
Abstract
A 6-year-old Haflinger mare was presented with a history of recurrent hemoabdomen. On necropsy, a firm infiltrative multinodular yellow mass was observed in the wall of the posterior abdomen. Histopathologic examination revealed a proliferation of fibroblastic cells, which were positive for α–smooth muscle actin and vimentin.
Case History
A 6-year-old, 454-kg Haflinger mare was examined at the Centre Hospitalier Universitaire Vétérinaire of the University of Montreal with a 24-hour history of lethargy and anorexia. The mare presented with dullness, muscular fasciculations, and profuse sweating. The rectal temperature was 37.9°C, heart rate was 100 beats per minute, and respiratory rate was 44 respirations per minute. A large amount of abdominal fluid was observed by ultrasonography, which on analysis was consistent with hemorrhagic effusion (PCV [Packed cell volume], 50%; total protein concentration, 5.9 g/dl). No neoplastic cells were seen on cytologic evaluation of the fluid. Four days after admission, a second abdominal ultrasonography revealed the presence of a large oval solid mass measuring 9 × 15 cm in the right caudal abdomen. On transrectal examination, the mass was firm, lobulated, nonmobile, and adhered to the abdominal wall. The following day, the mare became lethargic and anorexic, and euthanasia was performed.
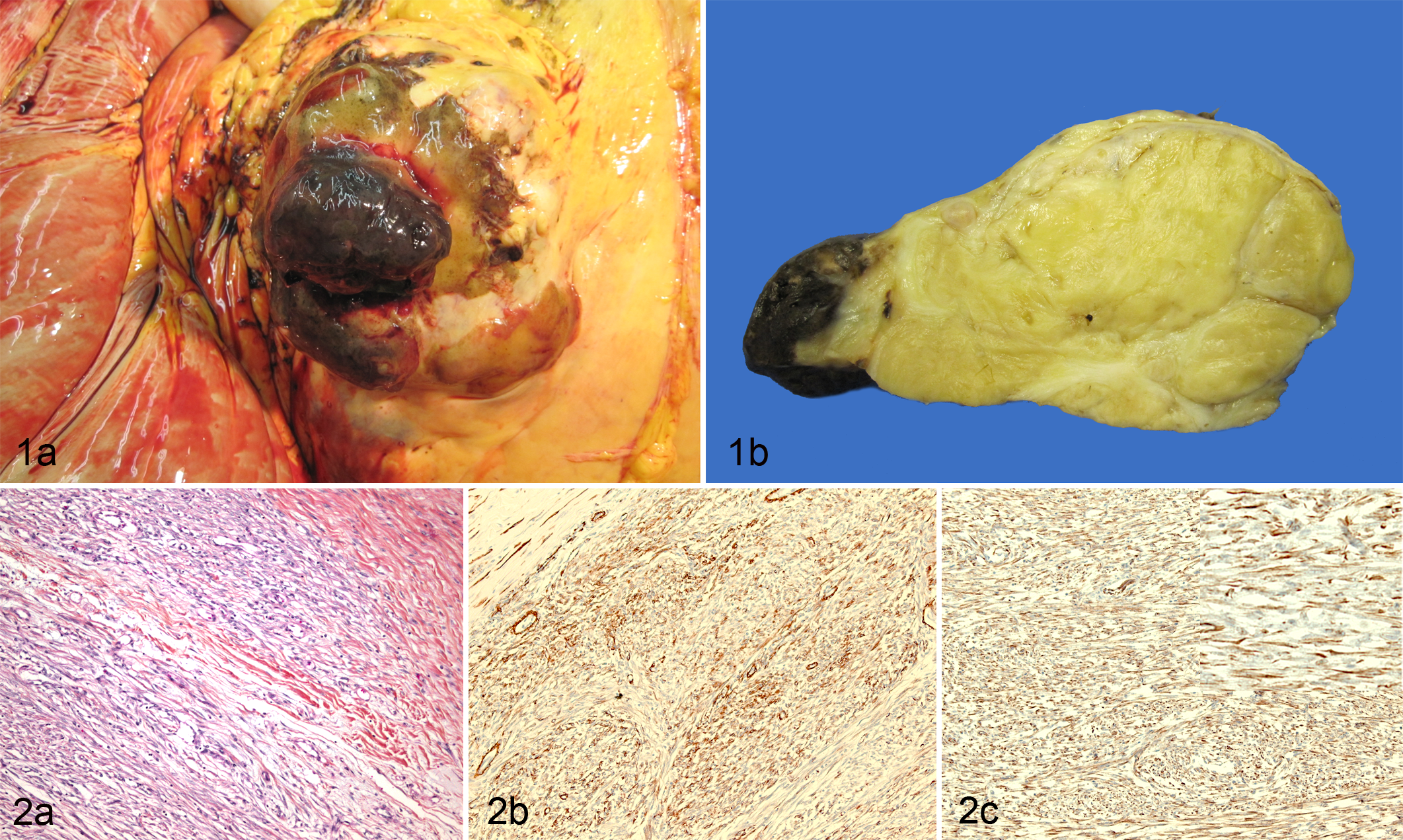
At necropsy, mild subcutaneous edema was present in the ventral aspect of the posterior abdomen. The abdominal cavity contained blood-tainted ascites (approximately 2.5 liters). A protruding mass measuring 10 × 15 × 8 cm was present in the abdominal wall, on the right posterior area close to the umbilicus (Fig. 1a). It was firm, infiltrative, multinodular, and yellow (Fig. 1b). The variably sized nodules were separated by a moderately abundant connective tissue. Hemorrhagic foci less than 2 cm in diameter were observed in the mass. Voluminous vessels were present at its base. Soft hemorrhagic projections 3 to 4 cm in diameter were extended into the abdomen. No other gross abnormality was observed in the mare.
Differential Diagnoses
The differential diagnoses considered in view of the gross observations were fibroma, desmoid fibromatosis, rhadomyoma, mesothelioma, hemangioma, hemangiosarcoma, giant cell tumor of soft parts, and fibrosarcoma.
Microscopic Findings
Histologically, the mass was unencapsulated and had no distinct borders. It was infiltrative and composed of bundles and sheets of densely packed fusiform cells forming collagen (Fig. 2a). The fibroblastic cells had a scant basophilic cytoplasm, with an elongated pale basophilic nucleus and 1 small eosinophilic nucleolus. No anaplastic features or mitosis were observed. A progressive maturation was present, with the density of cells becoming less as the density of the collagen was higher. Strands of dense collagenous tissue divided the mass in nodules. Mononuclear inflammatory cells and siderophages were present in zones of edema and necrosis. Large vessels were observed at the base of the mass, but the vascularity of the tissue was generally low. The abdominal surface was necrotic, and hemorrhagic and vessels of this area were thrombosed. Siderophages were present. Immunohistochemical labeling with antibodies to α–smooth muscle actin (Fig. 2b) and vimentin (Fig. 2c) revealed numerous positive-staining cells. Some cells labeled positively to desmin. Immunohistochemistry for estrogen receptor was negative.
Diagnosis
Abdominal wall desmoid fibromatosis was diagnosed, considering the histologic aspect of the mass, the low number of mitosis, the progressive maturation, and the immunohistochemical results.
Discussion
Fibromatoses are proliferative fibroblastic/myofibroblastic lesions that are infiltrative and often recur locally after surgery but are nonmetastasizing. 5 The exact nature of fibromatosis, reactive or neoplastic, has long been discussed, but cytogenetic analysis of human lesions and the propensity for destructive recurrence support a neoplastic process. 3,5,12 The cells generally have an ultrastructure compatible with mature fibroblasts but may show occasionally a myofibroblastoid appearance. 2,5,10 Some maturation occurs in fibromatosis, with the neoplastic cells being less abundant in the central portion than in the periphery of the tumor. 3
Depending on their localization, they are classified as superficial fibromatosis (in fascias or aponeurosis) or desmoid fibromatosis (in deep tissues). In humans, desmoid tumors can be localized in the abdominal wall, in the abdominal cavity, or in extra-abdominal sites and can attain a large size. 2,12 Some are associated with familial adenomatous polyposis. 9 In young women, they frequently appear during or soon after pregnancy and often tend to develop in a preceding scar. 5 Antiestrogens are used to treat this condition, but their effects do not seem to be attributable to the presence of estrogen receptor α. 8 In the present case, there was no history of previous foaling, and immunohistochemistry was negative for this receptor. The labeling of neoplastic cells by immunohistochemistry for α–smooth muscle actin is variable from a case to another. 4,7,13,15
Fibromatoses are rarely observed in domestic animals. 11 They have been reported in horse, 6,15 dog, 2,13 cattle, 4 goat, 14 rat, 7 and cat. 10 Aggressive fibromatous masses have been observed in a 9-month-old cat, infiltrating principally the subcutis and the bones of a forelimb. Histologically, an infiltrative growth of fibroblasts and some multinucleated giant cells invaded muscles and bones and were associated with deposition of a large amount of collagen. 10 A similar case in a young Bernese Mountain Dog was localized in a limb. 13 Congenital desmoid fibromatosis has been observed in the muscles of the head of a Holstein heifer. 4
As in other species, fibromatoses in horse principally affect skeletal muscles. 6,11,15 In 2 young horses, the cervical and the pectoral musculatures were affected; the presence of fluid-filled cavities associated with sterile inflammation suggested a possible traumatic origin in those cases. Surgical excision was possible in 1 case and seemed to have been curative. 15 Subcutaneous fibromatosis infiltrating the thorax and pectoral muscles, with scar-like bands of collagen extending from the dermal and subcutaneous tissues to the muscles, has been reported. 6 A paranasal sinus fibromatosis has been observed in a horse that previously had been treated for an ethmoid hematoma. The mass recurred some months after its excision. 1
Desmoid fibromatosis of the abdominal wall has been rarely reported in veterinary medicine. A case in a 10-week-old Akita, associated with a recurrent umbilical hernia, was similar to the desmoid-type fibromatosis of children. The tumor did not recur 14 months after extensive surgical resection. 2 Fibromatosis-type fibroma developed at laparotomy sites in heterozygous Nihon rats. 7 In a young goat, multiple hard, plate-forming fibromatous masses have been observed in the abdominal wall and in the medial aspect of the upper hind limbs. 14 In the present case, there was no history of previous abdominal wall anomaly or surgery.
The mass observed in this horse is compatible with a desmoid fibromatosis of the abdominal wall; there was an infiltrative proliferation of fibroblasts producing collagen with maturation, without anaplastic features or metastasis. To our knowledge, the localization and the clinical presentation have not been reported previously in the horse.
Footnotes
Acknowledgements
We thank Drs Matti Kiupel and Monique Doré for immunohistochemistry and Claude Paquet, Jacinthe Cardin, Nancy Veilleux, and Marco Langlois for technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.