
Abstract
Equine odontoclastic tooth resorption and hypercementosis (EOTRH) is a painful progressive condition of older horses that involves multiple teeth, including canines and incisors. EOTRH is uncommonly recognized by veterinary pathologists and in some cases may be misdiagnosed as cementoblastoma. The cause is unknown. The goals of this study were to describe the histopathologic features of EOTRH in 17 affected horses from the United States and to increase awareness of this condition. Samples ranged from affected tooth to the entire rostral mandible and maxilla. Affected teeth exhibited cemental hyperplasia and lysis. The marked proliferation of cementum in severe cases caused bulbous enlargement of the intra-alveolar portions of affected teeth. Several teeth contained necrotic debris, bacteria, and plant material in the regions of cemental lysis. All horses exhibited dentinal lysis in at least affected tooth, and several contained necrotic debris in these regions. Endodontic disease was often present with inflammation, lysis, necrotic debris, fibrosis, and/or a thin rim of atubular mineralized tissue in the pulp cavity. Periodontal disease was a common feature that was primarily characterized by moderate lymphoplasmacytic inflammation. Resorption with secondary hypercementosis appears to begin on the external surface of the teeth rather than within the pulp cavity. Distinguishing EOTRH from other diseases requires a complete history that includes the number and location of affected teeth, a gross description of regional hard/soft tissue health, and radiographic findings.
Keywords
Equine odontoclastic tooth resorption and hypercementosis (EOTRH) is a painful condition of older horses that primarily involves the canine and incisor teeth. 1,4,21 This condition was first described by Klugh in 2004. 9 EOTRH has been described in Europe, 21,22 the United States, 1,4 and, most recently, Australia. 11 The cause is unknown. Since disease begins in the reserve crown, early cases may be asymptomatic or exhibit only subtle changes, such as tooth discoloration, small pits at the gingival margin, or mild to moderate gingival hyperemia. Horses with advanced disease often present for dysphagia, painful and edematous gingivitis, suppurative periodontal draining tracts, and/or tooth fracture. 1,4
EOTRH is characterized by concomitant tooth resorption and hypercementosis that typically progresses from the third to first incisors. The canine teeth may also be affected with or without concurrent disease of the incisors. 4,6,21 Clinical findings can include enlarged submandibular lymph nodes, decreased incisor angle, prominent juga (depressions between the ridges of bone formed by roots in the alveolar process on the mandible or the premaxilla and maxilla), loss of dental papillae, gingival and mucogingival fistulas, severe inflammation (including purulent drainage, calculus, and feed accumulation), missing teeth, gingival hyperplasia or recession, bulbous enlargement of dental structures, tooth mobility, supragingival regions of dental resorption, and resorptive lesions under excessive calculus deposition on the canine teeth of older horses. 4 The degree of resorption versus hypercementosis can vary among affected teeth, and 3 patterns have been described: predominant tooth resorption, predominant hypercementosis, and combined tooth resorption and hypercementosis. 4 Tooth resorption is the breakdown/destruction and subsequent loss of dental hard tissue and periodontium by odontoclasts, cementoclasts, and osteoclasts. In cases where hypercementosis is the predominant feature, there is often bulging of the incisive bone or the rostral mandible with or without gingival recession and/or gingivitis. 4,6,21 While advanced EOTRH leads to varying degrees of tooth mobility, fracture, and avulsion, incisors with significant hypercementosis are generally immobile and not affected by fistulation in early stages. 4,6 Radiographically, varying degrees of tooth resorption and hypercementosis are present (Fig. 1). The hypercementosis often appears as radiopaque bulbous enlargements of the apex in more advanced cases. 1,4,7 Tooth fracture, changes in the width of the periodontal ligament (PDL) space, alveolar bone lysis, and osteitis may also be evident. 1,4 No treatments have been effective at slowing down the progression of the disease, and current recommendation is extraction of affected teeth. 16
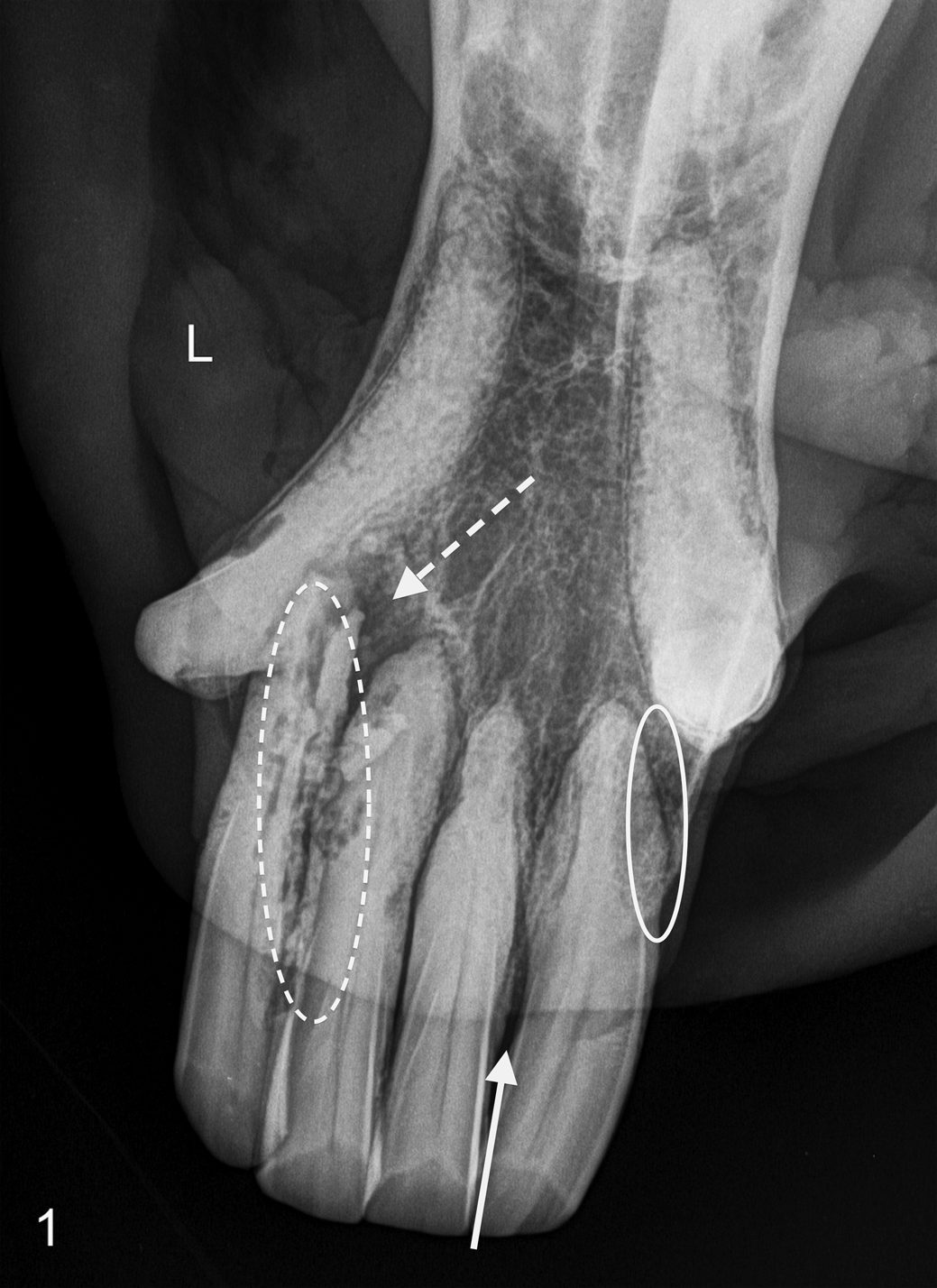
Equine odontoclastic tooth resorption and hypercementosis, teeth, horse. Intraoral bisecting angle radiograph of the mandibular incisors and canine teeth in a horse with clinically apparent tooth resorption. Both third incisors are missing. The radiograph demonstrates the classic signs of equine odontoclastic tooth resorption and hypercementosis: missing teeth, cemental thickening (solid oval), tooth resorption (dashed oval), apical osteolysis (dashed arrow), and attachment loss (solid arrow). L, left.
Grossly, hypercementosis can be misdiagnosed as dental calculi, and in severe cases, a misdiagnosis of cementoblastoma can be made. 10 If resorption is the primary lesion, a misdiagnosis of tooth root abscess can occur. Both of these occurrences generally happen when a single tooth is submitted for histopathology without adequate history or supporting materials (radiographs, gross description of surrounding tissue and teeth, etc). Thus, EOTRH is likely underdiagnosed. To diagnose EOTRH, it is important to inquire about regional hard and soft tissue health and, if possible, evaluate multiple affected incisors and canine teeth. Intraoral radiographs accompanying specimen submission make the diagnosis of EOTRH even clearer. The goals of this descriptive study were as follows: (1) to classify the histopathologic features of EOTRH in 17 affected horses from the United States, (2) to compare the histopathologic lesions to those described in European horses, and (3) to increase awareness of this condition among equine practitioners and veterinary pathologists.
Material and Methods
Histopathology was performed as a portion of a larger study looking at the complete clinical picture of horses affected by advanced stage (16 of 17) and early stage (1 of 17) resorption and hypercementosis with radiographic confirmation. Histopathology submissions were from October 2008 through October 2011 and included 1 to multiple extracted incisors or canine teeth from 15 live horses and en bloc excisional submissions of the rostral mandible and maxilla from 2 horses that were euthanized (Suppl. Table 1). The modified Triadan system was used for numbering equine dentition. 5 Two premolars, 1 from each of 2 horses (Nos. 12, 15), were also submitted. All samples were received in formalin. Each sample was photographed, briefly examined grossly (R.C.S.), and placed in fresh 10% neutral buffered formalin. Some teeth and jaw sections had been previously sectioned into multiple transverse sections, and others were submitted whole. Large en bloc jaw specimens were sectioned with a band saw to approximately 1-cm thickness to speed decalcification. Samples were routinely decalcified in RapidCal (BBC Biochemical, Mount Vernon, WA, USA) for an average of 1 to 2 weeks. Next, the samples were trimmed into 3-mm-thick transverse sections and placed into cassettes. The cassettes were rinsed in cold gentle-running water for 2–4 hours and then placed in 10% neutral buffered formalin for at least 48 hours before they were routinely processed, embedded, sectioned, and stained with hematoxylin and eosin.
The histologic sections were examined via light microscopy by a board-certified veterinary pathologist (R.C.S.) and classified as follows: cemental hyperplasia, cemental hypoplasia, lytic cemental/dentinal lesions, necrotic debris in the cementum/dentin, bacteria in the cementum/dentin, plant material in the cementum/dentin, pulp lesions (inflammation, lysis, necrosis, bacteria, plant material, and fibrosis), PDL lesions, gingival lesions, and alveolar bone lesions. Enamel cannot be evaluated in decalcified specimens. When bacteria were suspected in hematoxylin and eosin sections, Gram staining was performed but did not always identify the bacteria due to their loss during sectioning.
Results
The study population (Suppl. Table 1) consisted of 15 geldings, 1 stallion, and 1 mare that ranged in age from 10 to 32 years, with an average age of 21.7 years. There were 9 Thoroughbreds, 2 Warmbloods, 2 Quarter Horses, 1 Arabian, 1 Hanoverian, 1 Holsteiner, and 1 Appaloosa. Horses were evaluated by veterinarians with advanced training in equine dentistry, and samples were submitted from a variety of regions throughout the country. Samples received included extracted incisors (n = 18), extracted canines (n = 3), extracted premolars (n = 2), and en bloc maxillary/mandibular samples with incisors embedded in tissue (n = 2). Multiple teeth were submitted for 6 horses, including the 2 horses where en bloc maxillary/mandibular samples were submitted. The tooth number was not always indicated on the submittal form.
Most extracted incisors and 2 extracted canines (No. 14) were submitted intact. Grossly, all submitted extracted incisors and 1 affected canine (No. 3) had irregular and roughened surfaces, to varying degrees, with very small amounts of adhered soft tissue. Two incisors (Nos. 7, 9) exhibited marked bulbous enlargement of the apical portion; 2 incisors (No. 6 and 1 tooth from case No. 8) exhibited moderate apical enlargement; and 3 incisors (2 from No. 10 and 1 from No. 12) exhibited mild apical enlargement. Two submitted canines (No. 14) were the least severely affected. They did not appear thickened and only had very mildly roughened surfaces (Fig. 2). In 2 cases (Nos. 2, 11), the entire rostral mandible and maxilla were submitted and were characterized by large bulbous apical and reserve crown enlargements and multifocal gingival loss (Fig. 3). The lateral incisors were the most severely affected in these 2 horses. In these en bloc specimens, bulbous enlargements and variably sized, irregular, necrotic spaces (lytic foci) were often best seen in cross section (Figs. 4, 5).
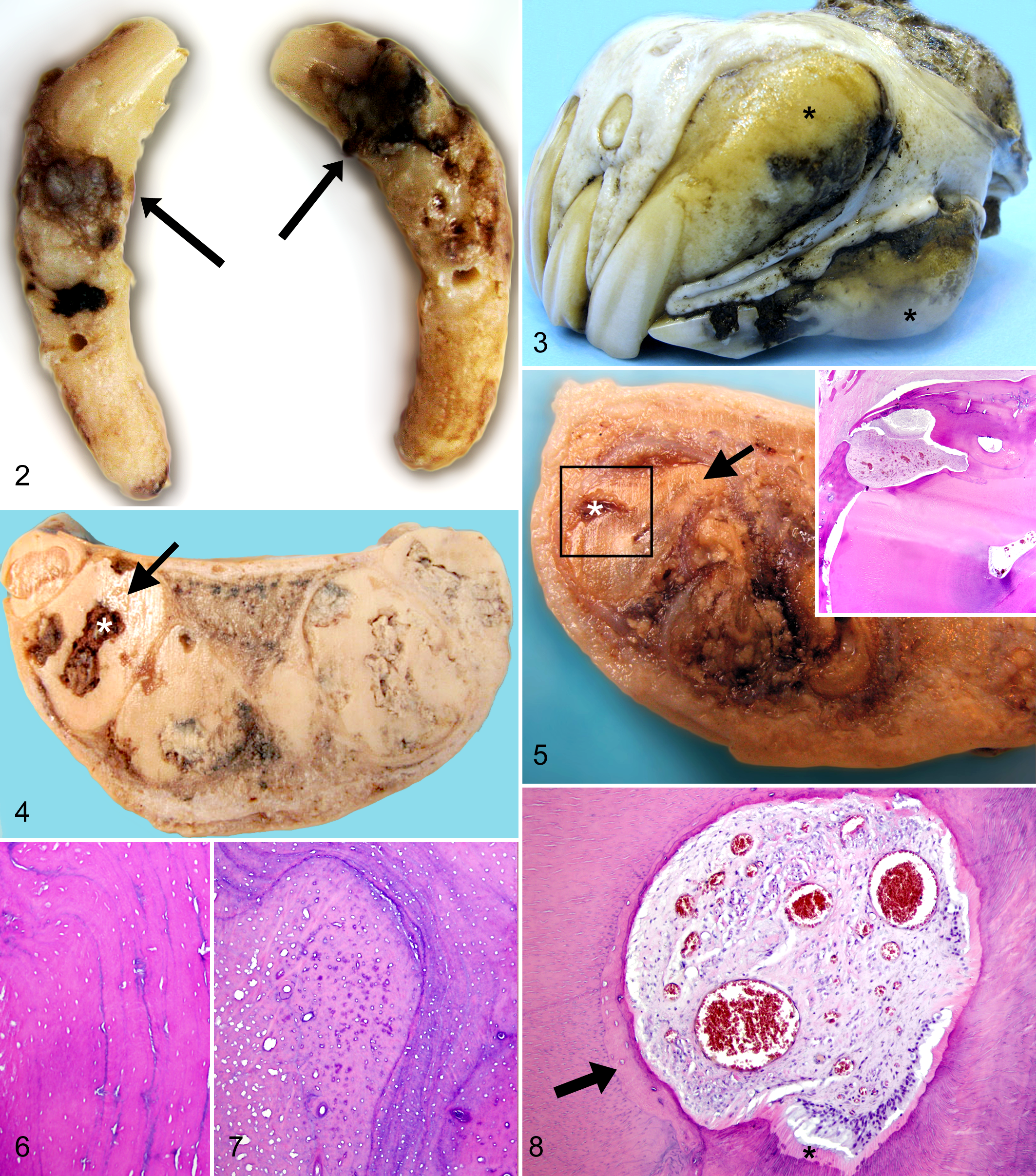
Equine odontoclastic tooth resorption and hypercementosis, teeth, horse.
Histologically, all affected incisors and the 3 examined canine teeth (Nos. 3, 14) had cemental lesions, which included cemental hyperplasia and lytic lesions (Fig. 5). Cemental hyperplasia was often circumferential (Suppl. Fig. S1). The cementum was generally more organized with parallel basophilic incremental lines away from areas of lysis (Fig. 6). In regions of lysis, the cemental hyperplasia was characterized by a proliferation of disorganized cementum with wavy basophilic incremental lines, large spaces, and large vascular channels creating a mosaic pattern (Fig. 7). The mildest lesions of cemental hyperplasia were in canine teeth from the youngest horse in the study (No. 14, 10 years of age). The cemental hyperplasia was primarily external, and disorganized cementum extended only slightly into the dentin layer in these 2 teeth. Teeth from 15 of 17 horses (88%; Nos. 1–13, 15, 16) had necrotic debris; 8 of 17 (47%; Nos. 1, 2, 6–8, 10, 11, 13) contained bacteria (cocci or filaments); and 6 of 17 (35%; Nos. 1, 6, 7, 10, 11, 13) contained plant material in at least 1 tooth.
Dentinal lysis was present in at least 1 tooth from all horses. In 2 of 17 cases (12%; Nos. 9, 11), lysis varied from a form of replacement resorption in all cases, where disorganized cementum extended into the dentin layer, to inflammatory resorption, in which infiltration of leukocytes was associated with marked destruction of the dentin. Debris was present in the dentinal layer in 8 of 17 cases (47%; Nos. 3–5, 7–11). In multiple sections of incisors from case No. 11, there were large lytic resorptive foci that extended from the cementum, through the dentin, and into the pulp cavity. These foci contained a large amount of necrotic cellular debris, degenerate mixed inflammatory cells (primarily neutrophils in some areas but lymphocytes and plasma cells in other areas), granulation tissue, and sometimes a downgrowth of gingival epithelium. Cementoclasts were present within resorptive pits along scalloped surfaces of necrotic cementum. In case No. 9, the lytic regions were characterized by marked fibrosis with sequestered fragments of dentin.
Endodontic lesions were present in 12 of the 15 horses (Nos. 1–6, 8–11, 13, 14 but not 12, 15, 17) in which the pulp cavity could be discerned. Lesions in the pulp cavity included mild neutrophilic to lymphoplasmacytic inflammation (n = 6; Nos. 1–6), internal lysis of dentin (n = 4; Nos. 5, 8, 9, 11), necrotic debris (n = 4; Nos. 6, 8, 9, 11), fibrosis (n = 10; Nos. 1, 2, 4–6, 8–10, 13, 14), and a rim of atubular mineralized material (n = 11; Nos. 1, 3–5, 7–13; Fig. 8). In 2 of these 12 horses (Nos. 9, 11), the pulp stroma was completely obliterated by large lytic areas that contained necrotic debris, fibrous connective tissue, mixed bacteria, and plant material.
Periodontal disease—primarily lymphoplasmacytic inflammation and fibrosis of the PDL—was noted in at least 1 tooth in 15 of 17 horses (88%; Nos. 1–7, 9–12, 14–17). Occasional areas of neutrophilic inflammation, hemosiderin-laden macrophages, multifocal hemorrhage, and/or small islands of cementum were also noted in some cases. Gingival lesions were noted in at least 1 tooth in 5 of 9 horses that had gingiva present in the sections examined (Nos. 1, 2, 7, 11, 12 but not 8–10, 14). Lesions included mild to moderate lymphoplasmacytic and neutrophilic inflammation (n = 3; Nos. 1, 2, 11), mild lymphoplasmacytic inflammation (n = 2; Nos. 7, 12), occasional downward growth of epithelium in regions of neutrophilic inflammation (n = 1; No. 2), and mild hyperplasia (n = 1; No. 12).
Lesions in the alveolar bone were present in at least 1 tooth in 5 of 9 horses that had alveolar bone present in the sections examined (Nos. 1, 2, 5, 11, 13 but not 4, 7, 10, 16). In these 5 cases, lesions were considered mild and included various combinations of osteolysis, new reactive bone formation, medullary fibrosis, and neutrophilic and lymphoplasmacytic inflammation. Alveolar bone lysis was characterized by a scalloped surface with occasional osteoclasts within resorptive pits. The entire alveolus was not examined for any of the cases. When present, there was only a small amount of alveolar bone within the soft tissue of extracted teeth specimens and only a small amount of alveolar bone within representative sections of affected teeth in the en bloc specimens.
A premolar tooth was examined from 2 horses (No. 12, tooth 406; No. 15, tooth 406), and both exhibited hypercementosis. One of these teeth (No. 15, tooth 406) exhibited very marked hypercementosis, but large lytic spaces filled with necrotic cellular debris and inflammatory cells were not a feature of either of these premolars. Some of the disorganized cementum in case No. 15 appeared to be degenerate/necrotic. Disorganized cementum with wavy basophilic incremental lines extended into the dentin, and a small amount of atubular mineralized material was present along the periphery of the pulp cavity in case No. 12. In the sections of the premolar from case No. 15, plant material and mixed bacteria were noted along the surface of the cementum in one fragmented section, but there was no reaction to it. Also, the dentin of this tooth appeared to be somewhat irregular in regard to orientation of tubules, but the significance of this finding is unknown. There was mild gingival hyperplasia and mild multifocal lymphoplasmacytic inflammation and fibrosis with occasional small islands of cementum in the PDL of the premolar in case No. 12. These tissues were not present in the sections of premolar from case No. 15. The lesions in the incisor teeth of these 2 horses were milder than those in the incisors from the other horses in the study. The PDL surrounding the examined incisors from both these horses exhibited mild lymphoplasmacytic inflammation.
Discussion
All affected incisor and canine teeth exhibited hypercementosis and lytic resorptive foci. The proliferation of cementum in severe cases caused bulbous enlargement of the intra-alveolar portions of affected teeth, and there were large regions of inflammatory resorption characterized by scalloped lytic lesions that often contained amorphous necrotic debris, mixed bacteria, and plant material. In some cases, proliferative disorganized cementum and lytic lesions extended through the dentin into the pulp cavity resulting in endodontic disease. In addition, periodontal disease, characterized primarily by moderate inflammation of the PDL, was a common feature. The reported histopathologic findings in the incisor and canine teeth and the PDL of this case series are similar to those reported in Europe. 21
This condition seems to have a male predominance, with geldings being the most commonly affected in the current study. In the study by Staszyk et al, 21 7 of the 8 horses were male. Baratt 1 described EOTRH in 4 horses, all of which were geldings, in another report. Affected horses were generally >12 years of age, but there are anecdotal reports of early lesions in horses as young as 5 years. In the current study, horses ranged in age from 10 to 32 years, with an average age of 21.7 years. This study had a bias toward older horses due to selection of cases with severe enough lesions that required extraction of affected teeth or, in 2 cases, euthanasia. There was no definitive breed predisposition; however, Warmbloods and Thoroughbreds were overrepresented in some studies, 1,21 including the current study, with these breeds making up well over half of the study population. However, this breed and sex predisposition may represent a biased population of horses receiving dental examinations by veterinarians with advanced dental training. A recent archival study of 3461 horses reported EOTRH in 1.8% of the study population, a mean age of 12.6 years for affected horses, and no predictive risk factors associated with breed, sex, or age. 15
The premolars from 2 affected horses (Nos. 12, 15) had similar lesions as those in their incisor teeth; however, there were no large lytic spaces or pulpal lesions to support a reparative function of the hypercementosis, and the lesions in the incisor teeth were milder than those in the incisors from the other horses in the study. EOTRH has not been described in premolars, and it is unclear if the lesions in these 2 premolars have the same pathogenesis as those in the incisor teeth. A normal aging response due to wear at the occlusal surface over time was also considered as a possible cause of the hypercementosis in these premolars. 13
On the surface, EOTRH may appear to be similar to multiple idiopathic root resorption in humans and tooth resorption in cats, but when examined closely, there are many differentiating clinical and histopathologic features. In the feline and human conditions, the resorptive process predominates, and hypercementosis is minimal. 3,8,17 –19,21 Feline resorption targets premolars, molars, and canines and frequently results in degenerative alveolar bone expansion and extrusion of the canine teeth. 12,17,18 In horses, hypercementosis is a common clinical feature, and incisors and canines are primarily involved without signs of tooth extrusion. The type of resorption also varies among species. Feline and human tooth resorption is primarily a form of external replacement resorption. 3,12 In comparison, equine teeth undergo a strong inflammatory resorptive process. On histologic examination of feline and human resorbed teeth, degeneration of the PDL leading to narrowing of the PDL space and ankylosis of affected teeth is prevalent, unlike in horses, where widening of the PDL space and reattachment of the PDL to cementum are possible. 3,8,12,17,21 A unique feature of the equine periodontium is the ability of cells within the PDL to initiate marked hypercementosis. 21 In this study, there were also unique equine pulpal changes not reported in the human and feline resorption literature. Atubular mineralized material was found in the pulp cavity of several equine incisors; the histologic appearance of this material is consistent with cementum or osteodentin. 21 Therefore, there are some significant features of EOTRH that appear to differ from the resorptive processes occurring in feline tooth resorption and multiple idiopathic root resorption. However, further characterization of these conditions in both cats and horses is needed.
While EOTRH has been increasingly recognized by veterinary equine practitioners and dentists, it is uncommonly encountered by veterinary pathologists. In some cases, it can be difficult to differentiate this condition from benign tumors of cementoblast origin. 23 Few suspected cases of cementoblastomas involving the incisors of horses have been reported in the veterinary literature. 10 Classically, these neoplasms affect only a single premolar or molar, and they are characterized by a bulbous enlargement with little inflammation or lysis. 10 In humans, most cases occur in young adults and children. They can be difficult to distinguish from hypercementosis but are characterized by destruction of the lamina dura, a feature that is not seen with hypercementosis. 14 In humans, idiopathic hypercementosis is asymptomatic and characterized by excessive acellular regularly mineralized cementum that is attached to the dental root and associated with a thin connective tissue without cementoblasts. 14 Cementoblastomas are composed of irregularly mineralized cementum with many reversal lines that is fused to the root of the tooth and embedded in fibrovascular stroma that may contain multinucleated osteoclast-type giant cells and plump cementoblasts. 10,14,23 It is important for the clinician to differentiate EOTRH from cementoblastoma, as EOTRH is a progressive disease that affects multiple teeth, and early lesions in seemingly normal teeth may be detected only with complete dental radiographs. Thus, management and prognosis are completely different. Given consistent histopathologic features, the rare diagnosis of cementoblastoma could be considered in cases that present as a single enlarged bulbous premolar with no evidence of lysis and no other radiographic abnormalities. However, an extracted bulbous incisor with evidence of lysis in a horse with a history of multiple affected incisors should be diagnosed as EOTRH. Thus, if only a single extracted tooth is submitted for histopathology, it is important for the clinician to provide a complete history, results of dental radiographs, and a list of differential diagnoses to the pathologist so that the correct histologic diagnosis can be made.
The cause of EOTRH remains unknown, but many etiologies have been proposed, including mechanical forces, ischemic necrosis, genetic factors, diet, fluorosis, underlying systemic disease processes, infectious agents, idiopathic, multifactorial genesis, and metabolic disorders involving abnormal blood calcium, vitamin D, parathyroid hormone, vitamin A, cortisol, or other hormone levels. 2,20 –22 Increased levels of vitamin D have been reported in cats with tooth resorption, and resorption has been experimentally induced in dogs and rats by administering excess vitamin D. 17 Thus, investigation of vitamin D levels in affected horses may be warranted. Occlusal stress has also been suggested as a cause of tooth resorption in cats, and occlusal wear and mechanical stress are currently favored by many researchers as a main underlying factor of EOTRH. 17,20,21 The PDL adheres the cemental surface of the tooth to the underlying alveolar bone. At approximately 13–15 years of age, equine incisors begin to decrease in length; this reduces the surface area to which the PDL can attach, and it increases the stress placed on the PDL. 20 Interestingly, PDL lesions, which consisted primarily of lymphoplasmacytic inflammation and fibrosis, were noted in at least 1 tooth of each of 15 horses in the current study. In addition, gingival inflammation and alveolar bone lesions (lysis, new bone formation, mixed inflammation, and fibrosis) were present in 5 of 9 horses. Thus, another hypothesis is that primary periodontal disease may lead to or perpetuate this condition by causing instability of the tooth and secondary repetitive cycles of lysis and repair by cemental deposition. 4 Entrapment of foreign material, such as feed particles, may further propagate and incite continued inflammation. The least affected teeth in the current study were from the youngest horse (No. 14), and the hypercementosis was primarily external, with only slight extension into the dentin layer. Large lytic foci were not a feature of these teeth, and other than mild fibrosis, the pulp cavity was unaffected. Thus, resorption with secondary hypercementosis appears to begin on the external surface of the teeth rather than within the pulp cavity. Further studies are needed to elucidate the pathogenesis of this disease.
In summary, EOTRH is a painful progressive condition of incisors and canine teeth in middle-aged to older horses of unknown cause. It has been reported in 3 continents and is characterized by resorption, hypercementosis, and often PDL inflammation. Lesions in this study were similar to those reported in Europe. EOTRH is likely underdiagnosed and misdiagnosed, especially in cases where a complete history and dental radiographs are lacking. Complete oral examination and dental radiographs are needed for clinical diagnosis, especially when lesions are early and mild. Microscopically, hypercementosis and lysis are both present to varying degrees in affected incisors and canine teeth. It is unclear if premolars can be affected by this same condition.
Footnotes
Acknowledgements
We thank the histology laboratory of the Diagnostic Center for Population and Animal Health, Michigan State University, especially Kelli Cicinelli, for tissue processing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Academy of Veterinary Dentistry Research Grant and by the authors. Additional support was provided by several contributing veterinarians.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.