
Abstract
A 13-week-old male intact Poodle mix dog developed an acute onset of vestibular ataxia, tetraparesis, and vomiting. The patient presented ambulatory, tetraparetic, and ataxic with a head tilt to the left and a disconjugate nystagmus (rotary nystagmus with fast phase to the right in right eye and vertical nystagmus in left eye). There were absent postural reactions in the left pelvic and left thoracic limbs and decreased right-sided postural reactions. Magnetic resonance imaging demonstrated an intra-axial mass within the left midcaudal medulla oblongata. On gross dissection, there was a left-sided neoplasm in the medulla oblongata with surrounding hemorrhage. The histologic findings indicated that the mass was a pleomorphic xanthoastrocytoma. This tumor, an uncommon variant of an astrocytoma most often seen in children and young adult humans, has yet to be described in dogs.
Signalment, History, and Clinical Findings
A 13-week-old male intact Poodle mix dog presented for evaluation of ataxia and vomiting. The patient had developed acute neurologic deficits that included ataxia and tetraparesis. On presentation, he was alert and responsive, ambulatory, ataxic, and tetraparetic. He had a head tilt to the left with disconjugate nystagmus. He had normal segmental spinal reflexes, absent postural reactions in the left pelvic and left thoracic limbs, and decreased right-sided postural reactions. The remainder of his physical examination yielded normal findings. The neuroanatomic localization of his lesion was in the central ventral system. No significant abnormalities were noted on the routine clinical blood chemistry panel, complete blood count, or urinalysis. The differential diagnoses considered at this time included inflammation (encephalitis), congenital malformation, infection, vascular disease, and neoplasia.
Imaging, Diagnosis, and Outcome
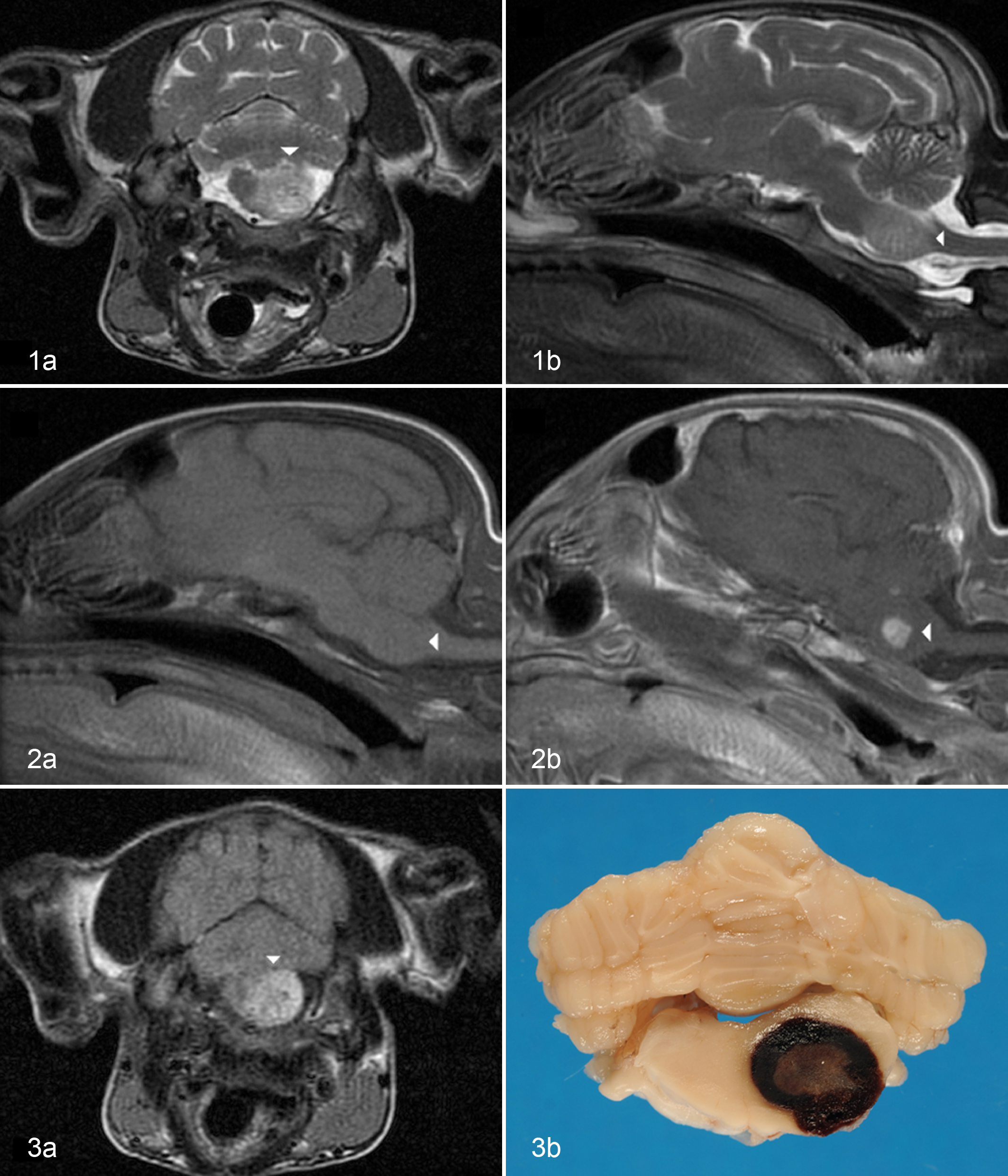
Magnetic resonance images were acquired (Signa Horizon 1.5T). The study consisted of transverse and sagittal images for T1-weighted (T1w) pre- and postcontrast (Omniscan Gadodiamide), T2-weighted (T2w), proton dense/intermediate weighted, and FLAIR (fluid-attenuated inversion recover) sequences. Gradient echo sequences were not acquired. There was a well-defined, roundish, left-sided, T2w hyperintense to normal, parenchymal, intra-axial mass within the midcaudal medulla that measured approximately 1 × 0.9 × 1.05 cm (Fig. 1a, 1b). The mass had a mixed-intensity appearance on T2w sequence. The mass was isointense on T1w precontrast images (Fig. 2a). Contrast administration showed a focal, central, contrast-enhancing mass on T1w images that measured 0.65 × 0.6 × 0.65 cm (Fig. 2b). The FLAIR sequence showed that the mass was hyperintense to normal parenchyma within the periphery of the swelling, while the center of the mass was relatively hypointense/isointense to the normal parenchyma (Fig. 3a). Differential diagnoses for a focal, central, contrast-enhancing mass within a young dog included abscess or focal granuloma, vascular malformation, thrombus, and neoplasm (primary or metastatic). 6 PCR (polymerase chain reaction) tests on whole blood for canine distemper virus and West Nile virus yielded negative results. Bacteria were not isolated from the cerebrospinal fluid on aerobic and anaerobic culture. Results were negative for whole blood PCR testing for Neospora caninum and N. hughesi, Borrelia burgdorferi, Anaplasma phagocytophilum, Ehrlichia canis, and Rickettsia spp; antibody testing (IgM and IgG) for Toxoplasma gondii and Neospora; and fungal cultures. Cytology of the cisternal cerebral spinal fluid showed elevated white blood cells, 7/cmm (normal range, 0–5); elevated red blood cells, 684/cmm (0); and normal protein, 47 mg/dL (0–48). A differential cell count was performed showing 3% eosinophils, 26% neutrophils, 34% lymphocytes, and 37% large mononuclear cells. The cerebrospinal fluid had an abnormally elevated population of eosinophils. The elevated red blood cells are likely secondary to blood contamination during the cerebral spinal tap. The patient was discharged with treatment directed at supportive care and anti-inflammatory efforts with corticosteroids (prednisone, 2.5 mg every 24 hours for 1 week).
The patient presented for the second time 16 days later for an episode of generalized convulsions and increased respiratory effort. The gag reflex was absent at this time. The owners elected euthanasia due to decline of health.
Pathologic Evaluation
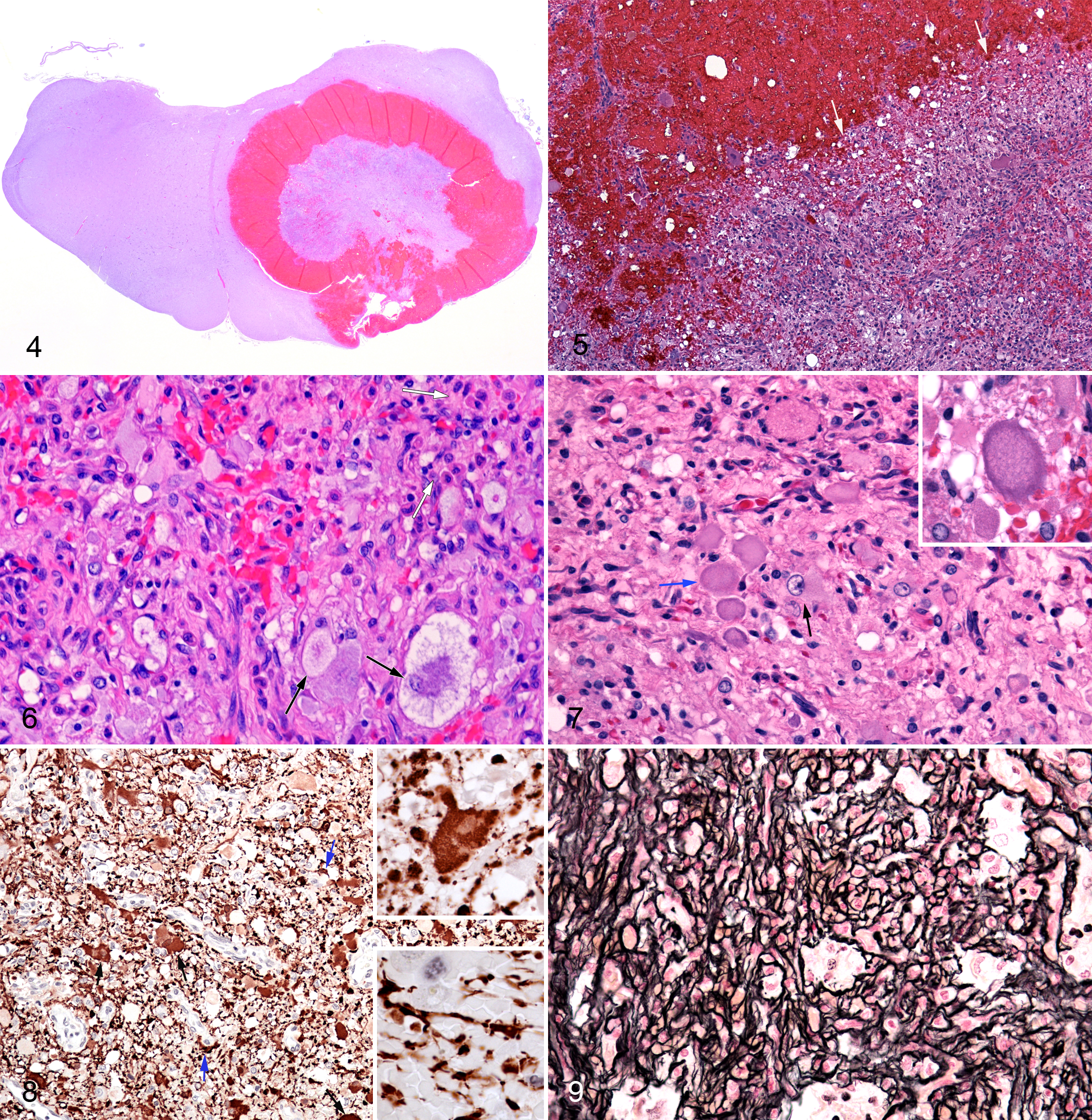
The brain and samples of trachea, lung, and liver were removed and fixed in 10% neutral buffered formalin. Gross examination of the formalin-fixed brain revealed a round mass in the left side of the medulla oblongata (Fig. 3b). The interior of the mass was solid and gray-tan and surrounded by a dark red corona consistent with hemorrhage (Fig. 3b). There was associated swelling of the left side of the medulla oblongata. Tissue blocks were embedded in Paraplast, sectioned at 5-μm thickness, and stained with hematoxylin and eosin. Selected brain sections also were stained with Chandler’s reticulin, PAS (periodic acid–Schiff), Masson’s trichrome procedures, and glial fibrillary acidic protein (GFAP) immunostain (1:350 dilution, Dako, GFAP, polyclonal, Z0334).
Microscopic examination of the mass revealed a neoplastic core and hemorrhagic corona (Figs. 4, 5). The neoplasm had a pleomorphic cell population, including prominent single nucleated giant cells with pale-stained or vacuolated cytoplasm (Figs. 6, 7), which did not react with the PAS stain. Neither mitotic activity nor necrosis was conspicuous. Many of these cells were GFAP positive (Fig. 8). In addition, there were many smaller elongated cells and cell processes within the tumor that reacted for this protein (Fig. 8). Reticulin fibers extended around individual and small groups of tumor cells (Fig. 9). There also were eosinophilic bodies, smaller round to elongated tumor cells, occasional entrapped large neurons, and scattered inflammatory cells (Figs. 6, 7). The neoplastic mass contained numerous hyperplastic, tortuous small blood vessels. In addition, there were some cavernous distended thin-walled blood vessels within the mass. There was a corona of recent hemorrhage dissecting some peripheral regions of the tumor and extending into the surrounding brain tissue (Figs. 4, 5). There was also associated edema and astrogliosis in the adjacent neuropil. The major extraneural finding was aspiration pneumonia.
Discussion
The microscopic appearance of this tumor is consistent with the pleomorphic xanthoastrocytomas as described in humans, a mass that has not been reported in dogs. In humans, this is considered a rare variant of the astrocytoma that is seen in children and young adults. 3,4,7 The lesion is almost always supratentorial, often involving the temporal lobe, where it tends to be superficial and may involve the leptomeninges. 8,9 Rarely, the tumor is found in the cerebellum or spinal cord.
Histologically, human pleomorphic xanthoastrocytoma is moderately cellular, composed of cells of varying size and shape—hence, its pleomorphic designation. 3,4,7 A characteristic feature is the presence of giant vacuolated lipid-bearing cells, which often express GFAP. Granular eosinophilic bodies are often noted. Reticulin fibers surround individual or small clusters of tumor cells. 3,4,7 Mitoses, regions of necrosis, and vascular proliferation are rare. 5 The neoplasm is usually well demarcated and has a favorable prognosis. 5 This case had many of the features of the pleomorphic xanthoastrocytoma in humans. It is a well-demarcated neoplasm with a pleomorphic cell population, many of which react immunohistochemically for GFAP. Importantly, this includes vacuolated, GFAP-expressing tumor giant cells and a prominent reticulin fiber network surrounding individual or small groups of tumor cells. Admittedly, there were features in the present case that are not common in the human form of this neoplasm. These include prominent microvascular proliferation and its location in the medulla oblongata. There was a prominent ring of recent hemorrhage around the neoplasm, which likely arose from tumor vasculature. Although not a common feature of pleomorphic xanthoastrocytoma in humans, bleeding is sometimes seen in association with that tumor. 8
Pleomorphic xanthoastrocytomas are reported to have a characteristic appearance on magnetic resonance within human medicine. Koeller and Henry 6 described that pleomorphic xanthoastrocytomas consistently show that the solid portion of the mass is iso- to hypointense on T1w images, while T2w images are hyper- to isointense. Douis et al 2 described similar findings, adding that the solid portion of the mass enhances with gadolinium on T1w images. Signal intensities described for various sequences in this case were consistent with that previously described in human medicine. 9 However, the study presented here does differ from the classic pleomorphic xanthoastrocytomas described in human medicine. The medulla oblongata is not the typical location for this cancer in humans, and the dog lacked the cystic portion commonly described in the superficial, supratentorial masses in humans.
A mass within the midcaudal medulla oblongata has the potential to cause dysfunction of the nucleus ambiguus (cranial nerve IX, X, XI), the vestibular system, and respiratory control. A lesion causing decreased function of the glossopharyngeal and vagus nerves can compromise control of the larynx and pharynx. A combination of vestibular disease and an inability to coordinate laryngeal function may lead to dysphagia and potential aspiration pneumonia. 1 A specific intracranial cause for the generalized convulsions was not found on necropsy. Therefore, extracranial causes, such as cerebral hypoxia secondary to aspiration pneumonia or vascular compromise associated with a bleeding mass within the brainstem, may have led to the convulsions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.