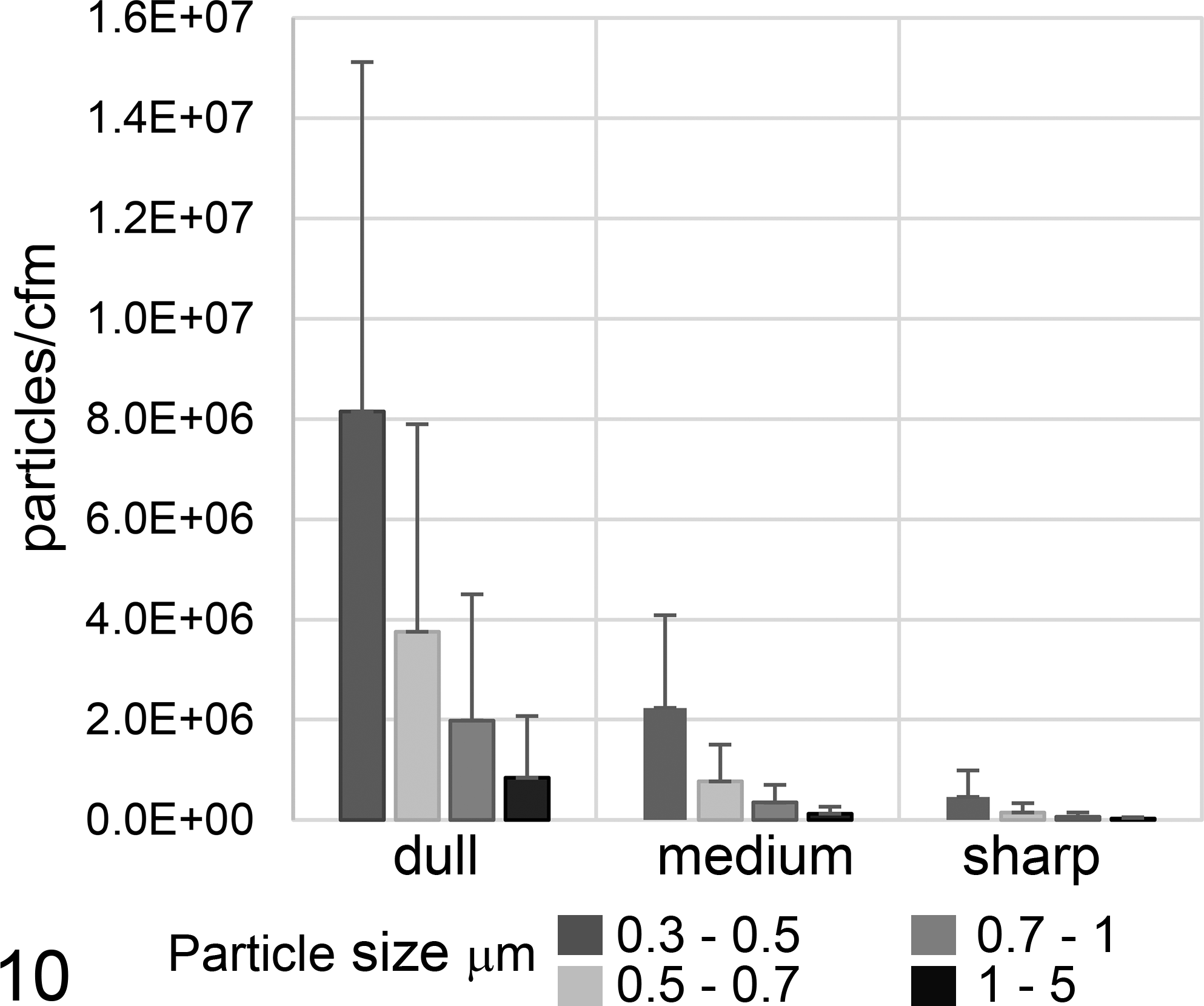
Impact of sharpness of band saw blades on aerosol production. Mean values (bars) and the standard deviations of 20 experiments. Each individual experiment included the mean of the first 4 time points (as determined for Fig. 1) of particle concentrations at the operator position during or after sawing. The differences between dull, medium, and sharp saw blades were significant for all 4 particle sizes shown (P < .005, univariate analysis of variance and Scheffé test). Bones used were bovine humeri or femurs.
Influence of Moistening of the Band Saw Blade
In addition, we tested whether continuous moistening of the band saw blade with running tap water could reduce aerosol production. Sawing with dry saw blades created almost twice as many particles compared with sawing with continuous water supply onto the saw blade (Fig. 11). There was a significant difference (P < .0004) between sawing with and without water supply for all particle sizes from 0.3 μm to 5 μm in diameter.
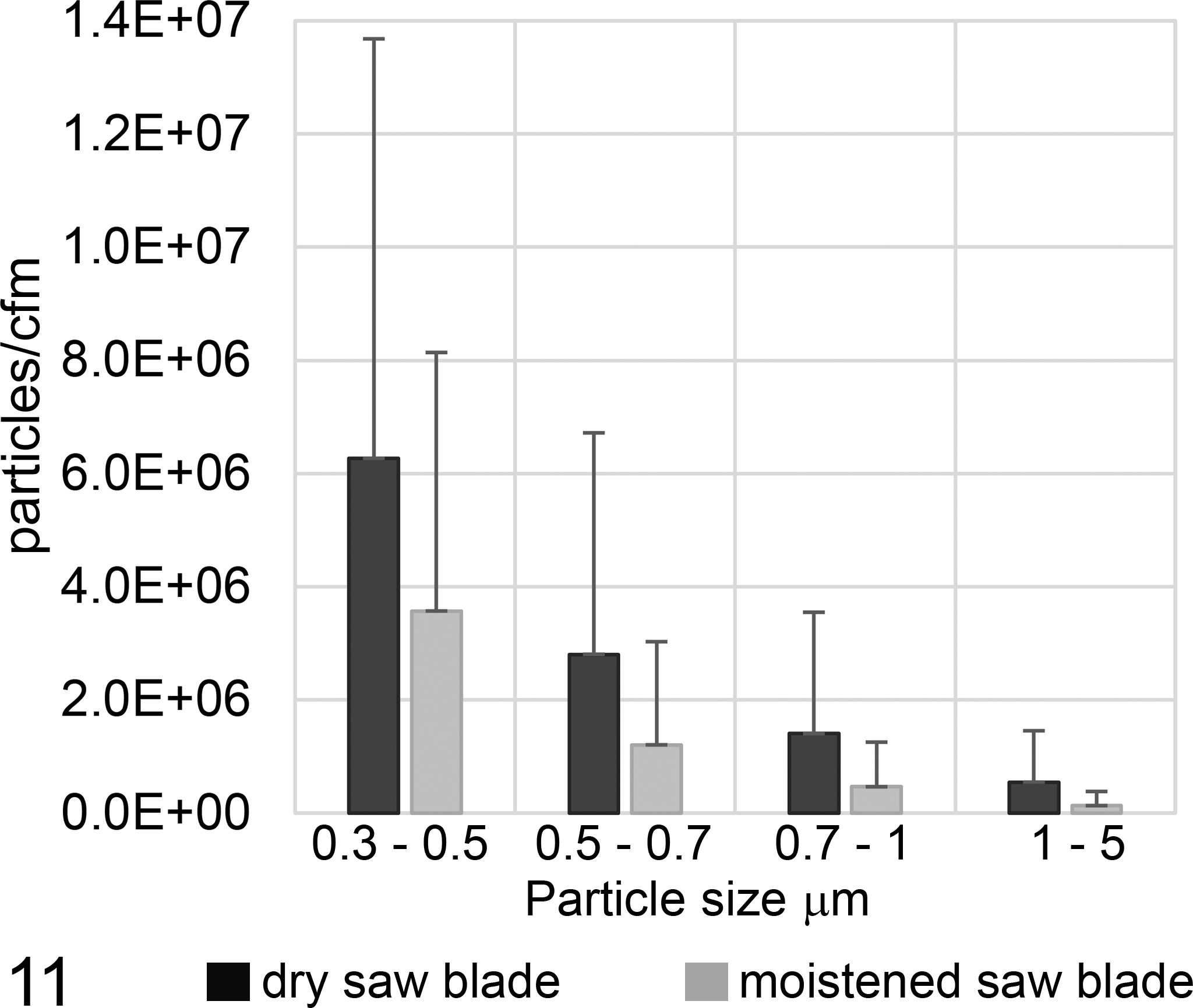
Impact of continuous moistening of the band saw blade on aerosol production. Mean values (bars) and the standard deviations of 10 experiments. Each individual experiment included the mean of the first 8 values of particle concentrations measured at the operator position during/after sawing as determined for Figure 3. The differences between the groups were significant for all 4 particle sizes shown (P < .005, univariate analysis of variance). Bones used were bovine humeri or femurs.
Diamond-Coated Cut Grinder
Aerosols were also produced by the diamond-coated cut grinder (Fig. 12; Suppl. Fig. S2). Nevertheless, in comparison with the standard bone band saw, this cut grinder produced considerably less particles/cfm (Suppl. Fig. S12) upon sawing the same material (swine feet). Aerosolized particles with a size of 1 to 5 μm were reduced by approximately 45%, and smaller particles with a size of 0.3 to 0.5 μm were reduced by approximately 80%. The difference between the 2 devices was significant for all particles with sizes from 0.3 to 5 μm in diameter (P < .004). Concentrations of particles larger than 5 μm and 10 μm were much lower, and we found no evidence of difference (P = .243 and P = .774, data not shown).
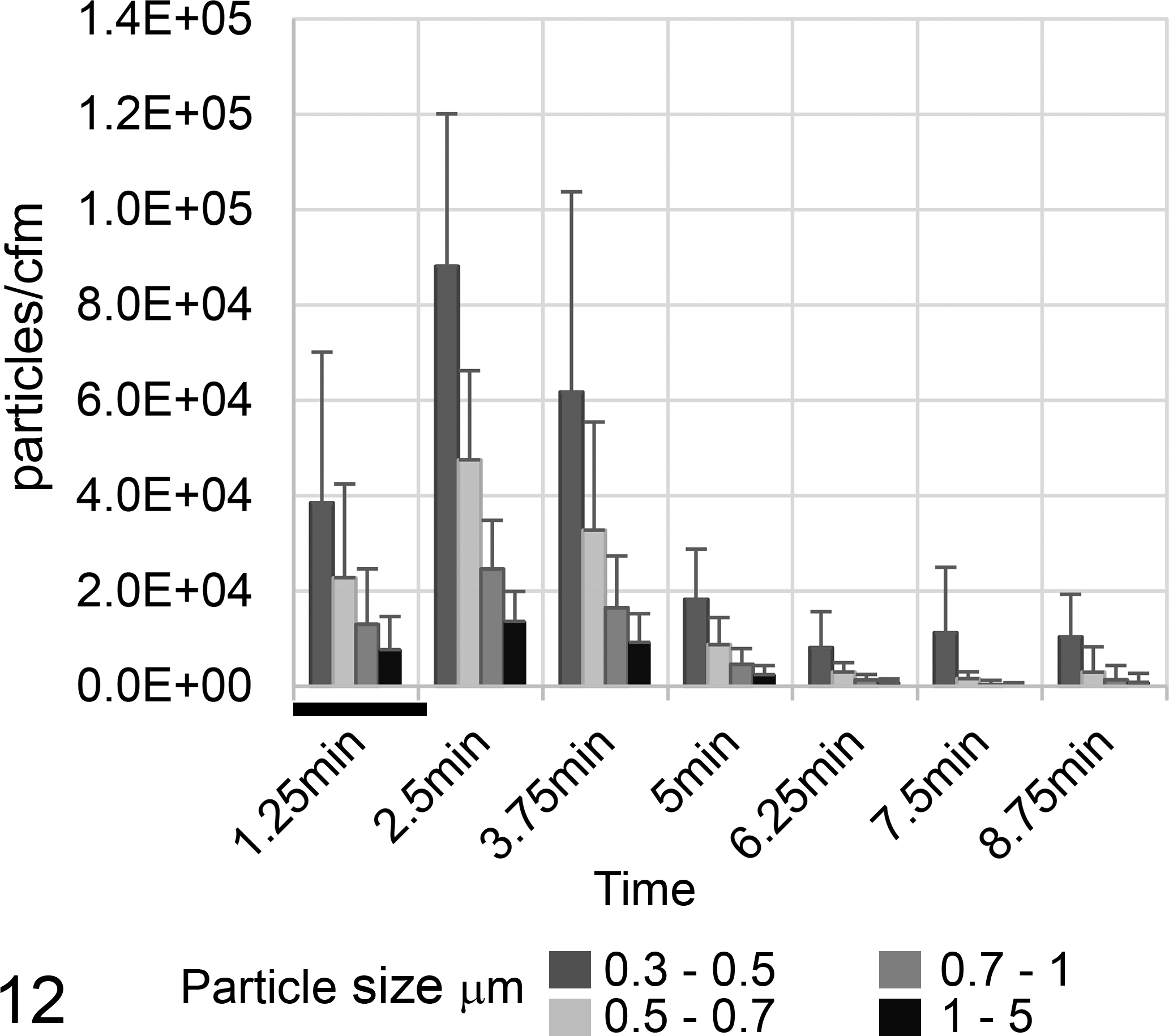
Particle concentrations at the operator position generated by the diamond-coated cut grinder in the sawing cabin. Mean values (bars) and the standard deviations of 10 experiments, grouped according to particle size. Bones used were pig feet. The cut grinder was operated during the first 2 minutes (indicated by a black bar).
Oscillating Autopsy Saw
Using the oscillating saw inside the autopsy hall (before renovation), an increase of particle counts was detected close to the operator only (Suppl. Figs. S4 and S13) and not at positions 2 and 3 (5 and 15 m from the saw, data not shown). Under these conditions, maximum concentrations of 2.2 × 104 particles/cfm (0.3–0.5 μm) were detected 2.5 minutes after the start of the sawing procedure, and values dropped to base levels within 5 minutes. Similar to the observation with the band saw, aerosol concentrations detected upon sawing inside the sawing cabin were higher than inside the autopsy hall (Fig. 13), with a maximum concentration of 7.2 × 104 particles/cfm (0.3–0.5 μm). The concentration of larger particles (0.5–5 μm) increased to a lesser degree (1.2–2.5 × 104 particles/cfm) and concentrations of particles larger than 5 μm only slightly (<4.8 × 102 particles/cfm). The drop to base levels inside the sawing cabin was achieved in approximately 5 minutes.
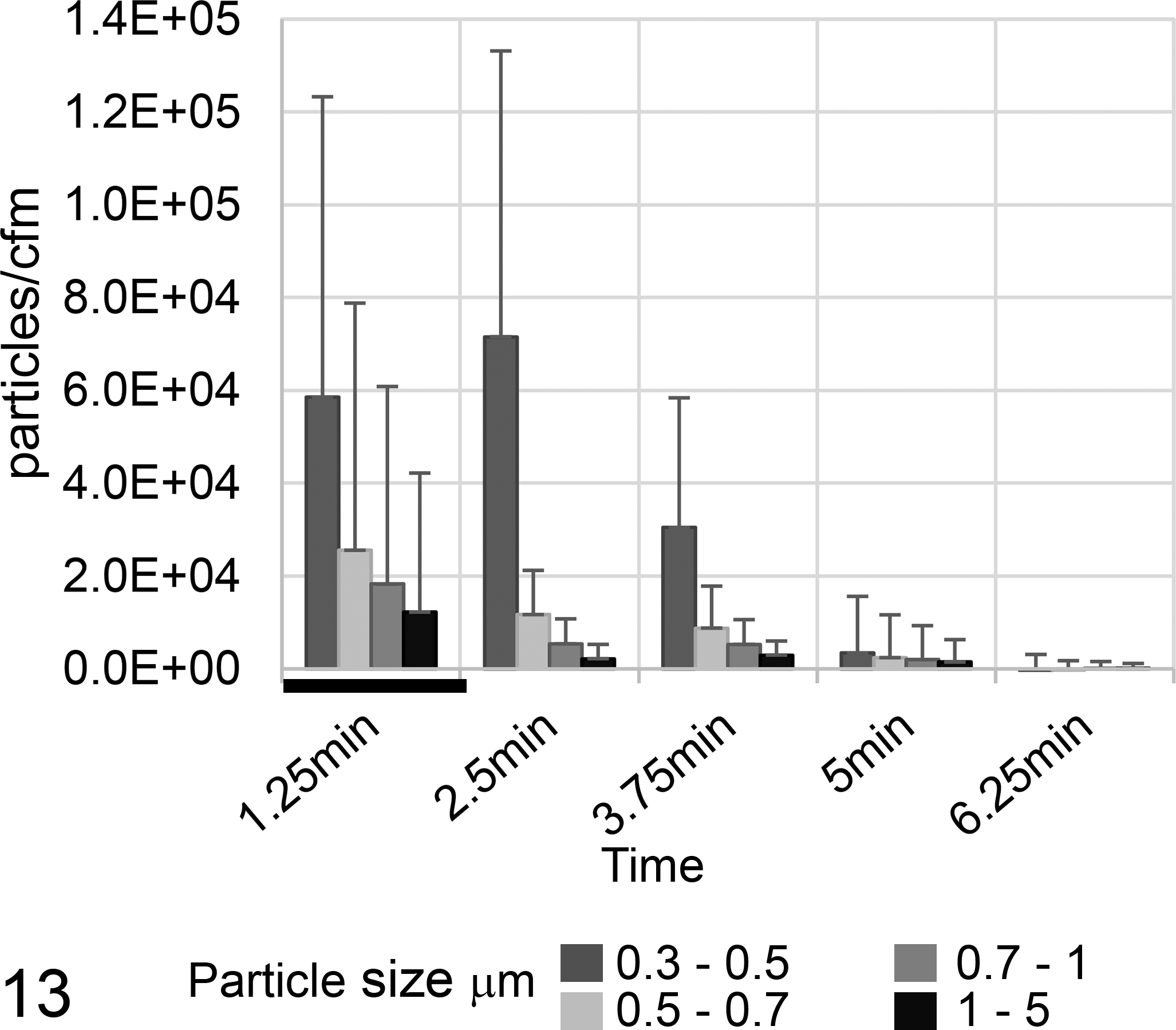
Particle concentrations at the operator position generated by the oscillating autopsy saw in the sawing cabin. Mean values (bars) and the standard deviations of 10 experiments, grouped according to particle size. Bones used were porcine spines. The saw operated during the first 2 minutes (indicated by a black bar).
Reciprocating Saw
Using the reciprocating saw to cut bovine rip cages, aerosolized particles of sizes up to 5 μm in diameter were detected, and a maximum concentration of 5.3 × 104 particles/cfm (0.3–0.5 μm) was reached after 2.5 minutes (Fig. 14 and Suppl. Fig. S5). The concentration of larger particles (0.5–5 μm) was lower (1.9 × 102 particles/cfm for 5–10 μm and 1.5 × 102 particles/cfm for >10 μm, data not shown). Base levels were reached after 5 minutes.
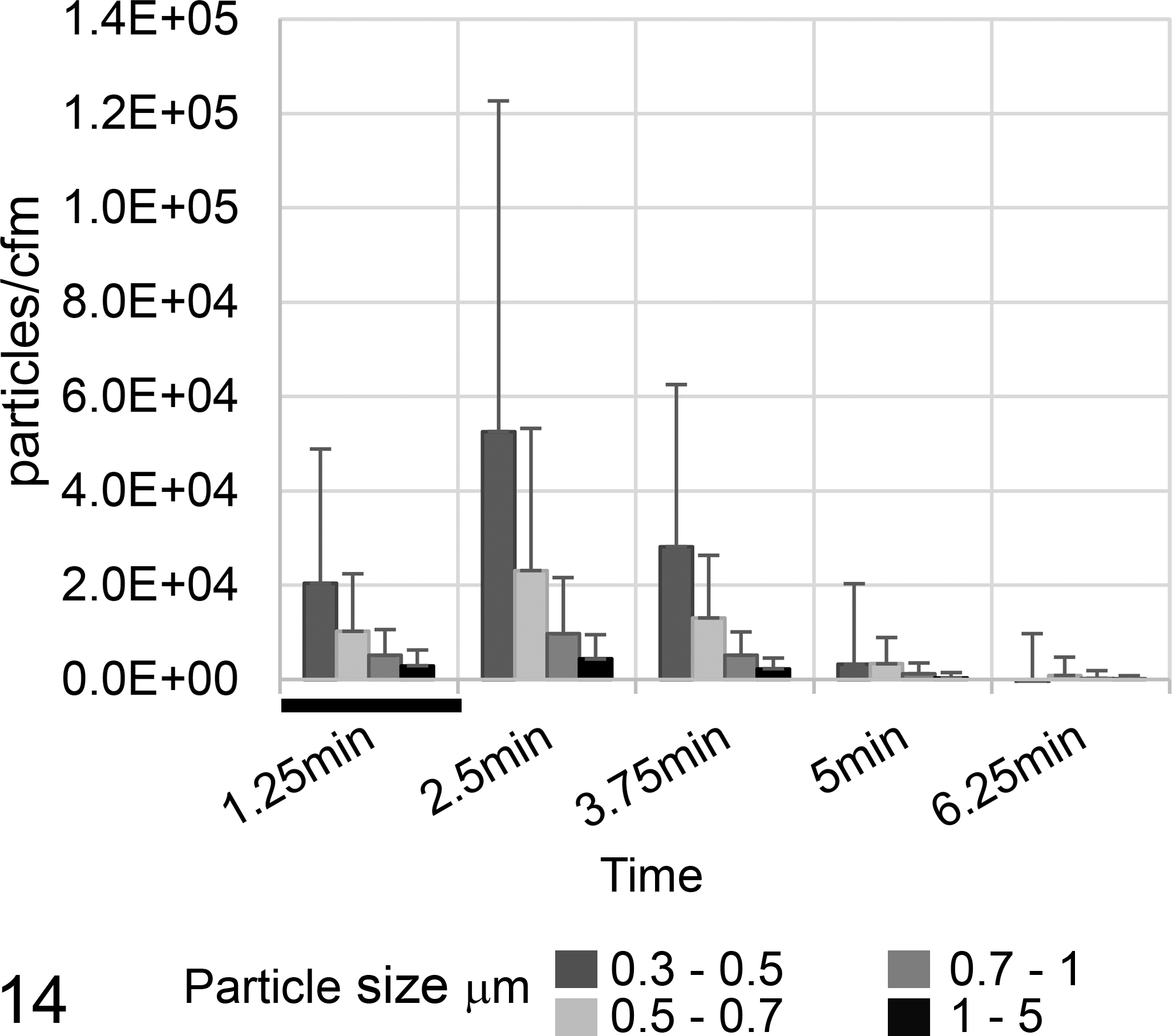
Particle concentrations at the operator position generated by the reciprocating saw. Mean values (bars) and the standard deviations of 11 experiments, grouped according to particle size. Bones used were entire bovine ribcages. The saw was operated during the first 2 minutes (indicated by a black bar).
Handsaw
Upon using the handsaw inside the autopsy hall, only small amounts of aerosolized particles at the position of the operator were detected (Suppl. Figs. 3 and 14). Particles of sizes between 0.5 and 5 μm in diameter were only detected during the first 5 minutes of the sawing procedure. Again, when the sawing was performed inside the cabin, aerosol concentrations were higher, and also particles with sizes 0.3 to 0.5 μm in diameter were detected (Fig. 15). The maximum concentration of 1.8 × 104 particles/cfm (0.3–0.5 μm) was detected after 2.5 minutes, and base levels were reached within 5 minutes. Only few particles with sizes 5 to 10 μm (2.8 × 102 particles/cfm) and >10 μm (2.1 × 102 particles/cfm) were detected (data not shown).
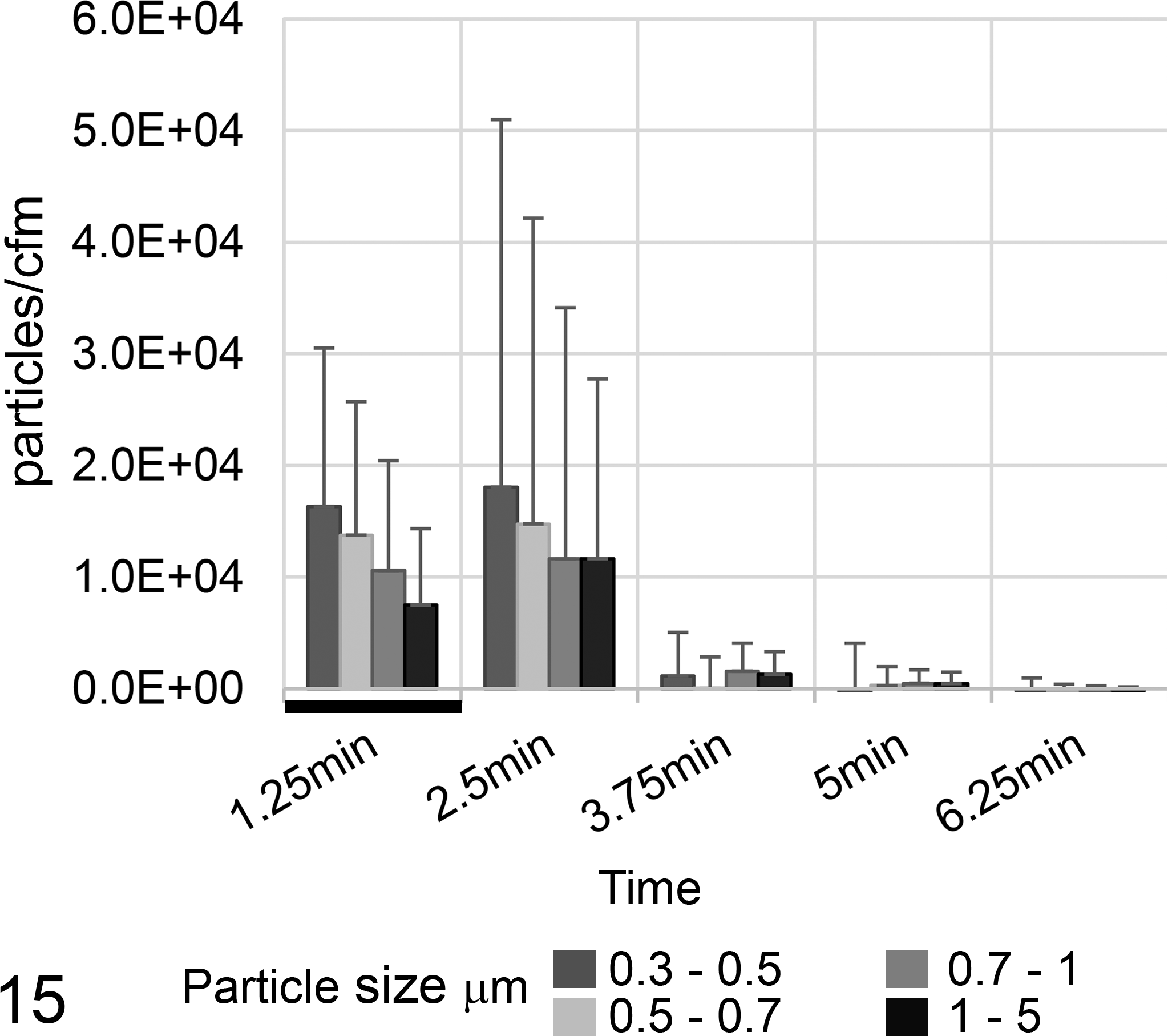
Particle concentrations at the operator position generated by the handsaw in the sawing cabin. Mean values (bars) and the standard deviations of 17 experiments, grouped according to particle size. Bones used were porcine skulls. The saw was operated during the first 2 minutes (indicated by a black bar).
PAPR Test
To test a commercially available PAPR, we used calf bones on the bone band saw inside the sawing cabin. The protocol, however, had to be adapted to calf femurs, as the aerosol concentrations generated during sawings of adult bovine femurs were too high for the TSI Portacount Pro+ Respirator Fit Tester. Using this test, we calculated an overall performance factor of this PAPR of 1.8 × 105 (ie, the concentration of particles inside was 1.8 × 105 times lower than outside of the PAPR).
Discussion
Bone-sawing procedures are frequently performed in veterinary and human autopsies and are therefore a regular source of aerosols in autopsy facilities. In this study, we demonstrate that most of the routine bone-sawing procedures produce aerosols in a range that could represent a health risk for autopsy personnel.
It is known that inhaled particles smaller than 5 μm can reach the lungs and may cause disease. 7,16,20,25 Consequently, in our study, aerosolized particles with sizes of 0.3 to 0.5 μm, 0.5 to 0.7 μm, 0.7 to 1 μm, and 1 to 5 μm are of particular concern. Depending on the type of saw and the size of the bone, peak concentrations of the sum of all particles of 0.3 to 5 µm in diameter ranged from 6.5 × 103 particles/cfm (handsaw in autopsy hall) to 19.6 × 106 particles/cfm (band saw in sawing cabin). Considering an average inhaled air volume of humans under resting conditions of approximately 6 l/min, 11 even at the lowest concentrations of respirable particles measured in our experiments, a nonprotected person would inhale approximately 1.4 × 103 particles per minute (Table 2). Although the majority of particles are presumably noninfectious bone dust, a percentage of those could, in the presence of zoonotic agents in the material being sawed, be infectious. Importantly, aerosol concentrations generated by saws cannot be predicted exactly as bone sizes and densities between autopsies vary considerably. Hence, concentrations of aerosolized infectious agents can vary and are unpredictable under most conditions present in routine autopsy facilities. Our results show that the minimal infectious dose for many zoonotic agents (Table 1) can potentially be inhaled during all investigated sawing procedures.
Calculated Particle Inhalation by Autopsy Personnel.
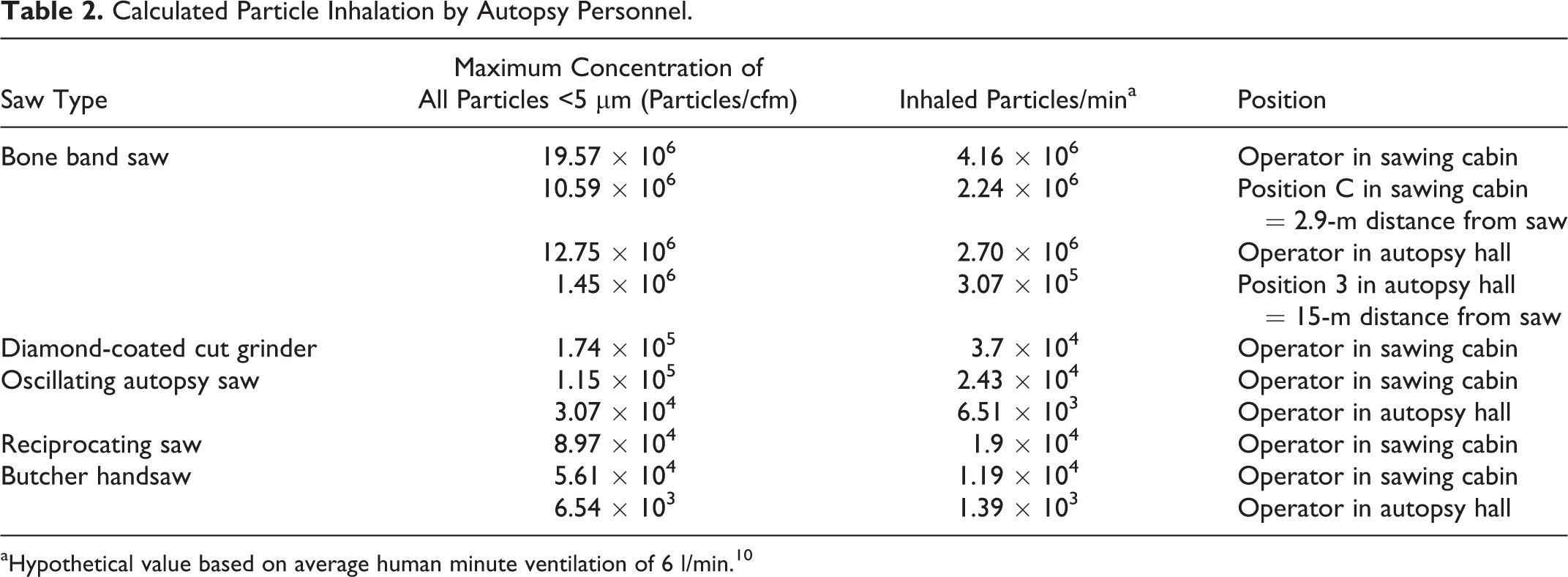
aHypothetical value based on average human minute ventilation of 6 l/min. 10
Our results clearly demonstrate that the bone band saw, a device that is regularly used in veterinary and human pathology, produces vast amounts of respirable aersolized particles (Suppl. Fig. S15). This confirms previous results by Saternus and Kernbach-Wighton, 25 who demonstrated considerable aerosol production by a bone band saw when cutting human skulls and cervical vertebral spines. Most important, under the circumstances in our autopsy hall, these aerosols distributed throughout the entire room and remained in the air for up to 1 hour despite the regular operation of our ventilation system. This unequivocally led to an exposure of all personnel in the autopsy hall. Even at a distance of 15 m from the band saw, we calculated a maximum inhalation of approximately 3 × 106 particles of less than 5 μm per minute (Table 2). Considering that aerosolized particles smaller than 5 μm have settling times of 60 minutes and longer, 29 this represents a considerable health risk for all personnel inside the room where infectious agents become aerosolized.
This spread was certainly influenced by an insufficient air exchange inside our autopsy hall and by downward-directed air turbulences caused by an inflow of cold air from the adjacent cool room, which, however, was technically not avoidable in our case. This situation might be less critical in other facilities in which the ventilation system could be better designed. Nevertheless, it has to be taken into account that our measurements were performed in an empty autopsy hall because movements of personnel and opening of doors disturbed the airflow. Properly designed ventilation systems have to take these massive and partly unpredictable disturbances in airflow into account to avoid the problem of spreading aerosols during regular working times.
In addition, we demonstrated that moistening of the saw blade leads to a significant reduction of aerosolized particles, although the overall amount was still very high and moistening alone is not sufficient for the protection of personnel against aerosols.
Not surprisingly, the sharpness of the saw blade had a significant effect on the amount of aerosol generated. However, it has to be considered that under practical conditions, saw blades will mostly be used until the main operator notices difficulties in cutting through bones (ie, until the stage where they were categorized as dull in our experiments). This will unequivocally result in large fluctuations of aerosol amounts between sawing procedures, and massive aerosol production at some stage can be expected.
Because complete renovation or reconstruction of the entire autopsy hall was not an option in our situation, we constructed a sawing cabin with a dedicated exhaust fan inside the existing autopsy hall. Even with the improved air exchange rate in this cabin, contamination of the entire sawing cabin with massive amounts of aerosols could not be avoided when the band saw was used to cut bones. Due to the smaller volume of the cabin, peak aerosol concentrations using all saws were even higher compared with the large-volume autopsy hall. Ideally, the air exhaust should have been located above the saw to reduce this problem, but due to the plan of placing several saws inside the cabin and the technical limitations imposed by the existing building, the exhaust was placed centrally. Due to the higher air change rate, particle concentrations dropped back to base levels much faster than in the autopsy hall. If used properly, with closed door and thus not impeding the airflow, contamination of the surrounding area during and after sawing was eliminated. However, if the door was left open, small particles (0.3–0.7 µm) still reached the surrounding autopsy hall, and thus personnel present outside the sawing cabin were potentially exposed to aerosols. Therefore, our results clearly demonstrate the need for properly designed and properly verified ventilation systems and the usefulness of well-separated areas for sawing procedures in autopsy facilities. For new buildings, these considerations should be included into the design of the facility. However, most pathology units will face a similar situation like ours, in which an old, preexisting building with suboptimal design and ventilation has to be retrofitted to limit work hazards for employees and students. Potentially hazardous activities, such as bone sawing, could be segregated from other routine procedures through constructions like separate rooms, sawing cabins, or ventilated tents.
It is important to note that sawing inside a separately ventilated room only protects persons outside this room, not the operator himself or herself. Regardless of the type of saw used, the operator is still exposed to aerosols. Consequently, personnel inside the cabin have to be protected against these aerosols. Many different systems are commercially available. 3 Pauli et al 22 demonstrated that the choice of the correct system is crucial. Many commercially available FFP3 respirators provide only partial protection, because they do not fit every person and only properly performed fit tests for each individual person would provide sufficient information of the degree of protection. Nevertheless, the fit factors published by Pauli et al 22 would, in case of bone dust generated by electrical power saws, be largely inefficient. In our experiments, a commercially available PAPR provided very good protective levels, demonstrated by a high performance factor. The use of such respirator systems as PPE for saw operators and personnel exposed to potentially infectious aerosols in combination with technical measures, such as moistening the saw blades and an airflow directed away from the operator, is therefore highly recommended.
While the bone band saw is usually applied for opening large bones, it is impractical or dangerous for smaller bones or particular bones (thorax, spine, skull). We therefore tested other regularly used devices for cutting bone. A diamond-coated cut grinder, which operates with constant moistening of the grinding blade to reduce heat excess while slicing bone, produced significantly less aerosol than the bone band saw. Nevertheless, particle counts, especially of respirable particles of less than 5 µm in diameter, were still high. Because of the grinding technique, which produces less artifacts or damage than sawing, and the improved safety for the operator, this equipment represents a very useful addition to an autopsy service. Grinding bone, however, is more time-consuming, and currently available models are mainly limited to small- or medium-sized bones.
Under conditions resembling routine use, the oscillating autopsy saw, the reciprocating saw, and the handsaw generated smaller amounts of aerosolized particles than the bone band saw. Nevertheless, concentrations of respirable particles were still remarkably high (Table 2). Reports by Posthaus et al 23 and Templeton et al 30 have previously shown that aerosols generated by the oscillating autopsy saws are a potential source of infection for humans, suggesting that the concentrations detected during our experiments should be considered a health risk for pathologists. The accidental infection of personnel described by Posthaus et al 23 took place in our autopsy hall while opening a dog skull under conditions similar to those tested in our study. When porcine spinal columns are sawed, we calculated a hypothetical value of approximately 6.5 × 103 to 2.4 × 104 inhaled particles per minute (Table 2) for an unprotected operator of an oscillating saw. Such concentrations should be considered a potential health risk when such bone contains infectious material. Using a handsaw certainly represents the lowest risk concerning aerosol production, and this finding correlates well with studies from human pathology. 14,32 The disadvantages of using a manual handsaw are the fact that it is physically more demanding and more time-consuming.
Conclusions
In conclusion, our results clearly demonstrate that different bone-sawing procedures applied in veterinary and human pathology produce aerosols that are of concern for the health of autopsy personnel. To reduce the risk of accidental infections by aerosolized infectious agents, appropriate measures should be implemented in autopsy facilities. These include (a) efficient and properly designed ventilation systems to limit the spread of aerosols throughout entire autopsy rooms, (b) distinct segregated areas where sawing activities are performed, (c) the choice of the proper saw according to a realistic risk assessment, and (d) adequate personal protective equipment for the operator in form of highly efficient PAPRs.
Footnotes
Acknowledgements
We thank Hansruedi Kaeser for technical support, Dr Conrad von Schubert for photographs, and Dr Kerry Woods for language corrections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.