
Abstract
Localized thermal injuries in animals may be caused by exposure to fire and radiant heat, contact with hot items including hot liquids or steam, inhalation of hot air, and exposure to cold temperatures. In addition, animal fire victims may have intoxications caused by smoke gas. This article reviews the causes, pathogenetic aspects, morphological findings, additional investigations, differential diagnoses, and causes of death in various forms of thermal injuries. Since these cases do not occur frequently in diagnostic pathology, they represent a challenging task in general but also with respect to forensic or criminal aspects, such as whether a lesion represents an accidental or nonaccidental effect. Besides detailed information about the circumstances at the location, thermal injuries in animals require a thorough morphological evaluation, including additional investigations in conjunction with a profound knowledge about the possible lesion spectrum and suitable additional investigations.
Keywords
Thermal wounds are relatively uncommon in veterinary pathology. 51 When present, they usually represent a diagnostic challenge. Prolonged exposure to excess heat or excess cold is an important cause of localized or generalized alterations, occasionally with fatal outcome. Localized heat lesions comprise burns, scalds, and inhalation trauma. Prolonged localized exposure to excess cold results in local hypothermia, local cold injury, or frostbite. Generalized thermal injuries caused by exposure to heat or high ambient temperatures (ie, heat exhaustion or heat stroke) and to cold (ie, general hypothermia) will be discussed elsewhere in this issue. 46 In addition, electrothermal lesions are described in a different review article of this issue. 75
Morphological changes after dry heat exposure are classified according to depth and area affected. In surviving animal victims, these factors are of clinical significance regarding the prognostic assessment. 36 Furthermore, chronic recurrent exposure to heat may induce proliferative skin lesions and even cancer. In fire victims, the pathologist has to consider whether the extent and degree of cutaneous lesions are serious enough to adequately explain death or whether other factors may be involved, such as deadly antemortem trauma, intoxications, or preexisting diseases. Inhalation of hot and toxic fumes is an additional important cause of death in fire victims, and toxicological investigations are required for their identification. The diagnostic pathologist has to search for evidence of whether an animal was alive when it was exposed to fire, a fact that may have serious criminal implications. Findings indicating vital exposure to fire usually occur simultaneously with various extents of postmortem heat damage. 43
Wet heat injuries or scalds typically display a morphological appearance different from lesions caused by dry heat exposure. The inhalation of hot gases or steam results in heat-associated alterations, particularly of the upper respiratory tract. Surviving patients often have necrotizing inflammation of the airways, and many victims die due to secondary bacterial infections. 43
Cold-associated injuries comprise localized lesions that are graded according to their severity. Local hypothermia induces cell and tissue damage directly as well as by circulatory changes. 36 Similar to the chronic effects of heat injury, cold injury may cause proliferative changes, including cancer. 91
This review gives an overview of causes, pathogenetic aspects, morphological findings, additional investigations, differential diagnoses, and causes of death in various forms of thermal injuries. Some aspects of thermal damage in this review article have deliberately been adopted from human legal medicine to complete the picture and alert the veterinary pathologist in this respect even if these findings have not yet been described in the veterinary literature.
Relationship Between Tissue Damage, Temperature, Duration of Exposure, and Lesional Extent in Heat Injury
Mammalian tissues can only survive within a narrow temperature range between 20°C and 44°C. 41 Parameters influencing the extent of burning damage include the applied temperature, the achieved temperature in the tissue, the ability of the body surface to conduct the excess heat away, the exposure time to the heat, and the thermal capacity of the tissue. 41,43,45,48 The relationship of temperature and time is important because even relatively low temperatures may be harmful; for example, skin exposed to water of 44°C causes scalds after an exposure time of 6 hours. 48 It has been shown on shaved skin of guinea pigs and rats that contact to a heated iron item for 60 seconds results in transient erythema at 50°C and a crust at 55°C. At 60–65°C, the epidermis is easily separated from the dermis, and at 70–80°C, heat coagulation induces a stiff yellow eschar representing dead tissue that sheds or falls off of healthy skin. 43 Full-thickness burns of rat skin occur within 10 minutes after exposure to 55°C, while the same lesion develops in 3 minutes at 60°C. 80
The temperature achieved in the tissue decreases progressively and rapidly with higher penetration depth. 43 Experimental exposure of shaved canine skin to steam for 20 seconds resulted in a temperature of 85°C at a tissue depth of 0.5 mm, 66°C at a depth of 1 mm, 60°C at a depth of 2 mm, and 50°C at a depth of 3 mm. 60 Exposure to a heat source of 70°C causes considerably more severe damage at a defined tissue depth after 60 seconds compared to after 10 seconds. The skin of animals does not disseminate heat to the same extent as the skin of humans because a superficial vascular plexus is lacking, resulting in a comparatively higher vulnerability to heat exposure.
Typically, various levels of injuries are present on an individual exposed to heat. The area of the most severe damage may indicate the initial, longest, or most intense contact with the heat source and that may help to identify where the burn started on the body. In cases with evenly distributed lesions of the same severity, an exposure to uniform heat has to be considered, such as a flash fire, hot steam or gases, or an immersion into hot fluids. Exposure to open fire may cause a wide distribution of separate burns where the fur acts as a wick for the fire to reach the skin. 45
Dry Heat Injury
Dry heat injuries are caused by direct contact or near contact to heat sources, resulting in burns characterized by desiccation and carbonization of tissues. 20 Such heat sources include flames of open fires (eg, house, stable, zoo, laboratory, bush and grass, and vehicle fires; candles; fireplaces; burning cigarettes; and others), hot items (eg, hot stoves, electric heating pads, hotplate, electric irons, car engines, mufflers or heating pipes, and others), hot air (eg, hair dryer, clothes dryer), or radiant heat in form of a near-contact exposure (eg, overexposure to open fires, heat lamps, oven, radiators, sunlight, or artificial sun-lamps) with conversion of infrared frequencies into thermal heat at the skin surface. 12,41,43,56
Heat damage has to be differentiated from electrothermal and chemical burns (eg, unslaked lime), 20,43,45 radiation injuries, and mechanically induced lesions and alterations of nonphysicochemical origin.
Criminal relevance in animal victims from dry heat exposure consists of the differentiation of accidental damage or death in a fire, accidental damage or death caused by an arson, disposal in fire of an animal that died of a natural cause, intentional harm or deliberate killing of an animal using fire, heat as an act of cruelty or to mask another unlawful act, 12 and setting light to a deliberately killed animal. 43 A deliberated infliction of thermal injuries on an animal has to be considered when the history mismatches with the actual circumstances at the scene of the accident and/or the pattern and location of lesions; for example, when a protected body area is damaged, an intentional injury is likely. 45 Intentional local dry heat injury also occurs in animals, such as hot branding of horses and cattle, resulting in third-degree burns. 4
General Aspects of Dry Heat Injury
In animal cruelty cases, it is mandatory to investigate the crime scene for further traces and evidence. Devices to ignite fires may be left behind at the scene, and odor or residues of the fire accelerant or burn agent may be present in the soil or other absorbent materials. Samples should be taken for further analysis, and a sample of the soil or other material from an adjacent unaffected area should be kept as a control. Fires causing fatalities in animals may be natural, accidental, or incendiary. Particularly in incendiary fires, an accelerant is often used. Gasoline is the most commonly used accelerant, and remnants of this accelerant are most likely to be found in porous, highly absorbent materials that have a large surface area to aid in the retention of the ignitable liquid residues. For toxicological analysis, these materials should be recovered and saved in a gas-tight container. 55
In necropsies of animal fire victims, several aspects should be considered, and these are summarized in a necropsy checklist (Table 1). For the diagnostic pathologist, detailed information from the scene may be extremely helpful for the interpretation of findings. Fire victims should always be necropsied. Even in cases with advanced combustion of external soft tissues, internal organs are comparatively well preserved due to the strong temperature gradient from the surface to the body center. 42 In severe burns, the identification of the individual animal may be difficult. Extended exposure to heat may cause loss of body fluids and reduction in body weight. Determination of the sex is usually possible even in severely burnt victims due to the preservation of internal organs. Microchip transponders (Virbac Co., Bad Oldesloe, Germany) covered either by glass or a biopolymer are experimentally resistant to oven heat of 200°C for at least 2 hours. Single transponders of both material groups were still readable after a heat exposure of 200°C for 7 hours (personal observation). In addition, a DNA sample, such as intact musculature or bone marrow, should be kept for further identification.
Necropsy Checklist for Fire Victims.a
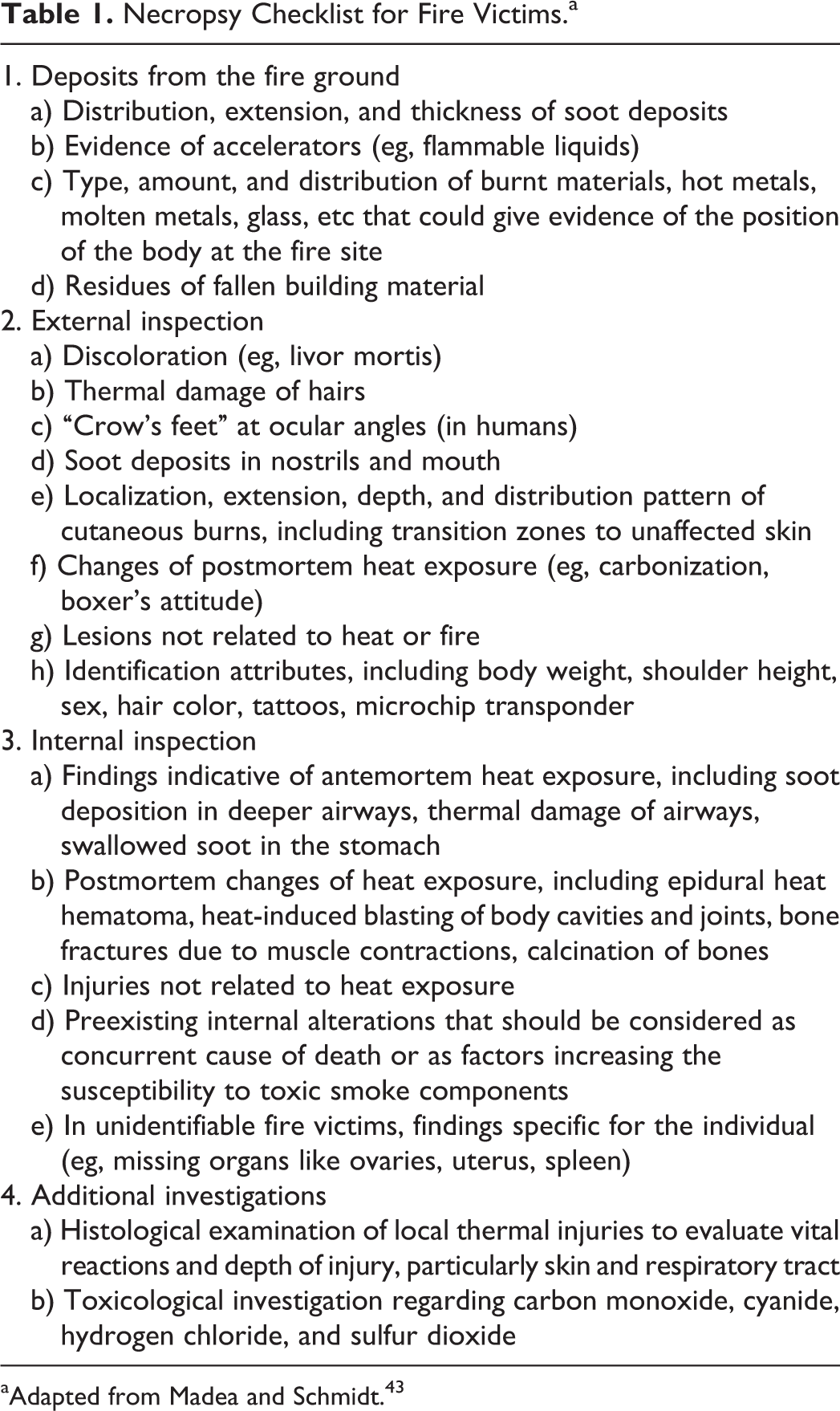
aAdapted from Madea and Schmidt. 43
The whole body of all fire victims should be radiographed for any evidence of antemortem trauma. Because fur and skin may contain residues of fire accelerants, chemicals, or other offending substances, samples of swabs, hair, and skin should be taken close to the burnt area before cleaning the lesions (for further details, see section “Smoke- and Gas-Associated and Toxicological Findings in Fire Victims”). 45
Soot is commonly found in fire victims on the mucous membranes of the oral and nasal cavities, the upper and lower respiratory tract, and after swallowing in the upper digestive tract and the stomach. With absorbent cotton stuffed into the mouth or larynx, contamination of soot particle droppings can be avoided. 45 Traces of soot can be collected using the blade of a scalpel and documented on white clean nonabsorbent paper towels.
Insects may feed on fire victims after death, and for the determination of the time of death, it may be helpful to collect all species and stages of insects for entomological investigations. Cooked or burnt insects in a carcass found at the site of a fire indicate that the animal was already dead for a certain time period prior to the fire.
Samples for histopathologic investigations should be taken from different locations to ensure a comprehensive overview of the extent and severity of the lesions. Similarly, for surviving fire victims, biopsies of burnt skin are a very useful diagnostic and prognostic tool to assess the severity of burns. 56,61
Burns—Severity Grading According to Depth of Injury
Burns should be judged according to their degree (depth) and the affected total body surface area. Burns to the face, eyes, ears, perineum, and feet are considered more severe than those to other body areas because they have the potential of serious disfigurement, loss of function, and severe pain. 45 In addition, thermal damage continues after the individual has been removed from the heat source, possibly resulting in an increase in severity in survivors. 68 Based on the depth of injury, burns are classified into different degrees (Table 2). 20,31,45 Depending on duration and applied heat, mild erythematous to severe necrotizing lesions develop. Unlike other dermatopathologic disorders, in most cases, burns do not progress after 5 days without repetitive injury. 50
Classification, Affected Tissues, Pain, and Morphological Findings of Burns (Adopted From Humans).
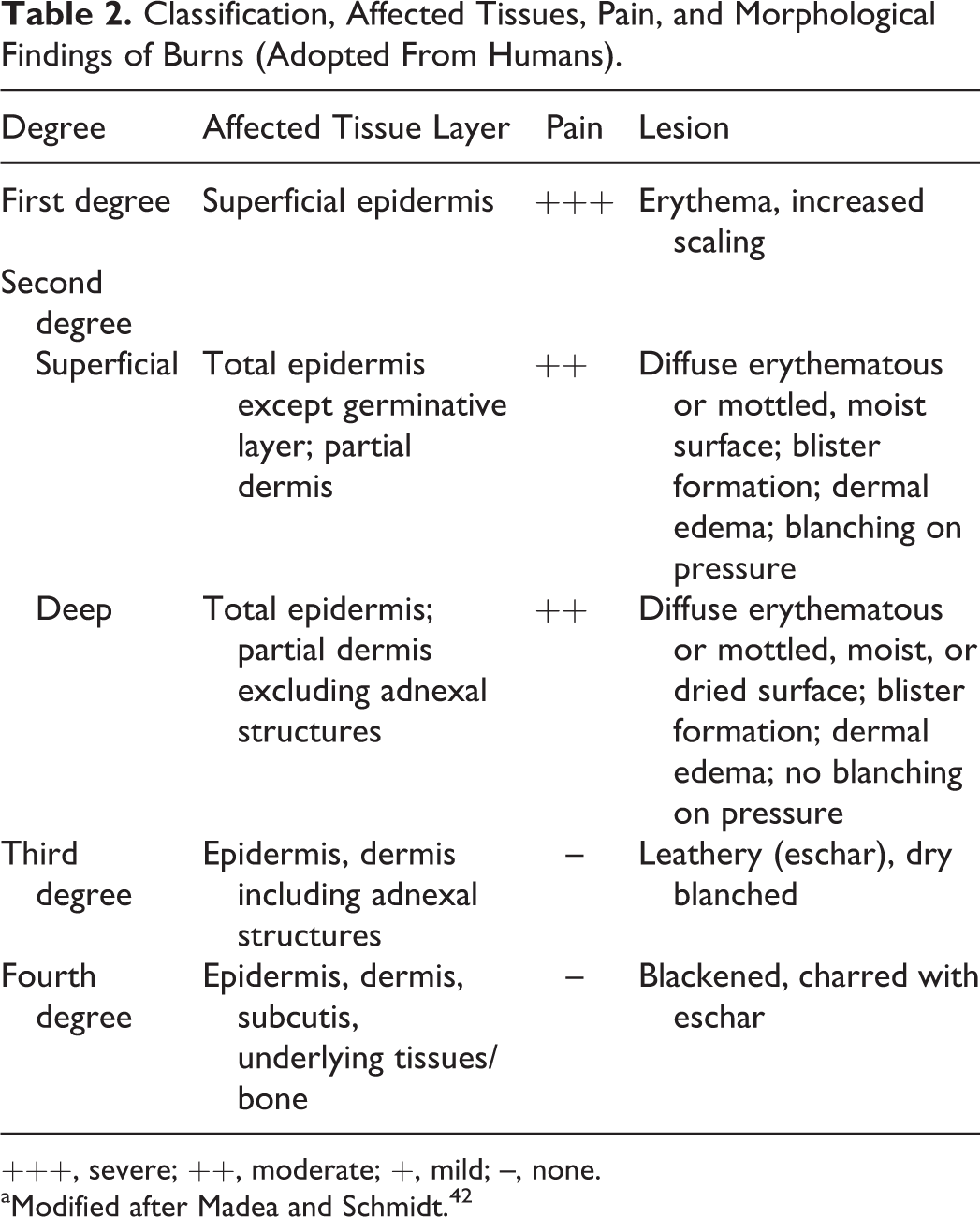
+++, severe; ++, moderate; +, mild; –, none.
aModified after Madea and Schmidt. 42
Damage in first-degree burns (combustio erythematosa), also termed superficial burns, is restricted to the epidermis (Fig. 1). 42 Distension and hyperemia of blood vessels are less prominent compared to humans because the superficial dermal vascular plexus is lacking in animals. Epidermal cells may show cytoplasmic vesiculation. Necrosis of superficial epidermal cells results in scaling a few days after the exposure. 20 Healing in uncomplicated burns occurs within 5 to 10 days and is without scarring. 42 First-degree burns are disregarded for the calculation of the affected body surface area unless they exceed 25%. 35
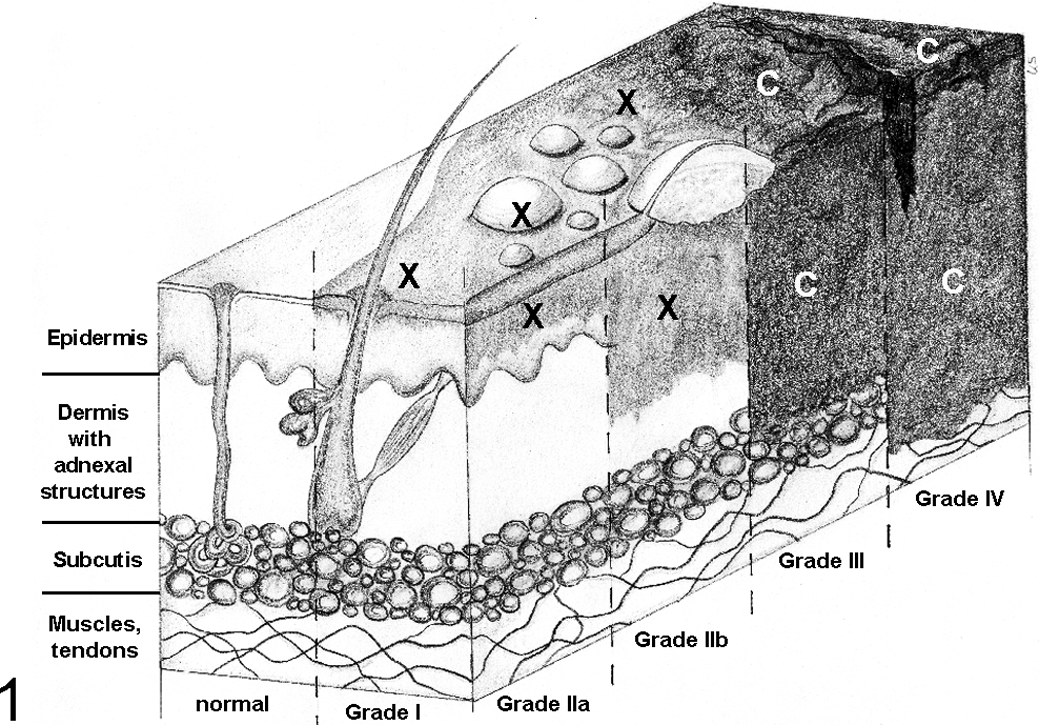
Grade of severity based on the depth of burns and the affected tissue layers. C, carbonized tissue; X, heat-induced lesion.
Second-degree burns (combustio bullosa), also termed partial-thickness burns, are subclassified into superficial dermal and deep dermal burns (Fig. 1). Superficial burns show serous or hemorrhagic intra- or subepidermal blister formation with accumulation of serum, occasional granular debris, and epithelial coagulative necrosis. 43 With the exception of the inner pinna and mucocutaneous junctions (personal observation), skin in dogs and cats normally does not blister, unlike in humans. 56 In second-degree burns, the cytoplasm of epidermal and superficial follicular epithelial cells is hypereosinophilic, and nuclei are shrunken or karyorrhexic. There is epidermal spongiosis, and epithelial cells show elongation and bundle formation toward the source of the heat. There may be an adjacent zone of hyperemia. Severe, protein-rich, perivascular edema is present in the dermis associated with sludge phenomena (ie, an agglutination of erythrocytes caused by reduced flow rate and acidosis) and increased connective tissue basophilia. In superficial second-degree burns, the germinative layer of the epidermis remains intact, whereas in deep second-degree burns, only adnexal structures remain intact, representing the origin of a multicentric reepithelialization. 42,43 Uncomplicated superficial second-degree burns heal within 2 to 3 weeks with mild scar formation, 45 whereas healing of deep second-degree burns takes more than 3 weeks with marked scarring. Blisters infiltrated with neutrophils represent a reliable evidence of a vital lesion. Progressive damage from heat and action of various biological molecules, including cytokines, prostaglandins, and proteinases, may cause continuing tissue damage and edema so that a second-degree burn may progress into a third-degree burn within 24 hours. 45
In third-degree burns (combustio escharotica), there is full-thickness destruction with coagulative necrosis of the epidermis and dermis, including adnexal structures down to the subcutis (Fig. 1). 31 The epidermis is often completely lost. There is a dark brown leathery eschar with white or charred coloration surrounded by hyperemia. Hairs are easily epilated. The heat causes coagulation necrosis of dermal blood vessels, vascular thrombosis, subcutaneous vasculitis, and leakage of deep blood vessels with subsequent coagulative necrosis and subcutaneous edema. 25 The lesion is not painful because pain receptors are destroyed. Spontaneous healing is impossible and occurs only by contraction, epithelialization, and granulation with surgical intervention such as skin transplantation.
In fourth-degree burns (combustio carbonisata), subcutis, musculature, and even bones are destroyed (“carbonization”; Fig. 1). The tissue appears blackened or charred with eschar. The musculature has lost its transverse striations. Usually, these burns lead to systemic illness and are often fatal. 35 Healing is impossible.
Burns—Severity Grading According to Area of the Injury
To estimate the burnt body surface area in adult humans, the “rule of 9” is usually sufficient for prognosis. Adapting this rule to animals is not accurate but can give the veterinarian a guesstimate of the percentage of total body surface area involved. 45,56,68 Specific body surface areas have been assigned to certain percentages: 9% for each forelimb, 18% for each hind limb, 9% for the head, 1% for the neck, 18% for the dorsal, and 18% for the ventral body trunk (Fig. 2). 45 To approximate the affected area of the total body surface, schematic diagrams may be used. Patients with second- to fourth-degree burns involving more than 20% of the body surface area are at risk of developing life-threatening metabolic derangements, and involvement approaching 50% of the body surface area is regarded as incompatible with survival. 56 In humans, old patients may die with considerably less damage, while juveniles appear to be more resistant. 41
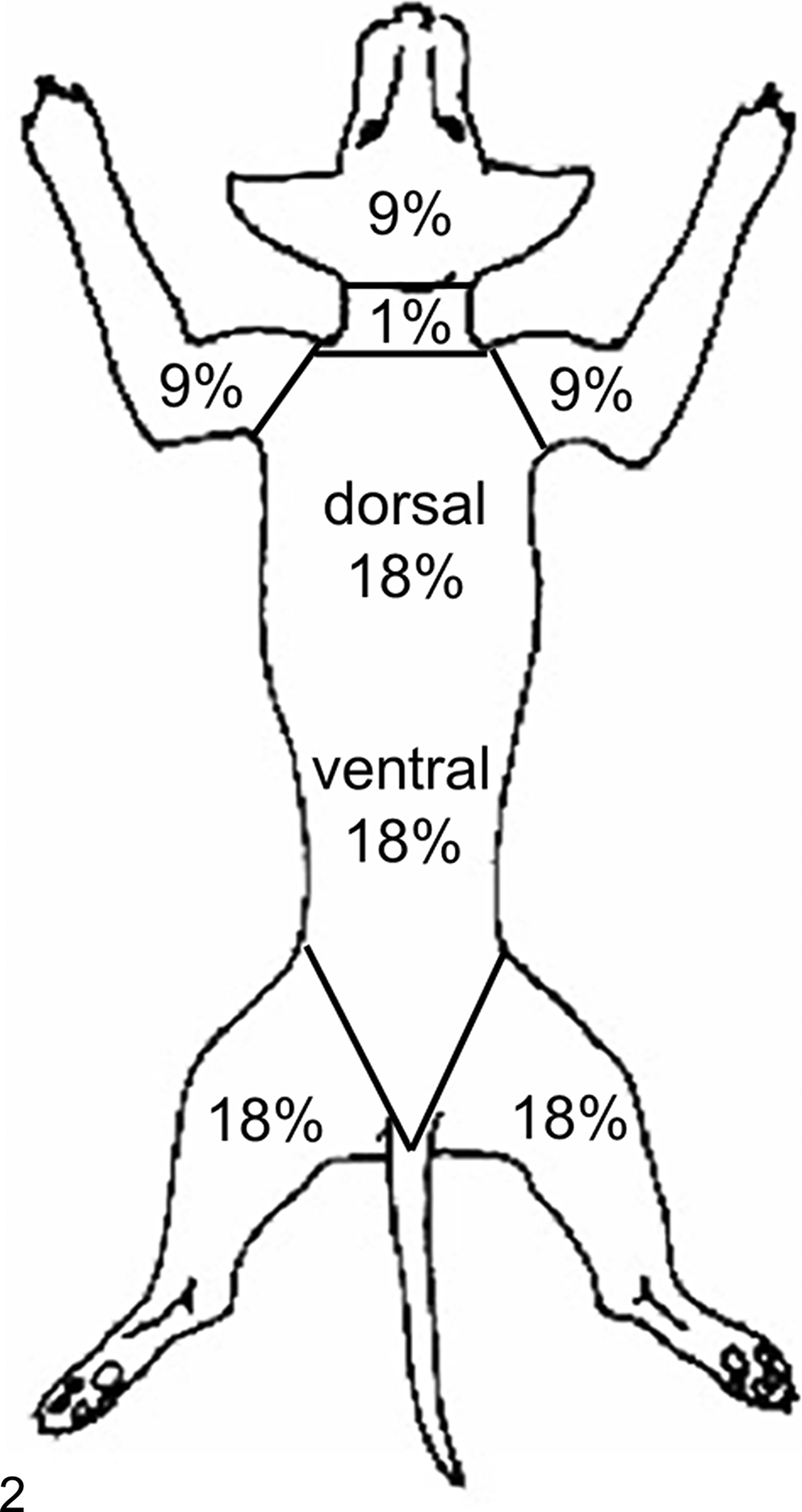
Estimation of the extent of the burned area according to the “rule of 9” schematically depicted in a dog.
Additional Morphological Findings in Local Dry Heat Injuries
Deposition of soot indicates exposure to open fire and may overlie the lesions, often obscuring changes like reddening. Due to the unequal exposure and contact to the flames of an open fire, there is typically a localized or asymmetrical pattern as well as different severity grades of burning lesions, admixed with burns caused by radiation heat. 45 Flash fires, caused by sudden ignition or explosion of gases, fuels, or fine particulate substances, cause extensive burns of a more homogeneous nature. Besides antemortem burns of different degrees, carcasses exposed to heat after death also often show changes of various degrees ranging from cutaneous reddening and blistering to almost total cremation caused by direct fire-related damage and development of aqueous vapor of the extra- and intracellular fluids (for details, see section of “Postmortem Heat Damage”). In many cases, it is impossible to decide unequivocally whether a change developed before or after death.
Most antemortem blisters show a bright red base and, after bursting, an erythematous area, 41 but postmortem hypostasis may obscure the reddening. Epithelial cells of the epidermis, hair follicles, or mucous membranes incline and elongate toward heat (Fig. 3). Intra- and subepidermal blisters are filled with protein-rich exudate (Fig. 4), fibrin, and, after a few hours of survival, also leukocytes. It has been shown experimentally at least in humans that postmortem exposure to heat or flames may also cause erythematous changes similar to first-degree burns and even serous blisters that cannot be differentiated with certainty from antemortem exposure to heat. 41,43 A displacement of blood to areas adjacent to the heat-exposed skin may result in a hyperemic rim that has been interpreted as a pseudovital reaction. 43
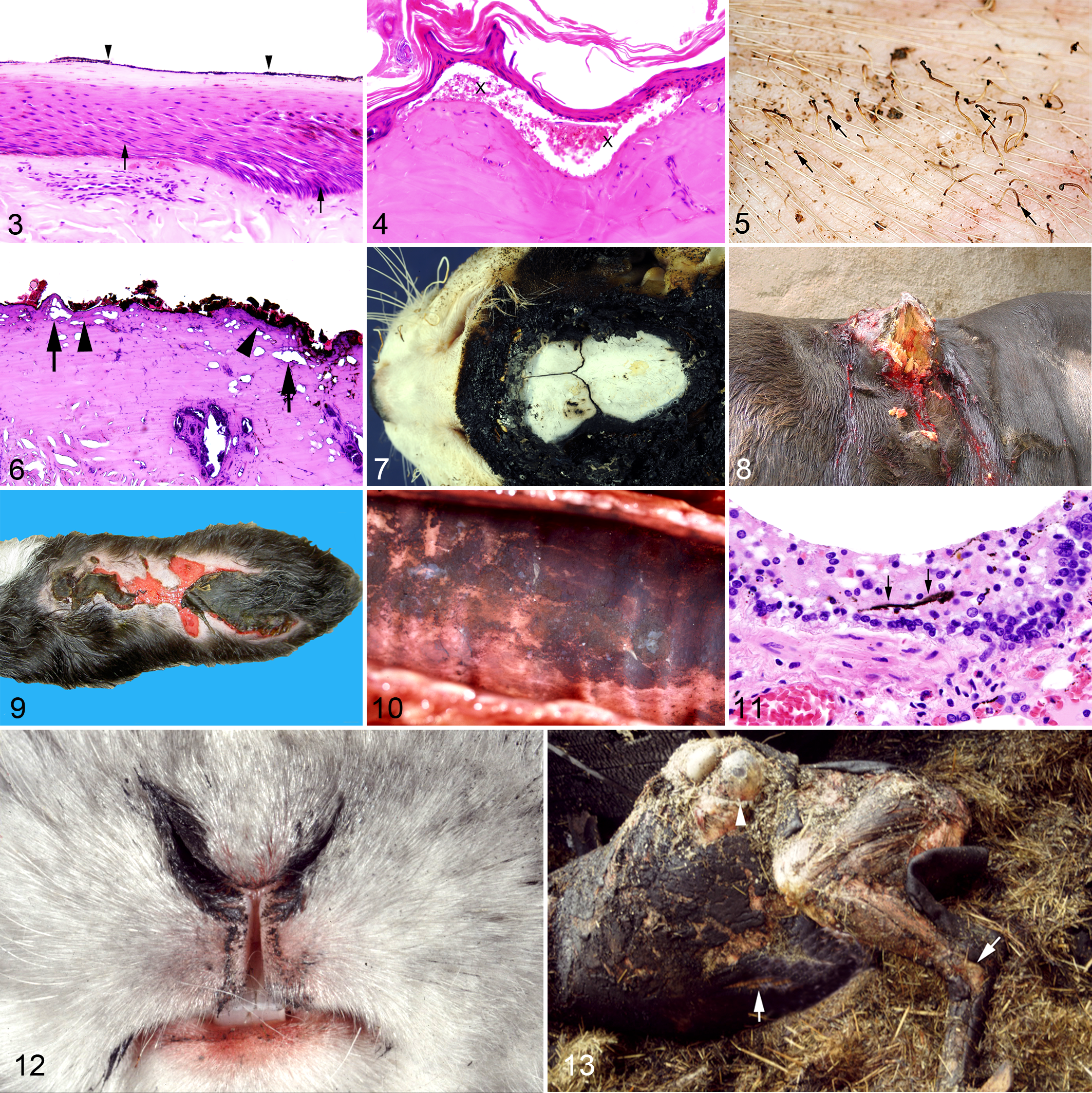
After exposure to dry heat, hairs, feathers, claws, and hooves may be singed or completely burnt away, but not after exposure to hot liquids or steam, which allows a differentiation between burns and scalds. In most cases of low-degree burns, hairs must be shaved or feathers plucked to visualize epidermal lesions. 12 Yellow discoloration of hairs is observed at 140°C, and at around 220°C, melanin is no longer detectable. Hair curling occurs at temperatures above 240°C and carbonization above 300–400°C. 43 Partial singeing of hairs typically results in clubbed ends due to melting of the keratin at the hair ends (Fig. 5).
In cases of skin burns caused by hot metallic objects, thermal metallization may be observed similar to that in electrical skin injuries characterized by metallic deposits on the surface of the lesion. 31
At temperatures above 65°C, the blood turns a brown color. Histologically, clumping and fragmentation of red blood cells may be observed, and leakage of the vessel walls results in serum loss and tissue edema. Coagulation of dermal proteins as in third-degree burns is histologically visible as hyalinization and increased basophilia (Fig. 6). 31 The transitional zone between devitalized and healthy tissue shows reduced blood perfusion with intravascular sludging and is surrounded by a hyperemic rim. Eschar is composed of coagulated skin elements like collagenous and elastic fibers forming a rigid and protective cover of the wound, whereas the crusted wound-cover (the scab), consisting of dead skin cells, blood cells, and fibrin, does not represent a wound protection. 45 In high-degree burns, the subcutaneous fat may act as a fuel and the skin is transformed into black brittle masses. 41 Local carbonization as a vital change is rare.
A fine network of superficial fractures may be visible on bones caused by heat exposure that crumble when handling. The external lamina of the skull bone can fracture or may be completely absent. Temperature, duration, and environmental conditions of a fire cause color changes in bones. A gradual darkening to dark brown occurs at temperatures around 200°C, black coloration is observed at 300°C, and above 300°C, the color shifts to tan and then to gray (Fig. 7) depending on the environmental conditions. Open-air fires cause a gray color in bones at 600°C and a purple tint around 1100°C. A topsoil environment results in a dark gray color at 800–900°C. A long-lasting exposure to high temperature causes calcination characterized by a loss in organic substances. 43,45 The bones are converted into calcinated grayish-white splinters or ash. Estimating the exposure time to fire based on the discoloration of bones should be done with caution in animals. Parameters influencing the color changes, like insulation or availability of oxygen, are unknown in most cases. Human bone and teeth remnants have been examined using X-ray powder diffraction. This method analyzes changes in the microstructural behavior of teeth and bone and allows an estimation of temperature and duration of heat exposure. 59
Cigarette burns on animals in most cases represent deliberate acts of cruelty. Cigarette ember develops a temperature of about 500°C. Acute burns are characterized by circular, circumscribed hyperemic areas of 6 to 8 mm diameter often with a full-thickness necrosis of the skin, resulting in a crater-like lesion. Hairs are singed and show yellowish discoloration. Chronic lesions exhibit thin scar tissue on the surface of the sunken area. Accidental cigarette burns are typically superficial lesions due to brief contact. 51
Healed cutaneous burns may exhibit leukoplakia and leukotrichia representing a desired effect of hot branding in animals. Long-term sequelae develop in some human and animal cases, mostly associated with complicated wound healing, and include loss of skin sensitivity, keloid formation characterized by excessive granulation tissue, hyperkeratosis, burning keratomas (ie, nonulcerated exophytic epidermal hyperplasia [acanthosis] with severe orthokeratotic hyperkeratosis [Fig. 8]), or even squamous cell carcinomas (so-called Marjolin’s ulcer or burn-scar carcinoma). 44,53,76,91
Radiant heat causes burns predominantly on the surface of the body. Depending on the temperature, the skin initially shows erythema (erythema ab igne), then blistering, and finally epidermal slippage. Hairs usually remain intact. After prolonged exposure, leathery skin with charring may develop (Fig. 9). Chronic recurrent erythema ab igne has been described in animals and humans 83 and may induce precancerous dermatosis and finally neoplastic transformation. Kangri cancer, a heat-induced squamous cell carcinoma at the abdomen or inner thighs, occurs in Kashmir people using embers in a clay pot, called Kangri, to produce warmth underneath the clothes during cold weather. Several other skin cancers arising from heat-induced skin damage have been described, including Kang cancer in China, Kairo cancer in Japan, turf or peat fire cancer in Ireland, epithelioma caused by eyeglasses focusing infrared radiation on the cheeks in Australia, and erythema ab igne–associated Merkel cell carcinoma. 26,34,47,85
Evidence of Vital Exposure to Dry Heat
In forensic veterinary pathology, it is important to determine whether an animal was alive or deceased prior to burning. In many fire victims, the terminal condition of a recovered carcass does not reflect the status at the time of death. In advanced cases of burns, it may be difficult or even impossible to determine the presence and extent of antemortem lesions. In most cases, in which fire victims already died from smoke inhalation, early intravital low-degree lesions are obscured by prolonged severe postmortem exposure to heat. The criteria of vital exposure to an open fire are listed in Table 3.
Morphologic Evidence of Vital Exposure to Heat.a
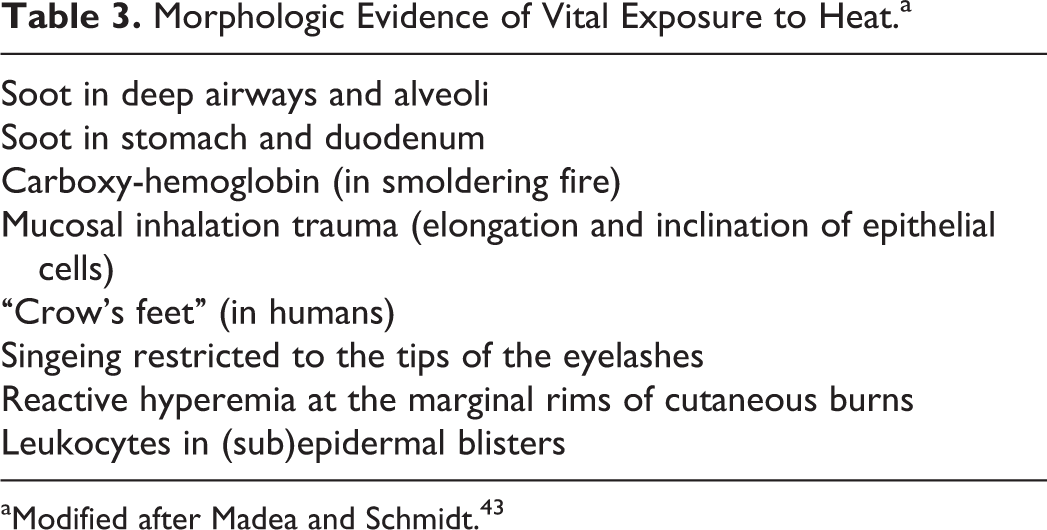
aModified after Madea and Schmidt. 43
The inhalation of soot into the deep airways associated with hypersecretion of mucus occurs only in intravital exposures to open or smoldering fires and represents proof of respiratory function. Grossly, the surface of the deeper airways is coated with dusty black material (Fig. 10) that is often also detectable at bronchiolo-alveolar junctions or even in alveoli as a fine granular, black material (Fig. 11). 31 It cannot be bleached with hydrogen peroxide (exclusion of melanin), does not contain iron (exclusion of hemosiderin), shows no birefringence under polarized light, and does not resolve after treatment with alkaline ethanol (according to Kardasewitsch 37 ) to remove artifactual formalin pigment. Soot phagocytosis by macrophages occurs only in cases that survived exposure to fire for at least some minutes or a few hours. However, it has been shown experimentally in combustions of dead animals and isolated human lungs that carbonized material can rarely be found in deep airways, alveoli, and interstitial tissue, 43 so that in severely combusted carcasses, the legal relevance of soot in deep airways and alveoli is limited. The lack of soot in deep airways does not rule out previous exposure to fire. 43 Soot particles may passively enter the open mouth of a dead individual, covering the tongue, pharynx, and even the glottis. 43 In contrast, the stomach and occasionally also the duodenal content may contain swallowed smoke particles, which are regarded as evidence for life during the smoky phase of the fire. 41,43
Carbon monoxide (CO) is a toxic gas that develops during incomplete burning. Demonstration of carboxy-hemoglobin (CO-Hb) is a valuable indicator that the victim was alive after the fire began (see section “Smoke- and Gas-Associated and Toxicological Findings in Fire Victims”). 43
Inhalation of hot air causes epithelial necrosis in trachea and bronchi, mucosal edema with lymphangiectasis, capillary and venous hyperemia with small hemorrhages, alveolar and interstitial pulmonary edema, and occasionally shock-related intravascular thrombi that are regarded as reliable evidence of antemortem heat exposure. 42,74
In humans, due to involuntary closure of the eyelids, soot is deposited on top of the skin folds, whereas the infolded parts of the skin remain clean. Consequently, after relaxation of the facial muscles, radially extending black streaks (“crow’s feet”) are visible at the lateral corner of the eye. 42,43 Similar observations have not been described in animals, most likely because the hairy coat around the eyes in most species represents a different surface structure of the skin compared to humans. However, soot deposition is found around the eyes, nares, and mouth (Fig. 12). In addition, closure of the eyelids results in a restricted singeing of the tips of the eyelashes. 43
Reactive hyperemia surrounding burn wounds represents additional evidence of an antemortem exposure to fire. 43 Infiltration of leukocytes, particularly neutrophils, in the perivascular dermis of damaged skin or into intra- or subepidermal blisters is reliable evidence of intravital heat exposure in cases with a survival time sufficient to allow inflammatory cell infiltration. Furthermore, various cytokines have been detected in blisters of burning wounds. 88 However, lack of cellular infiltration does not indicate that the burning lesion inevitably developed after death. Blister-like epidermal lesions caused by bruising, blistering, or bullous skin diseases and putrefaction have to be considered as differential diagnoses.
Conjunctival congestive hemorrhages have been described and interpreted as antemortem change in some human fire victims with severe heat-related shrinkage of the cervical and thoracic body parts (pseudostrangulation). However, conjunctival hemorrhages may also occur occasionally in postmortem fire exposure of the eyes. In animal experiments, similar conjunctival hemorrhages could not be reproduced on dead animals. 43
Causes of Death Due to Dry Heat Exposure
Immediate death in human and animal fire victims may be caused by oxygen deprivation, smoke gas intoxication, thermal damage to the airways with lethal laryngotracheal edema or to the body with sufficient depth and area affected, or a combination of these. In addition, preexisting diseases may play a role as contributing factors. 43,45 Sometimes, deadly cyanide intoxication may occur before CO-Hb values have increased. In flash fires, immediate respiratory arrest may be caused either by laryngo-/bronchospasms, vagal reflexes, or inhalative heat shock. A heat shock is thought to be caused by a centralization of circulating blood under heat exposure of the skin. In addition, the heat may induce a “heat rigor” of the thorax with subsequent functional impairment of breathing. 43 In these cases, there are neither morphological nor chemical changes detectable in the blood or lung tissue, and signs of antemortem exposure to fire may be missing. 43
Delayed causes of death in humans and animals who initially survived heat and flame exposure are complications of the burning disease and/or damage to the tracheobronchial airways due to inhalation trauma. 42 Burning disease usually develops in patients with severe burns consisting of second- or higher-degree alterations of more than 20% of the total body surface. 35 Traditionally, burning disease is subdivided into 4 periods: neurogenic shock, disturbance of permeability, intoxication, and infection. Local burns cause irritation of free sensitive nerve endings (neurogenic shock or “burning shock,” commotio neurovascularis), resulting in extensive activation of the central regulatory brain centers of circulation and respiration. The acute phase of shock in humans takes about 8 hours to reach its maximum and declines within the following 48 hours. Almost simultaneously to the neurogenic shock, heat-induced dilatation of capillaries with an increase in permeability takes place. This causes local but possibly also systemic edema that, in concert with exudation from overt fire wounds, results in a reduction in the circulatory blood volume, serum proteins, and electrolytes leading to hypovolemic shock. Systemic liberation of toxic lipoprotein complexes from heat-damaged cell membranes and vasoactive inflammatory mediators rapidly results in a systemic inflammatory response syndrome with increased capillary permeability, subsequent development of edema, and failure of the microvascular circulation. 40 The loss of fluid and protein due to heat exposure leads to hypovolemia, loss of myocardial function, and increased blood viscosity. 45 The increased vascular permeability causes also electrolyte imbalances. Endogenous intoxication develops within 3 days, particularly renal failure due to myoglobinemia and myoglobinuria similar to a crush kidney, and multiorgan failure. Additional complications include immunosuppression, liver failure, anemia, and disseminated intravascular coagulation. 25 Bacterial infections leading to additional local damage or sepsis characterize the late phase and may originate from infections of cutaneous wounds, the respiratory tract, and catheter sites. The mucosal barrier of the gastrointestinal tract is impaired, allowing bacteria and endotoxins to enter the circulation and to contribute to multiorgan failure. 35 Without intensive care, the prognosis for patients with systemic illness caused by burns is poor. Morphological findings in patients who died of acute burning disease may include lesions particularly in the heart, lung, liver, pancreas, and kidney (Table 4).
Morphological Findings in Human Patients Who Died of Acute Burning Disease.a
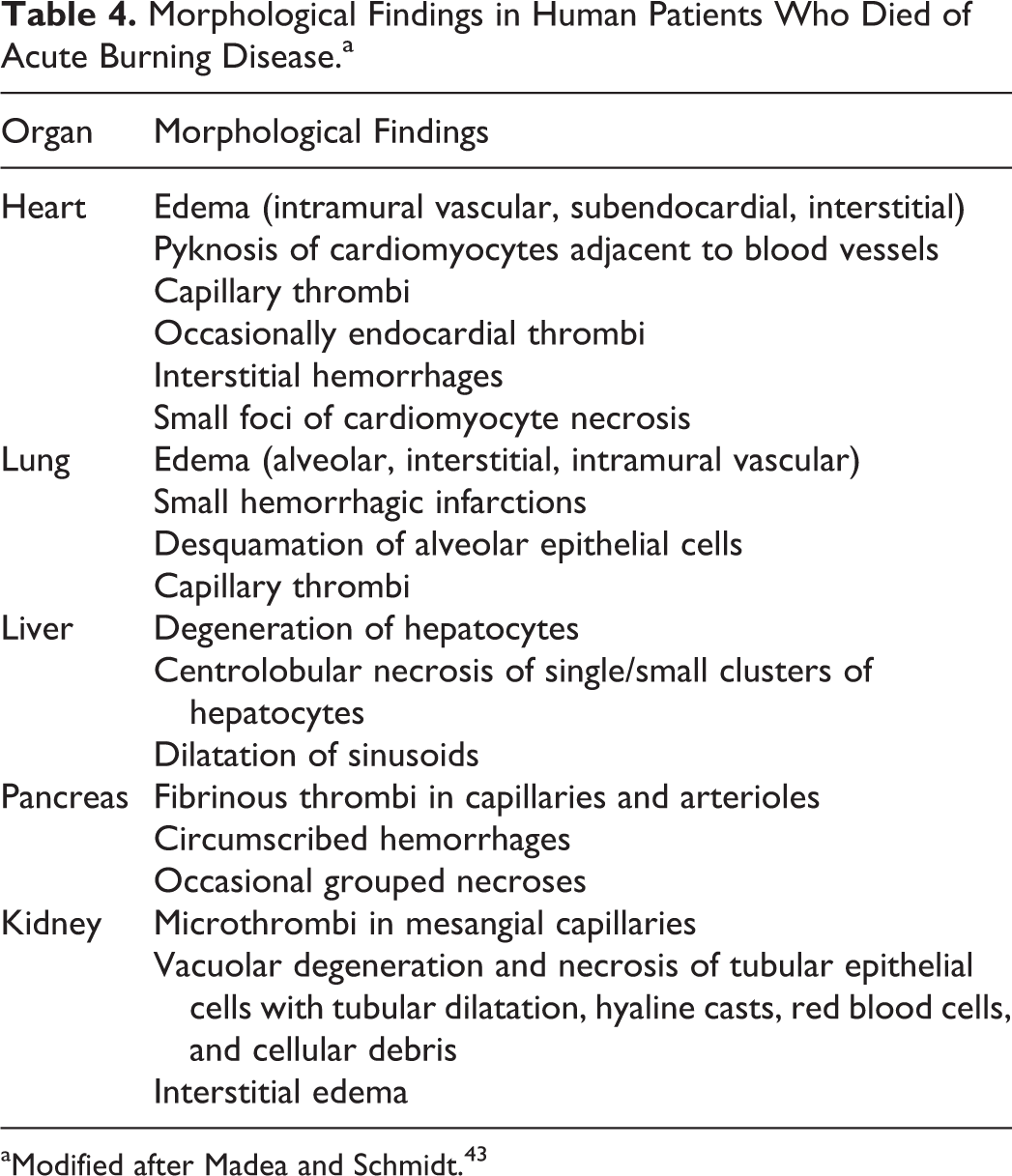
aModified after Madea and Schmidt. 43
Postmortem Heat Damage
In most cases of heat injuries, particularly in fire victims, postmortem heat-related changes are encountered. One main challenging problem—the distinction between antemortem and postmortem damage—may have serious criminal implications. Postmortem changes are caused by vaporization of body fluids, heat-related shrinkage of tissues, and direct impact of flames ultimately resulting in the destruction of the carcass (Table 5). 43
Postmortem Heat-Related Changes in Fire Victims.a
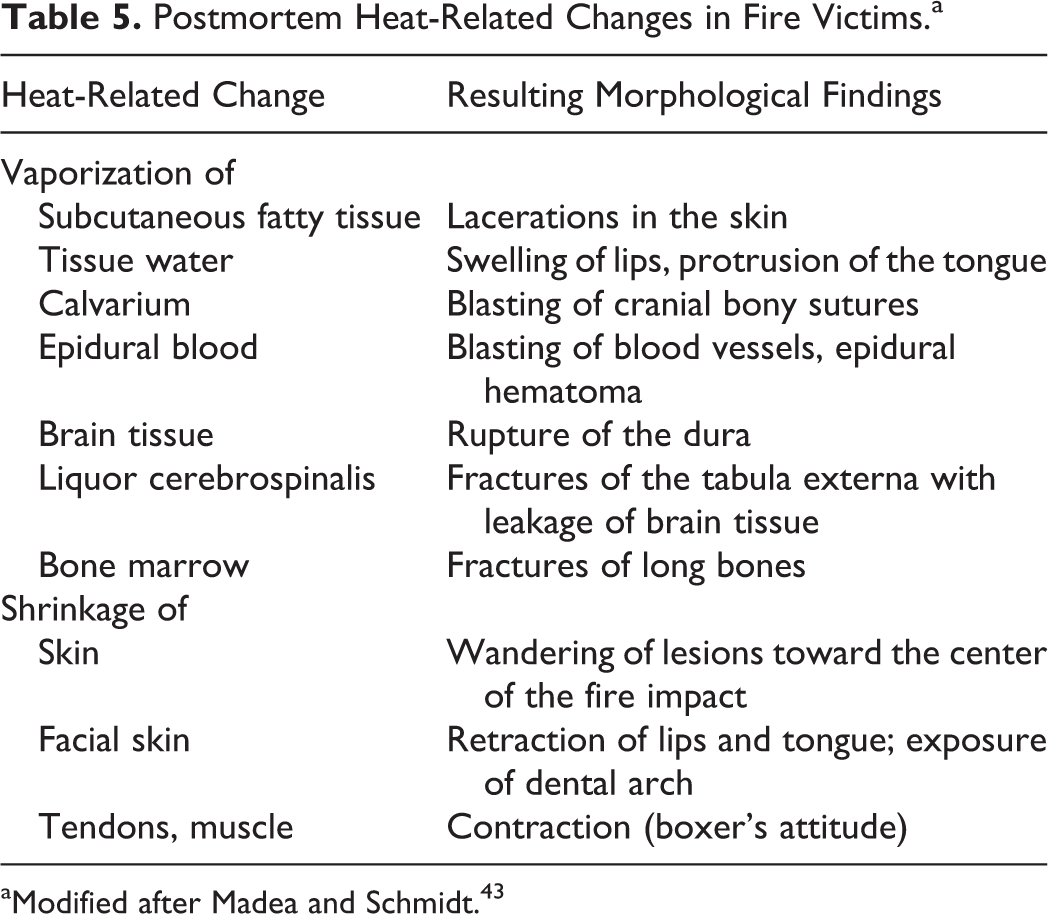
aModified after Madea and Schmidt. 43
Vaporization
Heat injury may cause a change to the aggregate state of intra- and intercellular fluids, when body fluids are boiled and evaporated into aqueous vapor that expands with a continuous increase in temperature. Consequently, heat-related warming of the body results in transient putrefaction-like distension due to gas development, such as swelling of lips and tongue with prolapse. 43 Blood is pressed by the developing vapor into the alveoli, airways, mouth, and nostrils simulating antemortem traumatic injuries. Sharply demarcated splits of the skin result from vaporization of dermal and subcutaneous tissue fluids (Fig. 13). The splits may occur anywhere on the body but are particularly located at joints and extensor surfaces, or the skin may be completely burnt away exposing the underlying tissues. 41 Heat-induced splits in the musculature follow the muscle fibers in contrast to traumatic skin wounds, stabs, or cuts, which often cause splits across or oblique to the muscle fibers. In these cases, it is mandatory to search for additional evidence of trauma, such as incisions of large blood vessels with bleeding in deeper tissues or blood clots attached to the skin or accumulated in body cavities. Blasting of the abdominal cavity is caused by high-pressure expansion predominantly of the gastrointestinal tract due to the development of aqueous vapor from the intestinal content (Fig. 13). Animal experiments revealed that the abdominal cavity does not rupture at temperatures around 500°C but at temperatures of 800°C. 43 Ruptures of joints due to boiling and vaporization of synovial fluid may result in amputation of limbs. 42 Vaporization of fluids in the cranial cavity and of blood in the cranial bones causes blasting of the bone sutures of the calvarium, rupture of the dura, and fractures of the skull with leakage of brain tissues. Fractures of long bones are caused by vaporization of fluids in the bone marrow.
Heat-Induced Shrinkage
Prolonged heat causes shrinkage of the skin surface of up to 70%. This is accompanied by a passive movement of antemortem skin lesions toward the center of the heat impact. It is of importance in criminal investigations that shrinkage of the skin also results in a reduced length of stab wounds causing a mismatch between wound length and width of the blade. 43 Heat-related drying results in a stiff, leathery consistency of the skin. Loss of tissue water causes retraction of the lips and exposure of the teeth (Fig. 14). The musculature appears pale, grayish, and partly cooked, which is almost always a postmortem change and often found in dead bodies remaining in the heated environment of a fire. Dehydration and protein denaturation result in shortening of the muscle fibers and tendons. The flexor muscles contract more than the extensors so that the limbs are typically fixed in a flexed position that is termed “boxer’s” or pugilistic attitude in humans 43 and may also be found in animals (Fig. 15). Contraction of the paraspinal musculature results in opisthotonus and rising of the tail (Fig. 15). Heat exposure to bone tissue causes loss of organic substances (calcination). In association with shrinkage and subsequent rupture of the dura mater, there may be formation of an extradural heat hematoma, which is accumulation in the extradural space of brick-red or brown, coarse granular, almost dry or clay-like material with numerous gas bubbles that may have a liquid fraction at the periphery (Fig. 16). 41,43 Histologically, the heat hematoma is mainly composed of liquefied fat and gelatinous masses and contains only few blood components. 31 As a differential diagnosis, a true intravital hematoma resulting from trauma has to be considered.

Direct Flame Destruction
In carbonized areas, the skin and often the adjacent soft tissues appear as black, rock-hard plate. There are no distinguishing features of ante- and postmortem carbonization. Extensive carbonizations mainly occur after death. 43 In typical house fires, temperatures reach 500–1000°C. 43 This may result in partial consumption of soft tissues or total combustion of an animal’s carcass depending on body size, exposure time, and heat impact. Normally, conditions for total burning of an animal exist only in a crematorium. Cremation of a carcass up to 1 kg body weight needs approximately 30 minutes and a temperature of 1000°C, resulting in 0.1–0.15 liters of ash; a carcass of 20 kg body weight yields approximately 1.5 liters of ash within 1.5 hours; and a carcass of 80 kg yields approximately 4.5 liters of ash within 2.5 hours (Tierbestattung Im Rosengarten, personal communication, 2015).
Duration of Heat Exposure
The estimation of the time of fire exposure based on the fire-induced lesions is difficult and is only rarely required in forensic cases. Experimental investigations have shown that rupture of the abdominal cavity and release of internal organs in rabbits exposed to fire occur after 4 to 5 minutes and in pigs after 15 minutes. Direct exposure to a Bunsen fire for 10 minutes causes severe carbonization of the skull with fissures, the skull sutures may move apart, and a 0.5-cm-thick epidural hematoma of several centimeters in diameter may develop. 43 After 20 minutes, the bone glows red.
Smoke- and Gas-Associated and Toxicological Findings in Fire Victims
In open fires, smoke gas (fire fumes) and accelerants such as gasoline are liberated that contain numerous toxic substances depending on the material that is ignited. Substances liberated in fires include toxic gases like CO, carbon dioxide, and cyanide, as well as pulmonary irritants like acrolein attached to carbon particles, aldehydes, ammonia, hydrogen bromide, hydrogen fluoride, isocyanide, nitrous gases, sulfur dioxide, hydrochloric acid, phosgene, and other more complex molecules. 1,43 Therefore, besides the direct heat-related damage to the body surface and upper airways, death in fire is often caused by mixed intoxications. Laboratory analysis is mandatory in every case of forensic fire victims. For this purpose, blood, preferentially taken from the heart, and lung tissue with respect to inhaled volatile ignitable liquids used as accelerants have to be kept in a gastight container without residual air. 55 Blood can be aspirated with a vacuum tube to avoid oxygenation of hemoglobin. Laboratory investigations should be performed as fast as possible. This procedure may help to determine whether a victim was alive and inhaling gases at the time of a fire. 55,58
Smoke and gas inhalation with subsequent respiratory failure is the leading cause of death in human fire victims 19 but also plays a significant role in animals. 18,79 Smoke contains toxic particles resulting from incomplete combustion of natural or synthetic materials like room or stable furnishings, clothing, plastics, and other materials causing chemical injury to the tracheobronchial airways and the pulmonary parenchyma. 15,18 According to experimentally controlled exposures of rabbits to smoke, the tracheobronchial epithelium is largely intact after 6 hours, but heterophilic granulocytes infiltrate the epithelium and the subepithelial connective tissue. After 24 hours, the ciliated and secretory lining cells are destroyed and the inflammatory reaction is at its maximum. However, basal epithelial cells retain their normal structure. After 72 hours, the epithelial surface is largely covered by a nonciliated, stratified reparative epithelium, causing impairment of mucociliary clearance. 82 A similar necrotizing tracheobronchitis has been observed in sheep experimentally exposed to smoke. 30 Additional lesions include pulmonary edema due to injury of the epithelial-endothelial interface and decreased surfactant synthesis. 68 Patients intoxicated by smoke and gas inhalation typically show extensive froth around the nostrils. Due to toxin-induced impaired macrophage function, bacterial colonization and pneumonia are the most frequent complication in surviving patients after 3 to 14 days. 18,45
In the following, the 2 most important gases, CO and cyanide, are discussed in more detail. CO is liberated in slow smoldering fires with inefficient combustion and is lethal for humans and all animals. CO intoxication is the main cause of death in room and house fires. CO has an approximately 250 times higher affinity for hemogloblin than oxygen, leading to anoxia or hypoxia caused by a failure of blood oxygenation. 64 It replaces oxygen, forming CO-Hb that results in severe decrease of oxygen supply of the tissues. In addition, the remaining oxygen molecules are more tightly bound to hemoglobin, augmenting the decreased oxygen supply of the tissues. 10 Furthermore, CO induces vasodilation and, thereby, systemic hypotension that exacerbates cerebral hypoxia. 86 Heart and brain are regarded as the most sensitive organs in CO intoxication. 45 Acute CO toxicity is most likely based on a combination of hypoxia, hypotension, cellular asphyxia from CO binding of mitochondrial cytochrome c, and reperfusion injury, leading to lipid peroxidation by free radicals. 39 Animals reach fatal CO-Hb levels much faster than humans because of their higher metabolic rate. CO-Hb levels between 6% and 8% result in decreased ability to concentrate; between 10% and 20%, clinical signs include mild dyspnea, shortened breath, and confusion followed by disorientation. At 20% to 40%, lethargy, gait disturbances, and electroencephalographic changes are reported. 10 Finally, central nervous system signs develop either during acute or delayed toxicity, characterized by nausea, vomiting, incoordination, and convulsions. Death is most likely the result of cardiac arrest. To be regarded as a sole cause of death, a CO-Hb concentration in the blood of about 50% is necessary. However, the laboratory results have to be interpreted with care. In cases with high-temperature exposure, such as rapid flash fires, CO-Hb content in the blood is more likely to be low or even absent, because exposure time is too short to cause changes. Therefore, in those cases, a low or negative CO-Hb content in the blood does not necessarily indicate death before exposure to fire. 41
Grossly, there may be a cherry-pink coloration of the skin, blood, and tissues, particularly musculature. This color may be better seen if blood is diluted with water and viewed against a white background. However, in individuals with severe anemia, this color change may be hardly detectable. 41 Other necropsy findings include bronchial dilatation, distension of major blood vessels, ventricular dilatation of the heart, and hypoxic necrosis of the cerebral cortex and white matter, globus pallidus, caudate nucleus, dorsal thalamus, hippocampus, substantia nigra, cerebellum, and brainstem with edema, demyelination, and hemorrhages. 10,39,86
In fires with incomplete combustion of many common synthetic substances, cyanide gas may form. This rarely represents the only cause of death, but more often it may be an additional contributing factor. 33 Cyanide binds to and inhibits the mitochondrial cytochrome oxidase and disrupts the ability of cells to use oxygen. After exposure, there is a brief stimulation of respiration followed by severe depression until convulsions, respiratory arrest, and death occur. 1 There may be a pink or cherry-red discoloration of the body similar to CO poisoning, and in rare cases, a bitter almond smell can be noticed after opening the thoracic cavity. 43 Care has to be taken in cases with advanced decomposition, because significant cyanide concentrations may be produced after death. In contrast, a postmortem decrease in the blood cyanide concentration may also occur due to binding to aldehydes. 43 Therefore, diagnostic testing should be performed immediately after sampling, because cyanide production and decrease may also continue in the test tube.
Scalding Burns
General Aspects of Scalding Burns
A scald refers to tissue damage from hot liquids. This usually involves water, such as garden hose scalding, which is a thermal scald injury in animals exposed to hot water from garden hoses that have been lying in the sun on a hot summer day, 61 but also from other hot fluids like molten rubber, tar, oil, liquid chemicals, hot gases, or steam. Damage caused by molten metal results in dry burns because the temperature is usually high. The severity of a scald depends on the duration of contact with the skin and the temperature. When hot liquids are tipped, splashed, or thrown, the duration of contact with the skin is very short because the liquid falls away under the force of gravity. Immersion scalds are characterized by a straight linear border line with the unaffected tissue. Scalds in animals develop at a fluid temperature above 48.8°C. 77 In contrast to humans, in most animals, the densely haired skin initially protects against immediate direct contact, but retention of the hot liquids by the haired skin prevents rapid draining and cooling. Often the contact area is large, allowing rapid cooling of the fluid. Compared to dry heat, lesions caused by steam and fluids occur at lower temperatures due to their higher conductive capacity.
Morphological Findings in Scalding Burns
Morphologically, scalds resemble dry burns except for the distribution of the lesions and lack of charring, carbonization, and singeing of hairs. Hot liquids typically cause sharply delineated flow lines from the liquid impact or gravity, and in cases with splashing, a trickle pattern occurs. The worst scalds develop at the initial contact area, because the distribution of the fluid over the surface allows rapid cooling so that the severity of lesions decreases along the flow lines. 45
Reversible scalding burns are characterized by hyperemia, erythema, and miliary blister formation. Irreversible lesions comprise epidermal and dermal necrosis with loss of regenerative capacity. 43 The skin appears wrinkled, the epidermis is macerated and may desquamate, and serum exudes on the surface. Scalding burns at the feet are characterized by loss of epithelium on the soles eventually with exudation, erythema, and hair loss on the lateral and dorsal aspects of the toes and normal, nonerythematous skin between the toes. 50 In severe cases of scalding, death may immediately occur due to systemic effects of shock, fluid loss, or electrolyte disturbances or delayed due to secondary systemic bacterial infections.
Thermal Inhalation Trauma
General Aspects of Thermal Inhalation Trauma
Thermal damage of airways resulting from inhalation of hot air, gases, or steam is termed thermal inhalation trauma. Particles smaller than 2.5 μm may be inhaled into the alveoli. 18 Inhaled hot particles may also cause thermal injury to deeper airways and can carry chemicals that are caustic to epithelial cells of the lung.
Animal experiments with hot air have shown that there is a marked temperature decrease from the oral cavity to the bronchi. For example, hot dry air of 350°C at the nostrils cools to 159–182°C at the level of the larynx and to normal body temperature at the tracheal bifurcation. Hot dry air of 550°C results in temperatures of 267–327°C at the larynx and 50°C at the tracheal bifurcation. 49 In contrast, inhaled steam of more than 100°C at the nares cools down to only 94–106°C at the larynx and to 53–94°C at the tracheal bifurcation, indicating that it is more likely than dry air to cause damage. 49
Morphological Findings in Thermal Inhalation Trauma
Thermal inhalation trauma is characterized by necrosis of the mucous membranes of the oral and nasal cavities, tongue, pharynx, larynx, trachea, and bronchi. Laryngeal, tracheal, and bronchial mucosae may be reddened and edematous or atrophic. However, in lesser degrees, only blanching of the mucosal surfaces may be present. 11 Shreds of epithelium are desquamated and epithelial cells show an elongation of the cell body and nucleus toward the lumen. Since this pattern of epithelial changes is also observed in electric injuries, 75 it was previously attributed to an electric polarization effect. 31 However, because similar observations have been made in burns caused by heat, cauterization, blunt dermal injuries, and blisters following barbiturate poisoning, 31 the pathogenesis of this changes remains undetermined. Inhaled heat causes pulmonary edema that is often visible at the nostrils as a pink-stained froth. The tongue is often protruded and burnt. Inhalation of air heated to at least 150°C results in burns restricted to the face, oropharynx, and upper airway to the larynx. Damage to the lower respiratory tract is normally prevented by laryngeal reflexes and efficient heat-exchanging mechanisms in the upper respiratory tract. Heat produces immediate injury to the airway mucosa characterized by mucosal hyperemia, ulceration, and edema of the upper airways. Severe, eventually life-threatening laryngeal edema or laryngospasm may result in airway occlusion and asphyxia. 45 Edema develops secondary to the release of oxygen-free radicals and thromboxane A2, which increase the pressure and permeability of small blood vessels. 18 Sloughing of necrotic mucous membranes may occur during the first week after heat exposure and results in obstruction of the airways due to pseudomembranous cast formation. 68 The lung shows a severe mixture of emphysematous and atelectatic areas. Histologically, neutrophils dominate the initial phase of the inflammatory reaction along the airways and are followed by macrophages. Patients dying during the first 4 days after inhalation trauma usually have necrotizing and exudative bronchopneumonia with diffuse alveolar damage and hyaline alveolar membranes. 43
Thermal Injury Caused by Microwaves
Microwaves are electromagnetic waves used in microwave ovens at a frequency of 2.45 GHz and different power stages to produce heat by agitation of molecules, particularly water. Heat production and tissue damage in an animal are directly related to the water content as well as the duration of exposition and the power of the microwaves.
At necropsy, the skin may show fragility, splitting with well-defined edges, hair and claw loss, crumpling and reddening of the tips of the pinnae, but no charring or singeing of hairs. Histological examination may show abrupt transition of affected and unaffected tissues depending on their water content; for example, there may be unchanged subcutaneous fatty tissue and coagulative necrosis of the adjacent musculature and skin. There is pulmonary congestion with or without edema, and internal organs have a cooked appearance and odor due to coagulative necrosis. 50
Local Cold Injury
General Aspects of Local Cold Injury
Local cold injury or frostbite is caused by direct freezing of tissues, cold-induced vascular damage, and tissue anoxia at dry temperatures below 0°C. It has to be differentiated from prolonged damp cold damage that does not need freezing temperatures. 41 The latter is known as “immersion foot” or “trench foot” from human cases. Interestingly, local cold injury in humans is rarely found in fatal hypothermia. 27 Local cold injury is common in captive animals in cold climates 12 but is also seen in wild animals and birds. It is fairly uncommon in companion animals, even those exposed to severe weather conditions. 89
The occurrence and severity of local cold injury depend on the acclimation of an animal to cold temperatures, 90 the thermoregulation capacity, the animal species, and the environmental conditions, like temperature, duration of exposure, direct or indirect contact with frozen material, wind, and humidity/rain. Risk factors, especially for birds, are wire caging, metal leg bands, previous injury, or aggressive bandaging with impaired blood supply. 87 In addition, a reduced general health condition or concurrent diseases, such as diarrhea with reduced plasma volume, may result in an impaired blood flow to the limbs predisposing for local cold injury. 42 Use of anesthetics in a cold environment may also predispose for local cold injury. Husbandry mistakes, especially in case of nonnative animals, might favor hypothermia and local cold injury.
Pathogenesis of Local Cold Injury
Several animal models have been established to study local cold injury, mainly with regard to pathogenesis, therapy, and prognosis (particularly to assess tissue viability after cold-induced injury and necessity for amputation). They include hairless mouse ears, depilated mouse ears, mouse tails, mouse leg muscle, mouse back, rabbit ears, rabbit feet, rabbit legs, rabbit mesenteries, rat hind limbs, golden hamster cheek pouch, and dog paws. 3 Technical conditions and investigation schemes in these models vary considerably. Due to the similarity between human and porcine skin, especially with regard to wound healing, 78 local cold injury models in miniature pigs are of particular significance. 66,67,70,72,73
The pathophysiologic process in local cold injuries is not completely understood. The breakdown of skin microcirculation and the leukocyte-endothelium interaction are assumed to play pathogenetic key roles. 21 In local cold injury, direct damage is caused by intra- and intercellular ice crystal formation and irreversible disruption of cellular structures. Cell dehydration caused by the increase of osmolality in the extracellular space results in changes in protein structures, altered membrane lipids, and lowered extracellular pH values. 3 Indirect damage is the consequence of inadequate blood supply caused by vasoconstriction, sludging of blood, endothelial injury, and thromboembolism. In addition, inflammatory mediators such as prostaglandins and oxygen free radicals are released by vascular endothelium. 67 Frostbitten rabbit ear tissue has markedly elevated levels of prostaglandin F2α and thromboxane B2, as well as increased numbers of mast cells and heterophilic granulocytes. 54 The microvascular occlusion in local cold injury is worsened by the body’s natural response to cold, termed the hunting reaction. This phenomenon is characterized by alternating cycles of vasoconstriction and vasodilation with increasing release of inflammatory mediators. Full development of local cold injury usually requires rewarming after cold exposure (reperfusion syndrome). As demonstrated in a mouse model, 3 the severity of the local cold insult can be aggravated by repeated freeze and thaw cycles in contrast to continuous freezing. Generally, a faster freezing and thawing process causes less injury. 28 It is difficult to predict the final outcome of local cold injury from early lesions because demarcation between viable and nonviable tissues occurs with a delay of weeks. 17,72,73 Furthermore, according to findings in birds, cold-associated vascular damage is not restricted to peripheral extremities but may also lead to development of coronary arterial amyloidosis, aortic atherosclerosis, chronic myocarditis, myocardial fibrosis, myocardial degeneration, cardiac microinfarcts, aseptic fibrinous endocarditis, or an endothelial hyperplasia of the atrioventricular valve. 9,87 In humans, an unusual fatal complication of local cold injury at both lower extremities is fat embolism of the lungs that may be caused by a release of fat through necrosis in the frozen body region. 24 To the authors’ knowledge, this has not been described in veterinary medicine.
Local Cold Injury—Severity Grading
There are 2 classification systems for local cold injuries. Both are based on the depth of injury to skin and underlying tissues. The 2-grade system distinguishes a superficial local cold injury involving skin and subcutaneous tissue, whereas deep local cold injury also involves muscles, tendons, and bones. 52,62 The second system classifies local cold injury clinically into 4 degrees, as follows. 62
First-degree frostbite (congelatio erythematosa) includes numbness of the affected skin area with a central white plaque. After rewarming, swelling, erythema, and pain develop. Histologically, there is reactive hyperemia in the superficial dermis, and granulocytes accumulate within blood vessels. Epidermal changes have been described in detail in experimental frostbite in Hanford Miniature pigs. 72 Early lesions include vacuolization of keratinocytes, pyknosis, and loss of keratinocyte cohesion with intercellular edema that prevails in the first week after the injury. Intermediate changes are advanced degeneration of the epidermis, which remains attached to the dermis, and accumulation of neutrophils at the dermoepidermal junction. These lesions start 48 hours after the insult and remain visible in most animals during the observation period of 2 weeks. Late changes are characterized by epidermal necrosis and regeneration. Necrosis is recognizable at the earliest after 1 week. The epithelium shows coagulation necrosis and is separated from the underlying dermis. Necrosis and regeneration may be observed simultaneously. Reepithelization starts from the border of the frostbite lesion or from beneath it when basal cells are left intact at the dermoepidermal junction.
Second-degree frostbite (congelatio bullosa) causes painful blister formation between epidermis and dermis surrounded by erythema and edema (Fig. 17). In second-degree frostbite, both epidermis and superficial dermis are injured. Frostbite blisters are mainly unicameral serum-filled cell-poor vesicles at the dermoepidermal junction. They may have a wide size range from microvesicles to large bullae and are morphologically indistinguishable from burn blisters. 57 The underlying dermis reveals hyperemia, edema, and neutrophilic infiltration. Frostbite blisters heal by resorption. The detached epidermis dries up and is scaled off. Regenerative epithelialization from the borders of the blister closes the defect. Sweat gland changes in experimental frostbite in miniature pigs comprise degeneration, necrosis, and squamous metaplasia. 70 In skin biopsies taken 15 weeks after the insult, sweat glands were often missing or decreased in number. 70
Third-degree frostbite (congelatio escharotica s. gangraenosa) is characterized by irreversible necrosis of epidermis, dermis, integumentary appendages, and subcutis. The necrotic tissue becomes dry and turns black. Finally, an eschar is formed. The lesion is not painful, because the innervation also undergoes necrosis. Adjacent to the central coagulative necrosis, a zone of inflammatory reaction is formed that becomes narrower with the development of a clear demarcation. Usually third-degree frostbite lesions require surgical intervention after a clear demarcation line between vital and necrotic tissue has developed. This may take weeks to months. Histologically, third-degree frostbite shows central coagulation necrosis of cutis and subcutis with destruction or loss of the overlying damaged epidermis. Experimentally in miniature pigs, third-degree frostbite started initially with hyperemia, edema, and leukocyte emigration followed by vascular changes. These vascular changes were not visible until 1 to 2 weeks after the experimental frostbite insult. 73 They consisted of leukocyte emigration with hemorrhage, vasculitis, degeneration of the media of arterial vessels, and thrombus formation often occluding the vascular lumina and leading to ischemic necrosis. A possible causal effect of frostbite on peripheral nerves that innervate vascular walls was suspected in a rabbit frostbite model. 81
Fourth-degree frostbite is characterized by complete necrosis (ie, dry gangrene, and loss of tissues) (Fig. 18). This severest grade of frostbite not only affects dermis and subcutis but also extends to muscles, tendons, and bones.
Additional Morphological Findings in Local Cold Injury
Recognition of local cold lesions depends on their stage, age, and the severity of damage. Knowledge of meteorologic data and the case history, especially the date, location, and condition under which an animal was found, is advantageous for the diagnostician. It has been shown in animal models of local cold injury and in spontaneous cases that there are species-specific differences regarding the localization of the frostbite. For example, blistering can be observed at the tips of the wings of raptors, 17 whereas the scaly skin of the legs of birds usually does not blister. 50,87 In small animals, ears, digits, scrotum, and tail tip are most commonly affected by spontaneous local cold injuries. In calves, hind feet, ear tips, and the distal 5 to 10 cm of the tail are prone to frostbite, and in adult cattle, the teats, 8 udder base, 50 and scrotum are affected. 16 In birds, the feet are often affected. Distal extremity necrosis in birds is usually caused either by local cold injury or by trauma. 9 Feet and feathers of ducks and other birds can freeze to the ice. 12 Wing tip edema of raptors in captivity followed by dry gangrene is suspected to be caused by local cold injury, eventually in combination with other disorders. 17 Freezing of comb and wattles may occur, especially in male birds.
Acute intravital local cold injury of porcine skin is grossly characterized by purple discoloration and subcutaneous edema and histologically by dilated, blood-filled, superficial capillaries. 50 In addition, epidermal cells are vacuolated and the dermis is edematous. Incipient accumulation of granulocytes along the endothelial lining of superficial cutaneous capillaries in the paw skin of guinea pigs develops within the first 2 to 6 hours after cold insult (–20°C). 29 In cases with demarcated ischemic necrosis without colonization of saprophytic bacteria, dry gangrene develops with a delay of days or weeks (so-called late-stage frostbite).
Scrotal frostbite is characterized by a necrotic area at the base of the scrotum. 7 In bulls, the severity of scrotal frostbite lesions is categorized depending on the size of the necrotic scrotal skin, with lesions less than 3 cm in diameter as mild and more than 75% of the scrotal area as severe. 16 The incidence and severity of scrotal frostbite acquired in 2 harsh winter periods were greater among older bulls probably because of their more pendulous, and thus more exposed, scrotums. 16 Besides dry cutaneous gangrene, testes and epididymides show atrophy of the seminiferous tubuli, loss of spermatogenic cells, necrosis, degeneration, and edema. As a consequence, severe scrotal frostbite significantly reduces the semen quality and the breeding soundness of affected bulls. 5 Adhesions of the testes to the serosal scrotal process may develop.
Interdigital web necrosis in waterfowl and leg necrosis in other avian species are common in harsh winters among captive and wild birds living outdoors. 84 Birds have developed special physiological adaptations to low temperatures like countercurrent vascular systems, 69 a rete mirabile vascular network in webbed feet, and other peripheral vascular control mechanisms, 63 but freezing temperatures may nonetheless induce local cold injury. Macroscopically, frostbitten toes and legs are dry, are hard, and often show a dark discoloration (Fig. 19). Affected joints are often not movable, may be swollen and erythematous, and show skin abrasions covered with crusted blood. There is often an irregular swollen whitish 0.5- to 1.0-cm band between the frostbitten and the unaffected tissue. Distinct demarcation between necrotic frostbitten and viable tissue in birds may take 3 to 6 weeks to develop. 87 Histologically, there is usually full-thickness necrosis of skin, as well as necrosis of tendons and possibly bone. Muscular atrophy develops in the affected leg. Depending on the severity of the local cold injury and the age of the lesions, periosteal and endosteal new bone formation may occur. Tendons may show metaplastic ossifications. Secondary bacterial or mycotic infections may lead to granulomatous inflammation if the frostbitten tissue has remained viable and may mask the primary insult.
Subsequent to local cold injury, animals experience intense pain after thawing of the frosted appendage, which may cause automutilation. Furthermore, especially in flocks of poultry, secondary traumatic insults of frostbitten tissue are common, such as from cannibalism. In humans, local cold injury is known as one possible cause of acroosteolysis with brachyonychia. 14 Similarly, destructive osteolytic changes to the distal phalanges may induce deformation of claws in animals. Deformed claws and stunted pinnae in a young wild boar in late spring were observed after a harsh winter and were most likely caused by local cold injury (Figs. 20–22). Acroosteolysis of the third phalanx has been previously described in Danish Landrace pigs as a consequence of vasculitis but without a history of cold injury. 2 Histological findings in Danish Landrace pigs were comparable to immune-mediated phenomena of acroosteolysis, such as in porcine erysipeloid or allergic acroosteolytic conditions in humans (Raynoud syndrome). These conditions should be considered a differential diagnosis to cold injuries.
As a long-term consequence, tumors may develop at the site of former local cold injury. In cattle, the occurrence of papillomas and squamous cell carcinomas was observed at the site of freeze branding with liquid nitrogen, and squamous cell carcinomas developed in sheep. 91 Cauliflower-like growth of papillomas was seen 8 to 12 weeks after branding in young animals, whereas cases of squamous cell carcinoma associated with ulceration and bleeding occurred in older cows and sheep. Therefore, local cold injury should not be neglected as a possible factor for tumor promotion, a fact that has been known for quite a long time. 6 In humans, there are several case reports of squamous cell carcinomas arising in old frostbite lesions. 13,38,65 With respect to squamous metaplasia in sweat glands of miniature pigs subsequent to experimental local cold injury, 70 it seems possible that squamous cell carcinoma may originate from both metaplastic sweat gland and epidermal squamous epithelium.
Cryoglobulinemia and cryofibrinogenemia are rare diseases in humans and animals and are caused by reversible intravascular precipitation of immunoglobulins in blood vessels exposed to cold. Precipitation of cold-reacting immunoglobulins or immune complexes results in infarction and leads to lesions in the skin (cutaneous cryopathy) and multiple organ systems. Cutaneous lesions include a bluish to white discoloration, ulceration, and/or dry gangrene in severe cases. Distal extremities, including pinnae, tail tip, paw pads, and nose, are most commonly affected. 23
Chilblains (pernio, perniosis) are painful erythematous macular or papular lesions in humans mainly with acral localization due to acute or repetitive exposure to near-freezing cold and wet conditions. Histopathological findings are unspecific and comprise occasional necrosis of keratinocytes, dermal periglandular infiltrates, and edema. Chilblains may be primary or idiopathic, or secondary to an underlying connective tissue disease, monoclonal gammopathy, or cryoglobulinemia. The differential diagnosis includes vasculitis, acral lesions of systemic lupus erythematosus, and embolism. A skin biopsy may help to rule out these disorders, but the histopathology of chilblains is nonspecific. 22 In domestic animals, a chilblain syndrome was suspected as the cause of an itchy skin lesion at the tail tip of dogs that frequently became ulcerated often after automutilation. 32
As clinical differential diagnoses of local cold injuries, several disorders have to be considered, including chemical burns, toxic epidermal necrolysis, erythema multiforme, bullous autoimmune diseases, vasculitis, and ischemic or pressure necrosis. 23 Formation of ice crystals with its detrimental effects on cellular integrity also occurs in carcasses frozen after death. 31 This should not be mistaken for an intravital local cold insult. However, purple discoloration of skin and histologically engorged hyperemic capillaries in the dermis are missing in postmortem freezing. 71 Most chemical burns are of partial epidermal thickness, particularly in areas where the epidermis is thick and may not penetrate the follicular epithelium beyond the depth to which the adjacent dermis is affected. The irritating substance damages the skin by direct toxic action, causing cellular damage. Rarely, chemical burns cause full-thickness epidermal lesions with necrosis of underlying dermal or subcutaneous structures. The superficial necrosis may be bordered by zones of parakeratosis. This may be the result of dilution of the offending chemical in the peripheral areas of exposure. 23 Therefore, a rim of parakeratosis around the lesion may be an important diagnostic hint for a chemical burn.
Primary vasculitis and secondary vascular inflammation may lead to tissue damage that can mimic local cold injury and burns since fibrinoid degeneration of the wall of small- and medium-sized arterioles, as well as occasionally fibrin thrombi, has been described in miniature pigs with severe frostbite. 73 In contrast, generalized vascular diseases are usually associated with severe systemic illness, and biopsies taken from other body parts will reveal vascular lesions.
Concluding Remarks
Forensic questions concerning dry and wet heat injury, inhalation trauma, exposure to microwaves, and cold injury represent relatively infrequent requests in diagnostic veterinary pathology. Besides detailed information about the circumstances under which the animal was found, a thorough gross and histological investigation must be performed with respect to the particular patterns of lesions that may occur in thermal injuries. The diagnostic pathologist should be aware of necessary additional investigations and adequate preservation of suitable samples. Frequently, questions about cause and prognosis have to be answered, and they might have far-reaching consequences. A well-trained and experienced veterinary pathologist should be able to handle even complex forensic cases, but they require a very different approach, and one should consider the history, read the submission form with care, pay especial attention to the request, and document and perform the necropsy with great care. Moreover, conclusions with respect to cause and consequences should consider various factors and differential diagnoses.
Footnotes
Acknowledgements
We thank K. Schöne for drawing Figure 1; Prof A. Mendez, University of Cordoba, Spain, for providing Figure 8; Dr C. Pötz, Hemer, Germany, for providing Figure 9; and Dr M. von Keyserlingk, LAVES, Hannover, Germany, for providing Figures 14 and ![]() . We are grateful to Virbac Co., Bad Oldesloe, Germany, for providing transponder microchips, and S. König and H. Janßen for performing the transponder experiments.
. We are grateful to Virbac Co., Bad Oldesloe, Germany, for providing transponder microchips, and S. König and H. Janßen for performing the transponder experiments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.