
Abstract
Autopsy of animals that die in the perianesthetic period allows identification of anesthetic and surgical complications as well as preexisting disease conditions that may have contributed to mortality. In most studies to date investigating perianesthetic mortality in animals, inclusion of autopsy data is very limited. This retrospective study evaluated autopsy findings in 221 cases of perianesthetic death submitted to a veterinary diagnostic laboratory from primary care and referral hospitals. Canine (n = 105; 48%) and feline (n = 90; 41%) cases predominated in the study, involving elective (71%) and emergency (19%) procedures. The clinical history provided to the pathologist was considered incomplete in 42 of 221 cases (19%), but this history was considered essential for evaluating the circumstances of perianesthetic death. Disease had been recognized clinically in 69 of 221 animals (31%). Death occurred in the premedication or sedation (n = 19; 9%), induction (n = 22; 11%), or maintenance (n = 73; 35%) phases or in the 24 hours postanesthesia (n = 93 animals; 45%). Lesions indicative of significant natural disease were present in 130 of 221 animals (59%), mainly involving the heart, upper respiratory tract, or lungs. Surgical or anesthesia-associated complications were identified in 10 of 221 cases (5%). No lesions were evident in 80 of 221 animals (36%), the majority of which were young, healthy, and undergoing elective surgical procedures. Lesions resulting from cardiopulmonary resuscitation were identified in 75 of 221 animals (34%). Investigation of perianesthetic death cases should be done with knowledge of prior clinical findings and antemortem surgical and medical procedures; the autopsy should particularly focus on the cardiovascular and respiratory system, including techniques to identify pneumothorax and venous air embolism.
Keywords
Animals that die while sedated or anesthetized contribute to a relatively small but important number of cases submitted for autopsy to veterinary diagnostic laboratories. These cases are stressful and emotional for both veterinarians and animal owners and may potentially involve litigation or disciplinary action by the veterinary licensing body.
There has been a trend over time toward a decrease in the rate of anesthesia-associated mortality among veterinary patients. 4 –6,8 This reduction is attributed to improvement in both anesthetic drugs and protocols, as well as implementation of progressively more advanced monitoring procedures. Retrospective studies from various geographic regions, and including both referral institutions and general practices, have identified variable overall rates of perianesthetic mortality in animals, ranging from 0.11% to 1.5% in dogs, 0.06% to 1.08% in cats, 1.39% in rabbits, 0.33% in ferrets, and 0.12% to 1.6% in horses. 2 –4,6,8,10,12,13,18,19 In contrast, a recent North American study of human patients identified an anesthesia-associated mortality rate of 0.033%. 30
Autopsy of animals that die in the perianesthetic period allows identification of anesthetic and surgical complications as well as preexisting disease conditions (either related or unrelated to the surgical or medical procedure) that may have contributed to mortality. In some situations, iatrogenic contribution to death may also be identified, as in cases of clinically undetected postsurgical hemorrhage. In one study evaluating the role of autopsy in human anesthesia malpractice claims, a significant nonanesthestic contribution to death was identified in 61% of cases. 15 However, in most studies to date investigating perianesthetic mortality in animals, conclusions are based on clinical information and expert review, and inclusion of autopsy data is very limited. 2 –4,6,8,10,12,13 One study found that autopsy was pursued only in approximately 10% of perianesthetic mortality cases. 4 A recent study provides the most comprehensive information to date regarding morphologic lesions in such cases and was limited to cats dying during or after general anesthesia for uncomplicated sterilization procedures. 9 In addition to the paucity of published reports of autopsy findings related to perianesthetic death in animals, resources addressing specific autopsy protocols and techniques for these cases are limited mainly to human pathology references. 7,9,14,28,29
This retrospective study evaluated cases of perianesthetic mortality in domestic animals submitted for autopsy to a veterinary diagnostic laboratory over an 8-year period. Special considerations for autopsy of perianesthetic mortality cases are also discussed, based on these results and a review of the existing literature.
Materials and Methods
Perianesthetic mortality cases submitted to the University of Guelph Animal Health Laboratory (AHL) from May 1, 2007 to July 31, 2015 were identified retrospectively. Autopsy records were searched in the laboratory’s information management system (LIMS; Sapphire, LabVantage Solutions Inc, Somerset, NJ, USA) using anesthesia-related etiology codes assigned by the coordinating pathologist for each case, as well as by a free-text search for the terms cardiopulmonary resuscitation (CPR), anesthesia, cardiac arrest, and respiratory arrest. Inclusion in the study was limited to cases in which death occurred within 24 hours of sedation or premedication for general anesthesia, or for sedation alone, and for which gross autopsy was carried out at the AHL. Cases for which the autopsy was conducted at another clinic or institution, and for which only histopathology samples were submitted to the AHL for examination, were excluded. Those cases for which death occurred >24 hours after general anesthesia or sedation were also excluded.
Data captured for each case from the LIMS search included the species, breed, age, and sex of the animal; clinical history as provided by the submitting veterinarian; and pathology diagnoses. Individual case reports were reviewed by the author and additional information was recorded based on both objective and subjective information included in the clinical history and pathology report, including pathologists’ comments and interpretation. Based on this review, additional data recorded for each case included autopsy lesion(s) interpreted by the case pathologist as most clinically relevant to the animal’s death and the category of these lesions (ie, cardiovascular, respiratory, neurologic, gastrointestinal, systemic, or neoplastic disease; lesions directly resulting from surgical or anesthetic complication; or no significant lesions), phase of sedation or general anesthesia during which death occurred (premedication or sedation, induction, maintenance, postanesthetic recovery), clinical description provided for anesthetic complication (cardiac and/or respiratory arrest, collapse, found dead, hypotension), type of surgery (elective vs emergency, and specific procedure), and history of CPR. Comments relating to clinically recognized anesthetic or surgical complications, as well as lesions interpreted by individual pathologists as potentially associated with CPR, were also recorded when this information was included in the clinical history or postmortem report, respectively.
Results
A total of 17,417 autopsy cases were submitted to the AHL between May 1, 2007 and July 31, 2015. The initial LIMS search using anesthesia-related etiology codes and free-text terms identified a subset of 608 potential perianesthetic mortality cases. Of these, 221 cases met the inclusion criteria for the study, representing 1.3% of all autopsy cases during this time. These consisted of 174 cases originating from primary care veterinary hospitals and 47 cases from veterinary referral hospitals. Cases of dogs (n = 105) and cats (n = 90) predominated, with fewer cases of other species including horses (n = 9), rabbits (n = 9), ferrets (n = 4), and a guinea pig, chinchilla, rat, and tortoise (n = 1 each). The proportion of cases from each species in the study compared with the total number of autopsy cases for the same species during this time period is shown in Supplemental Table S1. A total of 34 pathologists and pathology trainees contributed to the 221 cases in the study.
Clinical history as provided by the submitting veterinarian was considered incomplete in 42 of 221 cases (19%), based on lack of information concerning the clinical status of the animal at the time of surgery; the specific procedure being done for which sedation or anesthesia was required; when during the procedure and under what circumstances the animal died; and whether CPR was performed on the animal. Both referral institutions (11 of 42; 26%) and primary care veterinary facilities (31 of 42; 74%) contributed to the cases with incomplete historical information. A total of 69 animals (31%) had evidence of clinical disease prior to anesthesia, based on clinical histories provided by veterinarians. The presurgical health status of the animal, using American Society of Anesthesia (ASA) guidelines, 5 was included in the clinical history for only a single animal in the study. Of the total 221 cases, 158 animals (71%) were sedated or anesthetized for elective procedures; emergency procedures were carried out in 42 animals (19%), and the procedure was unknown based on the history provided for 21 animals (10%).
Both gross and histologic examinations were carried out for the majority of cases (218 of 221; 99%); evaluation was limited to gross examination for 3 cases. For 2 cases, partial or complete gross examination had been conducted by a veterinarian prior to submission of the body to the diagnostic laboratory. Timing of death was unknown for 14 cases (6%). Of the 207 cases in which the timing was specified, death occurred in the premedication or sedation (n = 19; 9%), induction (n = 22; 11%), or maintenance (n = 73; 35%) phases or in the 24 hours postanesthesia (n = 93; 45%).
A summary of autopsy findings is listed in Table 1. Among all species, 81 animals (37%) lacked lesions that reflected the cause of death (COD) or a contributing COD. No significant lesions were identified in 4 of 9 rabbits (44%), 45 of 105 dogs (43%), 31 of 90 cats (34%), and the single tortoise in the study. The median age of animals with no significant postmortem lesions was <1 year in each of these species (dogs: 9 months [range, 3 months to 19 years]; cats: 7 months [range, 2 months to 13 years]; and rabbits: 6 months [range, 3 months to 9.5 years]). The majority of animals in which no lesions were identified had undergone elective procedures (4 of 4 rabbits [100%]; 25 of 45 dogs [56%]; and 26 of 31 cats [84%]), including spay or neuter surgeries in 25 of 45 dogs (56%) and 18 of 31 cats (58%). The balance of cases included emergency surgeries and cases for which the procedure was not documented in the clinical history provided by the submitting veterinarian or in the autopsy report.
Autopsy Lesions in Perianesthetic Mortality Cases at a Veterinary Diagnostic Laboratory.a
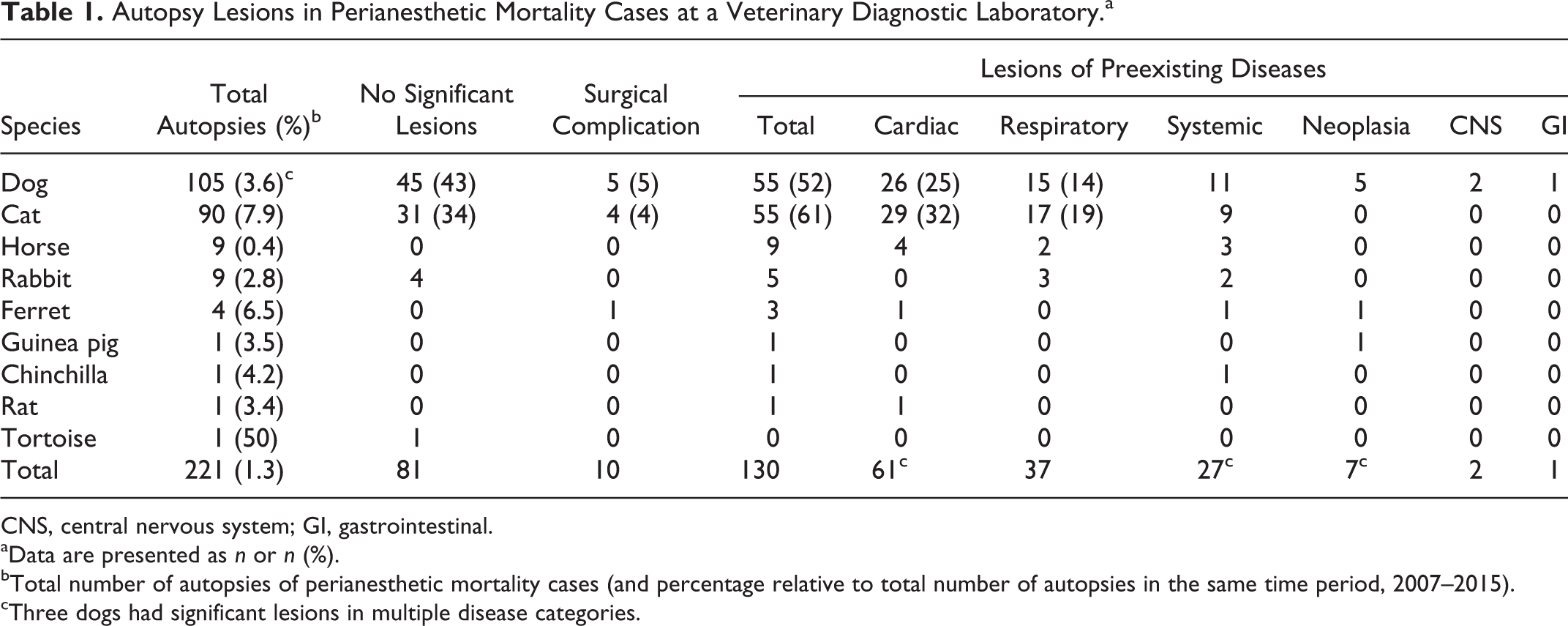
CNS, central nervous system; GI, gastrointestinal.
aData are presented as n or n (%).
bTotal number of autopsies of perianesthetic mortality cases (and percentage relative to total number of autopsies in the same time period, 2007–2015).
cThree dogs had significant lesions in multiple disease categories.
Specific anesthetic complications were reported clinically in 3 of the canine cases with no significant autopsy lesions. A closed adjustable pressure-limiting (APL) valve was identified during anesthesia in 2 cases involving a 4-month-old Shih Tzu and a 5-month-old Boston Terrier. Venous air embolism was identified clinically as the COD in a 5-month-old Dachshund in which dyspnea developed immediately after the start of intravenous fluid therapy and progressed to cardiac arrest; however, no gross lesions were identified during the autopsy to confirm this.
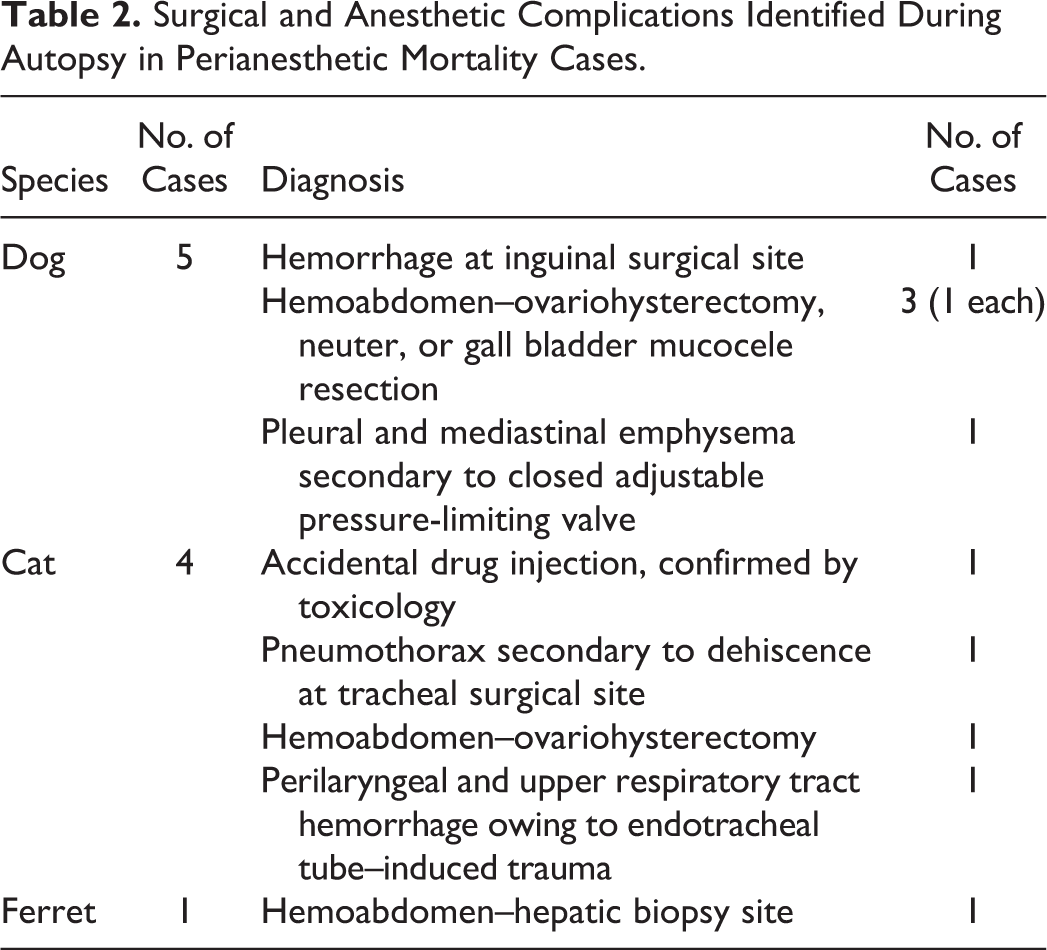
In addition to the above cases of anesthetic complications without significant autopsy lesions, complications of the surgical or anesthetic procedure were confirmed at autopsy and the COD was attributed to these in 10 of 221 animals (5%), including 5 dogs, 4 cats, and 1 ferret (Table 2). Of these, 7 cases involved surgical complications and 3 cases were directly related to anesthetic procedures or equipment. No lesions indicative of surgical complication were identified in horses, rabbits, or other species represented in the study.
Surgical and Anesthetic Complications Identified During Autopsy in Perianesthetic Mortality Cases.
The remaining 130 of 221 animals (59%) in the study had gross and/or histologic lesions indicative of naturally occurring disease that was considered the COD or a contributing COD. These included 55 of 105 dogs (52%), 55 of 90 cats (61%), 9 of 9 horses (100%), 5 of 9 rabbits (56%), and 3 of 4 ferrets (75%), as well as 1 each of the single guinea pig, rat, and chinchilla. Among dogs with natural disease, 3 animals had multiple significant lesions, involving ≥2 organ systems, that were determined to be either the COD or contributed to the COD. These individuals are included in multiple natural disease lesion categories. The majority of lesions involved the respiratory and cardiac systems.
Cardiac lesions were present in 61 of 130 (47%) animals with evidence of natural disease, including 26 of 55 dogs (47%), 29 of 55 cats (53%), 4 of 9 horses (44%), 1 of 3 ferrets (33%), and the single rat in the study (Table 3). Death in animals with cardiac lesions occurred most commonly during maintenance (20 of 61; 33%) and recovery (23 of 61; 38%) phases of anesthesia and infrequently in the phase of sedation or induction. Among dogs and cats, cardiomyopathy was the most frequently diagnosed cardiovascular condition. Lesions of cardiomyopathy were identified in 12 of 26 dogs with cardiac lesions (46%) (12 of 105 total dogs [11%]), representing 12 separate breeds: Macedonian Mountain Dog, Miniature Schnauzer, Whippet, Labrador Retriever, Border Collie, Toy Havanese terrier, Pomeranian, Boxer, Maltese, Chihuahua, Yorkshire Terrier, and mixed breed. The dogs ranged in age from 10 months to 16 years, with a median age of 4 years. No clinical indication of cardiac disease was listed in the history provided for any of the dogs. One dog was described as aggressive during preanesthetic clinical examination and premedication. Nine dogs were undergoing elective procedures, 2 dogs were emergency surgical patients (1 resulting from the presence of a gastric foreign body and the other due to gastric perforation), and the specific reason for anesthesia was unknown in 1 case. Cardiomyopathy was diagnosed based on combined gross and histologic lesions in 9 dogs and on gross lesions alone in 3 dogs that lacked supporting histologic lesions. Of the 10 dogs for which assessment of total heart weight/body weight and ventricular weight ratios (left ventricle + septum/right ventricle) was carried out, abnormalities in 1 or both of these ratios supported cardiomyopathy in 5 cases (50%). 32
Cardiac Lesions Identified During Autopsy in Perianesthetic Mortality Cases.
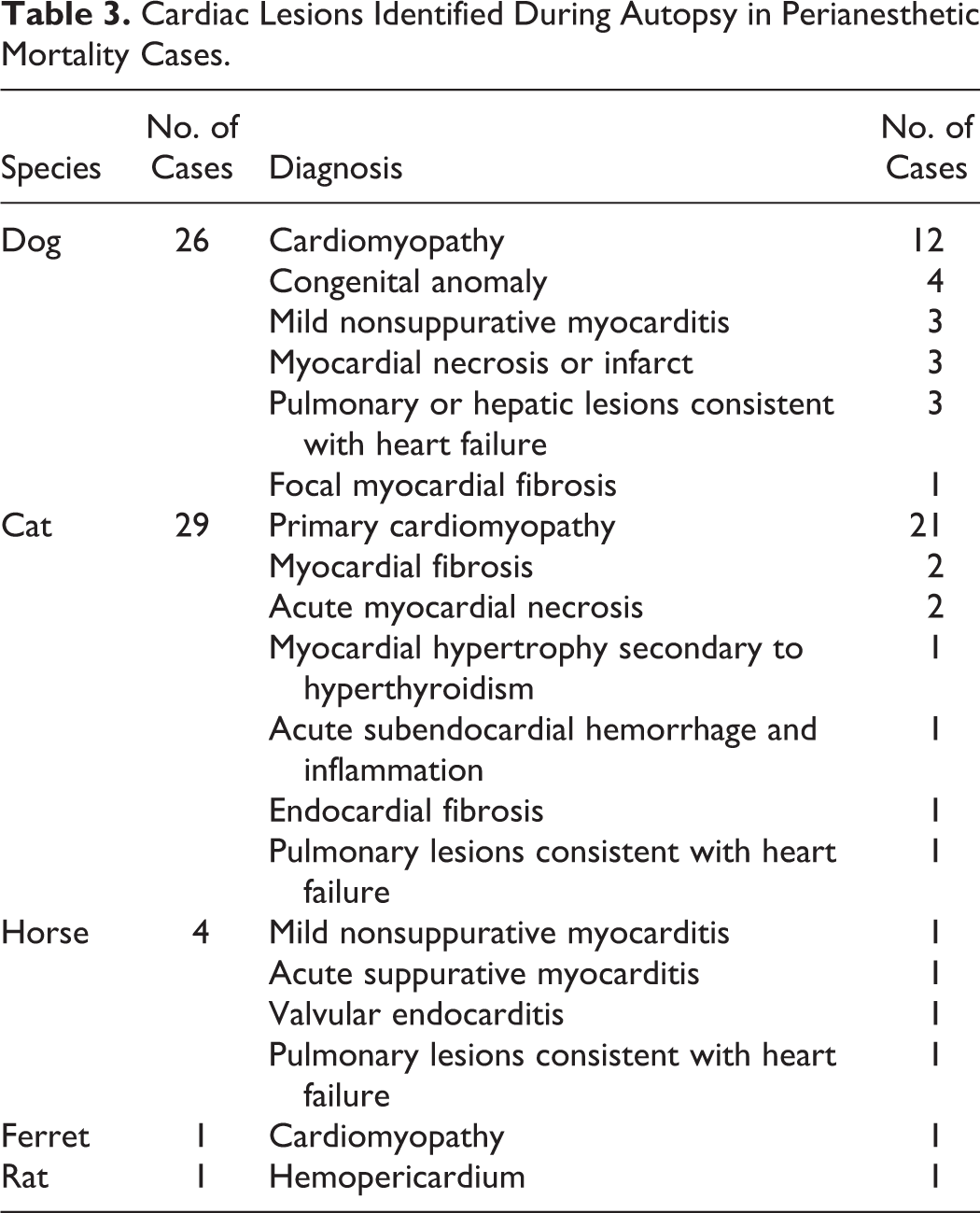
Lesions consistent with cardiomyopathy were identified in 21 of 29 cats with cardiac lesions (72%) and in 21 of 90 cats in the study (23%) and included hypertrophic cardiomyopathy (n = 7 cats), unclassified cardiomyopathy (n = 13 cats), and fatty replacement of right ventricular myocardium (n = 1 cat). Breed distribution of cats with lesions consistent with cardiomyopathy included 14 Domestic Shorthair, 4 Domestic Longhair, and 1 each of Burmese, Egyptian Mau, and Maine Coon breeds. The median age of cats diagnosed with cardiomyopathy was 4 years, with a range of 5 months to 16 years. Of the 4 cats with recognized clinical disease prior to anesthesia, signs of congestive heart failure were described in 2 cats. Nineteen of 21 cats with cardiomyopathy were undergoing elective procedures at the time of death; the reason for anesthesia in 2 cats was not stated. Heart weight/body weight ratios were recorded in 13 of 21 cases (62%), and left/right ventricular weight (left ventricle + septum/right ventricle) ratios were also recorded in 7 of 21 cases (33%). In these cases, increased left ventricle weight supported a diagnosis of left ventricular hypertrophy, compatible with cardiomyopathy in 2 of 7 cases (29%). 27 A diagnosis of cardiomyopathy was based on both gross and histologic lesions in 11 cats, on histologic lesions alone in 9 animals, and on gross lesions alone in 1 case. In addition to the 21 diagnoses of cardiomyopathy, left cardiac ventricular hypertrophy was attributed to hyperthyroidism associated with thyroid adenoma in 1 cat, and left ventricular endocardial fibrosis or myocardial fibrosis was identified in 3 additional cats but were not classified as cardiomyopathy.
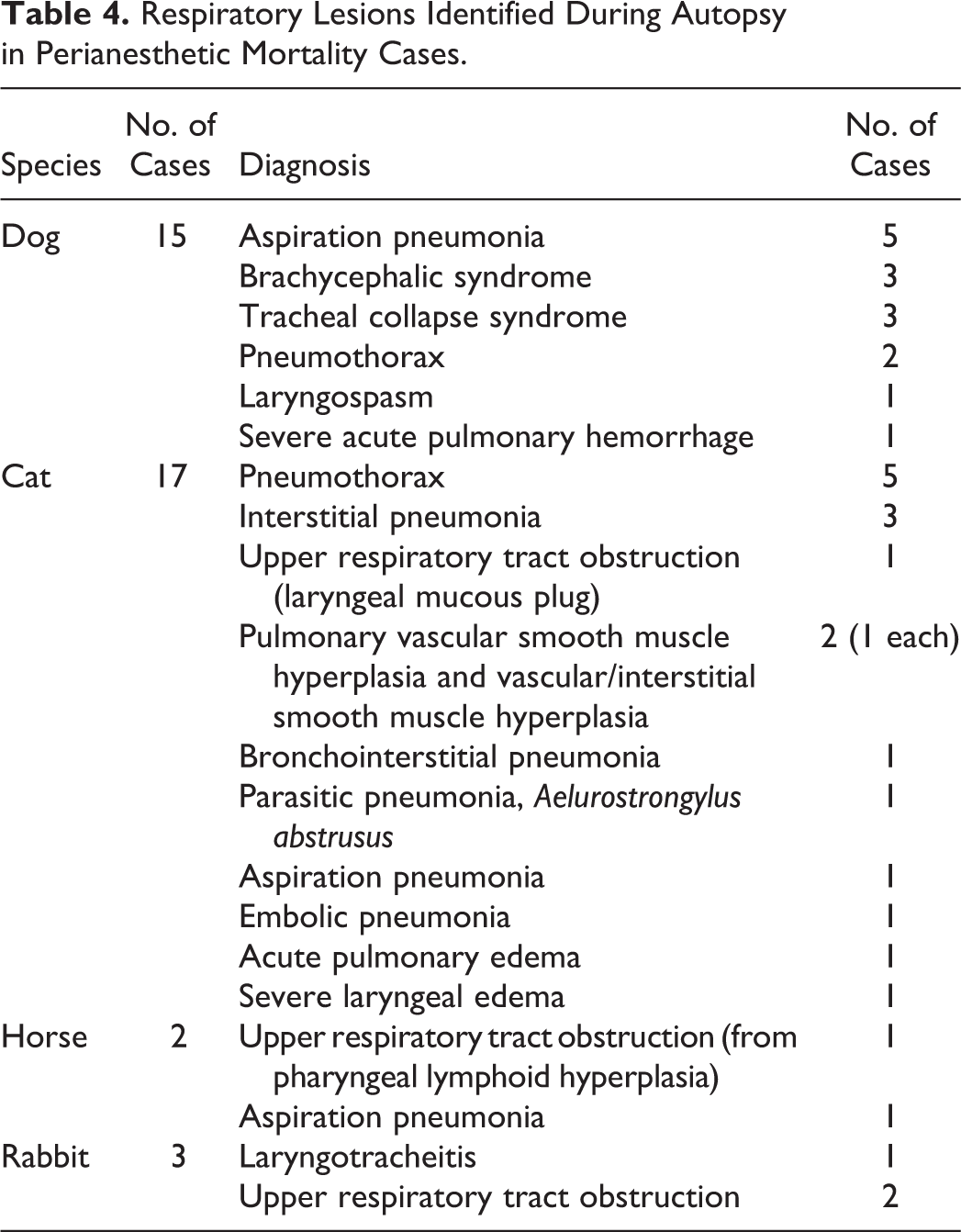
Respiratory tract lesions were present in 37 of 130 animals with natural disease (28%), including 17 of 55 cats (31%), 15 of 55 dogs (27%), 3 rabbits (60%), and 2 horses (22%) (Table 4). Among animals with respiratory lesions, death was reported most frequently during maintenance (10 of 37; 27%) and recovery (19 of 37; 51%) phases of anesthesia, with fewer deaths during sedation (2 of 37; 5%) or anesthetic induction (4 of 37; 11%). The timing of death was not provided in 2 cases. Acute aspiration pneumonia was identified in 7 of 37 animals with respiratory tract lesions (19%) and included 5 dogs, 1 cat, and 1 horse. Aspiration pneumonia was suspected as the primary lesion in 2 dogs in which sepsis was also identified. Among the 30 dogs of brachycephalic breeds included in the study, lesions of brachycephalic syndrome were considered the COD or contributing to the COD in 3 dogs, all of which were English Bulldogs. Death occurred during recovery from anesthesia in each of these 3 dogs. In these 3 dogs, acute aspiration pneumonia and ventricular septal defect were evident in 1 dog, and subaortic stenosis was present in 1 dog in which an episode of collapse had been described historically. Upper respiratory tract obstruction and predisposition to aspiration as a result of brachycephaly, as well as congenital cardiac anomalies, were considered to have contributed to the COD in these 3 animals.
Respiratory Lesions Identified During Autopsy in Perianesthetic Mortality Cases.
Significant systemic disease was evident in 27 of the 130 animals with natural disease (21%), including 10 dogs, 9 cats, 4 horses, 2 rabbits, 1 ferret, and 1 chinchilla. The majority of these animals (1 of 27; 63%) were anesthetized for emergency surgery as a result of various causes, including a gastrointestinal foreign body, intestinal torsion, and emergency caesarian section. Among animals with lesions of systemic disease, death occurred in the postanesthetic period in most cases and among all species (18 of 27; 67%). Lesions consistent with sepsis, endotoxemia, and/or disseminated intravascular coagulation were identified in the majority of animals (20 of 27; 74%). Postsurgical myopathy was evident in 1 horse, and skeletal muscle lesions compatible with malignant hyperthermia were present in 1 cat. Lesions of feline infectious peritonitis were confirmed in a single cat.
A variety of gross and histologic lesions were attributed by specific case pathologists to resuscitation efforts after cardiopulmonary arrest. Potential lesions reflective of CPR were identified in 75 of the 221 animals in the study (34%), including 36 of 105 dogs (34%) and 34 of 90 cats (38%), as well as in 3 rabbits, 1 horse, and 1 ferret (Table 5). Pneumothorax; pulmonary congestion, hemorrhage, and/or edema; pulmonary atelectasis; and multiorgan congestion and/or hemorrhage were the most common lesions ascribed to CPR attempts in dogs and cats. Pneumothorax unaccompanied by primary intrathoracic disease was identified during autopsy in a total of 12 of 105 dogs (11%) and 22 of 90 cats (24%), including cases in which the lesion was interpreted as potentially resulting from CPR, as well as those in which no such association was made by the pathologist. Pneumomediastinum and pleural emphysema were identified in 1 additional dog for which a closed APL valve was identified clinically prior to death (included with surgical and anesthetic complication cases). Pneumothorax was confirmed at autopsy in each of these cases by absence of normal negative intrathoracic pressure when the diaphragm was incised from the abdominal aspect. Pneumothorax was identified both clinically and during autopsy in 1 cat, confirming antemortem development of the condition in this particular animal. CPR was confirmed in the clinical history of 11 of 12 dogs (92%) and 16 of 22 cats (73%) in which pneumothorax was identified postmortem. Resuscitation history was unknown for 1 dog and 6 cats.
Autopsy Lesions Attributed to Resuscitation in Perianesthetic Mortality Cases.a
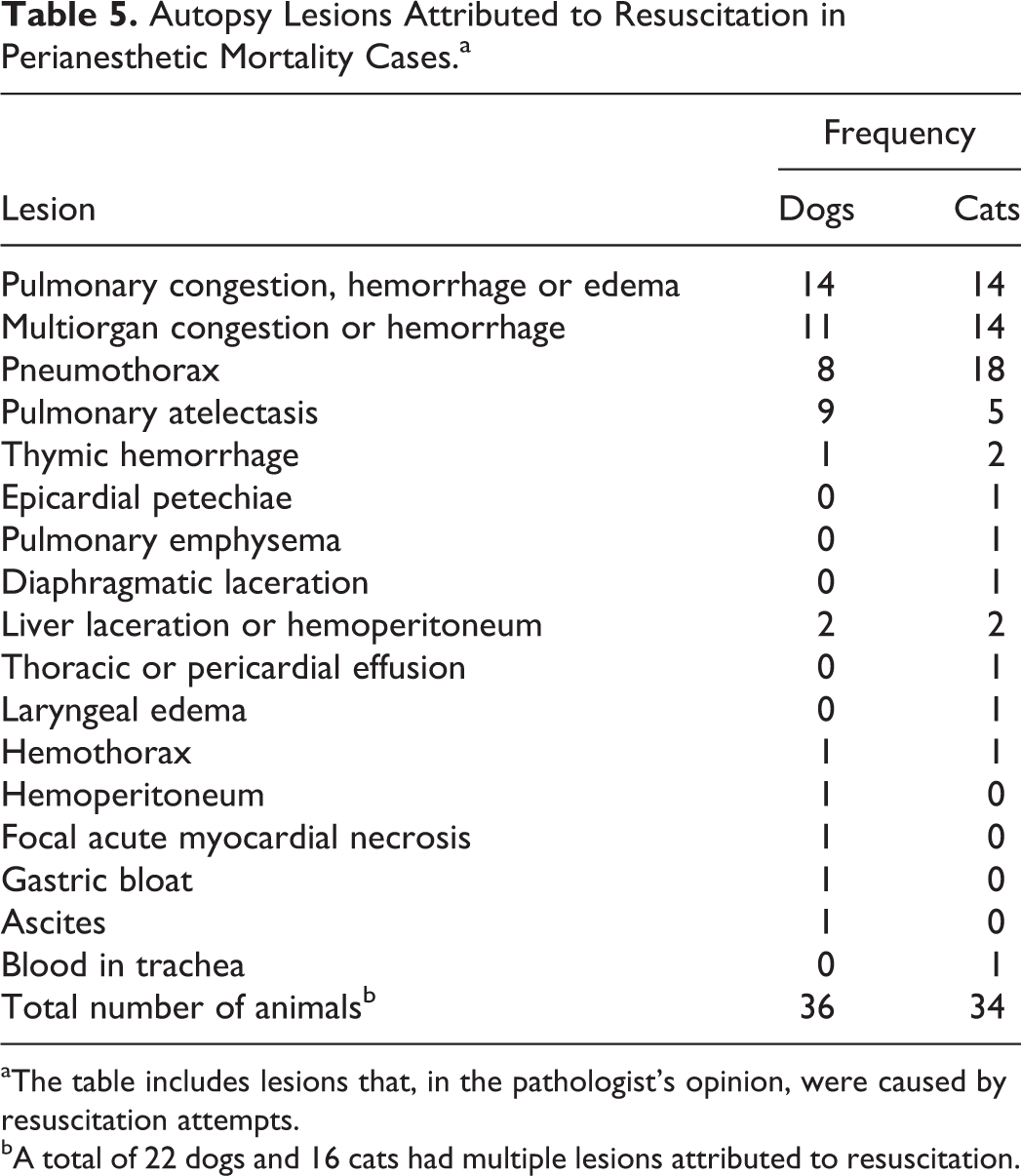
aThe table includes lesions that, in the pathologist’s opinion, were caused by resuscitation attempts.
bA total of 22 dogs and 16 cats had multiple lesions attributed to resuscitation.
Neoplasia was evident and was considered the significant COD in 5 of 105 dogs (5%), 1 of 4 ferrets (25%), and in the single guinea pig in the study. Splenic hemangiosarcoma was present in 4 dogs and was associated with hemoabdomen in 2 dogs, metastases involving myocardium and other organs in 1 dog, and multiorgan infarction in 1 dog. A heart-base chemodectoma with a space-occupying effect and resulting heart failure was identified in 1 dog. Disseminated lymphoma with myocardial infiltration was evident in the guinea pig. A pancreatic endocrine tumor (suspected insulinoma) was confirmed in 1 ferret and was considered likely to have caused hypoglycemia as a complicating factor during anesthesia.
Lesions involving the central nervous or gastrointestinal systems were present in 3 of 105 dogs (3%) and included extensive granulomatous meningoencephalitis in an 8-year-old American Staffordshire Terrier, caudal herniation of the cerebellum in a 7-year-old Pug anesthetized for emergency dorsal laminectomy at C1 to C2, and acute hemorrhagic enteritis of unknown cause in a mixed breed dog.
Discussion
Perianesthetic mortality is well recognized in veterinary medicine, and several clinical studies over the past 20 years have evaluated mortality rates and clinical causes. 2 –4,6,8,10,12,13 However, the use of autopsy to confirm or corroborate the COD is infrequently reported in these studies, 4,8 and only 1 comprehensive study has documented postmortem findings of perianesthetic mortality in animals. 9 The retrospective study reported here documents significant autopsy lesions in multiple species of animals submitted to a North American veterinary diagnostic laboratory over an 8-year time period. Dogs and cats were overrepresented in the study compared with other species and in the relative contribution of each to the overall autopsy caseload of the laboratory. This likely reflects the increased frequency of sedation, general anesthesia, and surgery among these species compared with others in veterinary practice.
Insight from autopsy into the potential COD in the perianesthetic period is limited to conditions or occurrences producing morphologic lesions detectable by gross or histologic examination. Death owing to several causes will not result in specific lesions, including anesthetic overdose, endobronchial intubation, hypersensitivity or idiosyncratic reactions to anesthetic drugs, hypotension, metabolic derangements, or cardiac dysrhythmias. As previously discussed, 9 postmortem toxicologic analysis is currently not practical for assessment of a potential anesthetic drug overdose or drug-related side effects in animals. As a result, the major emphasis in perianesthetic mortality cases is placed on exclusion of preexisting conditions that may have increased the inherent risk of general anesthesia and contributed to the animal’s demise, as well as on the identification of lesions indicative of complications associated with the surgical or anesthetic procedure. 14,28,29
In human pathology, autopsy findings in perianesthetic mortality cases may be divided into the following: (1) death caused by the disease or injury for which the procedure was being carried out; (2) death owing to preexisting disease other than that for which the procedure was being carried out; (3) death as a result of surgical complication; and (4) death attributable to anesthesia when other causes have been excluded. 28 Conclusions in human medicolegal cases involving perianesthetic mortality may be based on both pathology findings and expert clinical (anesthesia and surgery) review of the case, although the requirement for autopsy and the approach to the cases vary among institutions and jurisdictions. 15 Similar multidisciplinary review of perianesthetic death cases in veterinary medicine could provide additional insight into the COD in which postmortem findings do not provide a conclusive COD. Although it is not commonly done in routine veterinary diagnostic cases, consultation with veterinary anesthesiologists on these cases may be enlightening, especially in complex cases with no significant lesions to indicate the COD. In addition, correlation of lesions with clinical history and events that occurred during anesthesia is important. In this study, documented consultation with a veterinary anesthesiologist occurred in only 2 cases. Complete clinical records are required to facilitate this type of multidisciplinary review. The clinical history provided was limited in many cases in the present study and was considered incomplete in 42 cases (19%). This emphasizes the need for provision of more thorough clinical information to pathologists in perianesthetic mortality cases. Autopsy recommendations in human perianesthetic mortality cases recognize the potential for misinterpretation of findings if clinical records are not provided to allow correlation with autopsy findings. 14
Currently, a single comprehensive literature report describes postmortem lesions in perianesthetic mortality cases in animals. 9 That report evaluated cats undergoing general anesthesia for elective sterilization at 2 spay/neuter organizations. Complications of the surgical or anesthetic procedure were identified as the COD in 4% of animals in both the current study and the prior study. Lesions indicative of naturally occurring disease were present in 59% of all animals and in 61% of cats in the current study, compared with 33% of cats in the previous study. In the current study, no significant lesions were identified in 36% of all cases and in 34% of all cats, compared with an absence of lesions in 63% of cats in the previous study. Variations in the overall rates of naturally occurring disease and lesion absence between the current study and the prior study may be partly explained by the more homogenous population with respect to ASA class and procedure (spay/neuter) in that study . However even among cats undergoing elective sterilization surgery in the current study, no lesions indicative of the COD were identified in 44% of cats, compared with an absence of lesions in 63% of cats in the previous study. Factors contributing to the comparably lower rate of anesthesia-associated death with no significant lesions among the cat spay/neuter population in this study are unknown.
Emergency surgical procedures involved 19% of animals in the current study, and clinical disease prior to anesthesia was documented among 31% of animals in this study. An increased risk of death during anesthesia is recognized with increasing ASA classification prior to anesthetic induction, correlating with progressively poorer physical status, in dogs, cats, horses, and humans. 3,4,8,10,34 Emergency procedures have also been associated with an increased risk of anesthetic death in horses and humans. 12,19,34
Lesions associated with resuscitative efforts have been described in humans and animals and must be distinguished from lesions indicative of intercurrent disease. 11,14,23,25,29 In this study, a range of lesions identified in 34% of animals were interpreted by pathologists as directly reflective of external compression, internal cardiac massage, and/or positive pressure ventilation in animals with cardiopulmonary arrest. The majority of putative resuscitation-associated lesions involved vascular stasis primarily in the lung but also in other organs. Vigorous external chest compression was interpreted as the cause of thymic hemorrhage, hemothorax, hemoabdomen, lacerations in the liver and diaphragm, epicardial and pulmonary hemorrhage, and pneumothorax. Rib fracture is also reported as a resuscitation-associated lesion in humans, potentially causing pneumothorax, but was not identified among animals in this study. 25 A recent prospective study of CPR outcomes in dogs and cats identified lesions directly attributed to resuscitation in 34% of dogs and cats, and these were similar to presumed resuscitation-induced lesions in this study. 17 Notably, pneumothorax was not identified in that study and may reflect the experience of the personnel involved in resuscitation, which was limited to cases at a referral institution. This suggests that although pneumothorax may be induced by aggressive manual ventilation, especially in small animals with low tidal volumes, careful examination for other potential causes of pneumothorax should also be carried out.
Spontaneous pneumothorax may also develop antemortem in dogs and cats, prior to resuscitation, and may contribute to cardiopulmonary arrest during general anesthesia. Spontaneous pneumothorax in dogs most commonly results from rupture of pulmonary blebs or bullae that are unassociated with inflammatory, infectious, or neoplastic lung disease. 26 In contrast, spontaneous pneumothorax in cats has been reported only as a secondary event in conjunction with underlying, often extensive lung disease. 16,22 Pneumothorax, pneumomediastinum, and subcutaneous emphysema may also result from tracheal rupture, occasionally induced during the placement of an endotracheal tube in cats. 21,31 In this study, pneumothorax was most frequently identified in cats (22 cases; 24%). Four of the 8 dogs with detectable pneumothorax were of small breed, and all but 1 dog was 6 months of age or younger. Pneumomediastinum was present in 1 dog in which the APL valve on the anesthetic machine had remained closed. Differentiation at autopsy between spontaneous antemortem and resuscitation-induced pneumothorax is not possible; as a result, pathologists must be cautious in ascribing significance to pneumothorax as a contributing factor in individual cases of perianesthetic mortality.
Despite the difficulty in differentiating antemortem and resuscitation-induced pneumothorax, the autopsy should evaluate the presence of this condition. Radiography at the start of the examination, prior to opening the body, is the most reliable method for confirming the presence and magnitude of pneumothorax. During the autopsy, the presence of normal negative intrathoracic pressure, which would help exclude significant pneumothorax, can be confirmed by making a small incision at the abdominal aspect of the diaphragm and observing collapse of the concavity of the diaphragm into the thorax. In humans, a recommended technique for detection of pneumothorax involves careful dissection and removal of an intercostal muscle while preserving the underlying parietal pleural. 7 Visceral pleura will be evident adjacent to parietal pleura in the absence of pneumothorax, but it will not be visible if significant air is present in the pleural cavity. Ruptured pulmonary bullae, predisposing to spontaneous pneumothorax, may be identified by submerging the entire lung in water and injecting air into the trachea to inflate the lung while observing for air bubble escape into the surrounding liquid.
Venous air embolism has been reported as an uncommon but sometimes fatal complication of surgical and diagnostic procedures during general anesthesia in animals. 11,23,33 The clinical outcome of air embolism depends on the volume and rate of air introduction and on the clinical status of the animal. 20,35 A fatal intravenous bolus dose of air >2 ml/kg in dogs has been suggested, extrapolated from experimental data in pigs. 35 In the present study, air embolism was suspected as the COD in 1 dog based on clinical information, although this was not confirmed at autopsy. Various surgical manipulations may predispose to air embolism, including any surgery in which large veins are incised. 7 In dogs and cats, venous air embolism has been associated with inadvertent intravenous injection of air, dental procedures using a high-speed air-cooled drill, surgical techniques using air insufflation, and cryosurgery employing a spray technique. 11,23,24,30,33 Air emboli introduced inadvertently through intravenous injection may be a more significant risk factor in small breed dogs and possibly cats, because less air would be required to significantly affect the heart and vasculature in these animals. 23 Air emboli may result in physical air lock of the right ventricle and/or pulmonary hypertension. 1 Patients undergoing procedures at higher risk for this complication should be evaluated during the autopsy using special dissection techniques for detection of potential air emboli. These lesions may be easily missed during routine autopsy. As with pneumothorax, radiography prior to opening the body may identify air emboli in the thoracic cavity, primarily within the right ventricle and major blood vessels. 7 The presence of an air embolus in the right ventricle of the heart can be assessed by filling the unopened pericardium with water, then making a full-thickness stab incision in the right ventricular free wall or atrium, and monitoring for release of air bubbles into surrounding water. 7,23 Other techniques describe en bloc dissection of heart and lungs (pluck), then submerging the heart in water prior to incising the right ventricle and observing for air bubble escape. 33 Air may also be aspirated from the right ventricular lumen using an 18-gauge needle and large syringe. 11 Evaluating large veins for the presence of air bubbles may also aid in confirmation of a diagnosis of fatal air embolism. The state of preservation of the body is important to consider when interpreting results of these specialized dissection techniques, because putrefaction may result in intravascular accumulation of air unrelated to the COD.
Established procedural guidance for autopsy of veterinary perianesthetic mortality cases is limited. On the basis of the results of this study, in combination with review of human and veterinary literature, several recommendations can be made regarding the autopsy procedure in these cases. Review of the animal’s complete clinical history is imperative prior to beginning the autopsy, and the pathologist must ensure that all relevant information is obtained from the clinical veterinarian. Gerdin et al 9 provide recommendations for clinical information to be included with autopsy submissions in cases of perianesthetic mortality. Results of preanesthetic bloodwork, anesthetic and surgical records, and previous or concurrent disease conditions should be included in the history. The clinician’s accurate description of procedures around the time of the animal’s death, as well as the animal’s condition leading up to the time of death, can provide insight into potential causes of death. For example, arrest immediately after intravenous catheter placement could be suggestive of venous air embolism, or progressively shallow respiratory efforts may support antemortem pneumothorax. Direct dialogue between the pathologist and clinician may be the most efficient and informative way to obtain the level of clinical detail necessary for the pathologist to be completely informed of circumstances surrounding the animal’s death. Knowledge of potential complications inherent to the specific surgical or other procedure involved will alert the pathologist to purposely evaluate the lesions indicative of these complications. 14
The pathologist should proceed with external and internal examination using a familiar autopsy protocol, but with heightened attention to the heart, upper respiratory tract, and lungs. Prior to opening, the body should be examined for possible subcutaneous emphysema, and surgical incisions should be examined and recorded. Radiography should be considered for potential identification of pneumothorax, pneumomediastinum, and venous air embolism. Presence of pneumothorax may be assessed by incising the diaphragm or dissecting intercostal muscles, as described above, and prior to opening the thorax. Before dissection of lung and heart, lungs may be submerged in water and inflated by air introduced by large volume syringe via the trachea, monitoring for air bubbles indicative of ruptured pulmonary bullae. Upper airways should be evaluated for potential obstructive lesions, including soft palate abnormalities, laryngeal edema or hemorrhage, and mechanical obstruction by foreign bodies, mucus, inflammatory exudate, or other debris. Assessment of both the mucosal and outer surfaces of the trachea may identify lacerations or other traumatic lesions potentially associated with intubation. Evaluation of the pleural cavity, lung, and visceral and parietal pleura should include documentation of lung inflation, type and volume of any pleural fluid, and character and distribution of lung lesions. Important components of a heart examination include examination of each cardiac chamber and inclusion of chamber weights, as well as evaluation of the heart valves, myocardium, and endocardium. The autopsy should include evaluation and documentation of surgical sites, and the presence and volume of hemorrhage at any site should be recorded. A thorough set of tissue samples, including brain tissue, should be collected for histologic examination in order to confirm or exclude underlying natural disease processes. Samples should also be collected for microbiologic testing, if deemed necessary on the basis of gross lesions. Importantly, the interpretative section of the pathology report should attempt to correlate the clinical circumstances surrounding the perianesthetic death with lesions identified during the autopsy.
This retrospective study attempts to help fill a void in the veterinary literature regarding autopsy findings in animals dying during or within 24 hours of sedation or general anesthesia. Lesions indicative of significant, preexisting natural disease were identified in most animals, and surgical or anesthesia-related complications were evident in a much lower proportion of cases. However a significant number of animals lacked lesions indicative of a potential COD. Exclusion of underlying, preexisting disease and iatrogenic complications remains the primary goal in autopsy of perianesthetic mortality cases. Pathologists must be aware of potential complications and resultant lesions associated with various surgical and diagnostic procedures, as well as with lesions induced by resuscitation efforts. Correlation of autopsy lesions with the clinical history and potential COD is an important part of the pathology report.
Footnotes
Acknowledgements
I thank each of the 34 pathologists whose diagnostic reports contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.