
Abstract
A young, intact, male Bernese Mountain Dog was presented to the animal hospital for lameness and diffuse thickening of the soft tissue in the right hind limb. Magnetic resonance imaging revealed multiple, multilobular, space-occupying lesions within and between the muscles of the right femur. Biopsies taken from the lesions revealed an infiltrative mass composed mainly of collagen fibers and a low density of benign-appearing fibroblasts. These findings were compatible with a diagnosis of a fibromatosis. Taking the age of onset into account, infantile fibromatosis was most likely. A deep fibromatosis, similar to that seen in adults, could not be excluded based on histology.
Soft tissue tumors of fibroblastic origin range histologically from benign fibromas to highly malignant fibrosarcomas. The heterogeneous group of fibromatoses consists of approximately 20 disorders that are classified by their biological behavior to range between fibroma and fibrosarcoma. 22 Fibromatoses are defined as nonmetastasizing but progressively growing, infiltrative, fibroblastic masses that tend to recur after surgical excision. 1 Depending on the subtype and anatomical location, their outcome may be fatal or relatively harmless. In people, soft tissue tumors occur mainly in adults and consist mostly of well-differentiated fibrous tissue. These growths are firm, nonencapsulated, poorly circumscribed, solitary to multiple masses with a predilection for certain anatomical sites. Fibromatoses of adults can be divided in 2 major groups: 1) superficial (fascial) and 2) deep (musculoaponeurotic) fibromatoses. Superficial fibromatoses arise from fascia or aponeurosis, grow slowly, and are usually small. Deep fibromatoses involve deeper tissues and are subdivided into extra-abdominal, abdominal, or intra-abdominal fibromatoses. Deep fibromatoses grow rapidly and often attain a large size. The term “desmoid tumor” is still widely used in the veterinary literature as a synonym for this latter aggressive type of fibromatoses. Major groups' subgroups of fibromatoses may also be defined by anatomical location and clinical signs. 25
Aside from the fibromatoses known in adults, fibrous proliferations of infancy and childhood are also described. These entities can be subdivided into 2 groups: 1) growths that have no clinical or morphological counterpart in adults and 2) growths that correspond clinically and microscopically to lesions observed in adults. 26 One example in the second group is infantile (desmoid-type) fibromatosis, which represents a counterpart of deep fibromatoses in adults. Cases of fibromatoses have rarely been reported in the veterinary literature. Intramuscular desmoid tumors of the pectoral and lateral cervical muscles have been reported 10,23 in 3 horses. An extra-abdominal, aggressive, desmoid tumor was also reported in a 9-month-old cat. In this individual, the entire right forelimb was affected and multiple nodules extended from the shoulder to the mandible. 16 In dogs, a single case of infantile desmoid-type fibromatosis in an Akita puppy has been described. 4 In the present report, the clinical, magnetic resonance imaging (MRI), and histological findings of a desmoid tumor in a young Bernese Mountain Dog are described.
A 1-year-old, intact, male Bernese Mountain Dog was presented to the Small Animal Clinic of the Vetsuisse Faculty of the University of Berne (Berne, Switzerland) for evaluation of a skin nodule and chronic lameness. Lameness in the right hind limb, accompanied by a palpable induration of the soft tissue of this extremity, was first noted shortly after the dog was purchased at 12 weeks of age and progressed thereafter. A ventrodorsal radiograph of the hips was performed by the referring veterinarian when the dog was 7 months old and revealed diffuse thickening of the soft tissue of the right thigh (Fig. 1). At that time, no further diagnostic work was performed. Ten days prior to presentation to the Small Animal Clinic of the Vetsuisse Faculty of the University of Berne (Berne, Switzerland), the dog was again presented to the referring veterinarian with fever (40.5°C) and acute exacerbation of the lameness. A complete blood cell count (CBC) revealed leukocytosis (26,700/μl; reference interval: 6,000-16,900/μl). The dog was treated with prednisolone (1.5 mg/kg by mouth every 24 hr for 5 days) and amoxicillin/clavulanic acid (12.5 mg/kg by mouth every 12 hr for 5 days), which resulted in clinical improvement, but the palpable enlargement of the right thigh persisted.
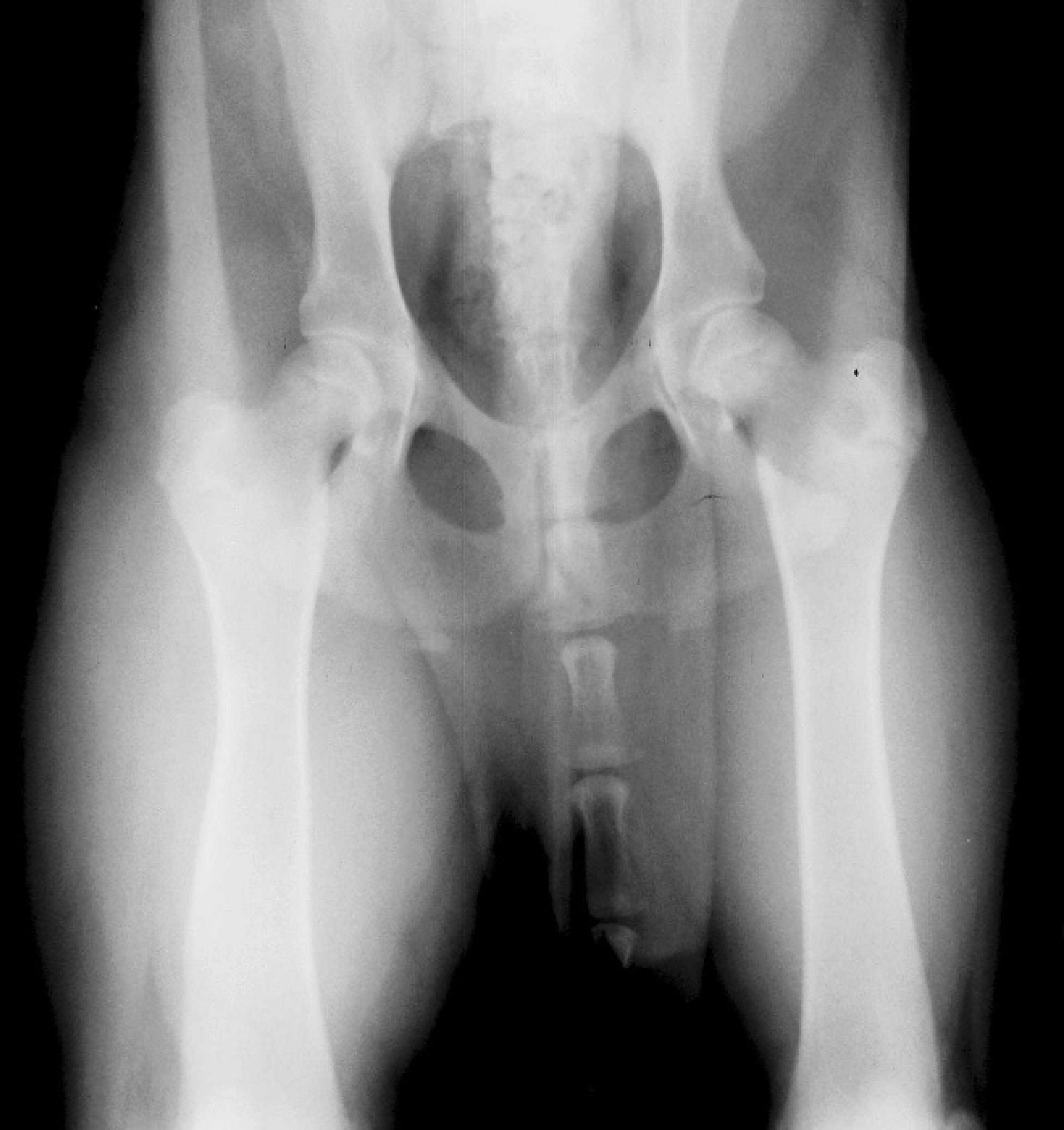
Ventrodorsal radiograph of the pelvis and femora of a 7-month-old Bernese Mountain Dog with fibromatosis. Notice the diffuse thickening of the soft tissues in the area of the right femur.
On physical examination, the dog was alert, in good body condition, and had a rectal temperature of 39°C. The dog was lame (3/5) in the right hind limb and had a stiff gait characterized by a markedly shortened stance phase. Passive movement of the limb revealed markedly restricted, nonpainful extension of the thigh. The entire vastus lateralis muscle and a large portion of the vastus medialis muscle of the quadriceps were firm, enlarged, and nonpainful on palpation. Multiple, firm, coalescing, approximately 1–2 cm-diameter, haired nodules and plaques were visible in the dermis cranial to the femur and were arranged in a 12-cm-long row. The CBC was within reference intervals and thoracic radiographs were unremarkable. Fine-needle aspirates and 5 biopsies were taken of the dermal and muscular masses.
Cytology of the dermal nodule was inconclusive since cellularity was very low. Cytology of the muscular mass revealed highly cellular slides with moderate numbers of red blood cells in the background. Nucleated cells were predominantly pleomorphic plump spindle cells scattered individually or arranged in tight clusters. These cells were often separated by thick bundles of fibrous-like extracellular material. Individual spindle cells had variable amounts of basophilic cytoplasm, an oval nucleus with 1–4 prominent nucleoli, and moderate anisokaryosis. Scattered lymphocytes and rare mast cells also were observed. The cytologic diagnosis was spindle cell tumor.
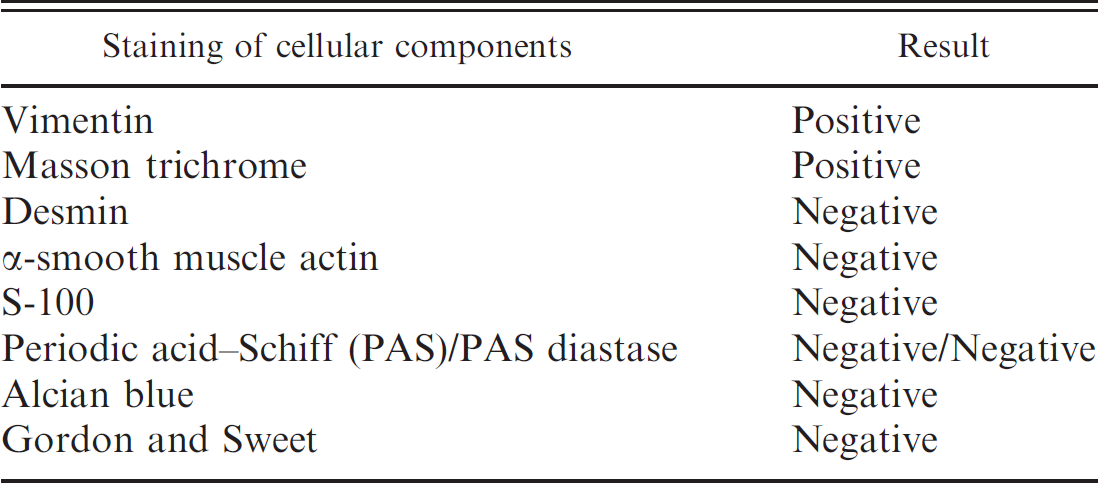
Histological findings were similar in all biopsies. The tissue sections were sparsely cellular and contained an infiltrative, nonencapsulated mass extending from the superficial dermis to the panniculus muscle and underlying striated muscle. Spindle cells were scattered singly or were occasionally aligned in fine streaming bundles. Individual spindle cells had a distinct cellular border and scant cytoplasm. The nucleus was elongated to round with finely stippled chromatin and 1–2 nucleoli. No mitoses were observed in ten 40 × fields of view. Cells were separated by abundant, fibrillar, eosinophilic material (mature collagen) arranged in bundles or occasionally in whorls. The mass was moderately vascularized by small- to medium-sized blood vessels. Mild multifocal infiltrates of lymphocytes were observed. The epidermis and adnexal structures were unremarkable. Multiple myocytes in the underlying muscle had centrally located nuclei (Fig. 2). The results of the histochemical and immunohistochemical staining are presented in Table 1. Based on the clinical and histological findings, a diagnosis of fibromatosis was made.
The dog was discharged without treatment and was presented again for neutering at 2 years of age. No further episodes of fever or acute worsening of lameness had occurred since the initial presentation. The dog was able to go for walks and had even been used to herd sheep. On presentation, the dog was bright and alert. The mass in the right thigh had increased in size. Passive extension of the thigh was severely restricted and flexion of the knee was no longer possible. Pain was not evident but the dog had a stiff gait with limited swing and stance phases. Results of a CBC and biochemical profile revealed no abnormalities. An MRI examination was performed during the anesthesia for neutering.
The MRI examination was performed with a low-field unit (0.3T). a The dog was positioned in lateral recumbency with the pelvis placed in a flexible coil. Sequences included a T2-weighted fast spin echo and a T1-weighted spin echo (SE) in sagittal and transverse orientation. Furthermore, a dorsal fat-suppressing short tau inversion recovery and a transverse T1-weighted high-resolution gradient echo (FE 3D MPR) were performed. The sagittal T1-weighted SE and the transverse FE 3D MPR were repeated after intravenous administration of contrast medium (gadodiamide, 0.15 mmol/kg body weight). The slice thickness ranged from 4.5 mm to 5.5 mm in the standard sequences and was 1.5 mm in the high-resolution gradient echo. Sequence orientation is given in relation to the pelvis. The MRI was performed from the level of the pelvis to the knees. Multiple, multilobular, well-delineated, space-occupying masses were observed within and between the iliopsoas, quadriceps, caudolateral muscles of the femur, and proximal gastrocnemius muscles of the right femoral region. More distal parts of the calf were not included in the field of view. The masses appeared to follow the muscles' anatomical course, were hypointense in all sequences, and generally lacked uptake of contrast media (Fig. 3).
The clinical findings, MRI imaging, and histological, histochemical, and immunohistological findings in the present case were compatible with a diagnosis of fibromatosis. The clinical findings and anatomical location were most consistent with either infantile fibromatosis or its adult counterpart, deep fibromatosis. The main histological feature was the abundance of collagen fibers associated with a moderate number of well-differentiated, benign-appearing fibroblasts. Based on the age of the dog, a diagnosis of an infantile or desmoid-type fibromatosis was most likely. In human medicine, few cases of infantile fibromatosis have been reported. This entity affects children from birth to 8 years of age. In most individuals, the masses originated in skeletal muscles, especially of the head and neck. Other muscles of origin, in descending order, included the shoulder, upper arm, and thigh. 7 These masses are described as gray-white, firm, usually solitary, nonencapsulated, and infiltrative growths. Microscopically, infantile fibromatosis is characterized by considerable variation in fibroblast differentiation. 1 The most common form of fibromatosis is the diffuse or mesenchymal type of infantile fibromatosis, found chiefly in infants during the first few months of life. In infantile fibromatosis, the cells are haphazardly arranged and are associated with mucoid material, residual muscle fibers, and lipocytes. The appearance of the cells range from primitive mesenchymal cells to fibroblasts. 8 Desmoid-type infantile fibromatosis is less common and is characterized by low cellularity, mature fibroblasts, and increased collagen bundles. 22,26 The histologic findings in the present case were compatible with desmoid-type infantile fibromatosis.
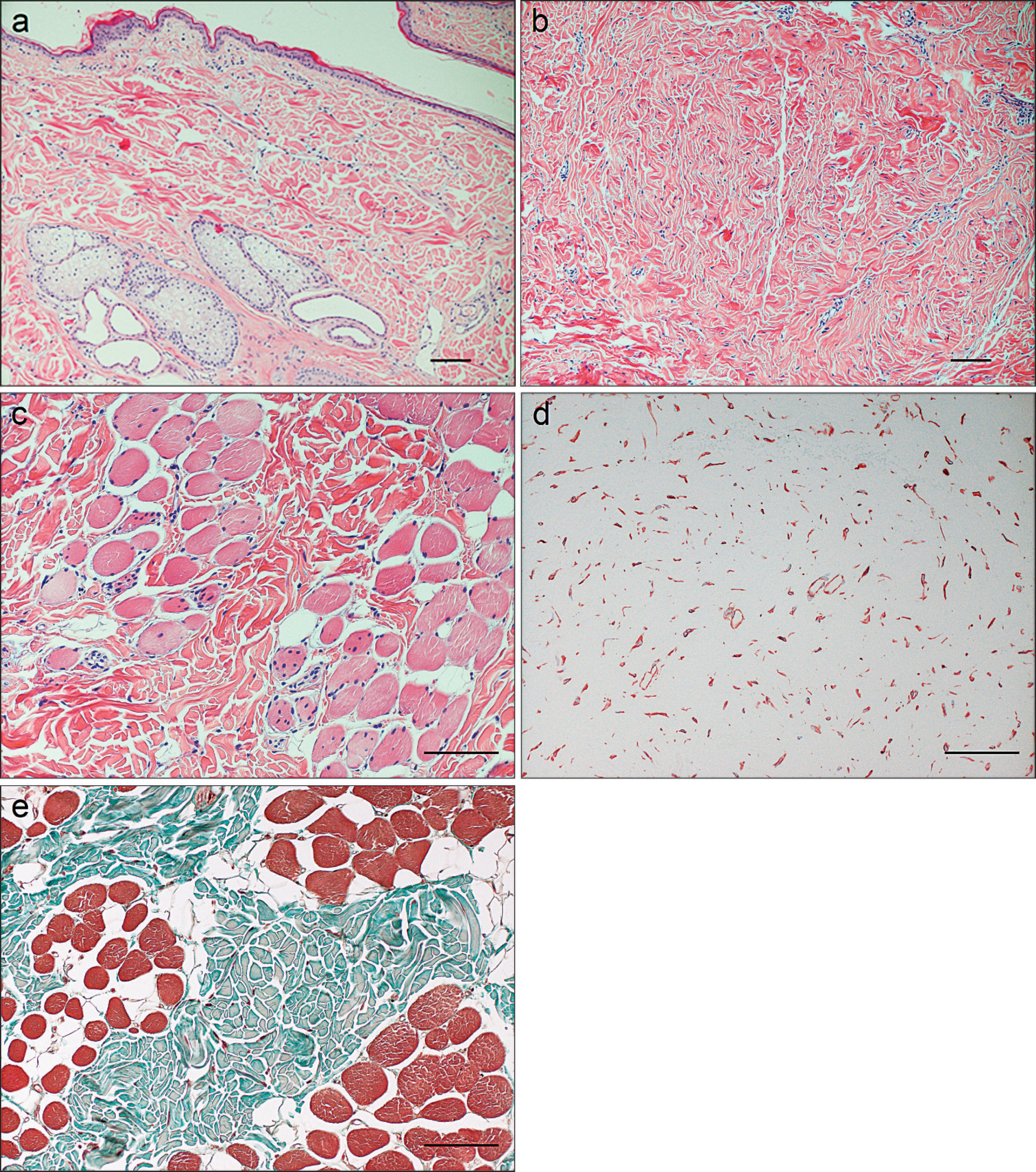
Histologic section of fibromatosis in a Bernese Mountain Dog. A diffuse, infiltrative mass of spindle cells extends from the superficial dermis to the panniculus muscle and underlying striated musculature of the right hind leg.

Sagittal magnetic resonance images (
Immunohistochemical and histochemical staining results of biopsy specimens from fibromatosis in a Bernese Mountain Dog.
Desmoid-type infantile fibromatosis is indistinguishable from deep fibromatosis of adults except in terms of the age of development. 25,26 Deep fibromatosis of adults usually occurs in patients between puberty and 40 years of age; however, the youngest reported patient was only 9 months old. 19 In humans, the main locations of extra-abdominal fibromatosis are the musculature of the shoulder, followed by that of the chest wall, back, and thigh. 25 Clinically, deep fibromatosis is characterized by deep, poorly circumscribed masses. Tenderness and pain may occur in association with decreased motion of the involved muscle(s). Motor weakness is possible if the tumor infiltrates or encases large nerves. Rare cases of multicentric lesions have been described 7,9,14 ; in most cases, the second growth develops proximal to the primary lesion. Microscopically, deep fibromatosis is poorly circumscribed and infiltrates the surrounding tissue, usually striated muscle. The tumor consists of elongated spindle-shaped cells of uniform appearance, which are embedded in an abundant amount of collagen. 6 At the periphery of the lesion, remnants of striated muscle fibers are frequently entrapped by the tumor tissue. Some muscle fibers appear atrophic or resemble multinucleated giant cells. Microhemorrhages and aggregates of lymphocytes also are commonly seen. 25
In humans, aggressive fibromatosis is either undetectable or is identified as an amorphous, dense, soft tissue mass by conventional radiography. Ultrasonography typically reveals a slightly hypoechoic, lobulated, or infiltrative mass. 12,13 Magnetic resonance imaging provides more optimal evaluation of the tumors. Aggressive fibromatosis typically has an infiltrative growth pattern, crosses fascial boundaries, and does not have central necrosis even in large lesions, unlike soft tissue sarcomas. On MRI, aggressive fibromatosis may also have bands of low signal intensity across all sequences and uniform, moderate to intense enhancement after gadolinium administration. On T1-weighted images, most lesions are rather homogeneous and isointense to muscle, whereas the lesions are more heterogeneous on T2-weighted images and have an overall signal intensity that is slightly lower than that of fat. Desmoid tumors often have irregular boundaries and extend across fascial boundaries into other tissue compartments; however, this is not a specific finding for all cases of aggressive fibromatosis. 13,15,24 The main differential diagnosis is soft tissue sarcoma, which is a space-occupying, intramuscular growth that enlarges in a centripetal fashion and displaces rather than infiltrates local structures. The MRI findings in the case described in the present report were similar to those of desmoid tumors in humans. All sequences showed lesions with low signal intensity, irregular boundaries, and absence of necrotic areas.
Both infantile fibromatosis and adult deep fibromatosis have been previously reported in the veterinary literature. Infantile desmoid-type fibromatosis was diagnosed in a 10-week-old Akita puppy. 4 In contrast to the current case, the Akita puppy had a mass within the abdominal wall that consisted of a proliferation of vacuolated, epithelioid to spindle cells surrounded by reticulin fibers. 4 A 9-month-old male cat also was reported 16 with an extra-abdominal desmoid tumor that affected the right forelimb, shoulder, and mandible. The mass was composed of large amounts of collagen and sparse numbers of fibroblasts. In contrast to the present case, the feline mass was highly cellular, contained multinucleated giant cells and immature fibroblasts, appeared highly aggressive, caused bone lysis, and recurred after surgery.
The pathogenesis of deep fibromatosis and infantile (desmoid-type) fibromatosis is unclear. Most of the fibromatoses in humans occur sporadically. Suspected causes of extra-abdominal deep fibromatosis in humans include trauma and endocrine factors. Estrogens have been implicated in the pathogenesis of sporadic desmoid tumors because females, particularly those of childbearing age, have an increased risk. For infantile fibromatosis, trauma has also been suspected as a causative factor, but this speculation remains unproven. An increased familial incidence of deep fibromatosis has never been observed. 3,18,20 In the previously reported 4 Akita puppy, surgical trauma was implicated as a causative factor in lesion development. However, no history of trauma was present in the Bernese Mountain Dog of the present report, and the siblings and parents were unaffected.
The optimal treatment for fibromatosis in humans is somewhat controversial. Although surgical excision has been preferred, 2,4 a multidisciplinary approach is often used that includes surgery, chemotherapy, and radiation therapy. 15,17,21 Wide surgical excision offers the best chance of avoiding recurrence but is difficult to achieve because of the infiltrative nature of desmoid tumors. 2 Spontaneous disappearance of desmoid tumors has occasionally been reported. 5,11 In the current report, the owner declined treatment. At the present time, the dog is 3 years old and, according to the owner, in good body condition.
In conclusion, the present report presents the clinical, radiographic, MRI, and histological findings of infantile desmoid-type fibromatosis or extra-abdominal fibromatosis in a young male Bernese Mountain Dog. This type of tumor has been reported rarely in the veterinary literature, indicating that fibromatoses are rare in animals. Nevertheless, fibromatoses should be considered as a differential diagnosis in young dogs presenting with a nodular mass, particularly around a limb or on the abdominal wall. Given the paucity of reports in animals, the morphological diagnoses in the published cases are largely based on the description of human lesions. Whether this extrapolation is justified remains unclear.
Acknowledgements. Yasminda Malik and Esther Sutter share first authorship.
Footnotes
a.
AIRIS® II, Hitachi Medical Systems Europe Holding AG, Zug, Switzerland.