
Abstract
Pulmonary hypertension is a well-known though poorly characterized disease in veterinary medicine. In humans, pulmonary veno-occlusive disease (PVOD) is a rare cause of severe pulmonary hypertension with a mean survival time of 2 years without lung transplantation. Eleven adult dogs (5 males, 6 females; median age 10.5 years, representing various breeds) were examined following the development of severe respiratory signs. Lungs of affected animals were evaluated morphologically and with immunohistochemistry for alpha smooth muscle actin, desmin, CD31, CD3, CD20, and CD204. All dogs had pulmonary lesions consistent with PVOD, consisting of occlusive remodeling of small- to medium-sized pulmonary veins, foci of pulmonary capillary hemangiomatosis (PCH), and accumulation of hemosiderophages; 6 of 11 dogs had substantial pulmonary arterial medial and intimal thickening. Ultrastructural examination and immunohistochemistry showed that smooth muscle cells contributed to the venous occlusion. Increased expression of CD31 was evident in regions of PCH indicating increased numbers of endothelial cells in these foci. Spindle cells strongly expressing alpha smooth muscle actin and desmin co-localized with foci of PCH; similar cells were present but less intensely labeled elsewhere in non-PCH alveoli. B cells and macrophages, detected by immunohistochemistry, were not co-localized with the venous lesions of canine PVOD; small numbers of CD3-positive T cells were occasionally in and around the wall of remodeled veins. These findings indicate a condition in dogs with clinically severe respiratory disease and pathologic features resembling human PVOD, including foci of pulmonary venous remodeling and PCH.
Keywords
Pulmonary hypertension is a clinical diagnosis established through the documentation of pulmonary arterial (PA) pressures above established normal values. In human medicine, the first efforts to classify pulmonary hypertension (PH) subdivided the disease into 2 categories—primary or secondary—based on whether or not an underlying disease could be identified as the cause of the PH (secondary PH). 42 Pulmonary hypertension in humans is now subdivided into 5 categories: (1) pulmonary arterial hypertension (so-called primary PH), (2) pulmonary venous hypertension (PVH), (3) pulmonary hypertension associated with underlying lung disorders or hypoxemia, (4) pulmonary hypertension caused by chronic thromboembolic/embolic lung disease, and (5) pulmonary hypertension caused by miscellaneous disorders affecting the pulmonary vasculature, for example, schistosomiasis, sarcoidosis, or alveolar remodeling associated with capillary hemangiomatosis. 8 Importantly, for the purposes of this study, pulmonary veno-occlusive disease (PVOD) is recognized as a distinct cause of pulmonary venous hypertension whose clinical expression is one of severe pulmonary arterial hypertension (PAH). 8
Pulmonary veno-occlusive disease is a rare severe form of PAH in humans; the incidence of disease has been estimated at .1 to .2 cases per million individuals, accounting for roughly 10% of the cases of idiopathic PAH diagnosed in people. 19 PVOD has been diagnosed in a wide age range, from infants to adults, with some reports suggesting a higher frequency in children. 22,43,47 Clinically, PVOD can be difficult to distinguish from other severe forms of PAH. Documentation of PH with radiographic evidence consistent with pulmonary edema in the face of normal left atrial and pulmonary arterial wedge pressures—both ruling out left-sided heart failure as a cause—is highly suggestive of a diagnosis of PVOD. 20,24 PVOD tends to be much more clinically severe than most other forms of PAH, with an average survival time of 2 years following diagnosis. 19,28
The severity of the clinical disease reflects the vascular remodeling characteristic of PVOD and its predicted impact on pulmonary blood flow. As the name suggests, the disease is characterized by occlusive remodeling of pulmonary veins. This remodeling primarily affects small pulmonary veins and venules leading to upstream alveolar capillary congestion and engorgement and accumulation of hemosiderophages. In addition to the veno-occlusive remodeling, a second lesion known as pulmonary capillary hemangiomatosis (PCH) is frequently present within the lungs of PVOD patients. PCH is comprised of regions of alveolar hypercellularity that reflect increased numbers of capillary endothelial cells. 6,9,17 In addition to the alveolar distribution, foci of PCH may infiltrate into the wall of small conducting airways and into the walls of pulmonary veins, contributing to the occlusive process in some cases of PVOD. Pulmonary arterial medial hypertrophy and intimal fibrosis are also common findings within PVOD lung. In part because of the frequency of PA lesions in PVOD, both PVOD and PCH have been classified together as a subgroup of PAH in the most recent clinical classification of PH in humans. 38
In veterinary medicine, there remains a poor understanding of the breadth of causes of pulmonary hypertension and the spectrum of vascular remodeling associated with the disease. 16 Unlike in human medicine, pulmonary arterial catheterization is rarely performed to measure PA pressures in dogs; instead, such pressures are estimated using Doppler echocardiography to measure tricuspid valve regurgitation velocity as a proxy for direct measurement of PA pressures. 13,29,35,36 PAH is most often recognized in dogs as a sequela to congestive heart failure and PVH in small breed dogs with chronic mitral valve disease, secondary to heartworm infection, or associated with chronic interstitial lung disease. 15,34,39,41 Idiopathic PAH (iPAH) is recognized clinically in dogs. A study of 6 dogs clinically diagnosed with iPAH 48 identified histologic PA changes similar to those in human iPAH, including arterial medial hypertrophy and intimal thickening, with rare plexiform lesions. 48 PH developing as a result of non-cardiogenic pulmonary venous hypertension has not been described in non-human animals.
Herein we describe the gross and histologic findings in 11 dogs that died from primary pulmonary disease, with similar lesions as PVOD in humans.
Materials and Methods
Tissue Collection and Preparation
Samples of lung were collected from 11 dogs that were euthanized for progressive respiratory disease. Sections of lung were fixed in 10% neutral buffered formalin and routinely processed, sectioned at 6 µm, and stained with hematoxylin and eosin (HE) and Verhoeff van Gieson (VVG). Histologic sections and immunohistochemistry together were evaluated by one author (K. Williams).
Transmission Electron Microscopy
Formalin-fixed lung from a single case of PVOD (dog No. 1) was rinsed in 0.1 mol/L phosphate buffer, placed in osmium tetroxide (Electron Microscopy Sciences; Fort Washington, PA, USA) for 3 hours, rinsed again in 0.1 M phosphate buffer, rinsed 3 times in 30% ethanol for 10 minutes each, transferred into 2% uranyl acetate (Electron Microscopy Sciences) for 1 hour, rinsed in 30% ethanol, and dehydrated in a graded series of ethanol. The tissues were placed in propylene oxide before being embedded in DMP-30 and araldite 501 (Electron Microscopy Sciences). One-µm sections were cut on an LKB microtome and stained with Toluidine blue. Tissues of interest were sectioned at 600 angstroms, stained with uranyl acetate and lead citrate and examined on a Phillips 301 electron microscope (Phillips; Atlanta, GA, USA).
Immunohistochemistry
Immunohistochemical labeling was performed on sections of lung from dogs No. 1, 2, 3, 4, 8, 9, 10, and 11 at the Diagnostic Center for Population and Animal Health at Michigan State University. The cases included for immunohistochemistry originated in the United Kingdom (dog No. 1), Michigan (dogs No. 2, 3, 4, 9, 10, 11), and Massachusetts (dog No. 8). Briefly, representative sections of lung were incubated with primary antibodies directed against CD204 for macrophage/dendritic cells (Trans Genic Inc, Kumamoto, Japan; mouse monoclonal 1:1000), CD3 for T cells (Dako, Carpinteria, CA, USA; rabbit polyclonal, 1:200), CD20 for B cells (Neomarkers Thermo-Scientific, San Jose, CA, USA; rabbit polyclonal, 1:500), αSMA (Dako; mouse monoclonal 1:50), desmin (Dako; mouse monoclonal, 1:400), and CD31 for endothelial cells (Dako; mouse monclonal, 1:50). The process was performed using the Bond Max Automated Staining system with the Bond Polymer Detection system (Vision Biosystems, Leica, Bannockburn, IL, USA) using 3,3’-diaminobenzadine as the chromogen with hematoxylin counterstain. Phosphate-buffered saline was substituted for the primary antibody as the negative control. Normal lung from a dog that died of non-pulmonary disease served as a control for comparison.
Results
Clinical Findings
The 11 dogs included in this study represent cases from Michigan (7 dogs), Massachusetts (1 dog), California (2 dogs), and the United Kingdom (1 dog). The average age was 10.5 years, and there were 5 males and 6 females (Supplemental Table 1). Breeds represented included mixed breed (2), Golden Retriever (2), Australian Shepherd (2), and a single Greyhound, German Shepherd, Beagle, Border Collie, and Labrador Retriever. Presenting signs included acute onset of respiratory distress (9), cough (4), inappetence (4), abdominal distension (1), and progressive lethargy leading to collapse (1). Duration of clinical signs prior to presentation ranged from 1 to 21 days in 6 dogs; this information was not available in the remaining 5 cases. Chest radiographs performed in 5 dogs showed a mixed bronchial and diffuse heavy interstitial pattern most prominent in the caudodorsal lung fields. Additional radiographic findings included focal areas of alveolar disease (4) and pulmonary arterial enlargement (4). Arterial blood gas composition was analyzed in 2 dogs and showed respiratory alkalosis with severe hypoxemia. Echocardiography with Doppler was performed in 3 dogs (dog Nos. 2, 6, and 7) and showed significant pulmonary arterial hypertension (gradients of 88, 52, and 89 mm Hg, respectively; normal ≈25 mm Hg). Five dogs were euthanized within hours of presentation due to rapidly deteriorating condition. The remaining animals survived a variable amount of time, no longer than 6 months post-presentation, before being euthanized.
Gross Pathology
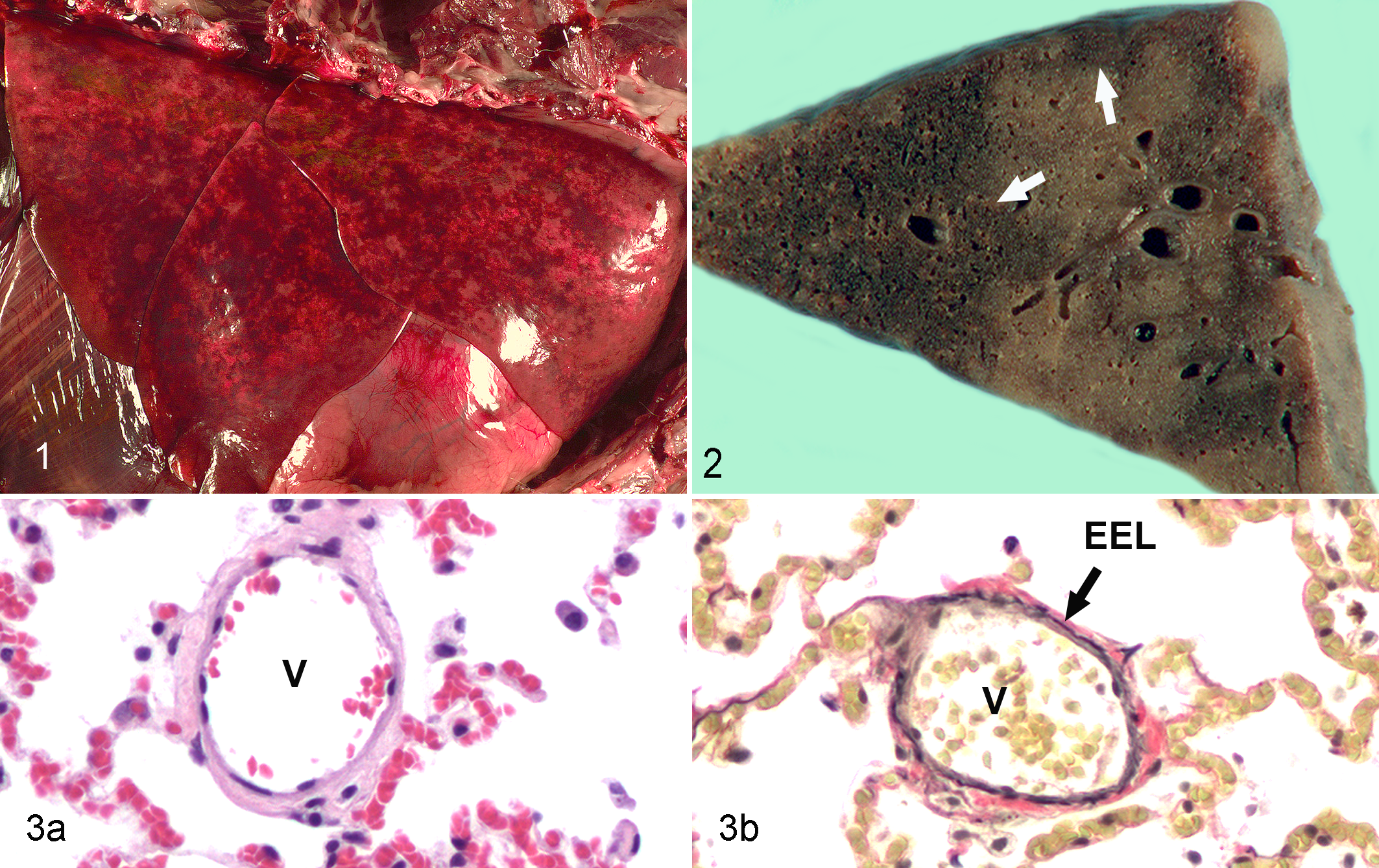
Significant gross lesions were restricted to the lungs. The lungs in PVOD dogs were diffusely moderately edematous and consolidated with a “meaty” consistency. Throughout the lungs were widespread, often discrete, foci of congestion (Fig. 1). On cut section, these foci extended well into the alveolar parenchyma and had relatively sharp borders delimiting the edge from the surrounding more normal parenchyma (Fig. 2). There was no gross evidence of pneumonia and no exudate in the examined airways. No gross evidence of underlying cardiac disease was documented in any of the dogs; compensatory hypertrophy of the right ventricle was noted grossly in 2 dogs.
Histopathology
In evaluating lungs where PVOD is suspected, it is essential to definitively distinguish between arteries and veins. In the current study, veins were identified using a combination of histologic features, anatomic localization, and Verhoeff-van Gieson staining to identify elastic laminae. Pulmonary veins were distinguished by their relatively thin tunica media and single external elastic lamina (Fig. 3); similarly sized pulmonary arteries had a thicker tunica media and internal and external elastic laminae (not shown). In addition, the small pulmonary veins most frequently affected in canine PVOD were isolated within the alveolar parenchyma, whereas most branches of similarly sized pulmonary arteries are associated with a conducting airway.
The main histologic findings (Fig. 4, Supplemental Table 2) consisted of venous remodeling with or without arterial remodeling, segmental congestion of alveolar capillaries, foci of PCH, and increased numbers of alveolar macrophages that frequently contained cytoplasmic hemosiderin. Occasional small foci of acute alveolar injury with fibrin exudation and hyaline membrane formation were noted in some of the dogs.
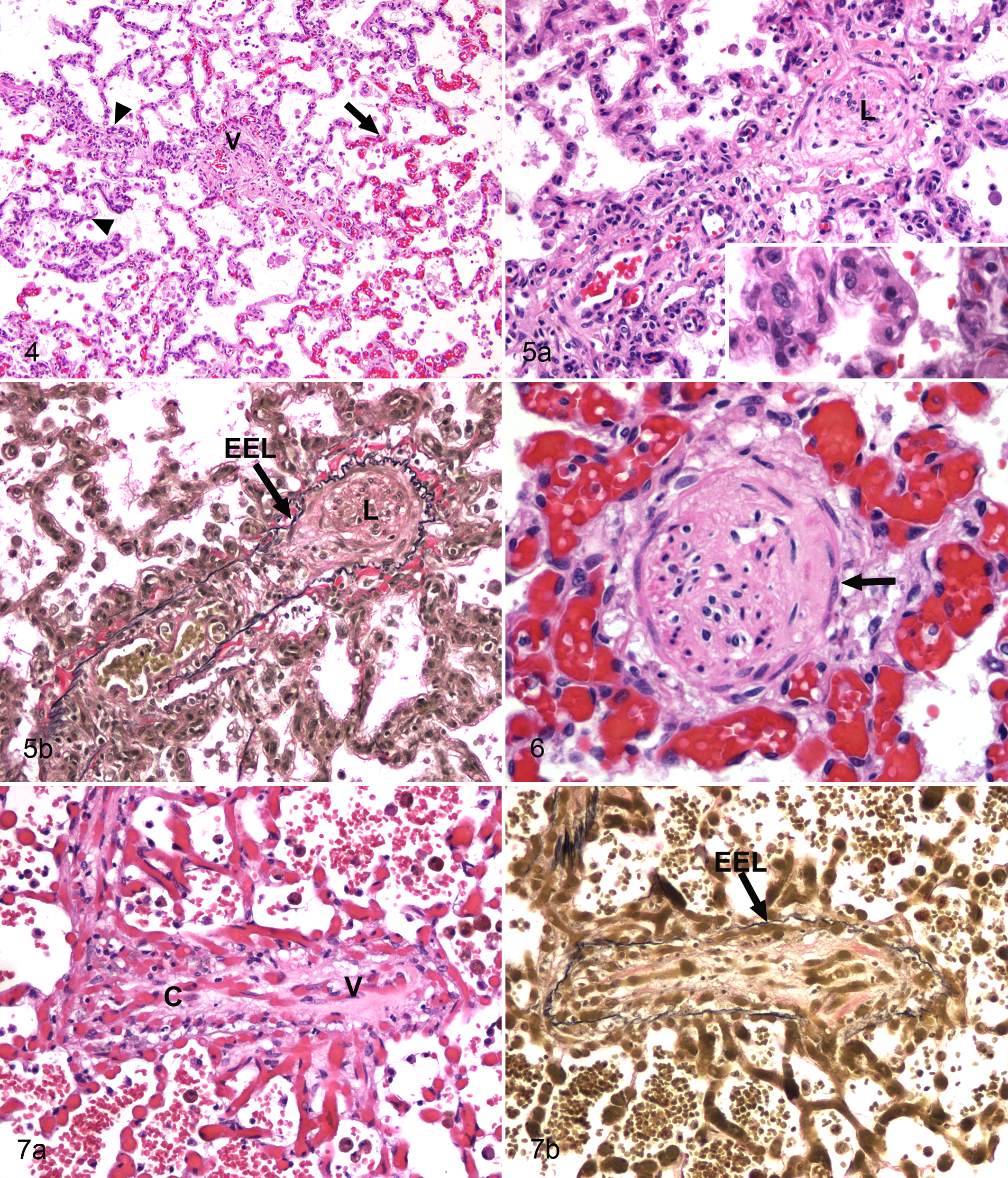
The venous remodeling in canine PVOD (11/11 dogs) mostly affected post-capillary venules and small (up to approximately 300 µm) intra-parenchymal veins. Not all pulmonary veins and venules examined were affected; some regions of the lung had few abnormal veins. The lumen of affected veins was partially to completely occluded by densely to loosely organized collagen, and there were numerous plump spindle cells within the intima (Fig. 5). When the venous lumen was evident, it was markedly reduced and tortuous. In small numbers of veins, well-organized bundles of smooth muscle cells were arranged parallel with the long axis of the vessel (Fig. 6). In a single dog (No. 5), the occlusive process developed primarily through the infiltration of vein walls with numerous small capillaries (Fig. 7). This case also had very large thin-walled dilated vascular structures without evident elastic lamina present around medium-sized pulmonary veins (not shown). In the most severely affected vessels, veins were replaced by collagen, and their identity could only be determined in the VVG-stained sections (not shown).
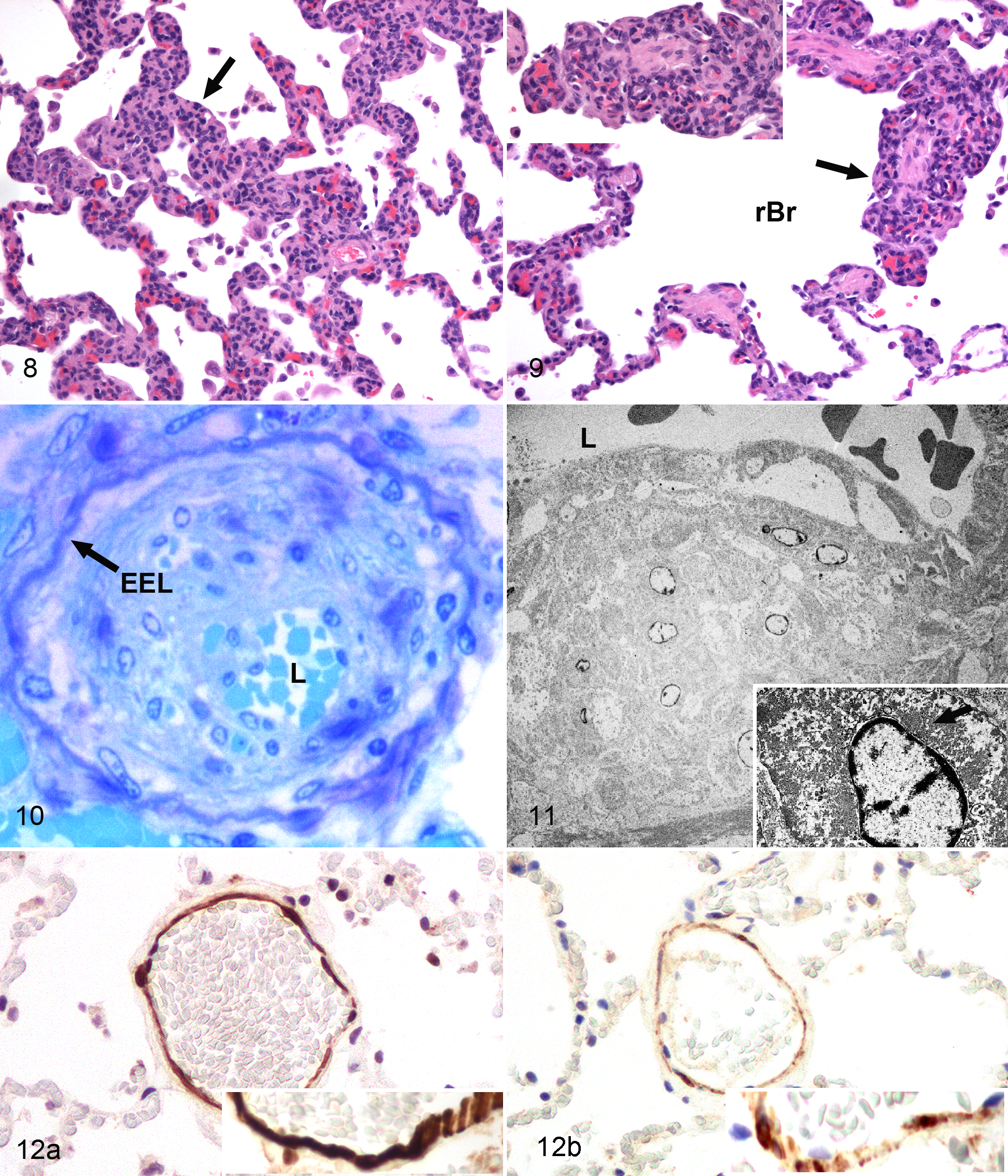
Foci of PCH were found in 11 of 11 cases. The affected alveoli were often localized around remodeled veins (Fig. 4); the hypercellularity of alveolar septa appeared to result from increased numbers of plump endothelial cells (Fig. 8). Frequently the foci of PCH were associated with segmental congestion of alveolar capillaries. In many cases, capillary profiles were evident within the wall of respiratory bronchioles, where they infiltrated around the smooth muscle bundles and beneath the luminal epithelium (Fig. 9) as well as within the walls of pulmonary veins. PCH was the main histologic finding in 2 dogs; in these cases, veno-occlusive remodeling of post-capillary venules was identified in the VVG-stained sections.
Pulmonary arterial remodeling was a significant finding within the lungs of 6 of 11 PVOD dogs (Supplemental Table 2). As with the venous disease, smaller pulmonary arteries were more commonly affected. The arterial lesions differed from those present in the veins, consisting of eccentric to concentric intimal expansion by increased extracellular matrix and moderate to marked medial hypertrophy.
Venous Ultrastructure
Transmission electron microscopy (TEM) was performed on a single case (dog No. 1). The intima of pulmonary veins was expanded by numerous smooth muscle cells and collagen (Figs. 10, 11).
Immunohistochemistry
In normal canine lung, expression of αSMA and desmin was evident within the smooth muscle cells of the tunica media of arteries and veins (Fig. 12); there was greater intensity of labeling for αSMA than desmin in these cells. Importantly, there was little expression of either of these proteins within the normal canine alveolar septum (Fig. 12). In cases of PVOD, the spindle cell component within the intima of the remodeled veins labeled intensely with antibodies against αSMA (Supplemental Figs. 1–2); desmin expression was also present, though less prominent than αSMA (not shown). αSMA immunolabeling highlighted the well-organized bundles of smooth muscle cells running parallel with the long axis of the veins as noted previously (Fig. 6, Supplemental Fig. 2). There was marked expression of αSMA within spindle cells in the alveolar septa in the PVOD lung. This expression was especially prominent within the foci of PCH (Supplemental Figs. 1–3) but also was increased within non-PCH alveoli compared to the control lung (Supplemental Fig. 3). Similar though less intense expression of desmin was also detected in these areas of the alveolar septa (not shown).
CD31 expression in normal canine lung was restricted to the plasma membrane of endothelial cells of arteries, veins, and capillaries (Supplemental Fig. 4). In PVOD, the expression of CD31 was markedly increased within the foci of PCH (Supplemental Fig. 5a) and also highlighted the endothelial cells lining the reduced lumen of remodeled veins (Supplemental Fig. 5b). In the dogs with capillary infiltration into pulmonary veins and airways, CD31-positive endothelial cells lined these vascular spaces (not shown).
Immunohistochemistry for CD20 identified small numbers of B cells within PVOD lung (not shown). There was no apparent pattern to their distribution and no association between these cells and the remodeled veins or foci of PCH. CD3-positive T cells were present scattered throughout the PVOD lungs. In addition, some remodeled veins had small numbers of CD3-positive cells at the periphery of the remodeled vessel as well as within the venous wall (Supplemental Fig. 6). Immunohistochemistry for CD204 identified macrophages throughout the PVOD lung, but this was not co-localized with the remodeled vasculature (data not shown). There was no labeling of the lung in the negative control slides for any of the antibodies.
Discussion
Pulmonary veno-occlusive disease was first reported in human medicine in 1934 after a 48-year-old baker in Germany died from a progressive respiratory disease characterized by dyspnea, pulmonary edema, and cyanosis. 11 It wasn’t until approximately 40 years after this initial description that PVOD was classified as a distinct and serious form of PH in humans. 8 Herein we provide the first description of a condition in adult dogs that shares the pathology and many clinical features with PVOD in people. Affected dogs experienced respiratory distress, which, based on our small cohort of cases, appears to be associated with severe PAH. The lung changes consist of severe and widely distributed veno-occlusive remodeling affecting post-capillary venules and small veins; this venous remodeling is, in part, characterized by smooth muscle cells occluding the vascular lumen. In addition, most dogs had alveolar foci consistent with PCH as well as remodeling of pulmonary arteries. Based on our findings, lung vascular remodeling with lesions similar to PVOD in humans occurs in dogs. The cause(s) of the vascular disease remains unknown.
The clinical presentation of PVOD in this series of dogs suggests that in most instances this is a rapidly progressive and severe disease leading to death or euthanasia. In people with PVOD, the clinical presentation is usually reported to be more gradual and initially is indistinguishable from other causes of PAH. 19,21 Rarely, human patients with PVOD experience hemoptysis as well as rapid decline and death that is more similar to the canine disease. 17 In canine PVOD, the disease has thus far only been documented in adults (mean age = 10.5 years) while in humans there is more variability in the age of affected individuals. Most studies of PVOD in people suggest that it is more prevalent in children and young adults, although there are well-documented cases developing in older individuals. 10,12,19,47 With the recognition of PVOD in dogs, it will be important to carefully assess the lungs of younger animals for similar pulmonary vascular pathology.
PVOD in humans is considered to be a rare form of severe PH, with an estimated incidence of approximately 10% of unexplained PH cases, or .1 to .2 cases per million individuals. 38 The incidence of PVOD in dogs is not known, but there is reason to think that it may be higher in the canine population than in people. Given that this is the first report of PVOD in dogs, it seems reasonable to assume that a significant number of cases may be unrecognized or misdiagnosed. Substantiating this assertion, 2 of the dogs in this study were initially diagnosed by pathologists as having chronic congestive heart failure based on the presence of hemosiderophages in the lung. More work is necessary to define the clinical presentation to facilitate prospective identification of cases and to aid in the clinical management of canine PVOD. It will be especially important to document PA pressures when possible in affected animals to expand our understanding of the pulmonary pathophysiology in canine PVOD.
Histopathology has played an important role in classifying phenotypes of human PAH. 38 Pulmonary arterial hypertension, regardless of the underlying cause and pathogenesis, is histologically characterized primarily by arterial medial hypertrophy (especially at the level of pre-capillary arterioles) and varying degrees of intimal fibrosis. 6,27 Complex lesions are typified by the development of plexiform arteriopathy, which consists of foci of arterial mural destruction and the development of associated perivascular endothelium-lined channels. These complex lesions are less common than the aforementioned primary lesions and associated with more severe clinical disease. 27,28 Importantly for the purposes of this study, venous remodeling is not a feature of iPH in humans, although arterial remodeling is often noted in human PVOD. 6,45 In the latest clinical classification of PH in humans, PVOD and PCH are placed within their own subgroup of PAH based in part on the frequency of PA remodeling in these diseases. 3,38 As in human PVOD, pulmonary arterial medial hypertrophy and intimal thickening were relatively common in small- to medium-sized PA in canine PVOD. The arterial changes in PVOD are assumed to be the result of increased arterial pressures that develop secondary to the downstream venous lesions. 45 This mechanism is unproven, and there are some who consider the venous and arterial lesions to reflect a continuum of vascular pathology affecting vessels on both sides of the capillary bed. 17
Efforts to classify PH in veterinary species, beyond documenting the clinical and hemodynamic features of PH, are lacking to date, and there is scant information correlating pulmonary vascular lesions with severity of clinical disease in veterinary medicine. Although PH is well recognized clinically in dogs, there is little information describing the pulmonary vascular histopathological changes of such patients. A retrospective study described the pulmonary arterial pathology in 6 dogs that were clinically classified as idiopathic pulmonary hypertension. The most frequent lesions were PA medial hypertrophy and intimal thickening as well as occasional complex lesions. 48 As described in human PH patients, in this small group of dogs, the presence of complex lesions was associated with more severe clinical disease; venous pathology was not noted in this study. 48
The histopathology of canine PVOD is very similar to the human disease and is central to definitively identifying the disease. In both canine and human PVOD, the diagnostic hallmark is the widespread remodeling of small- to medium-sized pulmonary veins. In human PVOD, remodeling of pre-septal venules is characteristic and a necessary finding to make the histologic diagnosis. 6 In canine PVOD, small- to medium-sized intra-parenchymal branches of pulmonary veins were the most commonly affected vessels. While the venous remodeling was widespread within individual sections of the lung, normal veins could still be detected, and in some lung regions most examined veins were essentially normal. This finding is consistent with reports of human PVOD where 10% to 90% of veins had histologic features diagnostic of the disease. 17,44 Therefore, in suspect cases of PVOD, it is important that the pathologist collect and histologically examine multiple sections from both lungs to maximize the opportunity to identify the characteristic vascular lesions.
The occlusive remodeling in pulmonary veins of canine PVOD is primarily the result of bundles of smooth muscle cells, although in an individual dog, the venous occlusion was the result of an apparent in-growth of capillary profiles. The identity of smooth muscle cells was confirmed through the use of αSMA and desmin immunohistochemical labeling as well as TEM on veins from a single PVOD dog. Similarly, in human PVOD, αSMA-positive cells can be found as a component of the vascular remodeling in the disease. 6,45 The origin of the smooth muscle cells in the remodeled veins is unknown in either the human or canine disease. Initial reports in human medicine suggest they migrate into the vasculature from the tunica media, 45 although this remains speculative at this time. Myofibroblasts also express αSMA and can express desmin and could be considered as an alternative cell contributing to the occlusive process, although the morphology of the cells in PVOD-affected veins makes this less likely. Studies in a hypoxia-induced model of PAH in mice have determined that the smooth muscle cells in the distal arterioles originate from preexisting smooth muscle cells rather than from other cell types such as myofibroblasts or pericytes. 37
Foci of pulmonary capillary hemangiomatosis—regions of alveolar hypercellularity determined to be proliferative capillaries—were the second most common finding within the lungs of canine PVOD. PCH in canine PVOD was present mostly within the alveoli but also surrounded and infiltrated into the walls of conducting airways, small veins, and venules; this distribution is similar to what is reported for PCH in human PVOD. 9,17 Immunohistochemistry demonstrated increased CD31, αSMA, and desmin labeling in foci of PCH, suggesting expansion of both endothelial cell and contractile interstitial cell populations. CD31 immunolabeling also confirmed the phenotype of capillary profiles within airway and vessel walls in the canine lung affected by PVOD and PCH. The ability of capillary endothelial cells in PCH to proliferate and infiltrate into airways and blood vessels initially led investigators to suggest that PCH is a low-grade vascular neoplasm. However, because there is no evidence of clonality and the cells are cytologically bland, PCH is no longer considered a neoplasm. 25
As noted previously, PVOD and PCH have been grouped together in the most recent clinical classification of PH in people, 38 although there is an ongoing discussion as to whether or not PVOD and PCH are 2 distinct diseases. The largest study to address this question examined 35 cases of PVOD and 5 of PCH and detected PCH in 73% of PVOD cases, leading the authors to conclude that most cases of PCH likely reflect underlying unrecognized PVOD. 17 In our study, all PVOD dogs had foci of PCH; in 2 cases, PCH was the predominant finding, and it was only after evaluation of VVG-stained lung that remodeled veins were identified. Therefore, the findings in these cases of canine PVOD are in agreement with the contention in human medicine that PVOD underpins the development of PCH. 17
Within canine PVOD lung, there was marked widespread distribution of αSMA- and desmin-expressing spindle cells in the alveolar septa that was especially prominent in areas of PCH. Similar cells expressing these proteins could only be found isolated in the interstitium between adjoining alveoli in normal canine lung. The cell morphology and location of these cells suggests that they could be interstitial myofibroblasts or pericytes. Pericytes are specialized mesenchymal cells closely apposed to endothelial cells in the microvasculature, 5 while myofibroblasts are αSMA-expressing spindle cells that can be induced in the lung under a variety of disease states, including pulmonary hypertension. 14 Pericytes are well known to play a role in vasoproliferative processes, 1,2,5 thus the co-localization of these cells in the foci of PCH suggests this may represent pericyte upregulation in support of capillary endothelial cell proliferation in the foci of PCH. The mechanism(s) for the induction of these cells—whatever their phenotype—within the alveolar septa may be in response to elevated vascular pressures within the capillary bed. αSMA-positive, desmin-negative spindle cells were identified as myofibroblasts in the lungs of human patients with post-capillary PH (including PVOD patients) but not in those with pre-capillary PH, suggesting that such cells are induced by the mechanical stretch caused by capillary congestion in post-capillary PH. 14
The cause(s) of canine PVOD is not known. Venous remodeling similar to that seen in PVOD has been noted in diseases that would be expected to lead to increased pulmonary venous pressures, including mitral valve stenosis and fibrosing mediastinitis in humans and in the lungs of horses experiencing severe exercise-induced pulmonary hemorrhage. 3,46 No coincidental left-sided cardiovascular disease was identified in the dogs in this study, suggesting that canine PVOD is not the result of sustained elevation in left atrial pressure.
It is possible that the vascular remodeling in canine PVOD is a common endpoint from a variety of possible causes. Potential causes suggested for human PVOD include genetic factors, exposure to toxins (especially alkylating chemotherapeutic agents), viral infections, and immune-mediated mechanisms. 19,31 A genetic basis has been documented in familial forms of the human disease. Mutations in the bone morphogenetic protein-2 receptor are associated with up to 50% of familial forms of PAH and have been identified in a small subset of human PVOD. 4,32 More recently, 13 families in France with a history of PVOD in at least 1 family member were determined to have mutations in the gene encoding the serine-threonine kinase EIF2AK4. 7 The lack of an apparent breed predilection for canine PVOD in our study does not suggest a genetic basis for the canine disease at this time.
Inflammatory and immune mechanisms are increasingly implicated in the pathogenesis of PAH, 30,40 though their role in PVOD is not known. PVOD patients but not PAH patients had decreased numbers of circulating cytotoxic lymphocytes and natural killer T cells and increased numbers of natural killer cells within their peripheral blood. 26 In addition, the amount of granulysin in these cells was decreased while free serum granulysin levels were increased, suggesting immune dysregulation as a factor in the pathogenesis of human PVOD. 26 As a first step toward investigating a role for immune mechanisms in canine PVOD, we utilized immunohistochemical labeling to look for co-localization of T cells, B cells, and macrophage/dendritic cells with the remodeled vasculature in canine PVOD. There was no evidence for such a relationship for B cells and macrophage/dendritic cells, but there were small numbers of T cells surrounding and within the wall of occasional remodeled veins. This limited study does not prove a role for T cells in the pathogenesis of canine PVOD but does warrant additional investigation.
Animal models to investigate the biology of PVOD had not been developed until recently. The transcription factor Erg is involved in a number of functions related to blood vessel formation and binds to the gene Aplnr, which is known to be expressed in venous endothelium. 23,33 Recently, a murine model of PVOD was developed by homozygous deletion of Erg. 18 Homozygotes died between embryonic day 16.5 and 3 months of age with severe pulmonary venous occlusion. 18 Furthermore, lungs from PVOD patients had decreased levels of Erg and Aplnr, suggesting that this pathway may provide a point of disruption in cell signaling within veins that can play a role in the development of PVOD. 18 Canine PVOD may provide a spontaneous model to investigate this and other potential pathways important in the development of the veno-occlusive remodeling in PVOD.
In summary, we have identified a form of pulmonary vascular remodeling in dogs with pathology similar to PVOD in humans. The lung lesions are comprised of severe and widely distributed veno-occlusive remodeling affecting post-capillary venules and small veins that was, in part, the result of smooth muscle cells and collagen occluding the vascular lumen. In addition, all dogs had foci consistent with PCH, as well as remodeling of pulmonary arteries, and numerous alveolar hemosiderophages. The cause and pathogenesis of this disease remain to be determined.
Footnotes
Acknowledgments
We would like to acknowledge Dr. Carol Reinero for her helpful comments during the preparation of this article. We would also like to acknowledge the various veterinarians and pathologists who contributed cases to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.