
Abstract
There are few reports of naturally occurring muscular dystrophy in domestic animals. Herein, we describe a case of muscular dystrophy in a 4-year-old neutered male American domestic shorthair cat that died unexpectedly following anesthesia for an elective surgical procedure. Macroscopic muscular hypertrophy and histologic evidence of myofiber size variation, mineralization, myofiber degeneration, and necrosis were compatible with a diagnosis of muscular dystrophy. Extensive endomysial fibrosis was noted histologically in the diaphragm. A complete absence of dystrophin protein in Western blot confirmed the diagnosis of Duchenne muscular dystrophy. Immunofluorescence microscopy revealed reduced levels of dystrophin-associated proteins and an upregulation of utrophin at the sarcolemma. Anesthetic deaths can occur in dystrophin-deficient cats, and therefore muscular dystrophy and the associated cardiomyopathy should be considered in the differential diagnoses for perianesthetic death in cats.
History
A 4-year-old neutered male American domestic shorthair cat underwent an elective front paw declawing procedure. Preanesthetic blood work performed at the referring veterinary clinic revealed increased alanine aminotransferase (ALT, 302 U/L; reference range provided was 12–130 U/L), and prior blood work showed that ALT was persistently elevated (data not available). Creatine kinase and aspartate aminotransferase (AST) activities were not included in the preanesthetic blood work. Between 50 and 55 minutes after anesthesia, the cat stopped breathing and died. The cat was submitted for necropsy to the University of Minnesota Veterinary Diagnostic Laboratory.
Gross Finding
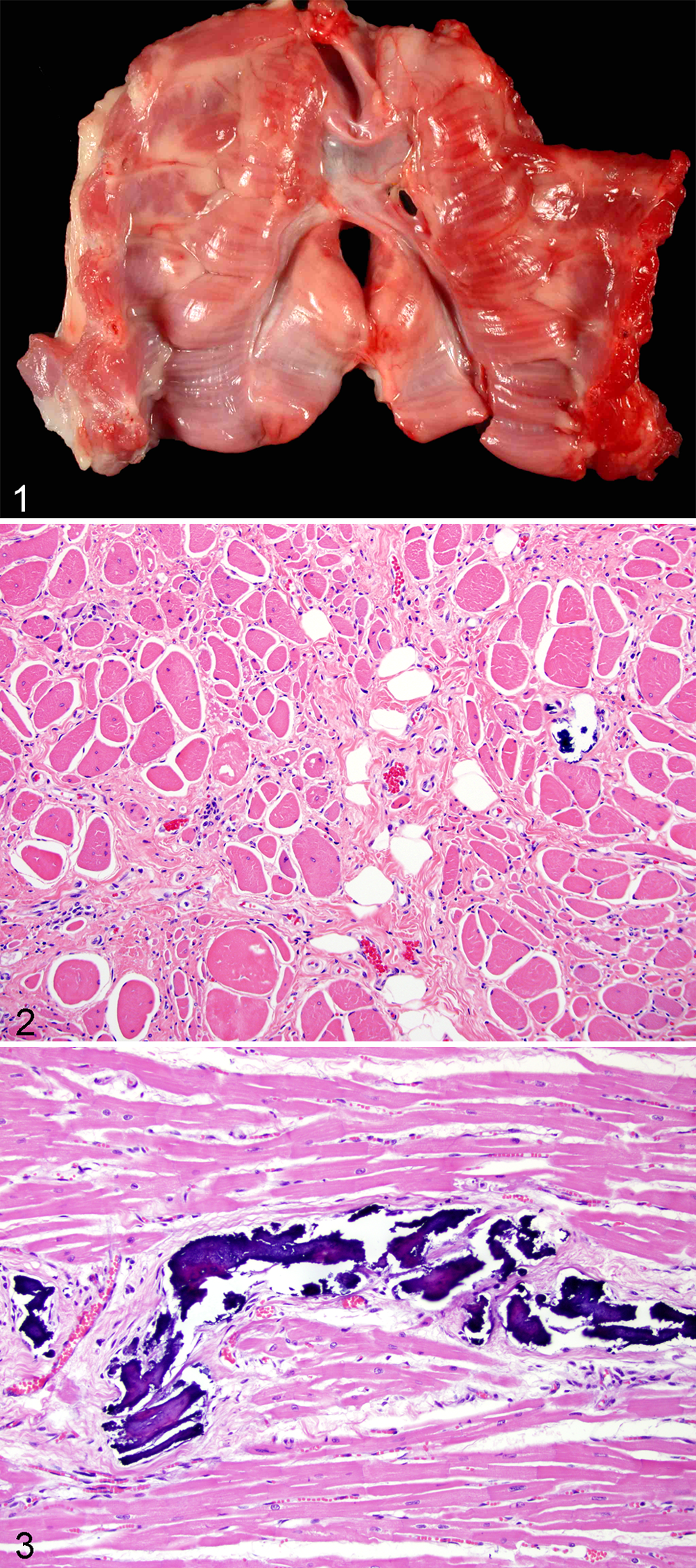
At necropsy, there was pronounced generalized skeletal muscle hypertrophy with the neck and forelimbs especially well muscled. The diaphragm had generalized and uniform thickening with multifocal nodular areas (Fig. 1). At the diaphragmatic esophageal hiatus, there was heavy muscling circumferentially with megaesophagus. The heart had thickened left ventricular muscle. There were no other macroscopic abnormalities in the rest of the organs examined. The only diagnosis considered at this point was muscular dystrophy (MD).
Histopathological Findings
Histological examination of skeletal muscle, including diaphragm, tongue, and intercostal muscles, revealed myofibers that were diffusely variable in size, with evidence of necrosis, degeneration, and regeneration. Degenerated and necrotic myofibers were surrounded by substantial interstitial fibrous connective tissue that was most pronounced in the diaphragm (endomysial fibrosis) (Fig. 2) and was further highlighted by Masson-Trichrome stain. Myofibers were either rounded and increased in diameter (hypertrophy) or shrunken and individualized (atrophy). Myofibers occasionally had hypereosinophilic, granular, or vacuolated sarcoplasm with multiple peripheral or centralized nuclei. Few regenerative muscle fibers with multiple rowing nuclei and slightly basophilic sarcoplasm were noted. Scattered necrotic myofibers with loss of striations, poorly delineated or fragmented sarcoplasmic membranes, and amorphous or flocculent sarcoplasm were present. Necrotic myofibers were surrounded by macrophages with phagocytized cellular debris. Multifocally, there was mild basophilic stippling (mineralization) in the sarcoplasm of degenerated and necrotic myofibers. The tongue and the heart (Fig. 3) had mild to moderate spotty mineralization primarily associated with the endomysium that likely replaced degenerated myocytes. Scattered mineral foci were also observed in other skeletal muscles. The diagnosis of MD was based on both gross and microscopic findings; no other differential diagnosis was considered. To further characterize the type of MD, immunofluorescence and Western blot analysis were performed on frozen skeletal muscle sections.
Immunofluorescence and Western Blots
Immunofluorescence microscopy revealed a loss of sarcolemmal dystrophin signal in the affected cat skeletal muscle, with the exception of an occasional positively stained revertant myofiber. Western blot analysis confirmed the complete absence of full-length and truncated dystrophin protein. Reduced expression of dystroglycan and sarcoglycan members was also observed in the affected cat. Utrophin staining was present at neuromuscular junctions in control and affected cat sections but was also upregulated and distributed at the sarcolemma in the affected cat myofibers. This combined histological and biochemical data provided a final diagnosis of dystrophin-deficient MD comparable to human Duchenne muscular dystrophy (DMD) in the affected feline.
Discussion
Differential diagnosis of various feline myopathies includes but is not limited to infectious myositis in association with necrotizing fasciitis, inflammatory polymyositis, congenital inherited myotonia in cats, and nutritional and metabolic myopathies. In this case, gross and microscopic findings led to an initial diagnosis of MD. The absence of dystrophin in skeletal muscle confirmed the diagnosis. Various forms of MD are caused by genetic mutations that result in a complete or partial deficiency in 1 or more of the dystrophin-associated proteins. Dystrophin-associated proteins form a large protein complex spanning the muscle fiber membrane, connecting the intracellular actin cytoskeleton and the extracellular matrix. In cats, deficiency in dystrophin, 1 β-sarcoglycan, 8 α-dystroglycan, 6 and laminin α2 (merosin) 7 have been reported. In this case, the dystrophin protein was absent, similar to DMD in humans. DMD in humans is an X-linked recessive disorder affecting 1 in 3500 male births that is fatal by the second decade of life. 10 Dystrophin deficiency has been reported as an X-linked recessive disorder in cats. 1 This condition has also been called feline hypertrophic muscular dystrophy 3 and is comparable to DMD.
Some dystrophin-deficient cats have severe axial and proximal appendicular skeletal muscle hypertrophy with involvement of the tongue and diaphragm. Hypertrophy of the diaphragm and esophageal musculature can lead to megaesophagus with signs of regurgitation. Hypertrophy of the tongue and pharyngeal muscle can cause dysphagia, dehydration, and dyspnea. 4 Histologic features of MD include marked variation in fiber size with numerous hypertrophied fibers often containing multiple internal nuclei and scattered clusters of necrotic and regenerative myofibers. Endomysial fibrosis is reported to be minimal in dystrophin-deficient cats, 1 except in 1 report in which endomysial fibrosis was present primarily in the diaphragm, 2 similar to the findings in the current case. Although electron microscopy can help in the diagnosis of MD, immunofluorescence is more specific to identify the type of dystrophy.
In contrast to feline cases that exhibit generalized muscular hypertrophy and little endomysial fibrosis, human patients with DMD experience focal muscular pseudo-hypertrophy, with progressive muscular atrophy and replacement with fibrous and adipose tissue. 1 For this reason, domestic cats are not a good model for the human disease. Dogs and mice are more commonly used since they can develop changes similar to human patients. 9
Dystrophin-deficient cats can also develop a “malignant hyperthermia-like syndrome” associated with restraint, stress, or general anesthesia. 3 A similar phenomenon exists in undiagnosed young children with MD who undergo anesthesia. 5 Two of 3 cats studied in 1 report 3 died during extubation and recovery from anesthesia. These authors concluded that this syndrome was likely the result of massive rhabdomyolysis, leading to severe metabolic imbalance and death. 3 The absence of overwhelming acute myofiber necrosis makes it less likely that this cat died of a hyperthermia-like syndrome. Findings in the current case and previous reports warrant consideration of MD as a probable cause of perianesthetic death in domestic cats.
In summary, MD is an uncommon disease of cats that can go unrecognized by owner and veterinarian. It should be suspected in animals of all ages, as shown in this case, but will typically affect mostly young males, with increased muscle mass and elevated serum muscle enzyme activities (CK, AST, and ALT). MD should be included in the list of causes for perianesthetic death. Revertant myofibers can be present on immunofluorescence staining for dystrophin and should not rule out a diagnosis of dystrophin deficiency. This case highlights the importance of precise classification of MD in animals to increase the awareness of the veterinary community for this disease, provide clear information to owners, and support research in human medicine.
Footnotes
Acknowledgements
We thank Dr Erik J. Olson and Dr Anibal G. Armien for technical support and communication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.