
Abstract
A 13-year-old female Persian cat died suddenly after severe respiratory distress. At necropsy, the changes were compatible with congestive heart failure. The heart was enlarged with a flabby and puckered sac-like aneurysm at the apex of the left ventricle. The apical zone showed a thin muscular wall arising from the free wall of the left ventricle connected to a bulged saccular area through a wide communication. Microscopically, the wall of the aneurysm was composed of fibrous connective tissue with neovascularization and sparse atrophied myocardial cells at the margins. A few isolated cardiomyocytes in the lesion stained positively for desmin, and the inner lining of the aneurysm had immunoreactivity to von Willebrand factor and CD31. Mature fibrous connective tissue was interspersed with degenerated and disorganized cardiomyocytes elsewhere in the myocardium, and many small myocardial arteries were tortuous and thickened. In this case of sudden death, the diagnosis was primary cardiomyopathy, with formation of a left ventricular apical aneurysm within an area of marked myocardial fibrosis and cardiomyocyte atrophy.
Primary cardiomyopathy is a term restricted to cases in which there is no clear cause of the heart failure or the changes in myocardium. 3 Originally identified in humans, cardiomyopathies constitute a heterogeneous but well-characterized group of pathological conditions in cats. 3 Primary cardiomyopathies are inherent while secondary cardiomyopathy refer to specific causes such as hypothyroidism, hypersomatotropism, systemic hypertension, and aortic stenosis, among others. 3 Four main primary cardiomyopathies are recognized: dilated or congestive, hypertrophic, restrictive, and arrhythmogenic right ventricular cardiomyopathy (ARVC). 3 The unclassified cardiomyopathy group includes cases that do not easily fit in one of the previous groups. 3 The commonest type of cardiomyopathy in cats is hypertrophic cardiomyopathy (HCM). 3,8 HCM is a continuum that may eventually lead to an end-stage lesion (ES-HCM). 2,3,8,10 This condition parallels ES-HCM in humans, and left ventricular apical aneurysm occurs in a subset of humans with ES-HCM. 2,8,9 Similarly, cats and humans with ARVC may develop right ventricular apical aneurysms. 4
The aim of this report is to describe the gross and histological findings in a case of sudden death in a cat with left ventricular apical aneurysm as a result of primary cardiomyopathy.
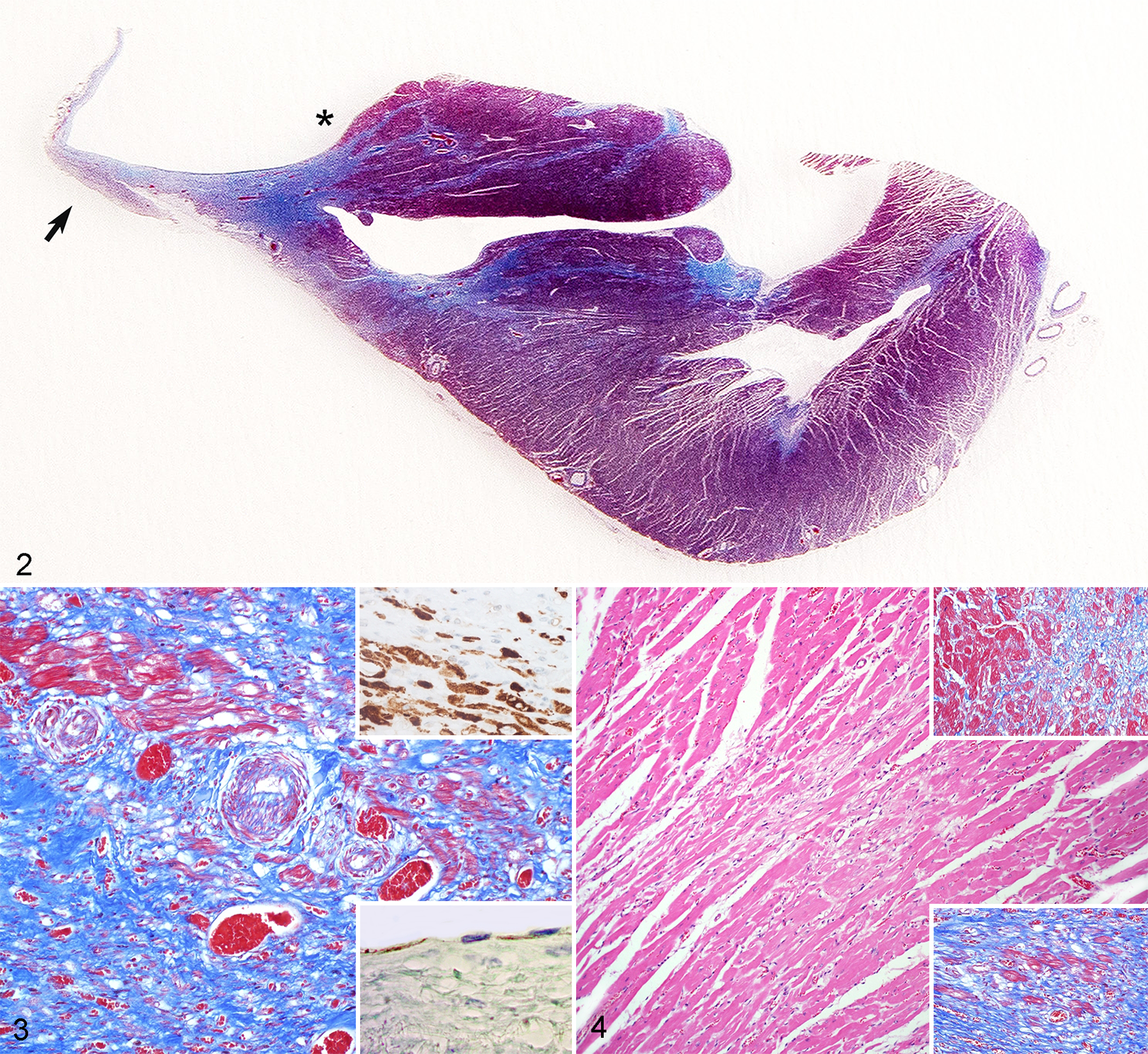
A 13-year-old Persian female cat had received routine grooming and returned home normally. However, 2 hours later, the owner noted sudden respiratory distress and frantic behavior. The cat was taken to the veterinarian but collapsed and died before receiving attention. Hydrothorax, hydropericardium, and edematous, noncollapsed lungs were noted at necropsy. The heart was enlarged with a flabby and puckered small sac (1 cm) at the apex of the left ventricle (Fig. 1). The apical zone had a pale and thin muscular wall arising from the free wall of the apex connected to a bulged saccular area through a wide communication (Fig. 2). Other changes included acute hepatic congestion and mild ascites.
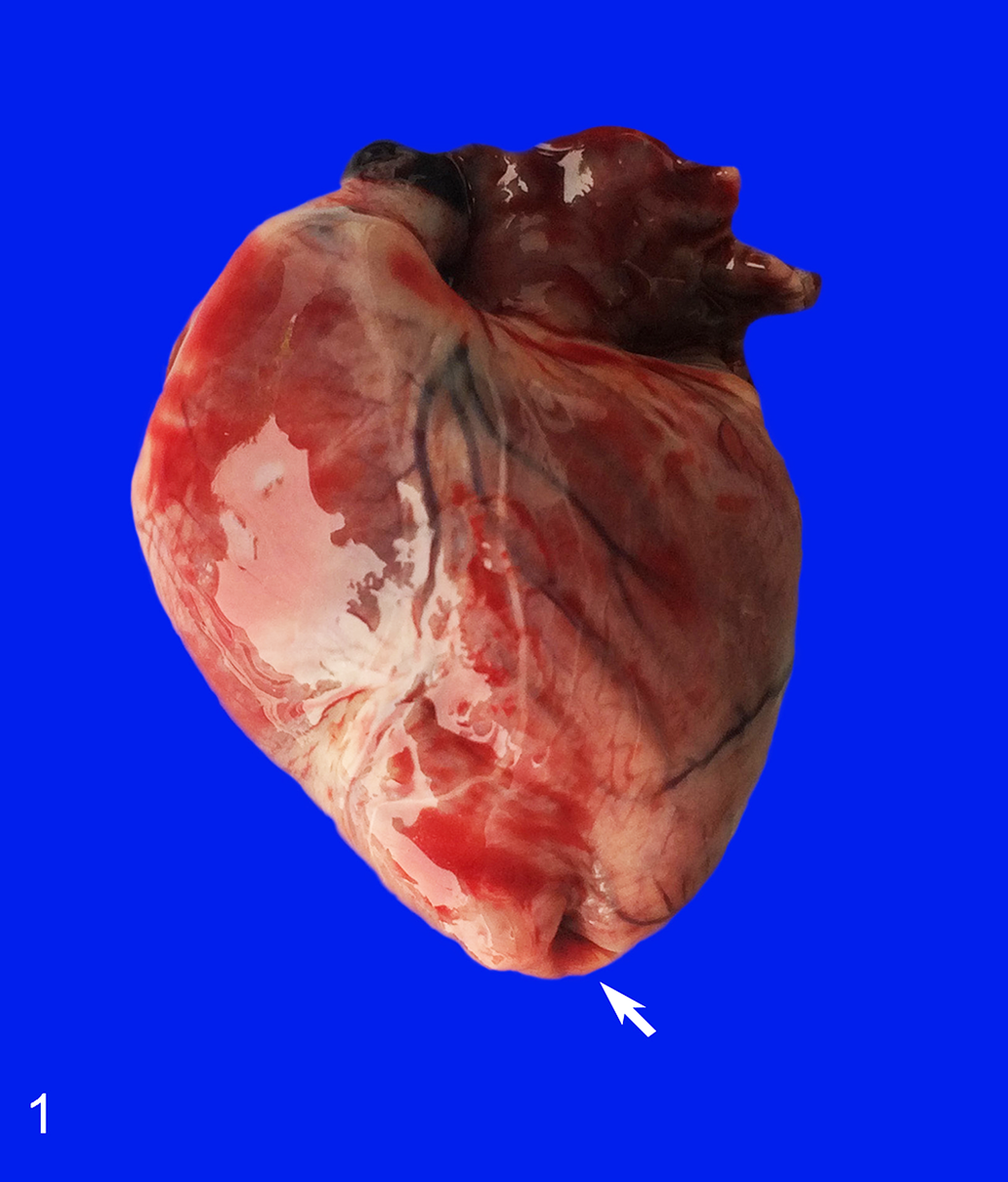
Primary cardiomyopathy with left ventricular aneurysm, heart, Persian cat. The heart is rounded with left atrial enlargement. The apex has a puckered and invaginated sac (arrow) and pallor of the myocardium.
Samples of the heart, lung, liver, spleen, and kidney were fixed in 10% neutral buffered formalin and processed routinely to obtain sections stained with hematoxylin and eosin and with Masson’s trichrome. Additional heart sections were labeled by immunohistochemistry using an avidin-biotin-peroxidase method (Autostainer Link 48; Agilent Technologies, Dako, Carpinteria, CA) using monoclonal antibodies against desmin, vimentin, α–smooth muscle actin, von Willebrand factor, and CD31 (Dako, Comercial Biomédico JR, México). The chromogen was diaminobenzidine, and the counterstain was Harris’s hematoxylin.
Microscopically, the paucity of the myocardium in the saccular wall of the left ventricle was obvious. In the left ventricle, near the sacculus, the small arteries were tortuous and thickened due to proliferation of the endothelium and hypertrophy of the tunica media (Fig. 3). No Purkinje fibers were recognized, and few infiltrating lymphocytes were noted. Furthermore, there were several foci of myocardial ischemic necrosis and occasionally large areas with scarring, suggesting previous infarcts (Fig. 4, upper inset). The saccular lesion was composed of abundant fibrous connective tissue, sparse and atrophied cardiomyocytes, and neovascularization (Fig. 4, lower inset). Sections of liver and lung confirmed acute centrilobular congestion and alveolar edema with numerous hypertrophied macrophages, respectively.
By immunohistochemistry, there was strong staining for desmin in isolated cardiomyocytes in the lesion (Fig. 3, upper inset) and in the remaining myocardium. The immunoreactivity to vimentin was moderate and was encountered in the fibrous connective tissue in the lesion but not in the cardiomyocytes. α–Smooth muscle actin staining was markedly positive in the walls of the new vessels and in vessels in the remaining myocardium. Finally, the cells lining the inner surface of the sacculus were positive for von Willebrand factor (factor VIII) and CD31 (Fig. 3, lower inset) similar to the endocardial lining.
In the remaining portions of the left ventricle and in the papillary muscles, fibrous connective tissue was interspersed with degenerated cardiomyocytes. The cardiomyocytes were hypertrophied or atrophied with hyaline, fragmented, hypereosinophilic, and densely staining cytoplasm; in some areas, the cardiomyocytes appeared disorganized with fibrous connective tissue interspersed (Fig. 4). The diagnosis was severe left ventricular fibrosis and myocardial atrophy with left ventricular apical aneurysm.
Protruding structures in the ventricles are extremely rare in animals and humans. Apical aneurysms in the right ventricle have been described in cats with ARVC. 4 Also, an aneurysm on the right ventricular free wall was encountered in a cat with a large atrial septal defect. 1 Recently, a congenital aneurysm in the right ventricle was reported in a pigeon 5 and a case of diverticula in both ventricles in a dog. 6 However, to our knowledge, left ventricular apical aneurysm has not been previously described in animals.
Ventricular diverticula, left ventricular apical aneurysm, and ventricular pseudo-aneurysm are well-characterized conditions in humans. 6,7 Although sometimes used interchangeably, cardiac diverticulum and aneurysm are different. 6,7 In humans, left ventricular aneurysm may be congenital or acquired. Congenital aneurysms are rare and are characterized by a wide channel of communication with the apical left ventricle and a limiting wall composed of a single layer of fibroelastic tissue that is sometimes calcified and lacks ventricular muscle. The anomaly is isolated and originates due to structural errors during embryogenesis. The condition is diagnosed after the exclusion of other pathologic changes. 7 Conversely, a left ventricular diverticulum is commonly associated with other cardiac anomalies and midline thoracoabdominal malformations. 7 In the case of a cardiac diverticulum, a thin layer containing endocardium, myocardium, and pericardium maintains contractility, whereas with an aneurysm, the fibrous tissue exhibits systolic dyskinesia/akinesia or paradoxical bulging. 7 However, left ventricular aneurysm may be acquired, in which case the most plausible origin is a myocardial infarct, with replacement by fibrous tissue. 6,7,9 The apical location is attributed to the thinness of the myocardium at this site. Systemic causes of acquired left ventricular apical aneurysm in humans include Chagas disease, mucopolysaccharidosis, and sarcoidosis, among others. 7 Ventricular pseudo-aneurysm (also called false aneurysm) is a similar condition but represents a rupture of the ventricular wall that is contained by adhesion of the pericardium. 7
The lesion encountered herein differs in several ways from those previously described in animals. In the cats with ARVC, the lesion occurs only in the free wall of the right ventricle. 4 Similarly, the right ventricular aneurysm reported in a cat was likely a consequence of a large atrial septal defect. 1 Conversely, in the dog, several lesions occurred in both ventricles, but not in the apex, and these had a narrow ventricular communication in contrast with the wide passage in our case. 6 Finally, the apical lesion in this cat was accompanied by the presence of disorganized cardiomyocytes in the myocardium as well occluding changes in the small arteries, which are evidence of primary cardiomyopathy. 2,3,8 Based on the absence of left ventricular hypertrophy, we considered ES-HCM, restrictive cardiomyopathy, and unclassified cardiomyopathy as possible differential diagnoses in this case, and cardiac ultrasound would be necessary to distinguish these possibilities. 3,10 There was also atrophy and scarring of the left ventricle adjacent to the aneurysm, suggesting these more severe localized myocardial changes as the cause for development of aneurysm. We suggest that these lesions may have arisen from a myocardial infarct.
This report describes a left ventricular aneurysm in a cat with primary cardiomyopathy that is considered to be an acquired lesion resulting from a localized area of myofiber atrophy and replacement fibrosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: C. Ramírez-Hernández received a graduate studies scholarship from CONACYT.